
Abstract

Injury to the larynx following intubation occurs in one-third of all patients. The national audit of the Royal College of Anaesthetists found that the larynx is the site most frequently injured (80%). 1 This may present difficult with adequate laryngeal assessment in patients undergoing microlaryngeal surgery. Trauma to intraluminal airway contents can occur. Unlike many anaesthetic challenges, this situation can be anticipated. Virtually all patients undergoing head and neck surgery have had direct flexibile laryngoscopy. As a result, many difficult situations can be pre-empted but despite this laryngeal trauma does occur.
With benign laryngeal lesions, surgical outcomes are voice improvement and histological diagnosis without deterioration in voice. Iatrogenic injury to professional voice users may in time present a medicolegal challenge. 3 Patient-reported outcome measures are increasingly used following microlaryngeal surgery and are the proposed subject matter for personal audit to provide evidence for revalidation in the United Kingdom. This may have implications for the surgeon.
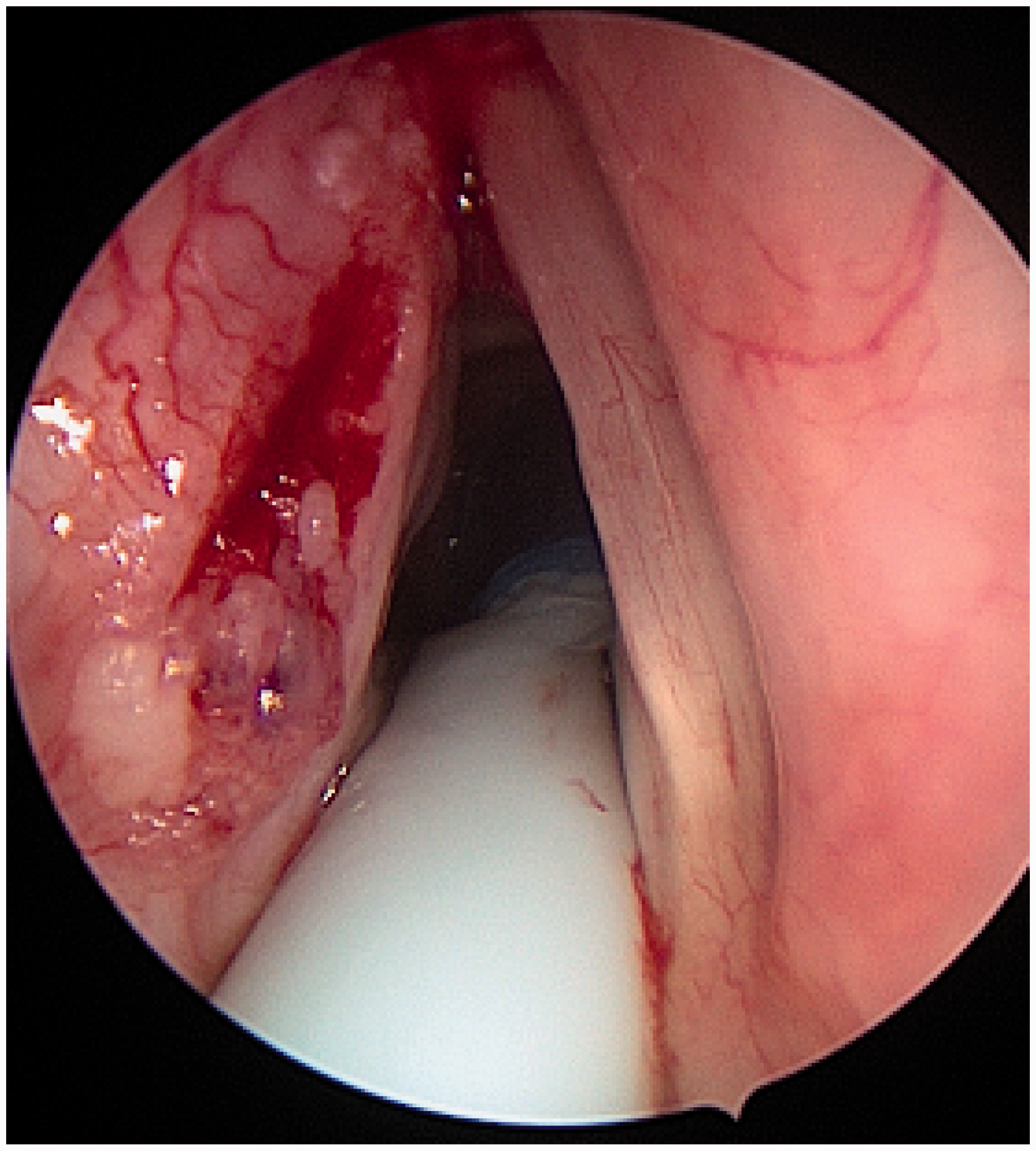
Difficulty intubating head and neck cancer patients is well recognised. Patients presenting with new cancers may have friable tumours that are dislodged into the airway or bleed. If they can bleed or be dislodged. Patients with previous head and neck cancer require long periods of surveillance, and often repeated examination under anaesthetic. Patients that have previously received chemoradiation have xerostomia, trismus, neck stiffness and fibrosis of their tissues (Figure 1). Even minimal trauma (Figure 2) might cause assessment and treatment difficulties. In the most difficult cases, tracheostomy may be required.
Typical appearance of stenotic larynx post chemoradiotherapy, tracheostomy tube seen between cords, feeding tube just visible posterior to larynx. Clinical photograph displaying left hemilaryngeal carcinoma in situ – the blood on the mid third of the left vocal cord displays some trauma caused during intubation.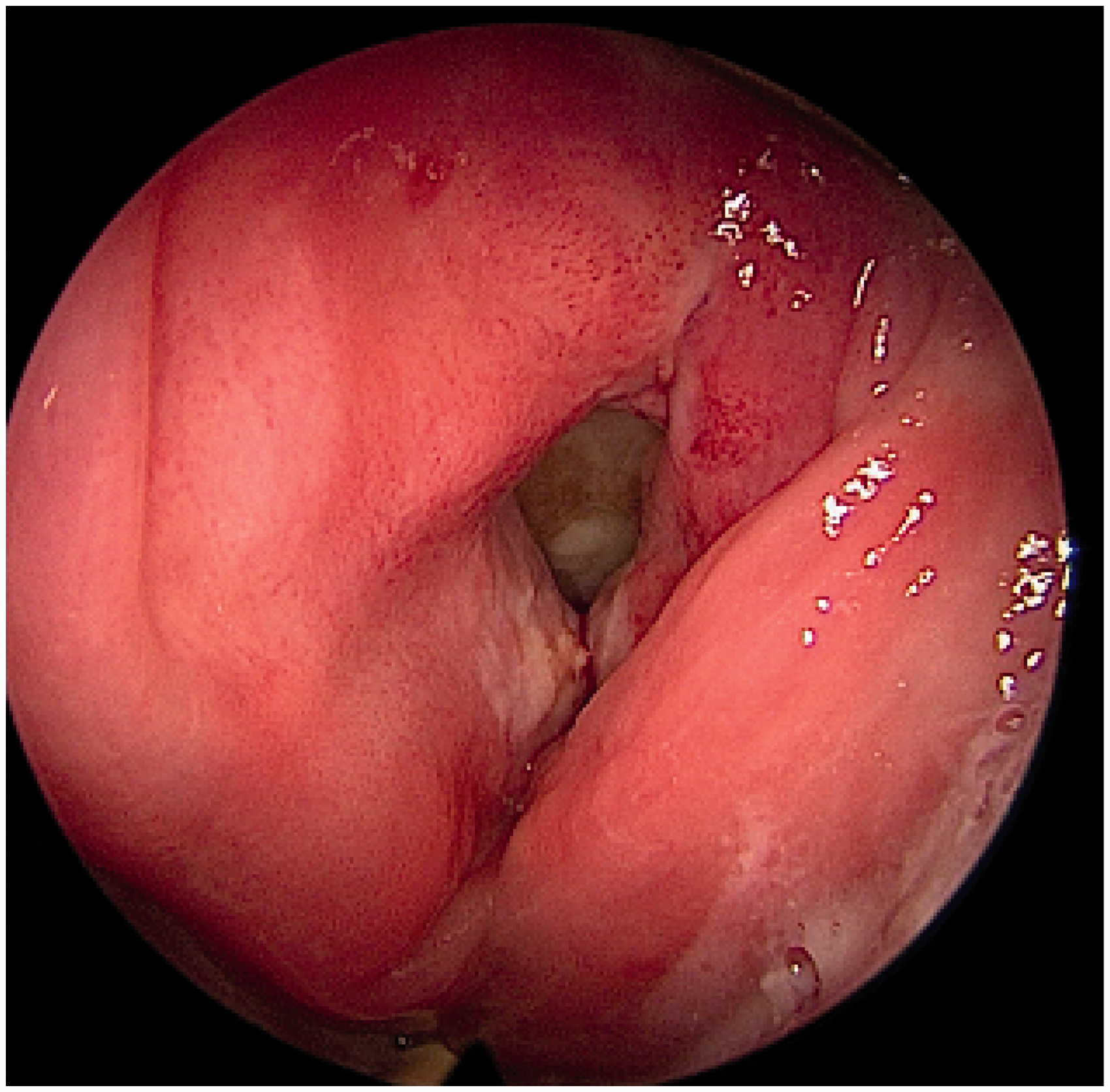
