
Abstract

Introduction
Patient and public involvement is an active partnership between patients, the public and researchers in the research process. 1 Patients and the public offer unique insights from their lived experiences which cannot be substituted by expert knowledge from clinicians, researchers or other specialist stakeholders. These insights are important to ensure research is relevant and high quality. 2 Furthermore, the public have a right to be involved in research which may affect them and, often, is publicly funded. 3 The active partnership distinguishes involvement activities from patient and public engagement which is the sharing of research, such as science festivals or newsletter articles, and people as ‘subjects’ or participants in research. 1
There has been an international drive to promote and raise the profile of patient public involvement in research and for patient public involvement to change how research is designed and conducted.4,5 Recently, an international network for patient public involvement in health and social care research was established which aims to promote and advance patient public involvement through a global partnership. 6 Major funders of healthcare research increasingly expect evidence of comprehensive, meaningful patient public involvement in the development of grant applications and planned patient public involvement within the proposed project.4,5 For example, in the United Kingdom, the National Institute for Health Research have patient public involvement policies within their research and grant committees and fund INVOLVE, a national advisory group to advance patient public involvement.4,7 Similarly, in the United States, the Patient Centred Outcomes Research Institute promotes patient input to guide research questions and supports active involvement from patients in reviewing applications, sitting on advisory committees and providing feedback on policy documents. 