
Abstract
Objective
To investigate trainee doctors’ and trainers’ perceptions of the validity of the Annual Review of Competence Progression (ARCP) using Messick’s conceptualisation of construct validity.
Design
Qualitative semi-structured focus groups and interviews with trainees and trainers.
Setting
Postgraduate medical training in London, Kent Surrey and Sussex, Yorkshire and Humber, and Wales in November/December 2015. Part of a larger study about the fairness of postgraduate medical training.
Participants
Ninety-six trainees and 41 trainers, comprising UK and international medical graduates from Foundation, General Practice, Medicine, Obstetrics and Gynaecology, Psychiatry, Radiology, and Surgery, at all levels of training.
Main outcome measures
Trainee and trainer perceptions of the validity of the ARCP as an assessment tool.
Results
Participants recognised the need for assessment, but were generally dissatisfied with ARCPs, especially UK graduate trainees. Participants criticised the perceived tick-box nature of ARCPs as measuring clerical rather than clinical ability, and which they found detrimental to learning. Trainees described being able to populate their e-portfolios with just positive feedback; they also experienced difficulty getting assessments signed off by supervisors. ARCPs were perceived as poor at identifying struggling trainees and/or as discouraging excellence by focussing on minimal competency. Positive experiences of ARCPs arose when trainees could discuss their progress with interested supervisors.
Conclusions
Trainee and trainer criticisms of ARCPs can be conceptualised as evidence that ARCPs lack validity as an assessment tool. Ongoing reforms to workplace-based assessments could address negative perceptions of the ‘tick-box’ elements, encourage constructive input from seniors and allow trainees to demonstrate excellence as well as minimal competency, while keeping patients safe.
Keywords
Introduction
All doctors in training in the UK (‘trainees’) are assessed annually by the Annual Review of Competence Progression (ARCP). The ARCP is a formal and structured way of monitoring trainees at each stage of training. It is intended to protect patients and ensure that doctors gain suitable and sufficient experience and training to progress. 1 Using an electronic portfolio (‘e-portfolio’), trainees collate evidence of their learning and experience which includes evidence that they have undertaken a set number of workplace-based assessments such as direct observations of procedural skills, case-note reviews and self-reflective learning logs. The e-portfolio is reviewed against a relevant curriculum by a panel who decides whether the trainee can progress. 2