Trauma prevention is important in these situations. Tracheostomy, while necessary for definitive airway control for patients in extremis, is a procedure that many patients would rather avoid. 4 Here, the focus is correctly on safe airway management. A detailed discussion during surgical briefing and agreed airway plans, with alternative plans if necessary between anaesthetist and surgeon, improves communication and promotes safer surgery. 5 Endotracheal tube placement under direct vision is safer than blind intubation. 6
If standard intubating techniques becomes difficult, then videolaryngoscopy can facilitate access. Alternatively, the surgical team may intubate the patient using an anterior commissure laryngoscope. This rigid straight blade laryngoscope has a triangular lumen, which helps access to the anterior larynx (Figure 3). When intubating patients in this way, it is possible to pass a gum elastic bougie, with a microlaryngeal endotracheal tube passed over it, for satisfactory intubation.
Microlaryngoscopy equipment (anterior commissure laryngoscope shown to right of standard rigid laryngoscope).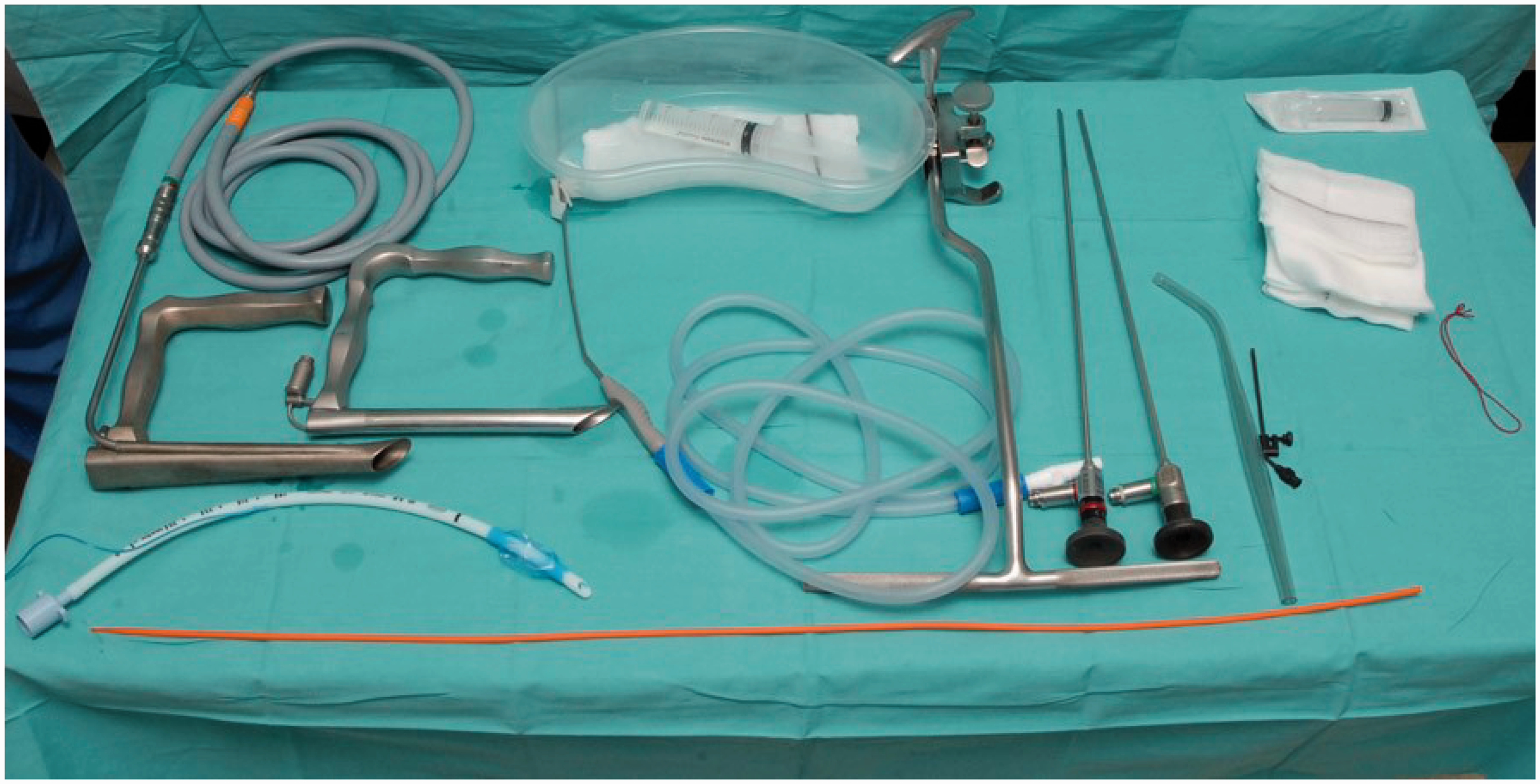
Optimised intubating conditions are achieved with full neuromuscular blockade. 7 Traditionally for shorter procedures, smaller doses of muscle relaxant were given for quicker reversal of anaesthesia. Lesser doses of muscle relaxant are, however, associated with postoperative airway symptoms and discomfort. 6 Sugammadex, a newer potent reversal agent, can be used to give an appropriate dose of relaxant, with no concern about complete reversal of blockade, even if the procedure is shorter than anticipated.
Specialist equipment can also cause injury. Recurrent laryngeal nerve monitoring is becoming the standard of care in thyroid surgery. Many surgeons use intermittent nerve monitoring, with continuous monitoring the subject of ongoing study.
8
This requires specialised endotracheal tubes, with electrodes attached to their outer surface positioned at the level of the vocal cords. These electrodes might cause injury to patients with pre-existing laryngeal disease, such as Reinke’s oedema, a condition of female smokers (see Figure 4).
