
Abstract

This is the ninth article in our series on population healthcare
It has been said that the NHS is overeducated and undertrained. What is meant by this is that we spend a very large amount of money educating people at the beginning of their careers but relatively small amounts of money for the next 40 years. But it is more than this. It is not just the balance between initial investment and continuing investment – it is the nature of that investment. There is an important distinction between education and training.
Education helps people learn how to think, how to grow and develop and how to analyse problems, and it is therefore vitally important for everyone working in the most complex business on earth – namely healthcare. Training is a different function: it gives people the skills, concepts and sometimes behaviours needed to carry out a particular task or a policy. The epitome of an organisation that focuses on training as well as education is the military, encompassing all three of the services. They expect people to be well educated, but when a new policy or technology is introduced, everyone has to go for training, and that means everyone. The same applies in industry, and people who have met pharma industry staff will know that when a new drug is introduced everyone must go on the training course to learn about the new drug, not just those who will be directly involved. The importance of this is reinforced by the behaviour of senior management in industry. If someone does not attend the training because they are high up in the leadership team and does not see what a new drug has to do with them, then they will probably be reported to the chief executive; they will possibly have their pay affected and they will certainly be seen as someone who is not ‘one of us’ and therefore would be on their way out of the company.
In the military, new technology as well as new concepts stimulate the need for training. There is no way that the military would have sought to do something like commissioning without a comprehensive plan for training everyone who needed to know, and that means everyone. They would have included every clinician involved in commissioning, even the GPs only working one or two sessions a week, as well as everyone above a certain grade in the commissioning organisation. The training would be accompanied by the introduction of a new doctrine and people would have to learn the new doctrine, namely the meaning of the new concepts and they would probably practise the new skills before returning to their units.
Simulation has been adopted now in the clinical arena, for example as a means of improving patient safety, but we surely have just as great a need in management, policy and commissioning. How else can people learn to apply the skills they have been taught and to find out how their colleagues would operate under pressure. In a typical organisation responsible for commissioning and managing resources, some people are at the utilitarian end of the spectrum; others see themselves as champions of people with uncommon and rare conditions; and yet others might position themselves in the middle of the road, but are these different perspectives every admitted, discussed or harmonised? Very rarely.
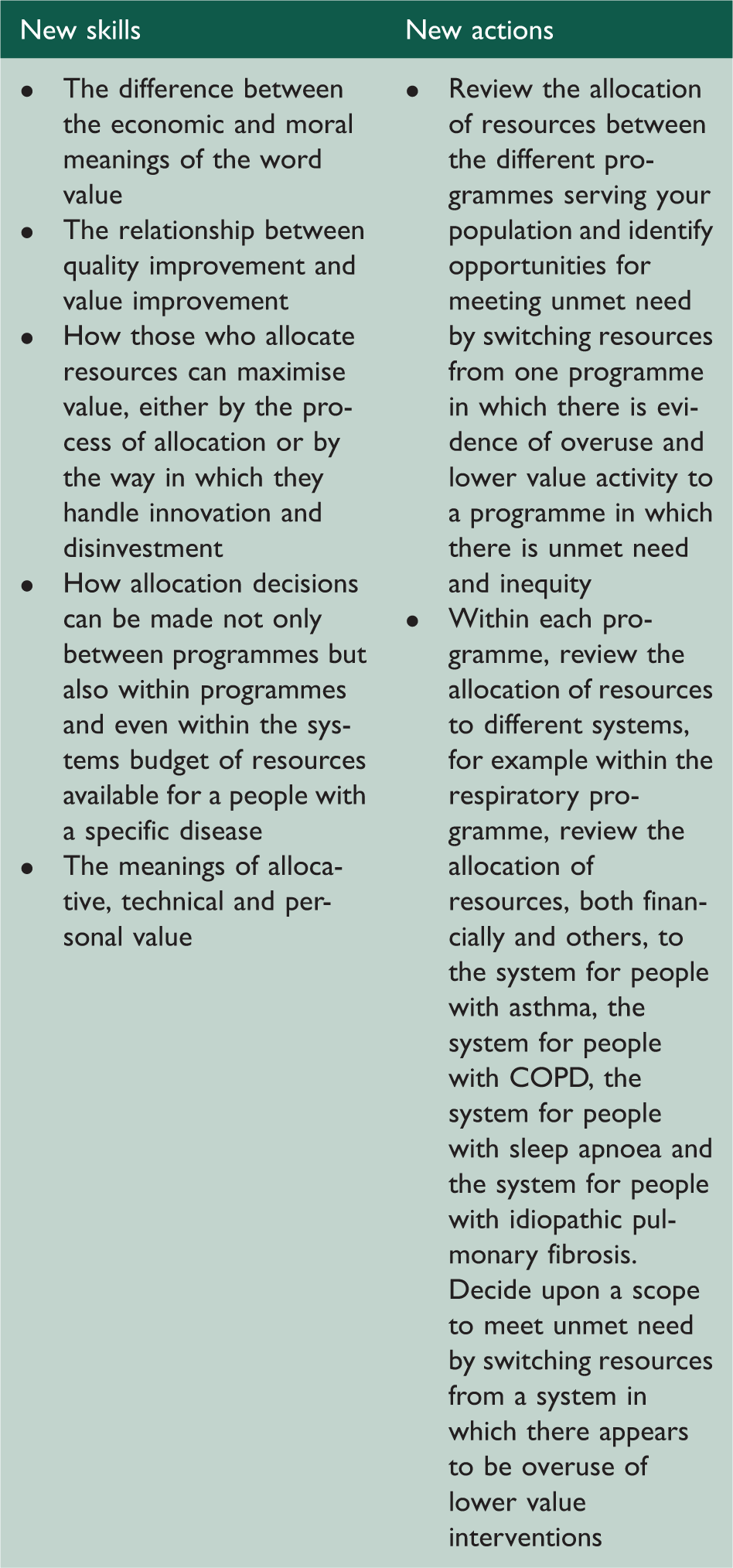
In developing population healthcare, we need excellent leadership but we also need training. Set out below are the ten skills and domains that are needed for each of the skills which are required and, a key principle, the actions of people being expected to carry out once they have had their training focused on the three new tasks:
Increasing personal value by ensuring that by providing people with full information about the risks and benefits of the intervention being offered; Increasing value for the population by shifting resource from budgets where there is evidence of overuse or lower value to budgets for populations in which there is evidence of underuse and inequity; Increasing value for the population of developing population-based systems that:
address the needs of all the people in need, with the specialist service seeing those who would benefit most; increase rates of higher value intervention (underuse) funded by reduced spending on lower value intervention (overuse), e.g. shift resources from treatment to prevention or polypharmacy to district nursing; implement high value innovation (underuse) funded by reduced spending on lower value intervention (overuse).
