
Abstract
The last 30 years have seen a revolution in the provision of minimal access surgery for many conditions, and technological advances are increasing exponentially. Many instruments are superseded by improved versions before the NHS and publicly funded health services can offer widespread coverage. Although we tend to think of minimal access surgery as a modern concept, Parts I and II of this series have shown that there is a 5000-year history to this specialty and our predecessors laid down many principles which still apply today. During the 19th and early 20th centuries, minimal access surgery was driven forward by visionary individuals, often in the face of opposition from colleagues and the medical establishment. However, in the last 30 years, innovation has been driven more in partnerships between healthcare, scientific, financial, educational and charitable organisations. There are far too many individuals involved to detail every contribution here, but this third part of the series will concentrate on some of the important themes in the development of minimal access surgery to its current status.
Professional organisations
In 1990, the Society of Laparoscopic Surgery was founded in the USA. This society is still a leading organisation in minimal access surgery worldwide, both for the expertise of its membership and for the reach of its house journal, the Journal of the Society of Laparoscopic Surgery, first published in January 1997. However, groups of surgeons interested in laparoscopic and minimal access surgery had begun to meet and correspond in order to encourage and support each other from the 1960s onwards. Initially, these arose out of existing surgical societies as mentioned in in Parts I and II1,2, and in 1964, the First International Symposium of Gynaecological Endoscopists was held in Palermo, Italy, which stimulated and enthused its participants to return to their home countries where they led the development of laparoscopic surgery within their own institutions. This was partly responsible for the resurgence of interest in laparoscopic surgery in the 1960s after a decade of relative stagnation.
The American Association of Gynaecologic Laparoscopists was founded by Jordan Phillips and colleagues in 1971 but has now grown to be one of the premier organisations leading laparoscopic surgery and has members in over 100 countries worldwide. As detailed in Part II, it was very much the gynaecologists who led the way in minimal access surgery for most of the 20th century, so it was not surprising that they founded the first professional organisation in this field.
After Semm publicised his technique of laparoscopic appendicectomy in 1980, and subsequently Műhe and Mouret reported laparoscopic cholecystectomy in the mid-1980s, general surgeons took to laparoscopic surgery with great enthusiasm and began to organise into local, national and international societies for mutual support, education and mentorship. The Society of American Gastrointestinal and Endoscopic Surgeons held its first meeting in Philadelphia in September 1983 as part of the American College of Surgeons Clinical Congress. Like many of its sister organisations, the Society of American Gastrointestinal and Endoscopic Surgeons has an official journal, Surgical Endoscopy, published by Springer-Verlag who assisted the Society of American Gastrointestinal and Endoscopic Surgeons to hold the First World Congress of Endoscopic Surgery in Berlin in 1988.
The European Association of Endoscopic Surgery was founded in Paris after a series of symposia in other European cities during 1989. Likewise, the Endoscopic and Laparoscopic Surgeons of Asia was founded by a small group of Asian endoscopic and laparoscopic surgery enthusiasts in 1990. The Endoscopic and Laparoscopic Surgeons of Asia’s objectives are to share experience and expertise, and to give advice on standards of practice in member countries which currently include Australia, Bangladesh, Brunei, China, England, Germany, Hong Kong, India, Indonesia, Japan, Korea, Macau, Malaysia, Myanmar, Nepal, Oman, Pakistan, Philippines, Russia, Sabah, Saudi Arabia, Singapore, Sri Lanka, Taiwan, Thailand, Turkey, UAE and Vietnam.
The Association of Laparoscopic Surgeons of Great Britain and Ireland was founded in 1994 in Harrogate by a merger of the Society of Minimally Invasive General surgeons and the British Surgical Stapling Group. Further detail of the history of each of these societies is given on their respective websites.
