
Abstract

Consultation time in adult general practice is affected by myriad practice, physician and patient factors, as well as by the type of problem. 1 This inherent complexity culminated in an average duration of consultation of a meagre 5.0–11.7 min in the UK, and 9.2–21.07 min in the USA according to higher quality studies. 2 Research has demonstrated a trend toward longer consultations, but surprisingly, the change is slow and small – often an additional minute or two. 3 For example, in Germany the average time per patient contact was 7.8 min in 2006, increasing to 9.1 in 2009. Virtual care that has increased since the COVID-19 pandemic has not made a substantial change, since most issues are much better dealt with in a personal visit.
How do these time constraints, closely monitored by third parties, compare to the expanding tasks that primary physicians are expected to perform during the encounter to be considered ‘professional’, ‘competent’ and ‘patient-centred’ by their peers and superiors, indeed by themselves? The gap between obligatory demands and the time allotted to complete them is appalling. A list of the obligatory requirements of a first clinical encounter in general practice consultations is presented in Table 1.
The obligatory requirements of a first clinical encounter in general practice consultations.
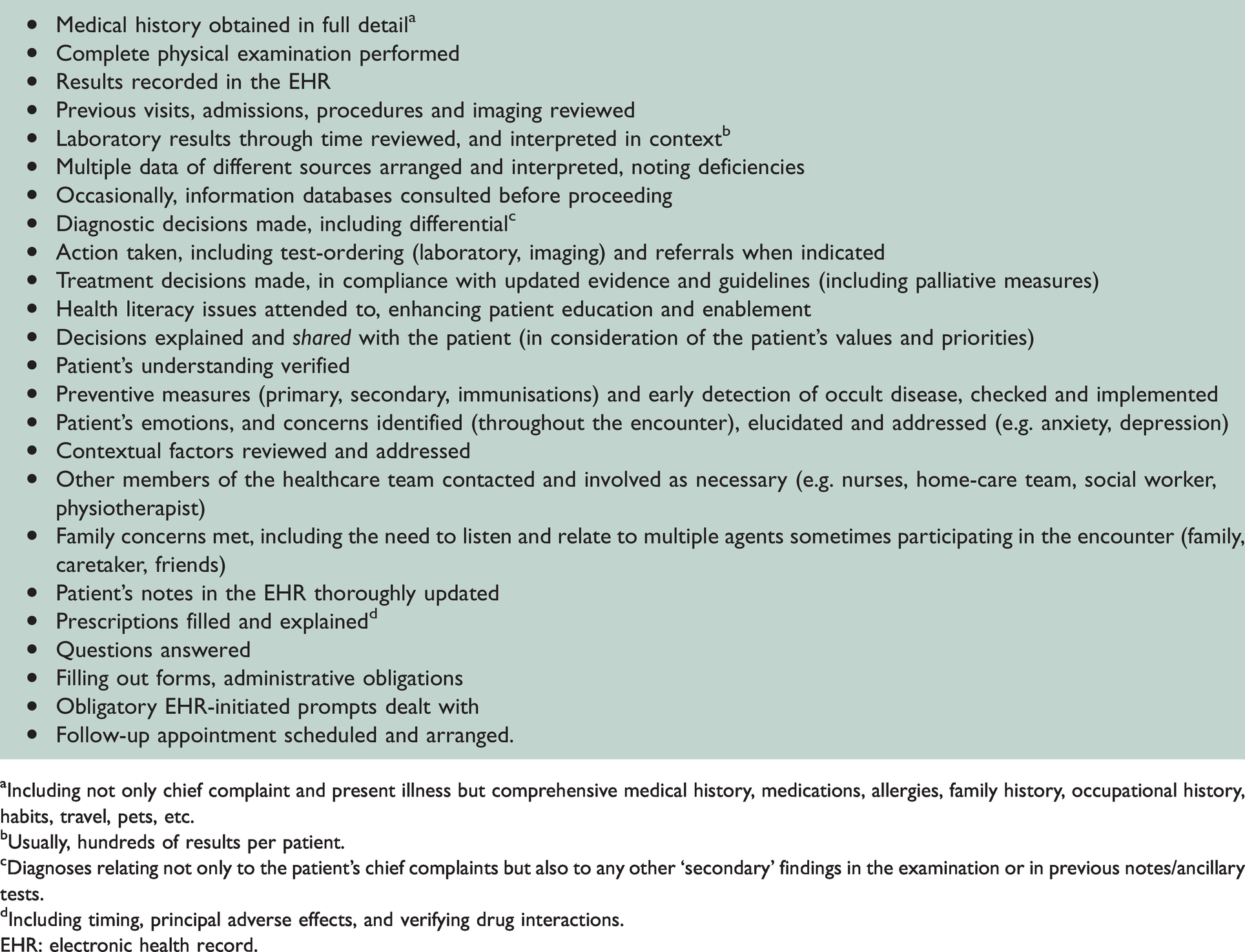
aIncluding not only chief complaint and present illness but comprehensive medical history, medications, allergies, family history, occupational history, habits, travel, pets, etc.
bUsually, hundreds of results per patient.
cDiagnoses relating not only to the patient’s chief complaints but also to any other ‘secondary’ findings in the examination or in previous notes/ancillary tests.
dIncluding timing, principal adverse effects, and verifying drug interactions.EHR: electronic health record.
