
Abstract

Background
Above recommended levels of intake, alcohol use is associated with harm including hypertension, haemorrhagic stroke, liver disease, mental health disorders and cancers, as well as accidents, injuries and assaults.1–3 The 2015 UK Global Burden of Disease study indicates that 2.9% of disability-adjusted life years and 1.9% of mortality are attributable to alcohol use, 4 and the 2013 Health Survey for England found that 23% of men and 16% of women in England drink at levels associated with risk to health. 5 This Health Survey for England estimate would now underestimate the proportion of men at risk, as a 2016 guidance update lowered the recommended maximum level of intake for men, and so would reclassify some of those previously considered at low risk, as at-risk drinkers. 6
Alcohol’s contribution to both mortality and morbidity rose steadily from 1990 to 2010. While this trend may have started to stabilise over the past five years, 4 alcohol-related hospital admissions continue to increase. 5 Alcohol was estimated to cost the National Health Service £3.3–3.5 billion/year between 2006–2007 and 2009–2010.7,8 The wider costs of alcohol use include costs to the criminal justice system, social services, employers, families and carers, among others, but as current alcohol pricing structures do not account for all externalities, much of the cost falls onto taxpayers. In 2012, the Westminster Government estimated that the annual cost of alcohol to UK society was £21 billion. 9 Despite these figures, alcohol affordability has risen steadily over many years, and alcohol is now estimated to be >50% more affordable than it was in 1980. 5 Alcohol is additionally an important driver of health inequalities.10,11
Alcohol price interventions considered and/or trialled in the UK.
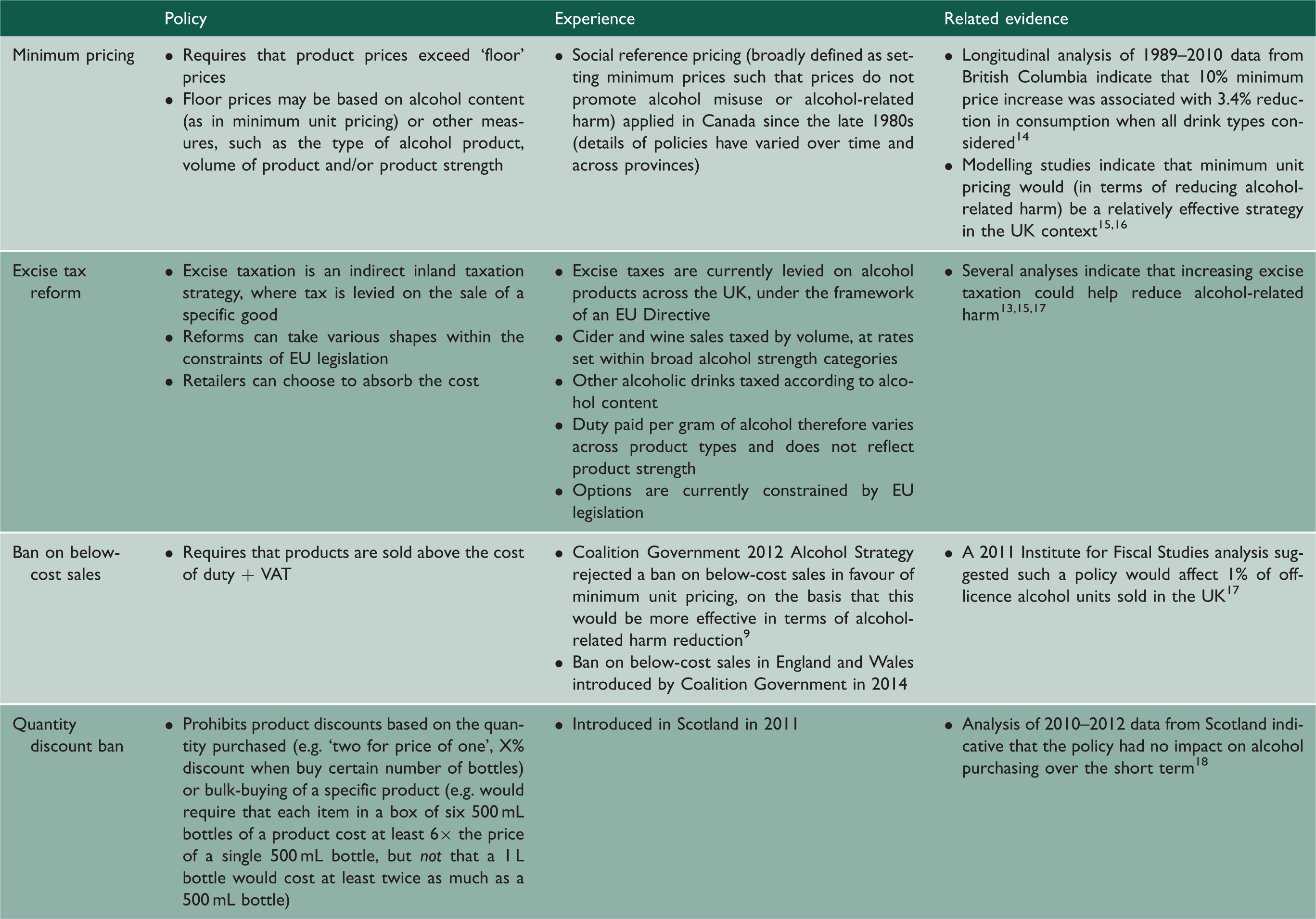
EU: European Union.
As minimum unit pricing has yet to be implemented in any country, modelling studies currently constitute much of the related evidence base. A recent study that compared alternative pricing strategies with minimum unit pricing for England in 2014–2015 concluded that content-based taxation or minimum unit pricing would be more effective than increasing taxation under the current system, or taxation based on product value, in terms of impact on harmful drinking and health inequalities. 15 Another recent study estimated that minimum unit pricing would have a 40–50 times greater effect on each of consumption, hospital admissions and deaths, than a ban on below-cost sales. 16 There are relevant empirical data from British Columbia, Canada, which has applied social reference pricing (which sets a minimum price per product type and volume rather than per volume/strength) to alcohol products for many years. A recent evaluation found that a 10% increase in the minimum price of any given alcohol product reduced consumption relative to other products by 14.6%–16.1%. 14
Introduction of minimum unit pricing policy in the UK