Quality assurance
Although much of the criticism of the pioneers described in Parts I and II had been due to personal conflicts, professional jealousies and territorial disputes, there were some substantive concerns regarding the safety of minimal access surgery and its appropriate use. Reports of iatrogenic injuries continued to occur with respect to gynaecologic surgery, especially in the use of the laparoscopic approach for emergency treatment of ectopic pregnancy. In 1980, the FDA published safety standards for gynaecological laparoscopy and many hospitals began to introduce their own codes of practice. However, the major problems started after the rapid uptake of laparoscopic cholecystectomy into widespread surgical practice in the late 1980s and early 1990s. This was done in a totally uncontrolled manner and many bile ducts were injured in the process. This led to a significant number of lawsuits with both financial implications and unwanted publicity and reputational damage. Analogous problems were occurring in laparoscopic gynaecology 3 and minimal access cardiac surgery. The latter led to a very critical article in the Wall Street Journal, 4 putting many enthusiastic laparoscopic surgeons on the back foot.
The profession responded by conducting well-constructed clinical trials and introducing mandatory training programmes in many branches of minimal access surgery (see below). These lessons have been applied in the current gradual introduction of robotic surgery. However, lest the profession becomes complacent, we should note that there are still areas of minimal access abdominopelvic surgery where sufficient caution has not been exercised and recent events have led to distress for patients and suspension or restriction of surgical practice.
The widespread adoption of mesh techniques to treat female pelvic problems from urinary incontinence to rectal prolapse, intussusception to dyspareunia, has led to an appalling trail of physical and functional damage. The National Institute for Health and Care Excellence belatedly introduced an effective ban on such treatments in 2017 but ‘nobody involved in the mesh revolution emerges covered in glory’.5–7 Colorectal surgeons and gynaecologists have more or less abandoned the operation of laparoscopic ventral mesh rectopexy, which had become extremely popular for a wide variety of pelvic floor problems during the previous decade. There are salutary lessons in this sorry episode that should be learned by professionals working in a system where ‘innovation’ is currently in vogue, attracting much funding and kudos.
Training
The requirement for training in surgery has been recognised since antiquity when the Hippocratic Corpus was practising in Kos in around 400 BC. The famous Hippocratic Oath (Ορκος) includes lines on the respect of a doctor for their teachers, and their duty to share their knowledge and craft with their sons and students. From Susrata in ancient India, via Arani in 16th century Italy, many of the surgeons mentioned in Parts I and II have taught and mentored their successors, even to the setting up of a formal training school by Palmer and the use of cadavers for training by Kelling. In the 1990s, the problems of iatrogenic injuries, lawsuits and reputational damage began to accrue and in some regions moratoria were placed on certain types of laparoscopic surgery. The need for both informal and formal training and mentorship was recognised, and the newly formed societies of laparoscopic and endoscopic surgeons were ideally placed to undertake this activity. Laparoscopic cholecystectomy was already in widespread practice, with sometimes disastrous results, but mentoring was offered to those in independent practice. It was easier to insist that aspiring surgeons in approved training programmes should undertake appropriate courses in both the basics of laparoscopic surgery and training for specific operations such as laparoscopic cholecystectomy. The American Board of Obstetrics and Gynaecology made training in laparoscopy a compulsory element of its residency programmes during the 1980s.
There was much controversy over the risk:benefit profile of laparoscopic resection for colorectal cancer during the early 1990s but, after the publication of the CLASSIC and COLOR trials (see below) and a change in NICE guidance, there was a need to train a large cadre of colorectal surgeons to perform these operations. The Department of Health, the Association of Coloproctology of Great Britain and Ireland and the Association of Laparoscopic Surgeons of Great Britain and Ireland, supported by Ethicon Endosurgery, set up LAPCO – a national training programme of laparoscopic colorectal surgery in England – and there have been similar programmes in most European countries and others worldwide.
Commercial collaboration
Minimally invasive surgery could not have developed to its current dominant position without close collaboration with commercial partners. Even in the 18th and 19th centuries, our surgical forebears worked with scientists and light makers in order to develop their early scopes. The French urologists who popularised endo-urology during the early 19th century entered into very fruitful partnerships with local instrument making companies such as Charrière and Luer in Paris, leading to the development of many improved endoscopes and attachments which became commercially available to colleagues throughout Europe. The concept of patenting inventions had long been in play, as evidenced by Edison’s patenting of the lightbulb in 1879, and it was generally accepted that technology could only improve if there was a financial model which rewarded investment and entrepreneurship.
