
Abstract
Objectives
To summarise the impact of community-based interventions for multimorbid patients on unplanned healthcare use. The prevalence of multimorbidity (co-existence of multiple chronic conditions) is rapidly increasing and affects one-third of the global population. Patients with multimorbidity have complex healthcare needs and greater unplanned healthcare usage. Community-based interventions allow for continued care of patients outside hospitals, but few studies have explored the effects of these interventions on unplanned healthcare usage.
Design
A systematic review was conducted. MEDLINE, EMBASE, PsychINFO and Cochrane Library online databases were searched. Studies were screened and underwent risk of bias assessment. Data were synthesised using narrative synthesis.
Setting
Community-based interventions.
Participants
Patients with multimorbidity.
Main outcome measures
Unplanned healthcare usage.
Results
Thirteen studies, including a total of 6148 participants, were included. All included studies came from high-income settings and had elderly populations. All studies measured emergency department attendances as their primary outcome. Risk of bias was generally low. Most community interventions were multifaceted with emphasis on education, self-monitoring of symptoms and regular follow-ups. Four studies looked at improved care coordination, advance care planning and palliative care. All 13 studies found a decrease in emergency department visits post-intervention with risk reduction ranging from 0 (95% confidencec interval [CI]: –0.37 to 0.37) to 0.735 (95% CI: 0.688–0.785).
Conclusions
Community-based interventions have potential to reduce emergency department visits in patients with multimorbidity. Identification of specific successful components of interventions was challenging given the overlaps between interventions. Policymakers should recognise the importance of community interventions and aim to integrate aspects of these into existing healthcare structures. Future research should investigate the impact of such interventions with broader participant characteristics.
Introduction
Multimorbidity, the coexistence of two or more chronic medical conditions, 1 affects one-third of the global population and two-thirds of over 65-year-olds. 2 Given that risk factors for multimorbidity include age, obesity and physical inactivity, 3 the ageing global population and obesity epidemic will contribute to its increasing prevalence worldwide.4,5 One-third of people with multimorbidity have both a physical and mental health disorder, 6 which may impede their ability to adhere to treatment, continue with physical activities and function socially. 7 Multimorbidity is therefore associated with reduced quality of life and increased mortality. 8
Patients with multimorbidity exhibit greater unplanned healthcare use. One UK study found 27.2% of patients had multimorbidity; yet, these accounted for 56.1% of hospital admissions and 78.7% of prescriptions. 9 Another found that patients with four conditions have almost 15 times the odds of an unplanned hospital admission. 10 This is consistent with research from other European countries.11,12 The financial cost of unplanned healthcare usage to the health system is immense 13 ; in England, in 2016, emergency department (ED) admissions alone cost the National Health Service £2.7 billion. 14
One way of reducing unplanned admissions is through community programmes supporting longer-term management outside of hospitals. A systematic review exploring general practitioners’ (GPs) perspectives on management of patients with multimorbidity highlighted challenges faced by these patients, including poor care coordination, polypharmacy and increased treatment burden. 15 Community care programmes help equip patients to manage their conditions long-term through educational resources, frequent follow-ups from healthcare teams, optimisation of polypharmacy and self-monitoring of symptoms.
Few studies assess interventions to improve outcomes for patients with multimorbidity. A systematic review of community care-based interventions looked primarily at quality-of-life outcomes and concluded that evidence on care targeted towards patients with multimorbidity was limited. 16 Similarly, a recent systematic review of goal-oriented care for adults with multimorbidity was inconclusive, finding no effect on quality of life or hospital admission. 17 Existing studies have placed little emphasis on clinical outcomes, and none have focussed on unplanned healthcare usage. This review therefore aims to summarise the effects of community-based interventions targeted at multimorbid patients, and explore and compare the different types of interventions implemented and their impact on unplanned healthcare usage.
Methods
A systematic review of the literature was carried out according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines 18 (Supplementary Appendix 1). Ethical approval was not required.