Based on the earlier contributions to this evidence base, and in keeping with national health strategy documents that have for many years highlighted the importance of investment in preventive healthcare, and promotion of healthy lifestyles including healthy levels of alcohol consumption,19,20 the Westminster Government’s 2012 alcohol strategy committed to minimum unit pricing for England and Wales. 9 In the same year, the Scottish parliament – led by the Scottish National Party with a newly elected parliamentary majority – voted in favour of minimum unit pricing legislation, which was then enacted (but is yet to be implemented – see below). 21 A minority Scottish National Party government had been defeated on the issue in 2010, and re-introduction of a minimum unit pricing bill was noted as a ‘priority’ in the party’s 2011 election manifesto, which also commented on the evidence base, and support from the medical and policing professions. 22
Subsequent policy movements
Although widely supported by these professional communities, many third-sector organisations, and some parts of the alcohol industry (e.g. the Scottish Licensed Trade Association and the C&C Group), 23 both the Scottish and Westminster Government 2012 policies were met with opposition from the industry and alcohol exporters. 24 The policy for England and Wales was subject to considerable industrial lobbying during its consultation phase, 24 and the Coalition Government at Westminster dropped the policy in 2013, in favour of a ban on low-cost sales, introduced in 2014. 25 In its consultation response, the Government stated that it would be a mistake to implement minimum unit pricing without empirical evidence, before going directly on to note that banning below-cost sales (for which no empirical evidence existed at the time, and which modelling suggested would have little impact),16,26 would be used to stop cheap and harmful alcohol sales. 25 The policy change was widely viewed as submission to industrial interest. 27 No Westminster Government has since re-established minimum unit pricing policy. A recent Home Office statement notes that the option remains ‘under review’. 28
Initial opposition to the Scottish minimum unit pricing legislation came from the major European Union exporters of alcohol products, resulting in the European Commission commenting that the policy was potentially disproportionate to Scotland’s alcohol problem, and risked violating European Union competition law. 29 A subsequent Scotch Whisky Association-led petition for judicial review – arguing that the legislation was outwith the legislative competence of the Scottish Government and incompatible with European Union law – was dismissed by the Scottish Court of Session, 30 but heard on appeal at the European Court of Justice. The European Court ruled that as minimum unit pricing threatened to constrain the market, it would only be justified if health could not be protected equally effectively by taxation measures that would be less restrictive in terms of limiting competition. 31 This posed a challenge as the existing evidence base had not yet demonstrated this specifically. The Scottish Government therefore commissioned specific research on this question, which demonstrated that minimum unit pricing would have greater impact on the most at-risk groups than an increase in alcohol taxation to levels that would lead to the same overall reduction in mortality. 32 Thus when the case – returned to the Scottish Court – was heard again in October 2016, the Court ruled in favour of the Government, citing evidence that the alternatives would be less effective than minimum unit pricing. 33 The Scotch Whisky Association has appealed and the case is to be heard by the UK Supreme Court.