Surgery has benefited from the revolution in lighting, photography and video technologies which have transferability to the medical field. The Heynmann Company in Germany produced the 135° angled lens system that Kalk introduced into clinical practice in the early part of the 19th century. However, it was the rise of the movie industry from the 1920s onwards that allowed ‘moving pictures’ to be applied to surgery and many other fields of human endeavour.
Karl Storz quotations.
Although there have been many controversies about the role of ‘Big Pharma’ in the practice of medicine and surgery, 9 it would have been impossible for minimal access surgery to have developed without commercial input. Most surgeons will have experience of company representatives attending theatre, bringing instruments and equipment for free trials, training theatre teams and sponsoring educational events and conferences. The potential for conflict of interest is ever-present and the professional must be alert to this, while not impeding innovations which may benefit their patients.
Clinical trials
The gold standard method of assessing any new intervention in medicine is a double-blinded randomised controlled clinical trial. However, such trials are rarely possible in surgery as blinding of the operator is impossible and the patient almost always knows which treatment they have or have not received. However, surgeons have made serious efforts in recent years to conduct robust multicentre trials and this is particularly the case for laparoscopic colorectal cancer surgery. Laparoscopic colectomy swiftly followed laparoscopic cholecystectomy in its uptake by general surgeons in the late 1980s and early 1990s. However, reports of poorer cancer survival outcomes and problems such as paucity of lymph node harvest and port site metastases began to arise, leading to a waning of enthusiasm for such operations. In order to allay these concerns, it became apparent that randomised clinical trials would be required. The UK multicentre CLASSIC trial was undertaken to compare open versus laparoscopic resection for colon and rectal cancers. The five-year survival was the same in both groups 10 but there were advantages in the laparoscopic group including lower rate of incisional hernia and fewer readmissions with small bowel obstruction. However, there was a 29% conversion rate to open surgery and a higher positive circumferential resection margin rate. Despite the latter, the long-term follow-up showed no difference in survival between the groups five years later. 11 The results of the CLASSIC trial along with those of the European COLOR trail persuaded the National Institute of Health and Care Excellence to recommend that ‘all patients deemed suitable must be offered laparoscopic surgery even if this means onward referral to a suitably qualified surgeon’. This decision transformed the practice of colorectal cancer surgery and was enabled by the LAPCO and similar laparoscopic training programmes (see above).
The rise of the robots
In the mid-1980s, neurosurgeons began to use robots for stereotactic procedures such as biopsies. 12 Around this time, many individuals and organisations were trying to apply robotic techniques to various types of surgery. In 1992, the first robotic-assisted hip replacement was performed in Sutter General Hospital Sacramento using the ROBODOC system that had been developed by Bargar and Paul 13 Ten patients were included in the first cohort and a randomised clinical trial was subsequently conducted (from 1994 to 1998) including 136 consecutive patients undergoing primary cementless hip arthroplasty at one of three centres. This trial showed improved fit, fill and alignment of the prosthesis in the robotic group, but no difference in the Harris Hip Scores at two years. Operating time was also longer in the ROBODOC group.14,15
In 1997, the world’s first robotic cholecystectomy was performed by Guy-Bernard Cadière and Jacques Himpens in Brussels.16,17 Despite this ground-breaking event, its report was rejected by both The Lancet and the New England Journal of Medicine as it was considered ‘inappropriate’ or ‘very unlikely to have actually happened’ and so it was reported by means of a letter to the editor in Surgical Endoscopy in 1998. Himpens and Cadière went on to perform the first robotic bariatric procedure (gastric banding) later in 1998. 18
In 2000, the U.S. Food and Drug Administration approved the first robotic surgical system, the Da Vinci robot (Intuitive Surgical). The Da Vinci robot at St Mary’s Hospital in London even had a starring role in the James Bond film, Die Another Day (Figure 1).