There is little research on the ARCP panel; however, workplace-based assessments have received more attention, with findings showing they are not always positively received by trainees. A narrative review of medical and dental workplace-based assessments found negativity due to assessments having unclear purpose, providing insufficient quality feedback and a lack of time to carry them out. 3 Formative workplace-based assessments are felt to be more educationally valuable than summative ones,4,5 and there are calls to move away from the tick-box culture of workplace-based assessments.6–8 Opinions on specific summative workplace-based assessments are mixed: mini-clinical evaluation exercises are viewed as beneficial for development but difficult to implement,9,10 and multi-source feedback can be effective but also unhelpful. 11 Relatively few studies have looked specifically at ARCPs in the UK, and those few report mixed views, with some trainees finding the e-portfolio confusing and lacking in educational value 12 and others feeling confident using the system and finding the panel fair but lacking individual feedback. 13 There are also concerns about the fairness of ARCP outcomes because doctors who graduated from medical schools outside the UK are at increased risk of poorer outcomes than UK graduates. 14
In this study, we examined the validity of ARCPs by exploring how ARCPs are perceived by trainees and trainers, using Messick 16 and Cook et al. 18 to guide our analysis. The data were gathered as part of a study of perceptions of the fairness of postgraduate medical training, commissioned by the General Medical Council. 20
Method
Participants and data gathering
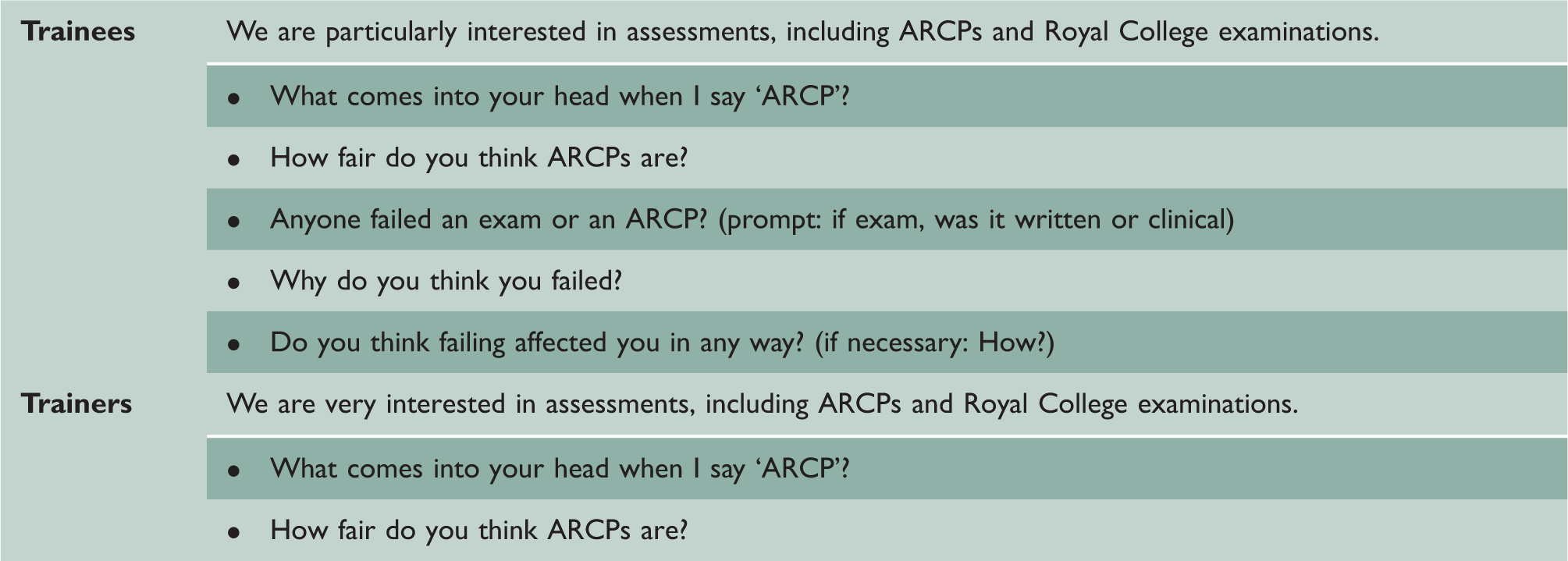
Questions specific to ARCPs asked in interviews and focus groups.
Analysis
Data were transcribed professionally. The research team (RV, AR and KW) examined the data to identify emerging themes, using thematic analysis
21
guided by Mountford-Zimdars et al.’s
22
analytic framework. A final coding framework was refined by KW, AR and RV after discussion. The whole dataset was coded by RV, with portions of the dataset second coded by the rest of the research team; consistency was ensured by discussing the framework with all team members and agreeing descriptors for each code; coding discrepancies were resolved through discussion. Coding was conducted using QSR International’s NVivo 10© software.
23
Two primary themes emerged around ARCPs: ‘ARCPs are fair’ and ‘ARCPs are not fair’. On further examination further subthemes emerged around why ARCPs were fair or unfair; these concerned the validity of ARCPs and were then analysed using Messick’s
17
framework as a guide (Figure 1).