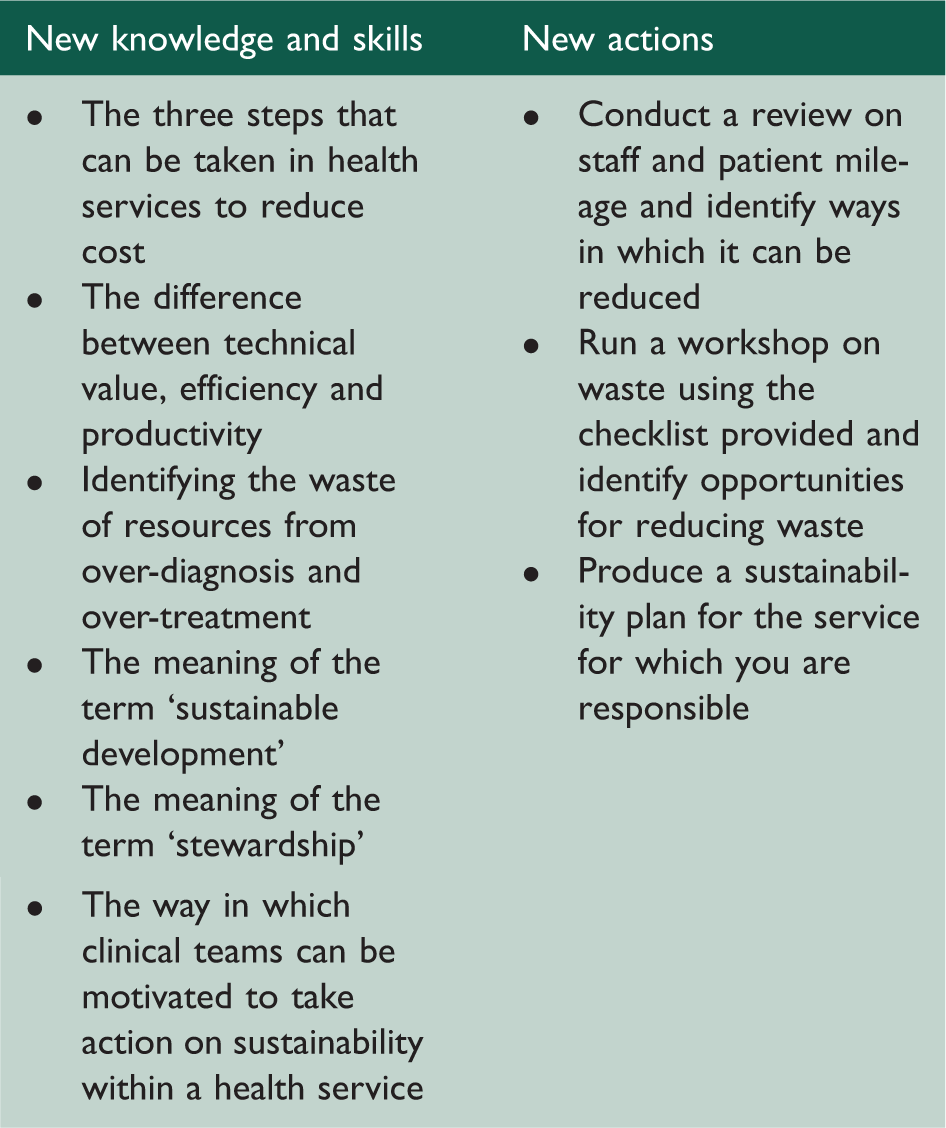
Sustainability
The term sustainability can be considered a narrow definition focused on environmental sustainability or the carbon footprint of the NHS, although this is not enough to form a major topic for debate. The term sustainability also has implications of the future. The leadership team needs to understand these issues and decide which definitions of sustainability it wishes to use.