19
There are several theoretical advantages of robotic surgery compared to laparoscopic surgery. These include magnified three-dimensional view, better ergonomics, a stable operating platform, the ability to operate at a distance and camera control by the operator. However, the most important advantage is the increased degrees of freedom of the instrumentation such that it more closely resembles movement of the human hand and wrist rather than the three up/down, back/forth and right/left movements of conventional laparoscopic instruments (Figure 2). There are, of course, disadvantages to robotic surgery and these include the large robotic arm with a limited range of motion, the lack of tactile sensation, poor moveability of the surgical cart, longer operating times and expense. Furthermore, the operating table is locked when the robot is docked, leading to delay in access to the patient and conversion to open surgery in the event of haemorrhage or other surgical emergency.
Da Vinci robot drawing blood from James Bond in the film Die Another Day (2002).19 For Video see www.youtube.com/watch?v=oXn7TyI1VEk. Illustration of robotic grasper with multiple degrees of freedom of movement mimicking human wrist mobility.

During the late 1990s and early 2000s, the number, range and publication of robotic procedures increased exponentially, such that there was barely a field of surgery where robotic operations were not attempted. This period coincided with rapid developments in optics, instrumentation and other technical advances along with the rise, fall and merger of companies developing this technology. 20 There have been conflicts of interests relating to the financial incentives and professional kudos associated with institutions offering robotic procedures which led to enthusiasm for this technique in the absence of evidence that it conferred any advantage to patients.
Initially, bariatric 21 and cardiothoracic surgery were the two specialties that embraced robotic surgery with great enthusiasm. However, other forms of minimal access surgery have proven to be just as effective (and cheaper and easier) in most cases, such that robotic procedures are the minority in these specialties now.
Robotic prostatectomy appears to be the operation for which there is currently most evidence of improved outcomes compared to either open or laparoscopic procedures. 22 This trial showed reduced blood loss, shorter duration of catheterisation, fewer positive margins, earlier return of continence and erectile function, and shorter length of hospital stay in the robot group compared to those undergoing open prostatectomy. In the last decade, multiple trials of robotic prostatectomy have been undertaken. A review performed by Allan and Ilic 23 concluded that robotic procedures offer advantages in short-term outcomes such as length of hospital stay and reduced blood loss along with preservation of erectile function, while oncologic outcomes and survival are similar to those for open procedures. Prostatectomy is a technically challenging operation to perform laparoscopically because of the requirement to suture an anastomosis between bladder and urethra in the depths of the pelvis. This is facilitated by robotic access, magnification and the increased mobility of wrist-like instruments.
Robotic colorectal surgery has been taken up by enthusiasts worldwide. However, in contrast to the findings for prostatectomy, it has been much harder to demonstrate significant advantages for robotic colorectal surgery. It was thought that anterior resection would be an analogous operation to prostatectomy where the issues of nerve preservation may be similar. Two systematic reviews on the use of robotic surgery for rectal cancer were published in 2014.24,25 These papers covered studies published between 2002 and 2014 during which time technology was improving and they included multiple papers from the same institutions with overlapping data collection periods, variable endpoints and small and non-randomised trials. However, the conclusions were that robotic surgery was associated with reduced conversion rates, slightly longer operative times and shorter length of hospital stay compared to laparoscopic rectal cancer surgery, while there was no significant difference in circumferential resection margin positivity, lymph node harvest, local recurrence or three-year disease-free survival. The ROLARR (Robot versus Laparoscopic Resection for Rectal Cancer) trial was a multicentre international randomised controlled trial comparing robotic versus laparoscopic operations for resection of rectal cancer. There were over 200 patients in each arm across Europe, North America and Asia and there was no significant difference in the conversion rate to open surgery (primary outcome) nor in oncologic outcomes such as circumferential resection margin positivity and local recurrence rates, nor in functional outcomes such as sexual and urinary function (secondary outcomes). 26
One of the problems in advancing the field of robotic surgery has been the cost of the robotic platforms and accompanying instruments, training requirements and service contracts. This has made it prohibitively expensive for many countries to contemplate using such technology and, even within relatively wealthy counties such as the UK, there is widespread variation in the availability of robotic prostatectomy, let alone procedures where the benefit is more nuanced. The last five years have seen a number of new companies and collaborative enterprises enter the market for developing robotic platforms and it is likely that competition will allow prices to fall and availability to expand.