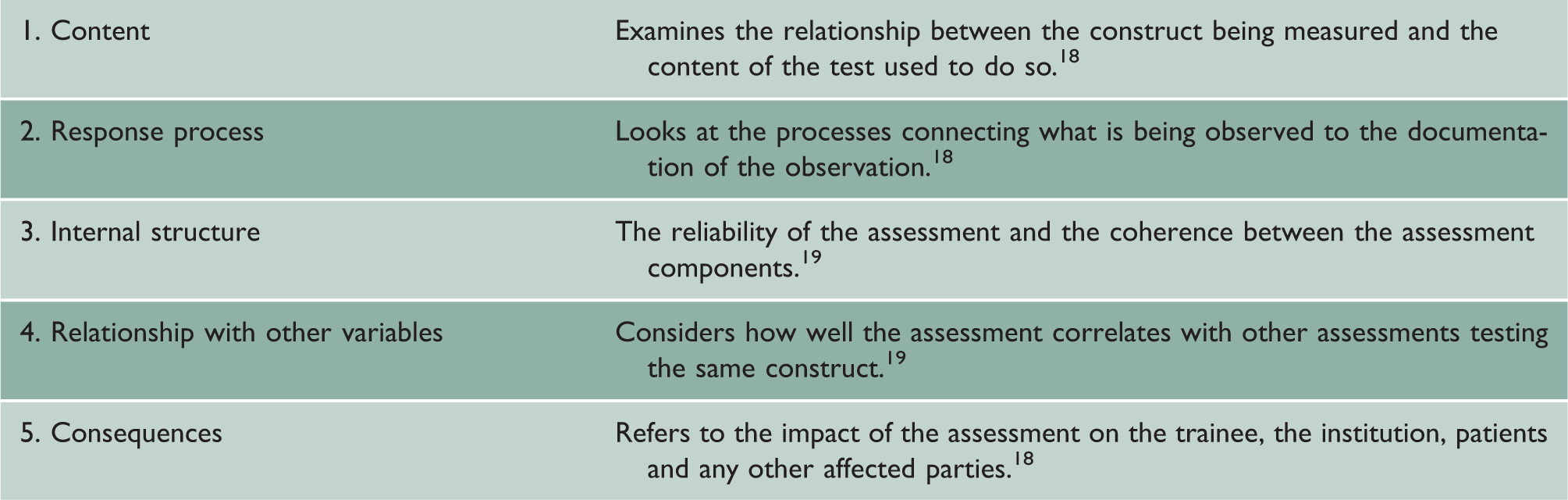
Subthemes within the five sources of construct validity evidence.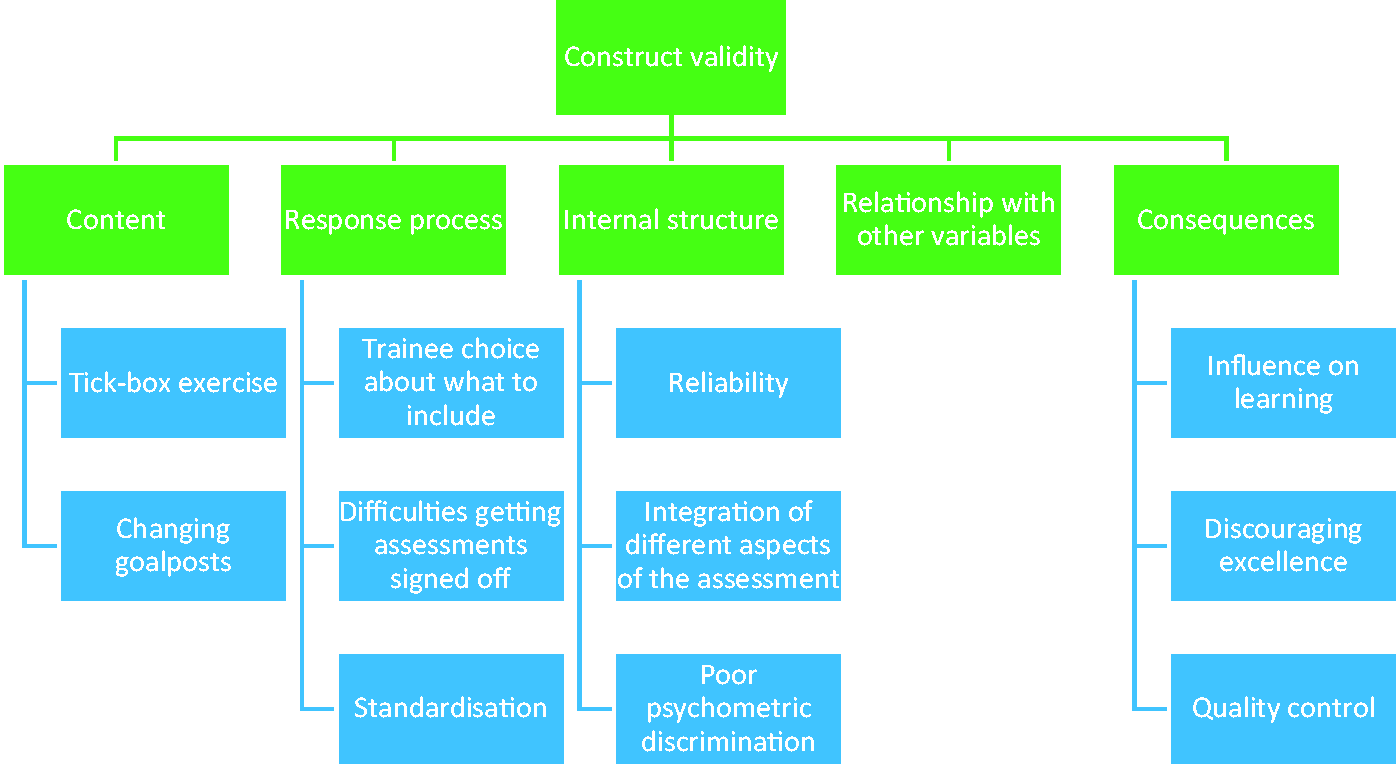
Results
Trainee and trainer perceptions of the validity of ARCPs are presented according to the five main sources of validity evidence described in Table 1. Subthemes are shown in Figure 1. Although the data for this analysis are participants’ perceptions and experiences of ARCPs, the various themes raised relate to all five sources of validity evidence and not just participants’ engagement with the process and its consequences.