The concept of stewardship is related and a shorter definition of stewardship is shown below:
‘Stewardship is to hold something in trust for another.’
It is not inappropriate to encourage staff to think about sustainability in the environmental sense because many frontline staff are not motivated by the fact that their organisation is in financial difficulty, whereas many are motivated by thinking about waste in an environmental context and taking action to reduce the carbon footprint for the service which will also have financial benefits.
Ten skills
Achieving triple value
COPD: chronic obstructive pulmonary disease.
Minimising waste and increasing sustainability
As we have emphasized it is often appropriate to engage staff in discussion about the carbon footprint when an organization is in financial difficulty because it will motivate some staff who are on different about financial problems. Reducing the carbon footprint often reduces financial cost also. The term sustainability is also important to use in both the sense of ensuring the sustainability of the NHS and the sustainability of our life on earth and examples of the broader definition are given below the integration of environmental, social, political and economic considerations and impacts within decision-making. It also includes notions of social justice and equity. Plans and decisions should meet the needs of the present without compromising the ability of future generations to meet their needs
2
.
Living on the earth’s income rather than eroding its capital. It means keeping the consumption of renewable resources within the limits of their replenishment. It means handling down to successive generations not only man-made wealth but also natural wealth, such as clean and adequate water supplies, good arable land, a wealth of wildlife and ample forests.
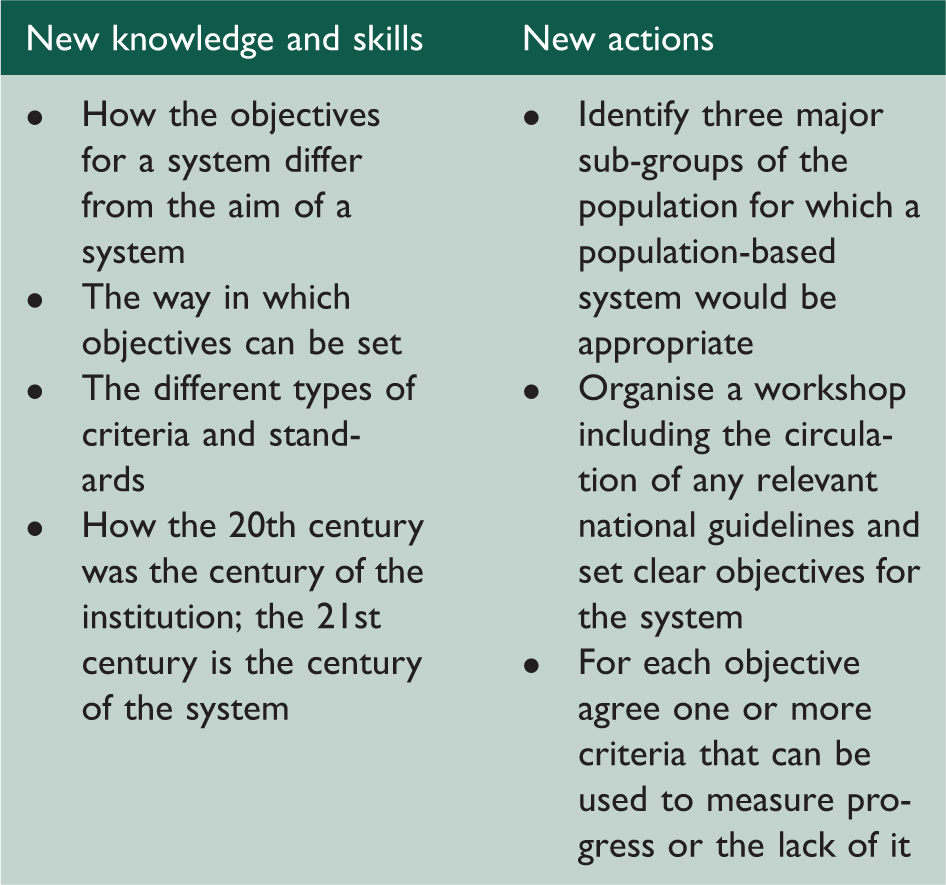
Designing and delivering population healthcare
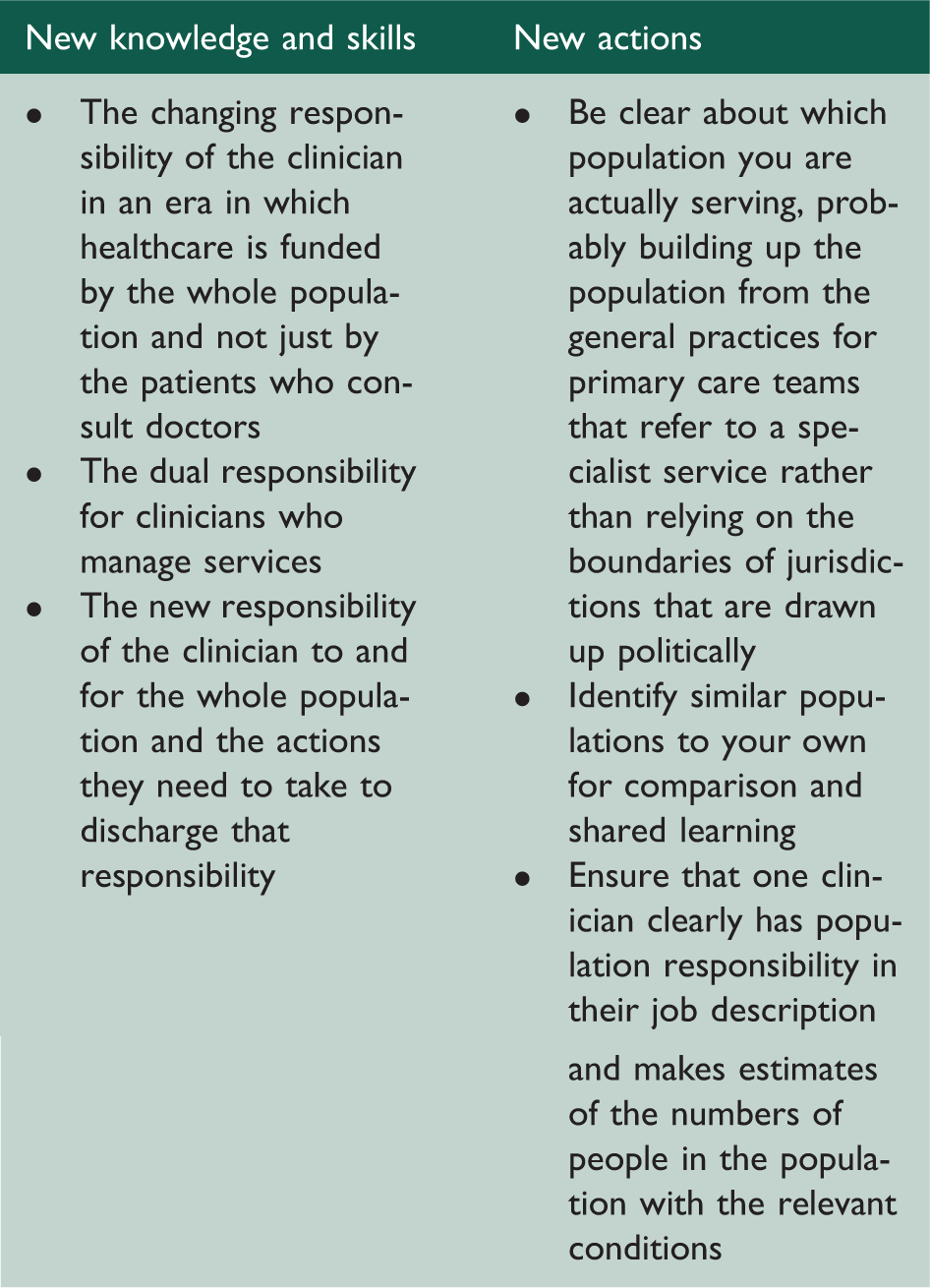
Developing population-based systems
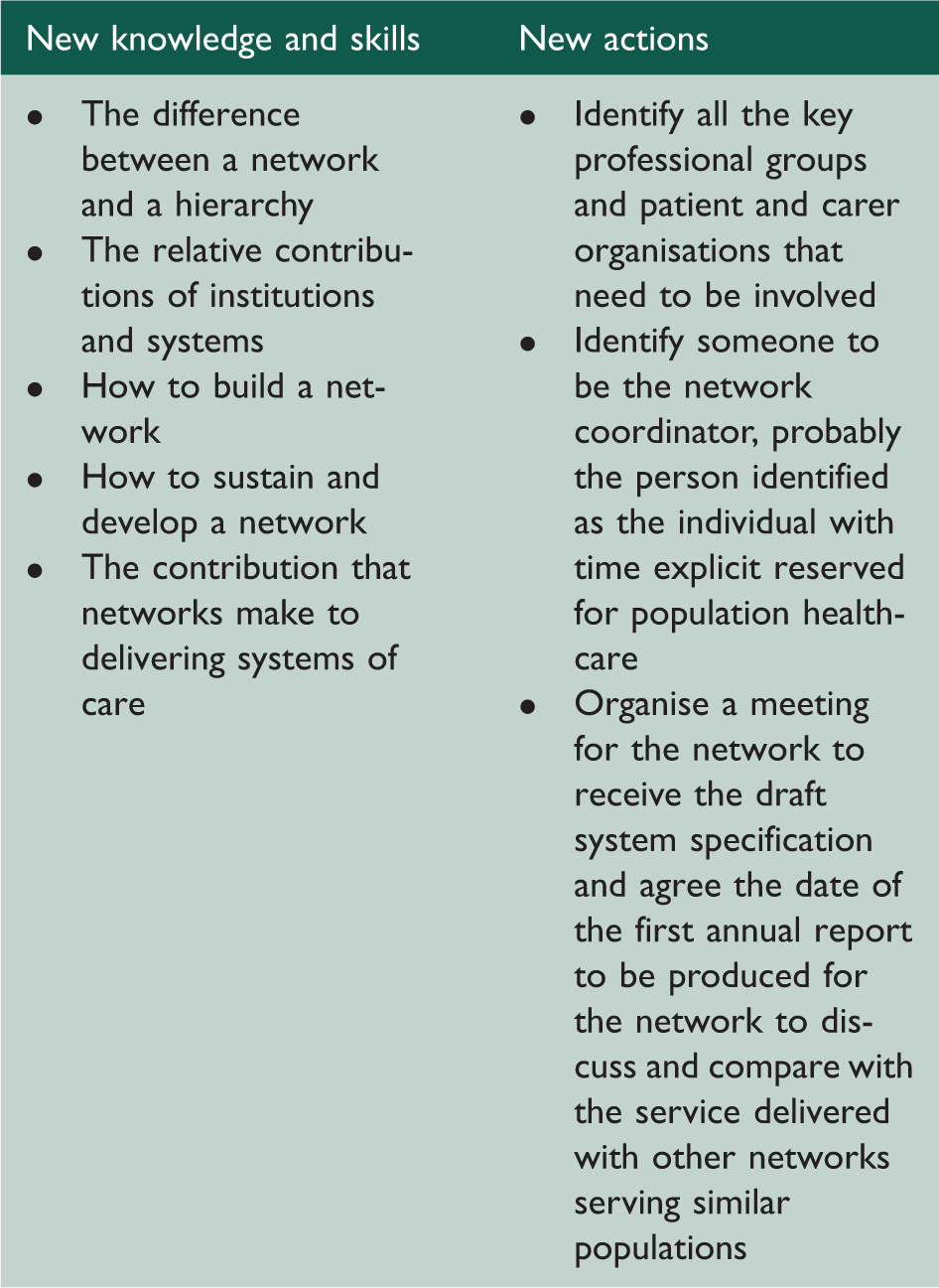
Creating and leading networks