Divergence of policy progress in Scotland versus Westminster
Minimum unit pricing policy in Scotland and Westminster – differential context and process factors.
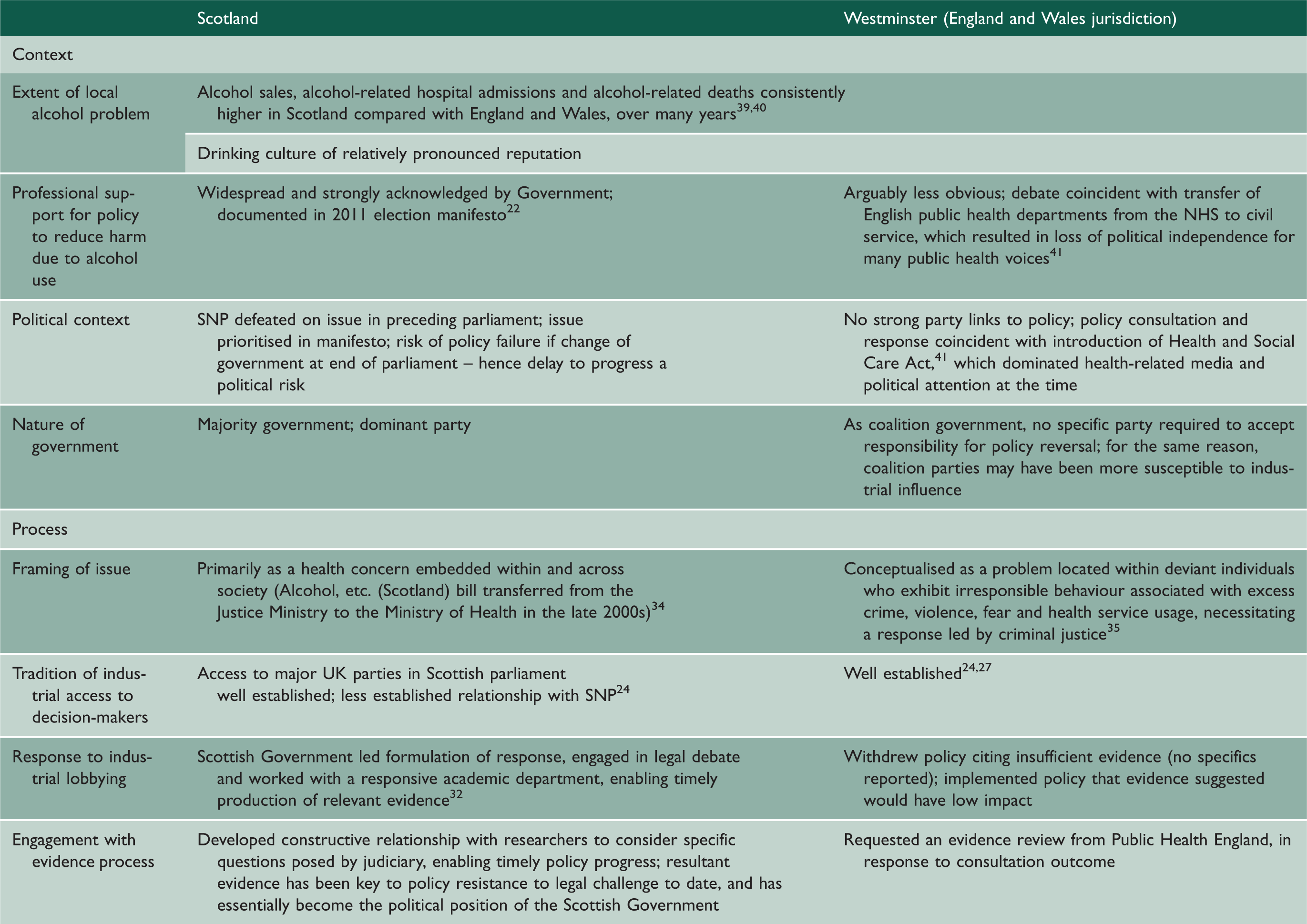
NHS: National Health Service; SNP: Scottish National Party.