Overall there was general dissatisfaction with ARCPs, especially among UK graduates – international medical graduates were more positive. Trainers tended to view the process more positively although they did voice negative views.
Content
‘Tick-box exercise’
ARCPs were described as a ‘tick-box exercise’ in 27 of the 65 interviews and focus groups
a
; this was generally a criticism of populating the e-portfolio. ARCPs were felt to test clerical ability rather than clinical ability, which some believed were inversely correlated: I’d say that people I’ve found who are very good at filling all their logs and do extremely well in the e-portfolio are actually the ones who are not very good clinically. (Trainee/GP/ST1-3/UKG/white/female)
b
Another common criticism was that the competencies being assessed were irrelevant to trainees' current or future work and a waste of time: With the practical, procedural skills that we have to get done, I feel like they’re more a tick-box exercise, and they’re not actually that useful because a lot of the skills are becoming more done by Radiology. (Trainee/Medicine/ST1-3/UKG/white/female) I think it is fair because it looks at ‘Have they passed the exams? … Have they done their workplace based assessment?’ … So I think it is fair, it does look at a large aspect of a broad training scheme. (Trainer/GP/UKG/white/male)
Changing goalposts
Some trainees described assessment criteria changing with little or no notice. One trainee said that after completing half of the necessary workplace-based assessments she discovered that the criteria had changed and the assessments she had completed were now redundant (Trainee/Medicine/ST4+/UK/white/female). In another instance, a trainee reported that miscommunication caused an entire cohort to fail for having an incorrect number of supervisor reports (Trainee/Medicine/ST4+/UKG/white/female).
Response process
Trainee choice about what to include
There was a perception that trainees could exclude anything negative from their e-portfolio. For example, trainees can carefully choose seniors to sign them off or give positive feedback because the trainee fits in socially: All my [Case Based Discussions], everything has been from registrars who have generally said, ‘Yeah, I’ll just do one for you’. It’s not been a formalised thing. It’s basically been the same as the rugby tie, but rather than wearing a tie, I’ve just known them and get on with them, and then they’ll do the thing for me. (Trainee/GP/ST1-3/UKG/white/male)
Difficulties getting assessments signed off
Several trainees described difficulties getting seniors to sign off assessments due to lack of engagement or system difficulties. Other trainees were unable to complete all the necessary supervised procedures, either due to the unavailability of clinical opportunities or because they were deemed competent to carry them out unsupervised. In extreme cases the failure of supervisors to sign off affected ARCP outcomes: Trainee 1 I’ve sat in an ACRP and been told I’ve not got enough assessments signed, I’ve just pulled out the list of all the tickets that I’d sent out that hadn’t been completed by consultants. … You can’t defend yourself in that situation. … Trainee 2 Yeah, the assumption is that the lack of work-based assessments is a reflection on the laziness or the lack of motivation or the lack of- Trainee 1 ‘Failure to engage with the portfolio’ is the phrase they use here. (Trainee 1/Medicine/ST4+/UKG/white/male) (Trainee 2/Medicine/ST1-3/UKG/white/female)
Standardisation
International medical graduates were most likely to say that ‘ticking boxes’ resulted in a standardised approach making the process fairer, although other trainees felt that standardisation did not make up for a lack of content validity: I think [ARCPs] are fair in the sense that they are a piece of standardised paperwork which anyone can learn to get filled out. I think if you ask ‘Are they an effective assessment of any practical measure of doctoring ability?’, that one I'm probably less certain about their quality. (Trainee/Medicine/ST4+/UKG/BME/male)
Internal structure
Reliability
There was concern at lack of consistency in ARCPs across specialties, regions and training grades. One trainee described completing extra documentation implemented by her training programme director, which was not used in other subspecialties or regions (Trainee/Medicine/ST4+/UKG/white/female). Some voiced concern about panel reliability and fairness. For example, one trainee described how a black colleague received a lower outcome and more ‘hassle’ than another equally experienced white trainee, which he thought was due to their ethnicity (Trainee/Surgery/ST4+/UKG/BME/male).