Eligibility criteria
Inclusion criteria were structured using the Population, Intervention, Comparison, Outcome and Study Design framework. 19 Studies were eligible for inclusion if the study sample consisted of adults with multimorbidity, defined as individuals over the age of 18 years with at least two co-existing chronic medical conditions. Interventions suitable for inclusion were conducted either in the primary healthcare setting or within the community and involved holistic management of the patient. The outcome measure was unplanned care, encompassing all forms of unscheduled healthcare.
Search strategy
The search strategy used key words, search headings such as ‘multimorbid’, ‘emergency care’ and ‘care plan’, and appropriate synonyms to identify relevant studies. The full search strategy for MEDLINE can be found in Supplementary Appendix 2.
Information sources and selection process
The online databases Medline, Embase, PsycINFO and Cochrane library were searched from January 1980 to March 2022. Identified studies were imported into the Covidence systematic review tool and de-duplicated. Two independent reviewers screened the titles and abstracts of articles, then full texts of eligible papers, to select the final sample of articles.
Data collection and synthesis
Data from eligible studies were extracted and collated into a table including study design, population characteristics, intervention details, outcome measures and findings.
Risk of bias assessment
Studies were appraised using quality assessment tools specific to each study design (randomised controlled trial [RCT], randomised non-controlled, observational, cohort) developed by the National Heart, Lung and Blood Institute (Supplementary Appendix 3). 20
Results