5 Funder requirements and expectations have been important drivers for the increase in number of research studies involving patient partners in the planning and delivery of research. 2
Research strategy and infrastructure
Embedding patient and public involvement in an academic research centre.
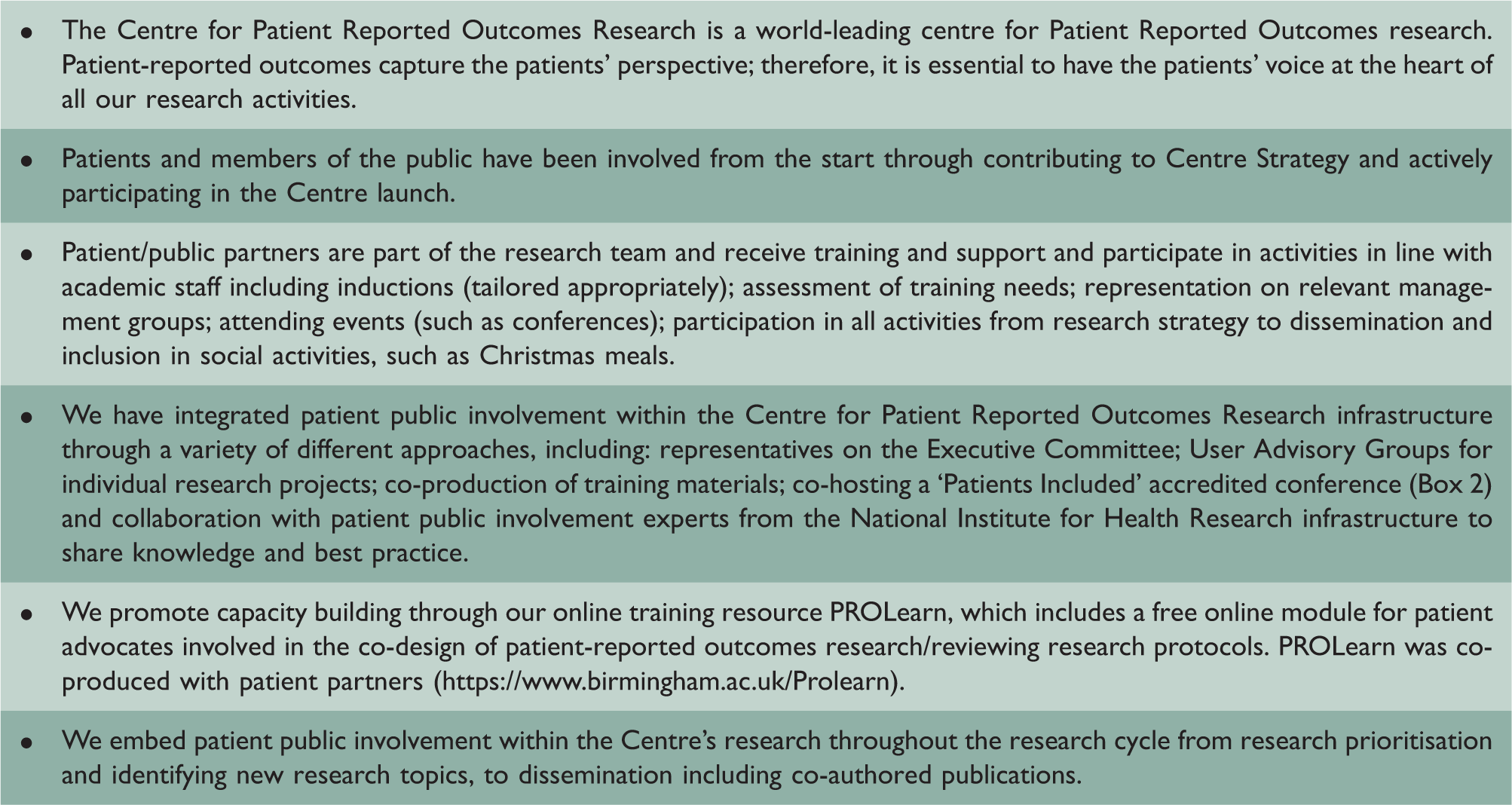
Benefits of an organisational level approach
Embedding patient public involvement at an organisational level facilitates opportunities for shared learning across different projects and accelerated skill development, for both patient partners and academic researchers. Developing connections with patient public involvement experts, such as patient public involvement leads, within the organisation and wider research infrastructures, enables direct access to advice and guidance, and facilitates sharing of best practice and knowledge, such as the latest guidance and standards. In turn, organisations may develop their own standards for patient public involvement based on their growing experience and expertise which enhances the conduct of future patient public involvement activities and creates continuity for long-term patient partners.
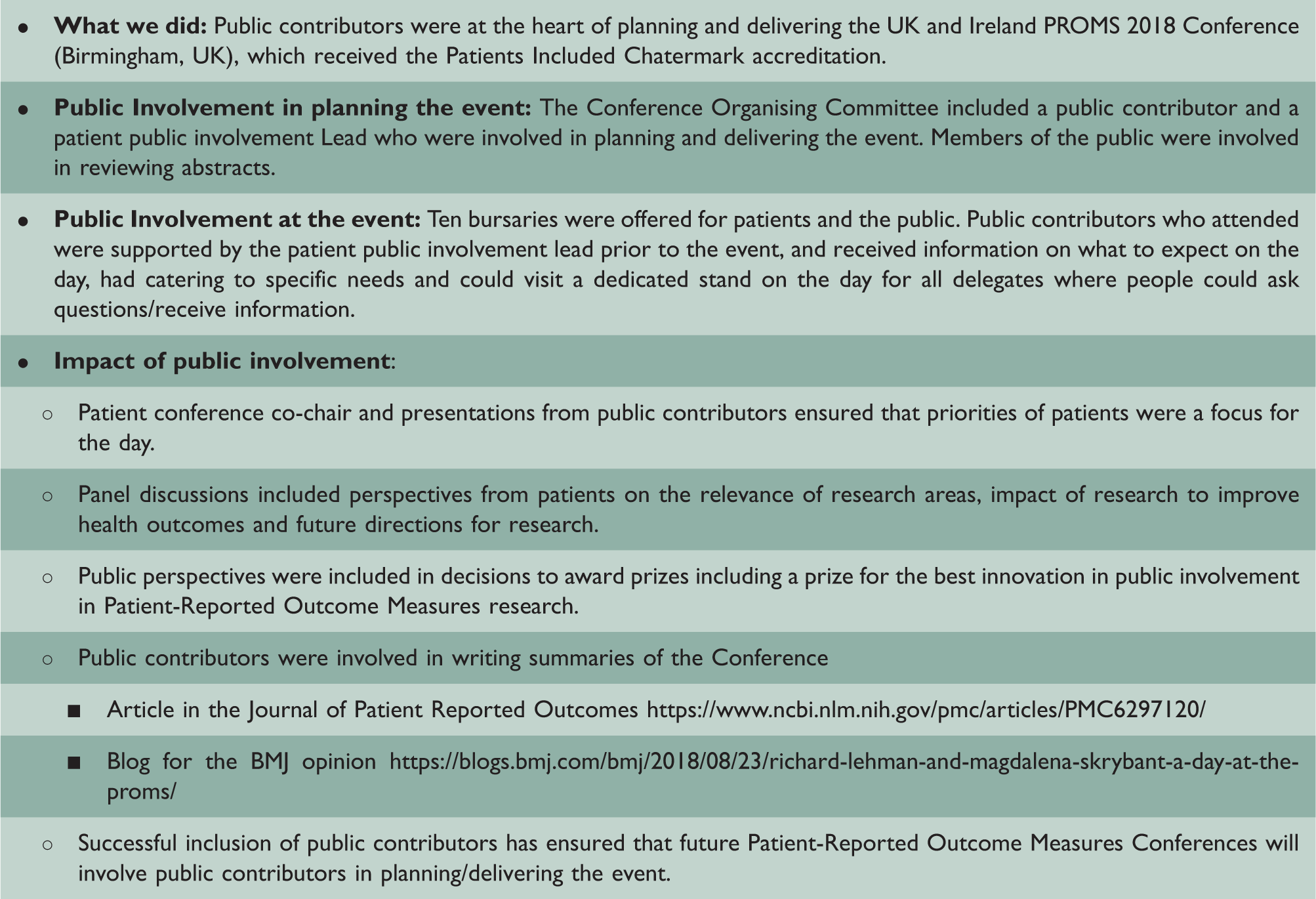
Patients Included accredited conference.
Thinking outside the box – innovative patient partner collaborations.

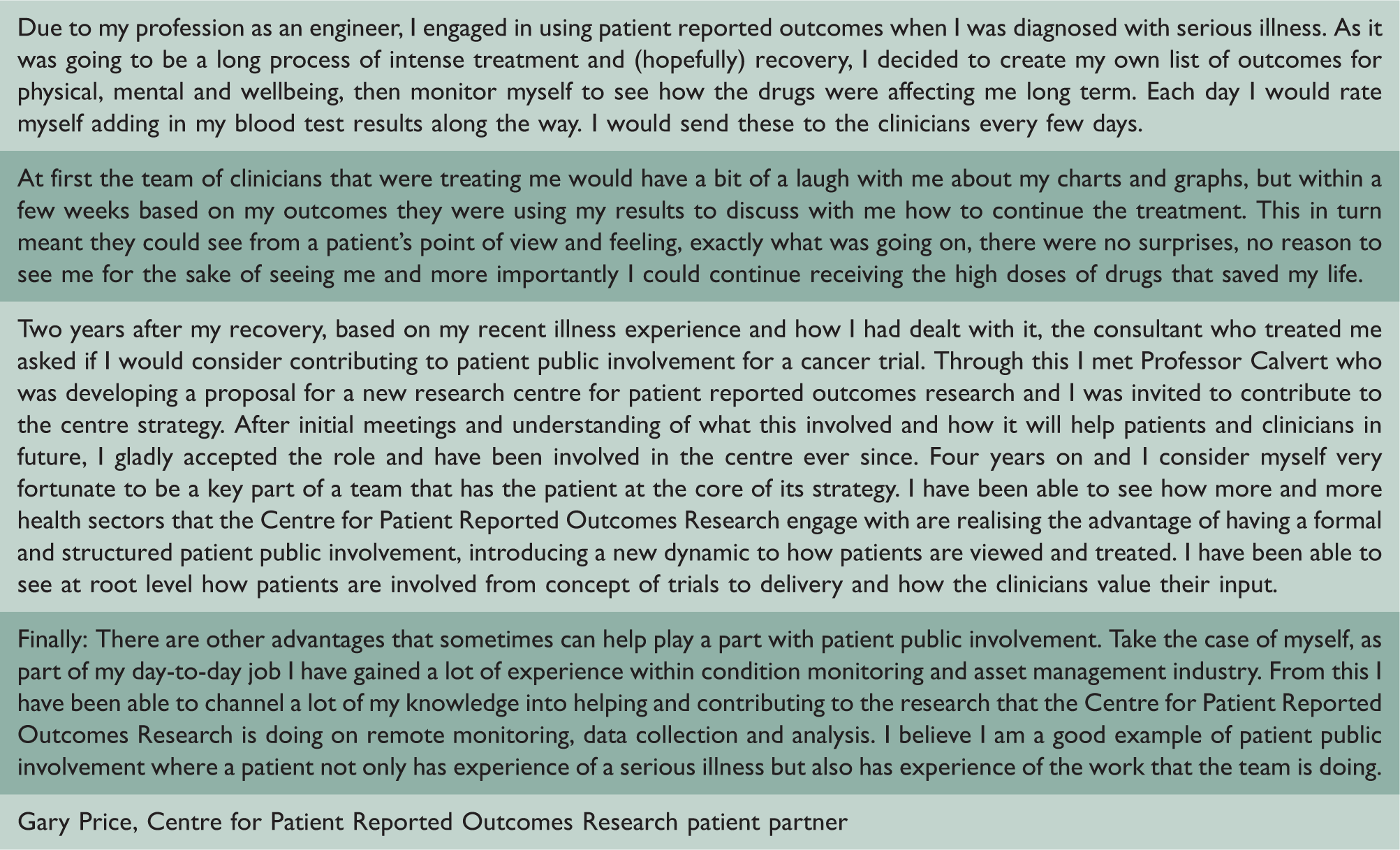
Experience of patient and public involvement from Centre for Patient Reported Outcomes Research patient partner Gary Price.