Several GP trainers voiced frustration at the apparent disconnect between their assessment of a trainee and that of the panel. GP trainees attend panel only if their progress raises concerns, which was compared to ‘Sending them to the headmaster’s office for a telling off’ (Trainer/GP/UKG/white/male). Yet if the panel passed a trainee, this undermined the trainers and could damage the trainer–trainee relationship irrevocably (Trainer/GP/IMG/BME/female).
Integration of different aspects of the assessment
Some trainees felt that the ARCP’s different criteria were poorly integrated; trainees could fail an ARCP for something trivial while significant achievements were ignored (see also ‘Discouraging excellence’ section): … it had been a big achievement and it sort of felt like in any process that’s supposed to be about your achievements and what you’ve done it’s just completely bonkers that they hadn’t mentioned that and they had mentioned the really basic thing that I hadn’t got a tick-box signature to do. (Trainee/O&G/ST4+/UKG/white/female)
Poor psychometric discrimination
Several trainees felt that ARCPs were poor at discriminating between trainees of different abilities: They’re not fit for purpose because they don’t identify poorly performing trainees. They don’t identify excellent trainees. (Trainee/Medicine/ST4+/UKG/white/male)
Relationships with other variables
Only one participant spoke about the relationship between ARCPs and other assessments. An internationally trained trainee knew two internationally trained colleagues who progressed well in their GP training (presumably passing their ARCPs) but failed their GP exit exam (Trainee/Psychiatry/ST4+/IMG/black/male).
Consequences
Influence on learning
In general, trainees did not feel that populating their e-portfolios encouraged learning; instead completing a large number of assessments impeded learning, either by demotivating trainees as ‘the more you do the less value you attach to each one’ (Trainee/Surgery/ST4+/UKG/BME/male) or by taking up time that could be better spent on another educational activity: Our e-portfolio seems to be ever expanding and sprawling and it gets to the point you wonder what the actual benefit of it is from an educational point of view. You find that you spend more time filling in boxes than you do reading about a subject. (Trainee/O&G/ST4+/UKG/white/female)
There were mixed views about attending ARCP panels. Several hospital medicine trainees disliked attending panels, finding them stressful, whereas others would prefer to attend the panel and have the opportunity to raise issues and get individualised feedback.
A few trainees commented that trainers’ understanding of the system and their willingness to engage with it influenced how useful the ARCP process was for learning: It all boils down to who’s your supervisor and whether they understand the system, whether they’re committed to you as a trainee. (Trainee/Medicine/ST1-3/UKG/white/female) Obviously people need to make sure that you are where you should be. That’s just it, they’re just trying to ensure that you’re getting the support you should be getting. (Trainee/Psychiatry/ST4+/IMG/BME/female)
Discouraging excellence
Some trainees felt that ARCPs encouraged minimal competency at the expense of excellence, and that trainees could effectively be penalised for being competent when they started a placement: There’s the expectation to show development through the year, so you’re supposed to start off bad and end up better. But if you start off good you’re in real trouble. (Trainee/Medicine/ST4+/UKG/white/male)
Quality control
Quality control was seen as an important purpose of ARCPs by trainees and trainers, but the concerns described above made trainees and some trainers question whether ARCPs were able to prevent poor trainees progressing and protect patients.