Searches identified 4454 studies (Figure 1). Thirteen studies were selected for inclusion; data were extracted and analysed using narrative synthesis.21 –33 Meta-analysis was not possible due to the heterogeneity of the study populations, with varying numbers and types of conditions across the populations.
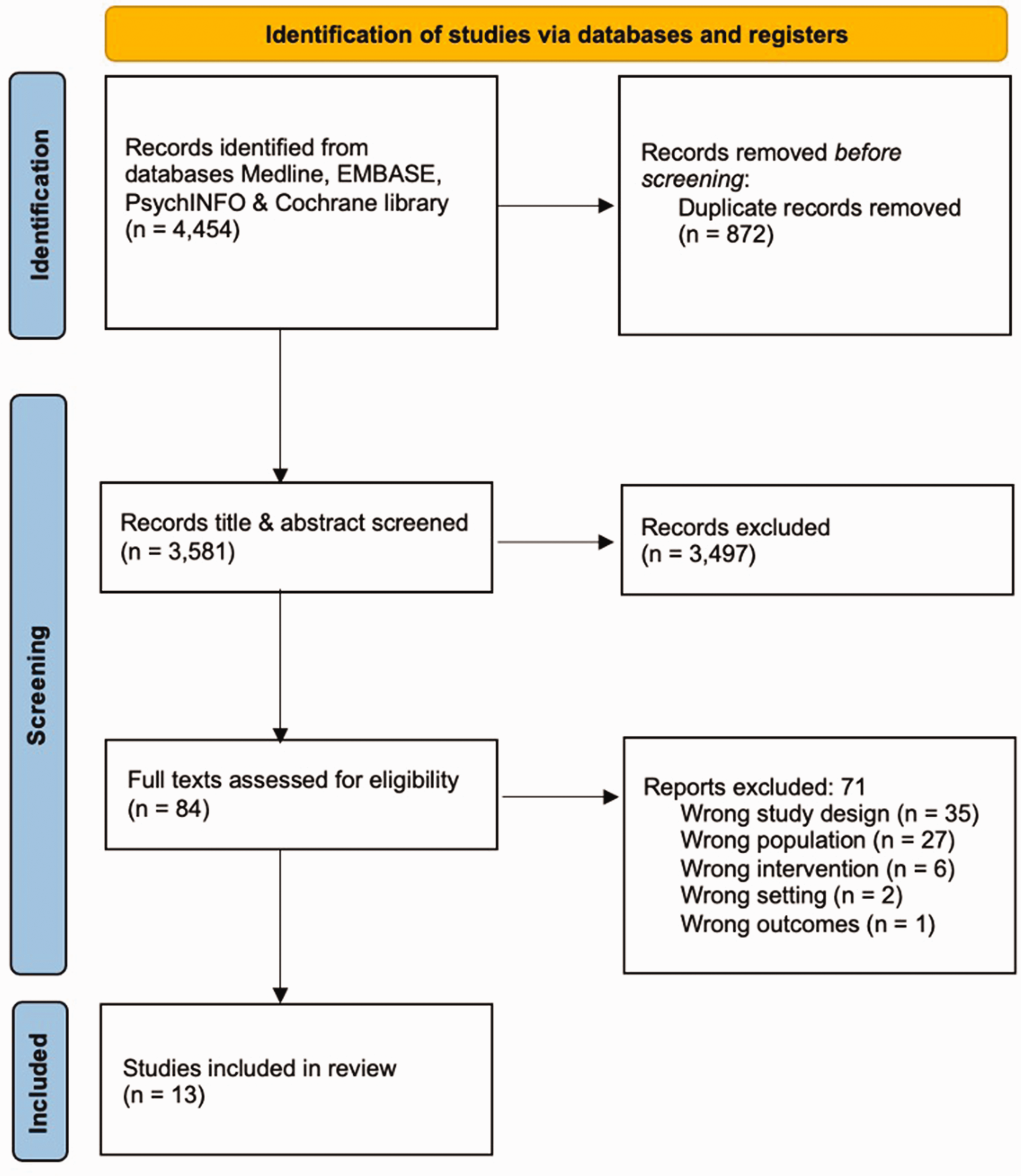
A PRISMA flowchart showing the identification and screening of studies from databases.
Study characteristics
All 13 studies (Table 1) were conducted in high-income countries (HICs), with study designs including RCTs (including a cost-utility analysis based on an RCT), prospective observational studies and retrospective cohort studies. A total of 6148 participants were included across all studies; sample sizes ranged from 15 to 3305, with the majority reporting on more than 200 patients. Most populations contained patients identified from a hospital setting or primary care databases. All studies reported ED attendances as a measure of unplanned healthcare usage.
A Table showing key information and results from each included study, categorised by the type of intervention.
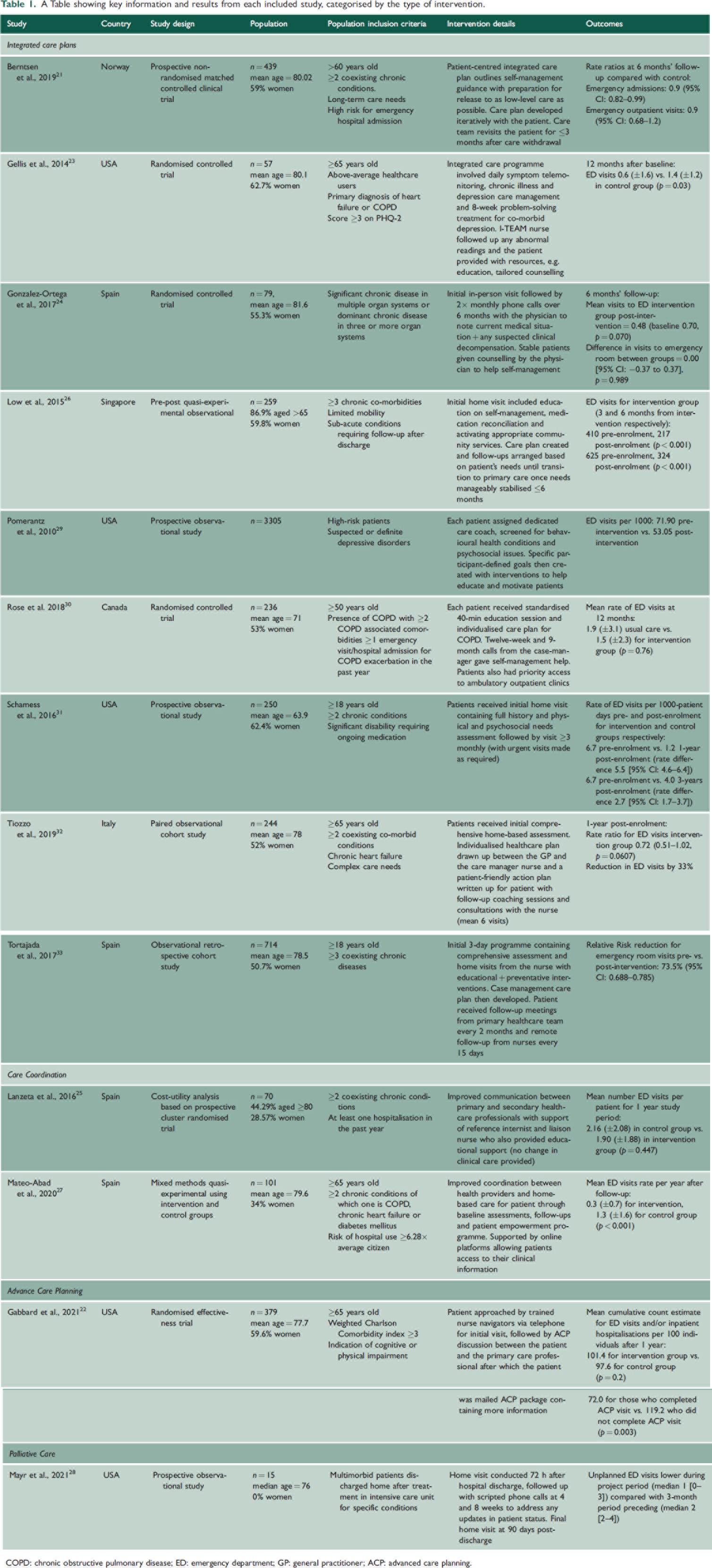
COPD: chronic obstructive pulmonary disease; ED: emergency department; GP: general practitioner; ACP: advanced care planning.
Risk of bias assessment
There was low risk of bias across the studies; three studies were rated good quality,23,26,30 eight were fair21,22,24,25,27,31 –33 and two were poor.28,29 Studies were not excluded based on quality. All studies had clearly defined objectives and recruited participants with the same eligibility criteria (Supplementary Appendix 3).
Populations
Studies provided varying detail regarding the complexity and severity of multimorbidity. Five studies specified co-morbidities within the inclusion criteria, including depression23,29 and chronic obstructive pulmonary disease. 30