Opportunities for public health input into minimum unit pricing policy and wider health policy
Considering these various factors in terms of options for public health input into ongoing policy development for England and Wales, the evidence review commissioned by the Westminster Government when it dropped its minimum unit pricing policy has recently been published, and provides a useful tool with which to advocate for government re-engagement with minimum unit pricing policy. 13 The Westminster Government is unlikely to re-establish minimum unit pricing policy while the legal process between the alcohol industry and Scottish Government is ongoing, but should the Scottish Government be successful at the Supreme Court, this combined with Public Health England’s recent recommendations would provide an opportunity to push for minimum unit pricing in England and Wales. Given the recent and ongoing cuts to local public health budgets, and the expectation that local public health departments should fund alcohol interventions understood to be less effective and less cost-effective than minimum unit pricing, 12 both local and national public health professionals should feel confident in their expectation and demand for national action.
Whether this confidence does exist, however, is questioned by one of our identified differences between the two policy contexts – namely the relatively constrained position of English service public health professionals in such public debate following their recent relocation to local authorities and the civil service. 41 Potentially the restrained nature of Public Health England’s comments on minimum unit pricing policy subsequent to publication of their assessment of the evidence (e.g. Public Health England statements in O’Dowd 28 ) is because of this. Thus, if expert input is a desired part of the policy development process, the new circumstances of English public health professionals may need to be balanced by changes to evidence review and policy development processes. The ease with which the current process can be misused by those with vested interests also favours the development of structures to facilitate rigorous discussion of evidence and defend the evidence review process. The minimum unit pricing experience indicates that more balanced opportunities for stakeholder representation to decision-makers (i.e. via widening access to decision-makers) could be usefully adopted at Westminster, following Scottish precedent. However, more fundamental changes to the evidence review process have been proposed elsewhere, 42 noting that reforming the process to promote fair-hearing of evidence should reduce both under- and over-use of evidence, and support democratic decision-making.
Such changes may be particularly wanting in Westminster in view of the renewed threat of Scottish independence, and the potential loss of public health advocacy, precedent in public health action and pre-emptive engagement with relevant legal processes, that Scotland has supplied several times over recent years. A reformed use of evidence would also be helpful in the pending opportunity to impact on decision-making, regulatory and legal processes in the UK, when European Union legislation is repealed. Failure to capitalise on the opportunity to influence such process development would potentially provide industrial and individual interests relatively unbalanced access to the UK policy agenda in future. Under such conditions, it would be likely that both evidence and health would be relatively side-lined in future policy development.
Finally, despite the ongoing discussion about minimum unit pricing policy across the UK, and although it is difficult to predict what it would take for the Westminster Government to revert to a minimum unit pricing policy, any minimum unit pricing policy that does come to be implemented in Scotland or England and Wales will only be implemented because the relevant evidence exists. The case is a positive example of the vital role evidence plays in the policy process, a demonstration of the benefit of relevant and timely evidence, and of the potential benefits to be gained through collaboration with policymakers, who in this case played an important role in the evidence-generation process. As others have previously suggested, 43 promoting such practical application of academic public health resources would likely enhance their impact.