A network is a set of organisations that deliver the systems. There is a glowing literature about working in networks, for example a book on connectedness by Nicholas Christakis and James Fowler is helpful and the key text suggests that: Social networks also have a memory of their own structure (staying intact even if people come and go) and their own function (preserving a culture even when people come and go). For example, if you join a trusting network of people, you benefit from that trust and are shaped by it. In many cases, it is not just that the people in your network are more trusting, or even that their trusting behaviour engenders trust in you; rather, the network facilitates this trust and changes the way individuals behave.
4
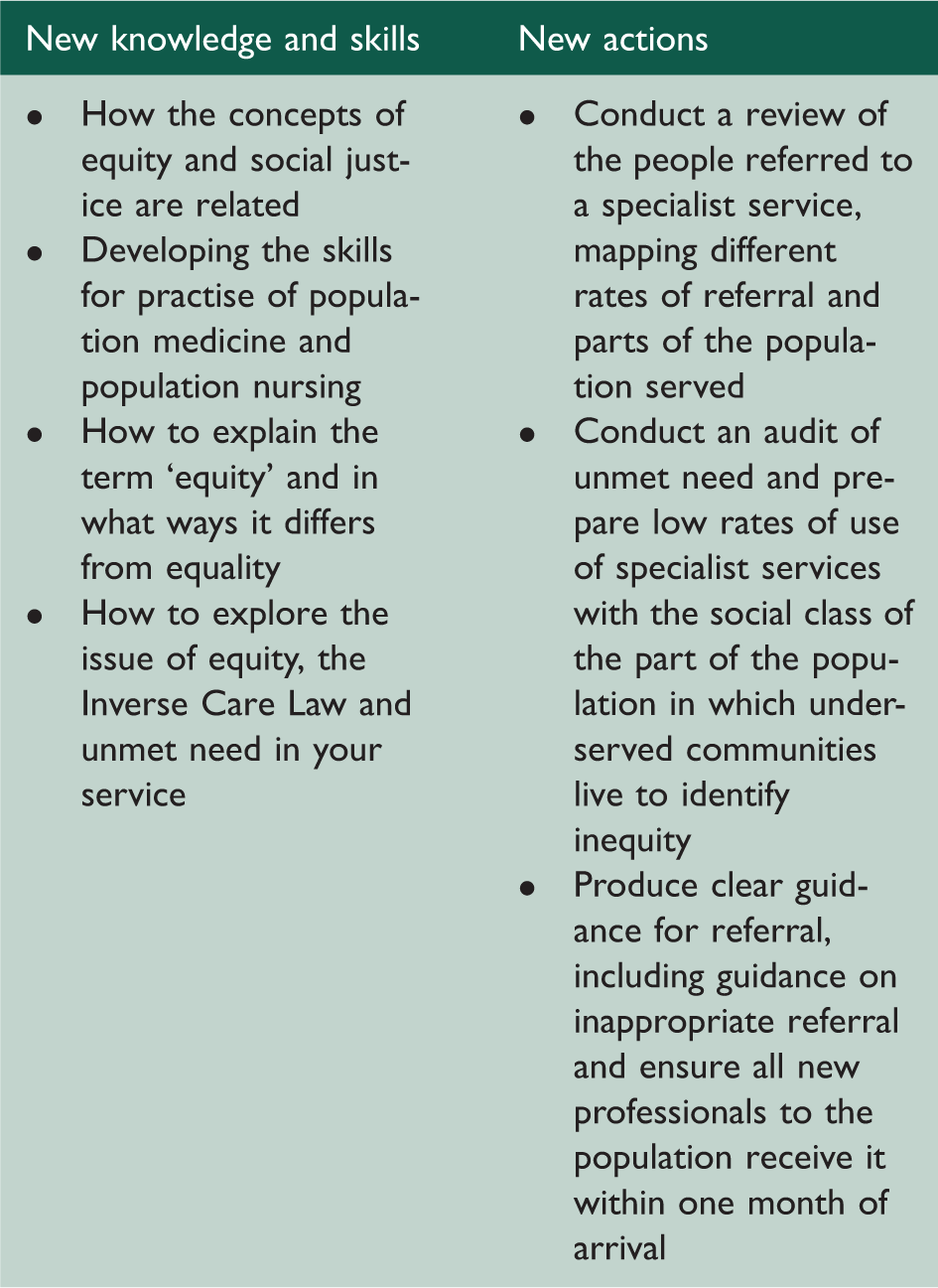
Seeing the right patients and mitigating inequity
Inequity is different from inequality. For example, there is inequality in the allocation of resources because people with severe health problems receive more healthcare and use more resources than people with mild self-limiting health problems. The allocation of resources is unequal, although it uses an example of inequity.