Eleven studies had additional population inclusion criteria, including those with complex care needs or disability,21,22,26,31,32 high risk of future hospital admission or current high-utilisers,21,23,27,29 and recent discharge from hospital.25,28,30
Six studies had an inclusion criteria of age ≥50 years.21 –23,27,29,32 The average age of participants within each study was ≥60 years in every study that reported population demographics21 –28,30 –32; eight had average ages ≥75 years.21 –24,27,28,32,33
Interventions
Ten interventions involved individual care plans,21,23,24,26,27,29 –33 two care coordination (one of which also had a care plan component),25,27 one advanced care planning (ACP) 22 and one palliative care. 28 Care plans primarily aimed to help the patient with self-management of their conditions through methods such as education, frequent follow-ups, counselling and goal-setting.
The ACP intervention involved a discussion between the patient and the nurse to inform of end-of-life options, 22 while Lanzeta et al. used an administrative member of staff to improve communication between primary and secondary healthcare professionals (HCPs) without changing clinical care. 25 Mayr et al. used follow-ups to monitor patients at the end of life; however, this study only had 15 participants as its primary aim was to assess the feasibility of the intervention and as such they did not comment on statistical significance of results. 28
ED visits
Twelve studies reported ED attendances as an outcome21,23 –33; one measured an estimate for ED visits and/or inpatient hospitalisations. 22 All 13 studies reported a decrease in ED attendances across the study period. Two did not report significance,28,29 and four did not find statistically significant differences.24,25,30,32 Of the significant results, six interventions were integrated care programmes21,23,26,27,31,33 and one ACP. 22 No studies included the reasons for ED visits.