Challenges and facilitators
Tips for successful partnerships.

In the past, clinical research was often based on research objectives and agendas of clinicians and researchers. The studies were mostly designed, conducted and disseminated by clinicians and researchers with little or no input from patients or the general public. 2 One of the issues with this traditional approach was that such objectives and outcomes may not match those prioritised highly by patients who are supposed to benefit from research studies, thus potentially limiting the usefulness and impact of research findings. 2 Patient and public involvement provides the opportunity for patients, their families, carers and the general public to become co-members of the research team, participate and contribute to research alongside clinicians and researchers. Widening involvement in research this way, particularly to include under-represented voices from minority and hard to reach communities, is a well-recognised challenge. 2 Embedding patient public involvement at an organisational level has potential to accentuate a lack of diversity as the nature of organisation level activities may unintentionally create bias in recruitment of patient partners. For example, attending an organisation’s executive committee meeting may not be possible for public contributors with work/carer responsibilities and individuals from low socioeconomic backgrounds may find these meetings intimidating. Therefore, it is important that organisations are aware of these risks and take steps to actively address diversity. These may involve: developing relationships with local communities; widely advertising involvement opportunities; provision of additional training and support for public contributors and ensuring chairs of meetings have the skills to involve public contributors in discussions and decision-making. 10 In addition, it is important to have varied, flexible opportunities for involvement (beyond formal meeting) and ability to adapt to people’s changing circumstances and changes how much they want to contribute.
Although the proposed embedded model of patient public involvement suggests all team members are actively engaged in patient public involvement, having a person(s) who co-ordinates and is responsible for patient public involvement can be beneficial to drive patient public involvement initiatives, maintain momentum, monitor involvement strategies and outcomes, and be a named point of contact. 2 However, there is a danger that research teams become reliant on the patient public involvement lead which may hinder team engagement with patient public involvement and shared learning. 2 Ongoing, regular communication with public contributors, both formal and informal contact, is critical for building and sustaining relationships. 12
Support from senior leadership is important to promote a culture of patient public involvement as standard practice and to ensure organisations have a public involvement strategy. Cultural changes are required to embed patient public involvement at an organisational level and to create an environment where patient public involvement is valued by researchers and viewed as the norm rather than an added extra. 9 Involving patient partners in research should be done instinctively by all team members and patient partners should be regarded as integral members of the research team (Box 1).