Inequity has concepts of unfairness. The inverse care law was invented by Julian Tudor Hart and he pointed out that often the amount and quality and care provided was inadvertently related to the need in the population served.
It is useful to consider four dimensions of inequity in training:
Inequity related to age: is there under-treatment of older people? Gender: are there treatments which women are not given, although there is evidence that they benefit just as much as men? Social class: best identified by relating referral patterns to the deprivation measures of the ward being served; Ethnic group: are there culture or linguistic problems that mean there are certain ethical groups who are not receiving care in a way that is unfair?
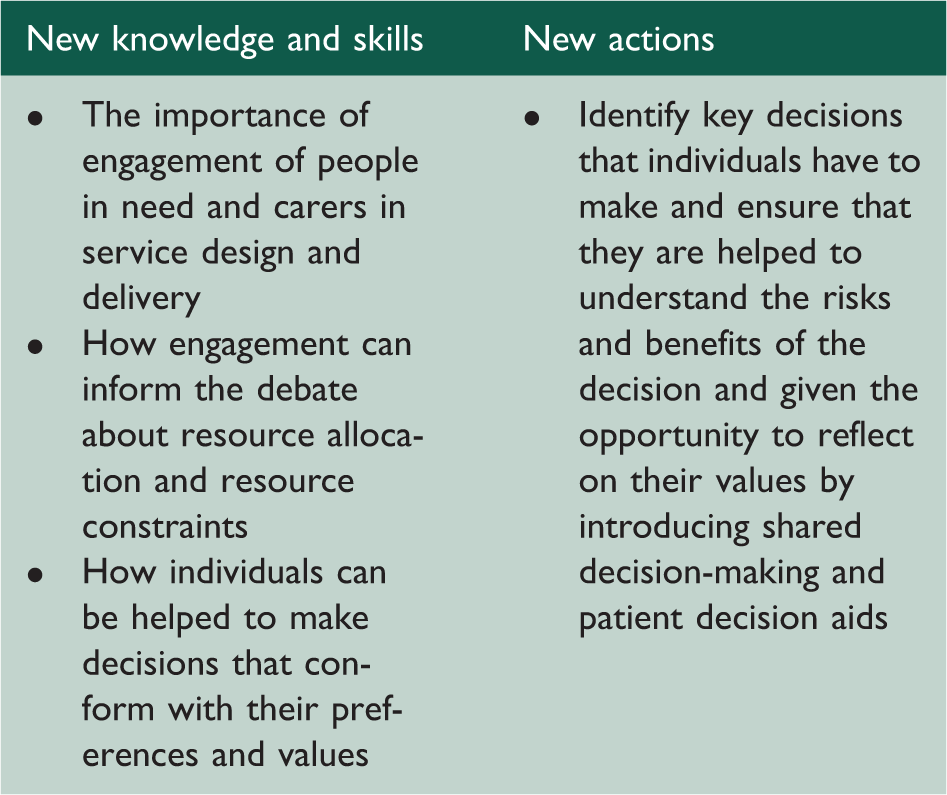
Engaging people in need
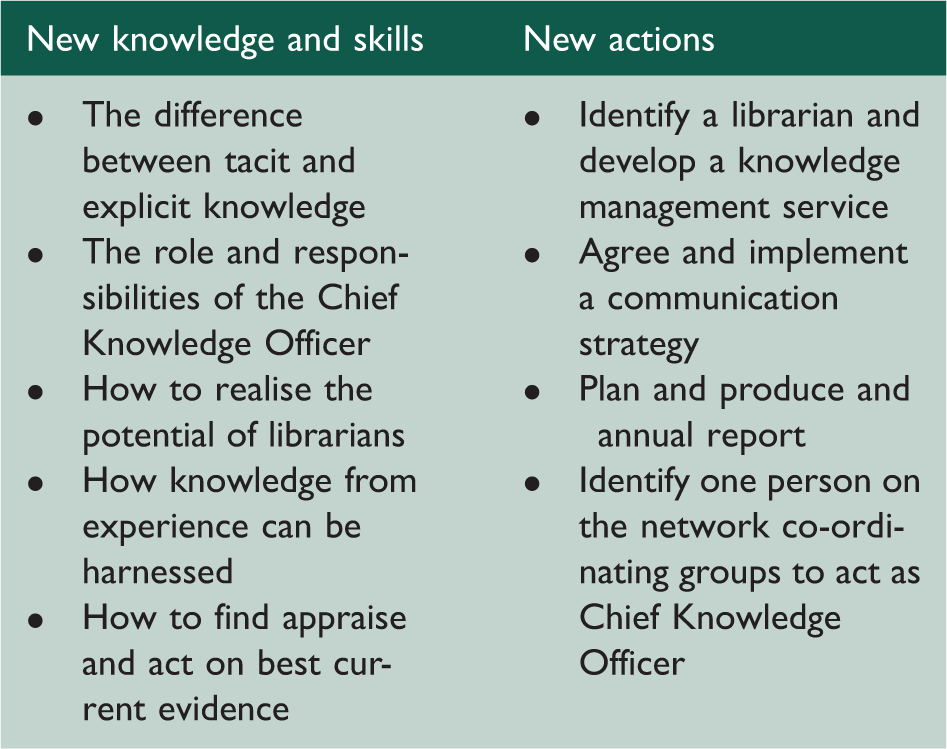
Managing knowledge
Promoting health and preventing disease
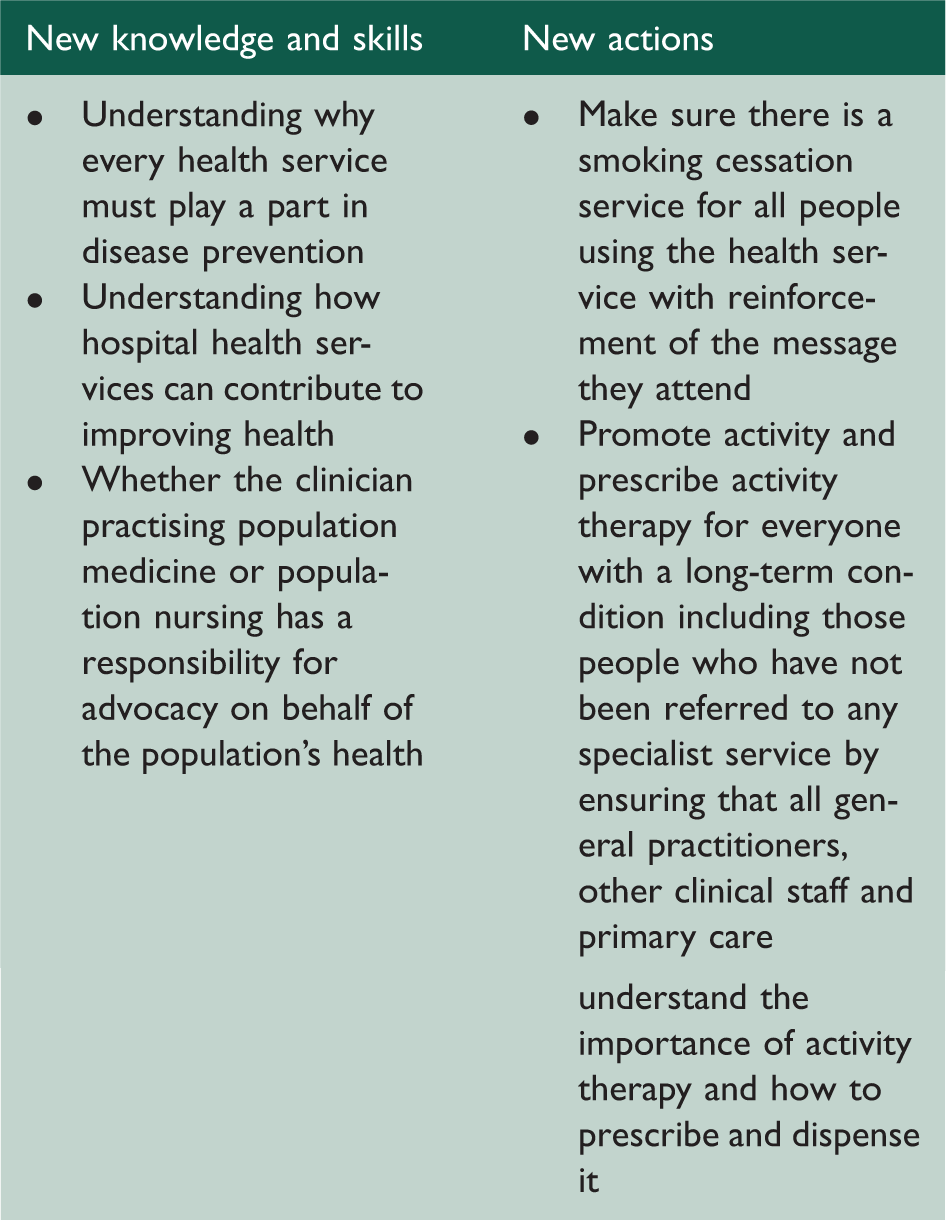
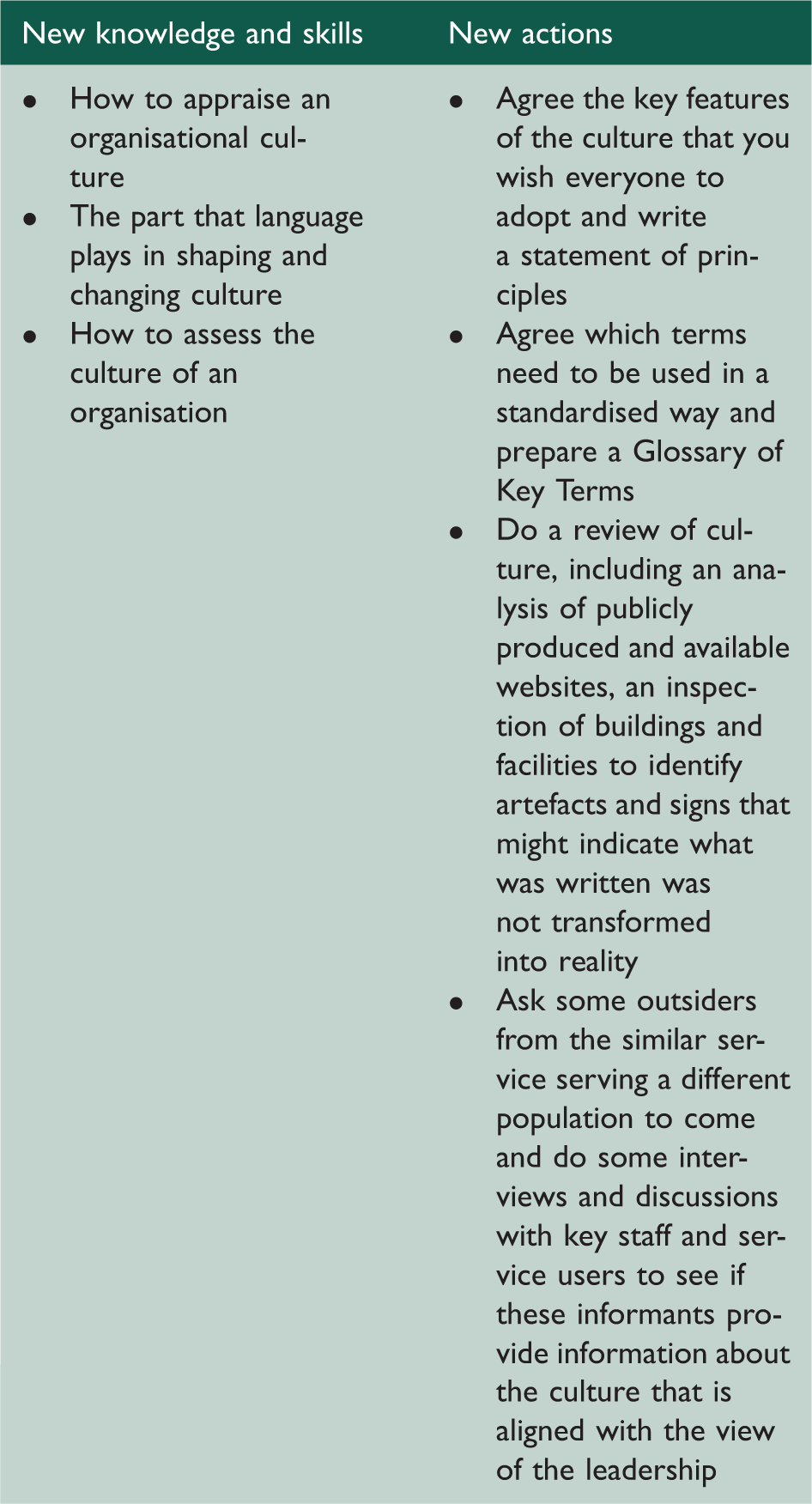
Leading the transformation and creating the right culture
Public Health professionals’ contribution