Delivery of interventions
Interventions were predominantly delivered through a combination of in-person visits and remote consultations between the patient and the care team.22,24,26 –28,30,32,33 One study used telephone communication only, with a focus on telemonitoring and management of depressive symptoms. 23 This found a significant decrease in mean ED visits after 12 months compared with the control group (0.6 ± 1.6 vs. 1.4 ± 1.2, p = 0.03). One study only used in-person visits and found a rate reduction of 5.5 ED visits per 1000-patient days (95% CI: 4.6–6.4). 31 In another study, there was no direct contact between the intervention team and the patient, as the focus was on care coordination within the healthcare team and no difference in mean ED visits per patient was found between study groups. 25
Three studies prioritised telemonitoring as a key component of their interventions.23,27,33 One also used an online platform to facilitate messaging between patients and carers and give patients access to their health information, 27 resulting in a significant difference in mean ED visits rate per year post follow-up between intervention and control groups (0.3 ± 0.7 vs. 1.3 ± 1.6, p < 0.01).
Two studies did not explicitly state the nature of interactions between the patient and the team.21,29
Multidisciplinary teams
Of the 10 care plan interventions, seven had nurse case-managers.21,22,26,27,30,32,33 All but one of the care plans involved a multidisciplinary team (MDT)21,23,26,27,29 –33; Gonzalez-Ortega et al. used an intervention conducted solely by a family physician and found a 5.6% decrease in ED visits in the intervention group, but when compared with the control group post-intervention, there was no difference. 24 Two of these MDTs consisted of several specialists including a doctor, nurse, physiotherapist, occupational therapist, speech therapist, social worker, 26 geriatric nurses, pharmacists and secretaries. 21
Care coordination
Mateo-Abad et al. 27 used an integrated care coordination and care plan intervention with follow-ups and a patient empowerment programme, accompanied by online access to their clinical records. The mean rate of ED visits after a year was 0.3 ± 0.7 for the intervention group compared with 1.3 ± 1.7 for the control group (p < 0.001). Both this study and Lanzeta et al. 25 used reference liaison nurses to improve coordination between HCPs and provide educational support to the patient; however, Lanzeta et al. did not find a significant difference in mean ED visits per patient between intervention and control group (1.90 vs. 2.16, p = 0.447).
Advanced care planning for end of life
Gabbard et al. 22 reported a risk ratio of 1.17 (95% CI: 0.92–1.50) for ED visits and/or inpatient hospitalisations for intervention (ACP) compared with control group. However, when comparing those who completed the intervention with those within the intervention group who did not have a completed telephone call/in-person visit, the risk ratio was 0.59 (95% CI: 0.42–0.83).
Depression
Two studies included interventions targeting depression. Gellis et al. 23 implemented an 8-week problem-solving therapy intervention to treat co-morbid depression. Pomerantz et al. 29 screened for behavioural and psychosocial issues at the start of the intervention, and then used personal goal-setting and motivational interventions throughout. Pomerantz et al. did not report on changes related to depression but found a 26.2% decrease in ED visits per 100 pre- versus post-intervention (the significance was not noted). Gellis et al. 23 found a significant reduction of 50% in the mean score on PHQ-9 at 3 months post-enrolment and a significant reduction in ED visits between the intervention and control groups.