Current status of minimal access surgery
All branches of surgery have benefited from the advances in minimal access surgery that have been made in recent years. Each specialty has achieved a good degree of consensus about the indications for, and limitations of, minimal access techniques for different procedures. Training programmes are now mandatory in most specialties and mentoring and proctorship are widely available. Surgical oncology specialties often have mandatory audits and these may include the proportion and type of cases undertaken via laparoscopic or other minimal access approaches. Figure 3 shows the trends in the proportion of colorectal cases in the UK undertaken laparoscopically between 2008 and 2017 (reported 2010–2019) in the National Bowel Cancer Audit Project.
27
The proportion of cases completed laparoscopically rose from approximately 25% in 2008–2009 to 61% in the most recent audit period (2017–2018).
Trends in proportion of laparoscopic colorectal cancer resections in the UK – taken from National Bowel Cancer Audit Project reports 2010–2019.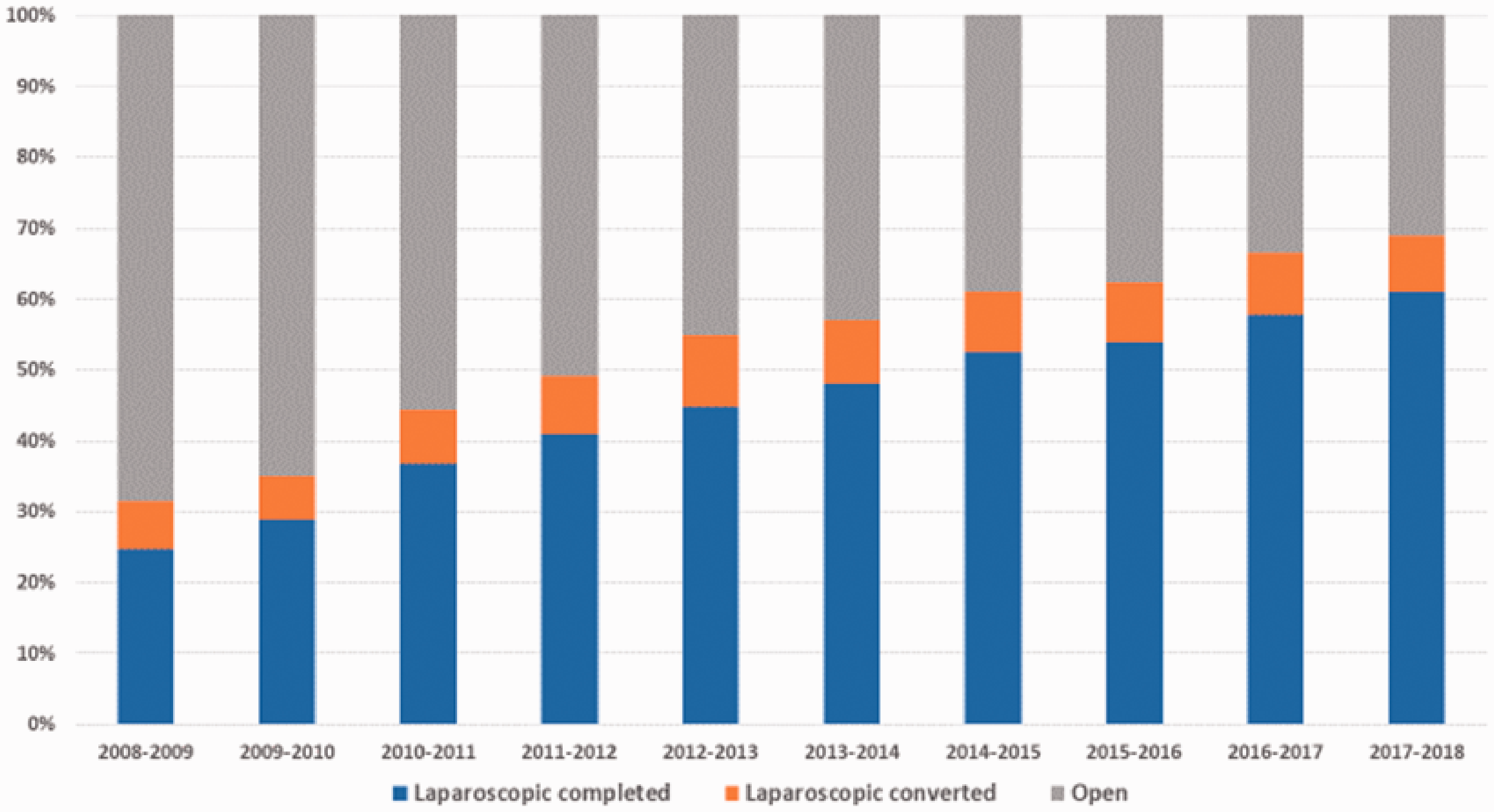
Single-incision laparoscopic surgery has been proposed as a way of improving cosmesis and avoiding port site complications such as hernia in abdominal laparoscopic surgery. A single multiport channel is inserted just below the umbilicus (Figure 4) but due to the reduced mobility of single-incision laparoscopic surgery instruments, it has limitations in its applicability. It may have a role in appendicectomy, division of adhesions and exploratory laparoscopy and biopsy, but more extensive colonic or gastric resections are very awkward, with reduced visibility and access and prolonged operating times. The cosmetic gains are marginal and the length of stay in major cases is rarely related to port site problems.
Single-incision laparoscopic surgery port and instruments.
Natural orifice transluminal endoscopic surgery is another area of minimal access surgery that has yet to find its place in the repertoire of most practising surgeons. Although Ott had reported the first natural orifice transluminal endoscopic surgery procedure, transvaginal appendicectomy, in the early 1900s, 28 natural orifice transluminal endoscopic surgery did not take off until almost a century later. Improvement in flexible endoscopes allowed free-thinking