Although a more focused, shorter approach may be sufficient in simple, straightforward presentations (e.g. a young woman with cystitis or a patient with an ankle sprain), many patients, even on repeated visits, require a full workup. Clearly, with so many items to be addressed through the visit, the time-per-item has markedly decreased.4,5 As an inescapable result, the depth and quality suffer, and important issues tend to be performed in a perfunctory manner, or skipped altogether. The impact of these increasing requirements is even more striking when ubiquitous ongoing changes affecting the encounter and its escalating complexity are being considered. 6 They are very familiar to every clinician and include global, social, and practice trends. These trends encompass the ageing of the population, increasing longevity and concurrently mounting co-morbidity, polypharmacy – carrying higher risk of adverse effects and drug interactions, and, often, ethnic diversity with cultural and communication barriers to overcome. The current, frequently fragmented care and consequent need to become acquainted with, and consider other physicians’ actions, adds to the practitioner’s burden. In addition, patients with cognitive and motor function decline are more frequently encountered, slowing the tempo of the encounter, as do patients with medically unexplained symptoms (11% in one study), 7 highlighting the implicit uncertainty in many encounters, and the need of some physicians ‘to protect their backs’ in an era of increasing negligence claims. Into this boiling cauldron are thrown in the typical high workload each day, and the overwhelming volume of evidence and guidelines coming at the physician and constantly changing.
Thus, it is hardly surprising that physicians working under such hectic conditions, with the Damocles sword of time constraints hanging over their heads, adapt by skipping important history and examination elements; deficient data entry in the patients’ charts, increased use of heuristics (associated with more diagnostic errors); ‘tunnel vision’ (focusing on the major complaint at the expense of other less pressing but meaningful pathologies); a ‘shotgun approach’ in test-ordering and referrals (incurring delays, cost, anxiety and cascades of incidental findings leading to more testing);8,9 decreased provision of preventive services; and poor attention to patient cues, emotional state and suffering. In addition, patient-centred care and shared decision-making are very often neglected, even in complex decisions where patient and family involvement is most required.10 These deficiencies occur despite the high yield (positive and negative) of simple tests such as a careful history and physical examination, and the pivotal role of patient-centred care in implementing the patient’s autonomy and health care quality.
Being aware of these deficiencies and compromises in the delivery of care, one patient after another, day after day, burnout among providers is common in all settings, with associated depersonalisation, negative patient care experiences, increasing errors and physicians’ deteriorating quality of life and health, among other damages. Not surprisingly, physicians in primary care have among the highest prevalence of burnout of any medical specialty (63% in 2014).
Since the relatively very short face-time with the patient in primary care seems the ‘origin of evil’ as supported by much data on the relationship between consultation length and outcomes, 10 one would expect to find a strong body of evidence on interventions to lengthen the time per patient, and their effects. However, such research is conspicuously lacking, and studies that have been done are deficient in that a minuscule increase in time has been usually examined, and even this, looking into neither cost-effectiveness nor validated outcomes. 11 This absence is particularly conspicuous when indications of improved quality of care associated with longer consultation durations are considered,2,10,11 together with the suggestion to view consultation length as a proxy measure of quality of care.
A fresh start is urgently needed, adapting the consultation time in primary care that has shown little change over time, to the advances of our century, including the information and communication technology revolution, evidence-based practice, patient-centeredness and enablement, and resurrection of empathy in the clinical encounter. Noting the absence of data on the length of consultation that can accommodate its quintessential elements, and the very low grading and inadequacy of current evidence, extensive time-motion studies of primary care providers’ performance, are needed to first determine the optimal duration of quality consultation of new patients (which may be age-dependent and complexity-dependent), regardless of current norms and restrictions. Next, large-scale long-term studies must be organised to compare new versus current consultations, focusing on many variables including quality of care, patient satisfaction, physician satisfaction, health outcomes and cost-effectiveness. Ideally, a physician could choose to label a consultation as ‘complex’ (requiring more time to cover challenges); or ‘regular’ (simple focused problems, filling of prescriptions or certificates, etc.) – where current time allotment will suffice. This option of flexible encounter duration will also give physicians back the control over their schedule, that many feel was absent in many settings. It is likely that part of the cost entailed in allowing for longer consultations will be covered by fewer tests, fewer referrals, contained use of drugs, fewer errors, less legislation and, quite possibly, strengthened patient–physician relationship, enhanced patient satisfaction and adherence, and improved health outcomes. All this will have to be confirmed first in large-scale, long-term trials.
Just as the Accreditation Council for Graduate Medical Education reform transformed the US residency programmes by allowing a maximum of 80-h work-week, an entirely new approach to redesign, uplift and remedy the primary care consultation will allow providers to take advantage of the astounding advances in medicine and treat their patients as they deserve, achieving improved health outcomes as well as the satisfaction of all partners and, very possibly, diminution of the burnout scourge.