Social care
Five care plans specifically addressed the social care needs of participants.24,26,31 –33 Of these, Schamess et al. 31 aimed to address social issues in subsequent visits, while Tortajada et al. 33 involved a social worker in the care plan where needed. Low et al. 26 activated community services to aid the patient’s care at home. These three studies that described how they addressed social care needs yielded statistically significant results. Of the two that only mentioned assessing care needs, one had a rate ratio of 0.72 (95% CI: 0.51–1.02) for ED visits in the intervention group, 32 while the other had a rate ratio of 0.00 (95% CI: −0.37 to 0.37). 23
Planned healthcare usage
Six studies reported outcomes of planned healthcare usage.21,24 –27,33 Berntsen et al. 21 reported that planned outpatient visits increased significantly in the intervention group. Low et al. 26 found a statistically significant increase in specialist outpatient clinic visits; similarly, Tortajada et al. 33 found a statistically significant increase in rate of admissions to a community healthcare unit (risk ratio: 1.502, 95% CI: :1.346–1.675). Mateo-Abad et al. 27 found a statistically significant difference between intervention versus control group in rate of GP appointments per year both face-to-face (12.2 vs. 9.6) and over the phone (6.7 vs. 3.6). Gonzalez-Ortega et al. 24 found a notable, but not statistically significant, increase in elective hospital admissions in the intervention group (mean 0.04 ± 0.26 at baseline vs. 0.13 ± 0.34 at follow-up). On the other hand, Lanzeta et al. 25 found little difference in primary care consultations between intervention and control groups (median visits 22.7 vs. 20.04).
Discussion
Summary of findings
This review of community interventions for patients with multimorbidity included 13 studies with an overall low risk of bias. Most included elderly, high-risk populations. All studies found that community interventions for patients with multimorbidity decrease the likelihood of ED visits, with seven reporting statistically significant decreases.21 –23,26,27,31,33 Successful interventions emphasised a personalised approach, working synergistically with the patient to ensure their needs were met.
Strengths and limitations
This is, to our knowledge, the first review focussing on unplanned healthcare usage outcomes of community-based interventions for multimorbid patients. A previous review of systematic reviews on the community interventions for multimorbid patients found a significant improvement in clinical outcomes 34 ; however, the effect on healthcare usage outcomes has not been found to be significant by other reviews.16,34 This may be due to a paucity of studies using well-defined measures of healthcare usage as an outcome, or different definitions of community interventions, impacting the comparability between studies. Our review provides compelling evidence as to the benefits of holistic community interventions for this patient population.
Implications for policy and practice
The results of this review address an eminent literature gap for patients with multimorbidity, adding valuable insights into the benefits of community interventions to reduce ED admissions. It is crucial to utilise this growing evidence base to guide health services through a difficult period of demographic transition, to mitigate the burden placed on systems by complex populations.
Wider inclusion criteria for studies included in national guidelines
Policy makers at the national level should prioritise the inclusion and focus on patients with multimorbidity within national guidelines to improve the quality of care for this growing patient population. Historically, healthcare systems have focussed on acute care delivery and individual diseases rather than coexisting conditions. 35 Additionally, guidelines are often based on evidence from RCTs that exclude elderly or multimorbid patients.36,37 Emphasis therefore should be placed on modifying guidelines to include studies with wider population inclusion criteria to reflect the ever-changing demographic of patients.
Greater provision of telemonitoring solutions
Health service providers should take advantage of the benefits of telehealth and remote monitoring of patients to alleviate pressures in an increasingly technological world. Many chronic conditions stem from issues such as obesity and hypertension that can be easily monitored remotely by the patient themselves 38 ; several lobbying powers, including NGOs, are already calling for greater accessibility to such home-monitoring devices. 39 Telehealth also has great potential to ease the increased waiting times and backlog of patients in the post-pandemic era. 40 Throughout the pandemic, telemedicine rapidly became an essential part of primary care, 41 demonstrating the feasibility of its widespread adoption. Greater trust should be placed in at-home equipment and remote monitoring of patients, and healthcare providers should additionally consider promoting and supporting schemes to distribute these equipment to aid in eliminating any financial and educational barriers to access.
Redistributing workload between different HCPs
Healthcare service decision makers should better utilise the strengths of multidisciplinary working and the varied skillsets of different HCPs. 42 Most studies in this review used nurses who acted as case-managers, with other non-medical HCPs delivering many of the interventions. The specialist skillset of nurses ensures a high standard of, and satisfaction with, care43,44; other HCPs, such as pharmacists, could also suitably fill similar roles. 45 The number of people in England waiting for consultant-led elective care has increased from 4.05 million pre-pandemic to 7.2 million in December 2022, with a record 3.1 million waiting for over 18 weeks. 46 Redistributing workload among different HCPs could help ease this strain 47 and prove more cost-effective long-term.