Measuring the impact of patient and public involvement
Patient public involvement has the potential to positively impact on research at multiple levels, promoting quality and relevance of research and benefitting the wider research system. 11 Impact should be assessed by measuring pre-determined key performance indicators linked to research outcomes and processes 14 through qualitative and/or quantitative methods. 3 Individual level performance indicators could include acquisition of new skills and knowledge for the patient public involvement contributors and better understanding of the research field from a patient perspective for the research team. 11 Research quality indicators could include patient public involvement in research prioritisation, 15 contributions to research design and methods, 16 collaborations on grant applications17,18 and dissemination of findings via co-authorship on publications and presentations at conferences. 3 Wider research system impact could be measured by assessing influence on advocacy and accountability in terms of the allocation of research resources. 14
There is drive to capture key performance indicators for individual research projects; however, it is also important to document these indicators at an organisational level and think beyond project-specific objectives. The use of the Guidance for reporting patient and public involvement version 2 checklist 13 to report patient public involvement activities and utilisation of the newly developed Cost and Consequences Framework 19 may enhance transparency and accuracy in the reporting of positive and negative impacts. Furthermore, consideration should be given to capturing ‘soft’ outcomes, such as relationship building, which are often more difficult to measure.
Conclusion
There is a need to move away from patients and the public only being involved in individual research projects and move towards models where patient public involvement is considered at an organisational level and patient partners are valued team members. This approach has potential to promote relationship building, generate more sustainable, efficient patient public involvement practices and accelerate development of skills and expertise for patient partners, researchers and other stakeholder collaborators. However, it requires adequate resourcing, co-ordination and cultural change.
Key messages
Patient and public involvement in research is predominantly focused at the level of individual research studies; however, a move toward patient public involvement being embedded within the wider infrastructure of the organisation may maximise benefits for all involved. This approach has potential to promote relationship building, generate more sustainable, efficient patient public involvement practices and accelerate development of skills and expertise for patient partners, researchers and other stakeholder collaborators. Organisational level patient public involvement requires adequate resourcing, co-ordination and cultural change.
Patient involvement
Patient partner, Gary Price, has significantly contributed to this paper and is a co-author. Price has been actively involved in planning the content and structure of the manuscript, wrote a reflection of his patient public involvement experiences (Box 4) and has reviewed drafts of the manuscript. Magdalena Skrybant has a wealth of experience working with public contributors and has represented their voices during the planning and writing of the manuscript.
Footnotes
Declarations
Funding
GT is funded by a National Institute for Health Research Postdoctoral Fellowship Award. OLA is funded by the Health Foundation, an independent charity committed to bringing about better health and healthcare for people in the United Kingdom. He also receives funding from the National Institute for Health Research Birmingham Biomedical Research Centre. MC is funded by National Institute for Health Research Biomedical Research Centre, National Institute for Health Research Applied Research Centre West Midlands, the National Institute for Health Research Surgical Reconstruction and Microbiology Research Centre at the University Hospitals Birmingham National Health Service Foundation Trust, the University of Birmingham, Health Data Research UK, Innovate UK and Macmillan Cancer Support. MS is funded by National Institute for Health Research Applied Research Centre West Midlands. This paper presents independent research and the views expressed are those of the author(s) and not necessarily those of the organisations mentioned above. This research is supported by the National Institute for Health Research Applied Research Centre West Midlands.
Guarantor
MC.
Ethics approval
Not required
Contributorship
GT and OLA drafted the initial manuscript. All the authors reviewed, revised and approved the final manuscript.
Acknowledgements
The authors thank ERIKs European Technology Centre, Rotterdam, Netherlands, for hosting them during their industry visit.
Provenance
Not commissioned; peer-reviewed by Eugene Yeung.