Discussion
Statement of principle findings
Many trainees and trainers felt that ARCPs could be useful and that assessment is necessary to check progress; however, the way that ARCPs are currently conducted is problematic. Viewed in terms of psychometric validity, participants’ – especially trainees’ – views suggested a lack of evidence for the validity of ARCPs as a means of assessing progress. In particular, there was poor evidence for the e-portfolio’s content validity with its ‘tick-box’ nature viewed as assessing trainees on clerical rather than clinical ability and concerns that trainees could select only positive assessments for their e-portfolio. Other major concerns were that ARCPs encourage minimal competency instead of excellence while not being sensitive enough to identify poorly performing trainees, and that ARCPs discourage learning and disengage trainees. Attending the panel could be stressful but also an opportunity to gain individualised feedback. Positive experiences of ARCPs arose when trainees could discuss their progress with interested supervisors. International medical graduates felt more positive about having standardised boxes to tick which they felt was fair.
Strengths and weaknesses of the study
This was a large study across four regions in England and Wales, involving doctors from six specialties plus foundation, from all stages at trainee or trainer level. Participants included female and male UK and international medical graduates from various ethnic backgrounds. The scale of the research resulted in a rich qualitative dataset with 137 participants from across the UK. However, we spoke to more GPs and fewer radiologists, limiting our ability to examine differences between specialties. The research was conducted during negotiations between the British Medical Association and the UK government regarding the new junior doctors’ contract in England; however, the negative opinions expressed by participants reflect those reported in earlier research24,25 and so the political climate did not appear to influence participants’ reports unduly. Response bias is possible, as participants volunteered in response to circulated information about the research and those with negative experiences may have been more interested in taking part; however, most participants shared both negative and positive experiences.
Strengths and weaknesses in relation to other studies
The findings presented here reflect prior research on trainees’ opinions about ARCPs and workplace-based assessments; for example, that trainees feel disillusioned with the process and ARCPs discourage excellence, 25 and that ARCP outcomes are not a useful evaluation measure of a curriculum. 24 Our research suggests that ‘tick-boxes’ are often perceived as reductionist and that assessments which provide more quality formative feedback during training as well as at the annual review would be beneficial. Much previous research has focused on limited geographical areas or specific specialties;12,13,26 as this study involved participants from across England and Wales, and across specialties, its findings may have a greater reach.
Meaning of the study: possible mechanisms and implications for clinicians or policymakers
In September 2016, Health Education England acknowledged that the ‘tick box culture of the ARCP’ has become problematic and announced a review of ARCPs to begin in October 2016. 27 Similarly, the Joint Royal College of Physicians Training Board has outlined the move within UK internal medicine training to a model of entrustable professional activities, 28 with the outcome of training being that trainees are ‘trusted to undertake all the key critical tasks needed to work as a consultant’. 6 To make a trust judgement, supervisors will need a holistic view of trainees’ abilities and our findings suggest that the input from trainers required to accurately form this holistic view (such as frequent formative assessment) is something trainees would value. Indeed, in related work, we found that good relationships with trainers are a key influence on trainees’ learning, 20 a point echoed in a call to return to an apprenticeship model in surgery training. 29 More opportunity for constructive feedback from the ARCP panel could be similarly beneficial. The 2008 Tooke report 30 emphasised the need for excellence in selection into postgraduate training, and our findings suggest that the revisions to workplace-based assessments should similarly allow trainees to demonstrate excellence as well as minimal competency, while keeping patients safe.
Unanswered questions and future research
Some participants mentioned differences in the ARCP process across specialties, grades, and regions; however, as ARCPs were not the sole focus of the research from which this paper stemmed, we were unable to include more detailed questions on this. It would be useful to establish if there are differences along these lines, and if so to investigate what they are and why they exist. Further work on the ARCPs’ components, including the panel, would also be of interest, as from our data it appears that different types of workplace-based assessment are prone to different problems. With the anticipated changes to workplace-based assessments 6 and a call to improve the training system for trainees, including strengthening the trainee–trainer relationship, 29 it will be useful to monitor trainees’ and trainers’ perceptions of the ARCP (or its replacement) after this change.