It could be argued that many of the skills and principles of population healthcare are simply the application of public health principles to the delivery of health services as opposed to using public health skills to prevent disease, promote health and mitigate inequity. The term ‘population healthcare’ and the related term ‘population medicine’ were, however, chosen because of the resistance of many clinicians to be encouraged to work like public health professionals. There is still a social class hierarchy in medicine with public health, at least until very recently being seen in the lower classes intellectually and socially. However, public health professionals are increasingly playing a part in working with colleagues, paying for and managing health services to get them to think of population healthcare and the needs of the whole population, rather than simply meeting the needs of the patients referred to them.
Thinking digital
Pervading all of this transformation is an appreciation of the principle that healthcare, needs to be transformed from its focus on the institutions that have served us reasonably well in the past to systems and networks that will help as adapt the complex needs of a population and the individuals within it. Digital developments both enable and drive this change, and of course as Manuel Castells emphasises in his trilogy on the Network Society
5
in which he describes how the third industrial revolution, after the revolutions of steam and high technology, is being driven by three forces – citizens, knowledge and the Internet. A network is a set of interconnected nodes. A node is a point where the network intersects itself. A network has no centre, just nodes. Nodes may be of varying relevance to the network. A network is defined by the programme that assign the network its goals and rules of performance. The program is made up of codes that include the valuation of performance and criteria for success or failure.
5
There are skills required for digital healthcare, but it is better to think of the change needed as a cultural change because digital resources can enable any clinical or managerial activity. What is needed as well as a formal training programme is a group of enthusiasts in every population healthcare organisation, the Accountable Care System, for example, that promotes and enables the transformation to population and personalisation by realising the potential offered by the Internet, to use an old-fashioned term.