‘Stripping’ injury of right vocal cord caused by electrode attachment to endotracheal tube.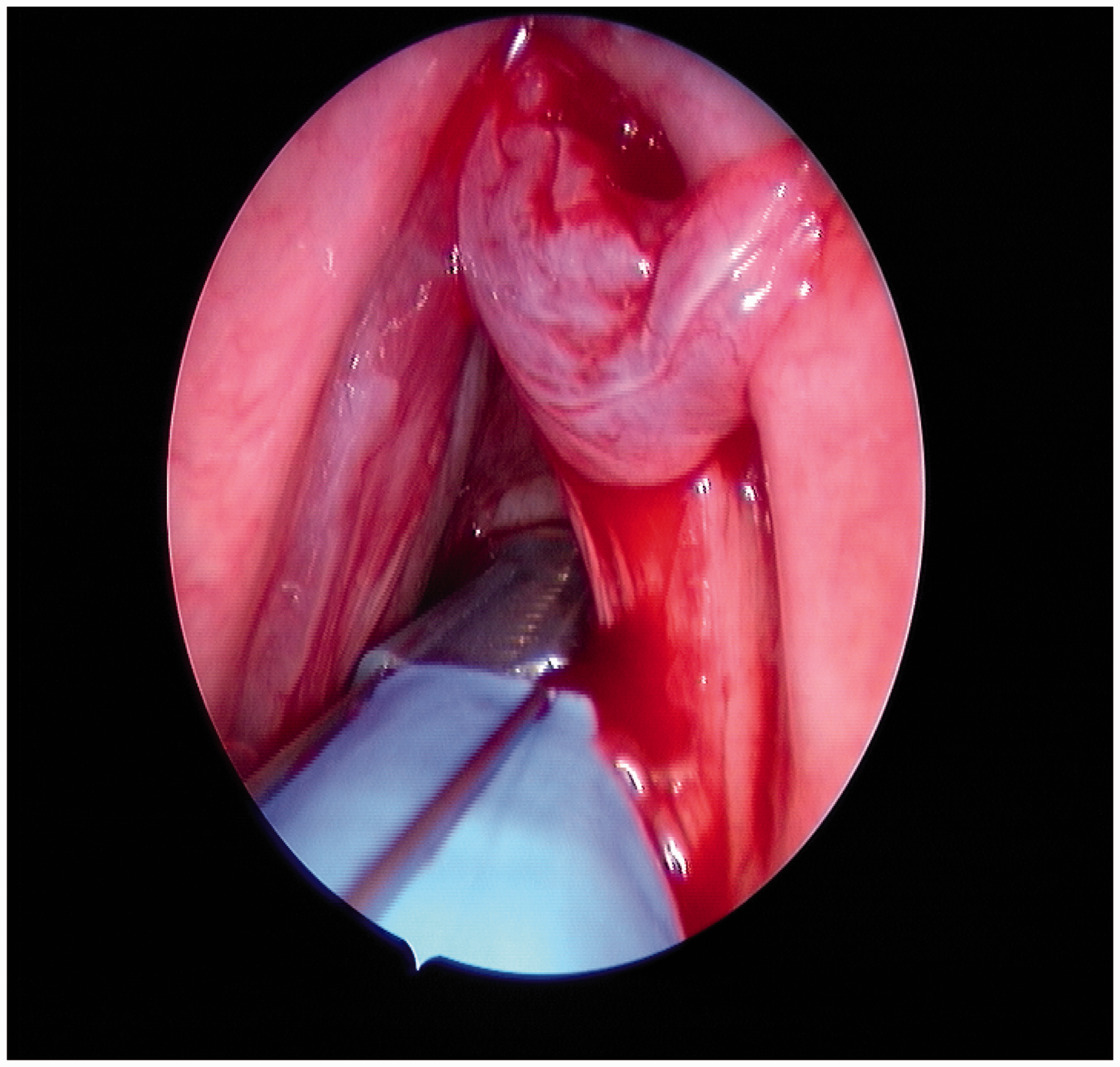
Vocal cord palsy is a well-described complication of endotracheal intubation. It is usually temporary, secondary to compression of the recurrent laryngeal nerve. The left vocal cord is more vulnerable as the laryngoscope is a left-handed instrument and the tube more likely to be secured against the left side. Vocal cord palsy rates are higher in patients with increasing age, co-morbidities and with longer duration of intubation. 9 Vocal cord palsies cause weakness of the voice, dyspnoea and risk of aspiration. Voice therapy and medical therapy can be considered if the palsy fails to resolve.
Laryngeal cartilage injuries are extremely rare; the most common of these is arytenoid dislocation or subluxation. This can cause hoarseness and is often mistaken for vocal cord palsy. Dislocation has an estimated incidence of 0.1%. 10 It can be readily diagnosed by flexible laryngoscopy. There is some benefit to closed reduction and voice therapy.
When iatrogenic laryngeal trauma does occur, it can adversely affect surgery. Increased awareness of the challenges of intubating patients with laryngeal pathology is important for prevention. When injuries do occur, laryngologists have a variety of options available, with the aim of treating disease, maintaining the airway and preserving the patient’s voice.