surgeons, gynaecologists and gastroenterologists to undertake operations such as appendicectomy, removal of ovarian cyst or cholecystectomy by using an endoscope via the mouth, rectum or vagina. The advantage of natural orifice transluminal endoscopic surgery is that there is no surface wound or scar, but the disadvantages include technical difficulties, prolonged operating time and the risk of sepsis.
Robotic surgery has become established for significant numbers of patients with prostate cancer in high-income countries and is finding its niche for rectal cancer and bariatric surgery. Its role in other branches of surgical oncology is still subject to clinical trials, but improved ability of training, a generation of surgeons who are already experienced in laparoscopic skills and a reduction in cost due to new commercial opportunities may all allow this area of minimal access surgery to flourish in the near future.
Conclusion
For over 5000 years, doctors and scientists have advanced the practice of minimal access surgery. Techniques have developed from simple wood and metal tubes that opened natural orifices to allow in natural light for vision, to complex electronic and robotic systems that allow access to every part of the body for both diagnosis and intervention. However, the basic principles of anatomical identification, illumination and assessment of pathology, therapeutic intervention, training of younger members of the profession and meticulous record keeping have been established for millennia and are equally applicable today.
In 1902, George Santayana was reported as saying ‘Those who cannot remember the past are condemned to repeat it’ and similar statements have been made by, among others, Winston Churchill. It is important that the current generation of surgeons does not repeat the mistakes of our predecessors with respect to conflicts of interest for financial gain or professional advancement, nor to expose our patients to unnecessary risks in the pursuit of new technology and innovation. 9 The litany of bile duct damage from over-enthusiastic uptake of laparoscopic cholecystectomy 30 years ago, and more recently the iatrogenic consequences of pelvic floor mesh insertion, should serve as salutary reminders of what can go wrong when the profession forgets its primary duty – First do no harm (ὠϕɛλέɛιν ή μή βλάπτɛιν). 29