Implications for future research
Most studies only reported a few outcomes, and most did not explore the reasoning for ED visits in any depth. Further research into specific aspects of care plans may help determine ideal care plan designs and exploration of outcomes such as quality of life and patient satisfaction. In combination with healthcare usage, this may help create a more holistic understanding of the impact of community interventions. Given that several social and structural factors are involved in determining outcomes for patients with multimorbidity, studies should also aim to consider how effective interventions are within different populations. Future studies may also consider longitudinal study designs, allowing for a more comprehensive understanding of the long-term impact.
The small number of studies eligible for inclusion in this review may indicate a paucity of research; emphasis should therefore continue to be placed on the exploration of long-term community-based interventions. Focus should be placed on research within lower-income countries. Moreover, within the literature, multimorbidity is defined and measured in several different ways 48 and is sometimes conflated with other similar terms such as ‘complex’ or ‘frail’; future research should clearly state how multimorbidity is understood.
All populations included were elderly. Although the prevalence of multimorbidity is greater in older populations, the needs of younger adults living with multimorbidity are likely different and should be carefully considered. Additionally, several studies excluded participants with poor cognitive functioning; a significant proportion of elderly people with multimorbidity have a form of cognitive impairment 49 and this may affect implementation of interventions.
Financial benefits of interventions make compelling arguments for commissioners and politicians when considering policy changes. Although this review has demonstrated that ED wait times are reduced using community interventions – and this therefore reduces strain on the healthcare system – the direct costs of implementing these interventions compared with the financial benefits have not been investigated in depth. Future research should therefore consider the monetary aspect of such interventions to determine their overall viability.
Conclusion
Community interventions for patients with multimorbidity are useful in continuing longer-term care. All studies included in this review found a decrease in ED visits within intervention groups; the majority were statistically significant. Interventions with the most significant improvements placed emphasis on education, goal-setting and regular follow-ups. Policy-makers should consider the long-term benefits of these interventions both from a financial and healthcare perspective, with a view to integrate elements of the interventions such as telehealth and tailored education into existing healthcare structures. However, further research into the specific components of successful interventions and their financial consequences is required to ascertain how to practically and successfully implement these interventions on a wider scale.
Supplemental Material
sj-pdf-1-jrs-10.1177_01410768231186224 - Supplemental material for The effects of community interventions on unplanned healthcare use in patients with multimorbidity: a systematic review
Supplemental material, sj-pdf-1-jrs-10.1177_01410768231186224 for The effects of community interventions on unplanned healthcare use in patients with multimorbidity: a systematic review by Tavleen Wasan, Benedict Hayhoe, Meryem Cicek, Elena Lammila-Escalera, Dasha Nicholls, Azeem Majeed and Geva Greenfield in Journal of the Royal Society of Medicine
Supplemental Material
sj-pdf-2-jrs-10.1177_01410768231186224 - Supplemental material for The effects of community interventions on unplanned healthcare use in patients with multimorbidity: a systematic review
Supplemental material, sj-pdf-2-jrs-10.1177_01410768231186224 for The effects of community interventions on unplanned healthcare use in patients with multimorbidity: a systematic review by Tavleen Wasan, Benedict Hayhoe, Meryem Cicek, Elena Lammila-Escalera, Dasha Nicholls, Azeem Majeed and Geva Greenfield in Journal of the Royal Society of Medicine
Supplemental Material
sj-pdf-3-jrs-10.1177_01410768231186224 - Supplemental material for The effects of community interventions on unplanned healthcare use in patients with multimorbidity: a systematic review
Supplemental material, sj-pdf-3-jrs-10.1177_01410768231186224 for The effects of community interventions on unplanned healthcare use in patients with multimorbidity: a systematic review by Tavleen Wasan, Benedict Hayhoe, Meryem Cicek, Elena Lammila-Escalera, Dasha Nicholls, Azeem Majeed and Geva Greenfield in Journal of the Royal Society of Medicine
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.