
Abstract
Objectives
To explore the impact of Modernising Medical Careers (MMC) training on the stability of medical career choices in the UK.
Setting
UK
Participants
Graduates of 2002 and 2008 from all UK medical schools, 1 and 3 years postgraduation.
Design
Questionnaire surveys were conducted of 2002 and 2008 graduates from all UK medical schools 1 and 3 years post graduation.
Main outcome measures
Doctors gave their specialty choice(s) and rated the influence of each of 11 factors on their career choice.
Results
2008 graduates were a little more likely than graduates of 2002 to retain their year 1 choice in year 3 (77.3% vs. 73.3%; p = 0.002). Among 2008 graduates, the percentage retaining their year 1 choice varied between 42% (clinical oncology) and 79% (general practice). Enthusiasm for a specialty, student experience and inclinations before medical school were associated with choice retention; consideration of domestic circumstances and hours/working conditions were associated with changes of choice. 2008 graduates were more likely than 2002s to be influenced by enthusiasm for a specialty, self-appraisal of their skills, working hours and their domestic circumstances; and less likely to be influenced by their experience of jobs, a particular teacher/department or eventual financial prospects.
Conclusions
Post-MMC, graduates were less likely to change their career choice and more likely to be motivated by personal factors and self-assessment of their suitability to a particular area of work.
Introduction
In any healthcare system it is crucial to have adequate numbers of doctors in each clinical specialty. From the perspectives both of workforce planning and of postgraduate training, it is important to examine not only how many doctors complete their training in a particular specialty, but also specialty changes along the way. Late changes of choice of specialty can create problems for the individual and the healthcare system. For trainees, a change of specialty may require them to train for longer, or even to repeat elements of their training, if training in the new specialty does not take account of transferable competencies. For the national healthcare system, the final numbers of trained doctors in each specialty may differ from what was forecast, necessitating recruitment by immigration to meet shortfalls. Further, doctors in training provide patient treatment in the course of their training, and changing numbers of trainees will therefore also have an impact on levels of service.
In our previous UK national cohort studies of career choices 1 we found early career choices to be predictive of eventual career destination. Ten years after graduation, over half of UK doctors were working in the specialty that they had specified as their first preference for their future career 1 year after graduation. Among doctors who described their year 1 career choice as definite, the figure increased to three-quarters. Recent changes to UK medical training might influence the stability and predictive power of early career choices. In 2005, Modernising Medical Careers (MMC) 2 was implemented. In this postgraduate training scheme, medical school graduates complete a 2-year foundation programme, termed the F1 and F2 years, which includes placements of several months’ duration in different hospital specialties. Those wishing to be GPs then undertake a 3-year training course, while for the hospital-based specialties the training is typically 6–8 years in length with an increasing depth of specialty focus over time. MMC has made postgraduate training shorter and more structured. However, graduates are now required to choose their broad specialty earlier than their predecessors, and normally apply for specialty training halfway through the F2 year.
The aim of the paper was to explore the impact of MMC on the stability of early career choices. We compare the level of changes of specialty choice between years 1 and 3 after graduation of two cohorts of UK medical graduates: the graduates of 2002 (pre-MMC) and those of 2008 (post-MMC). In year 1, the doctors in both cohorts gave us their preference of specialty before being on a specialty training programme; by year 3 many will have started training in their chosen specialty.
Method
All graduates of 2002 and 2008 from all medical schools in the UK were identified from registration information supplied by the General Medical Council. Our methods were as previously described.3–5 In brief, graduates were sent a postal questionnaire towards the end of their first and third postgraduate years, with non-respondents being sent a maximum of five reminders. Contact was also made by email using an online equivalent of the postal questionnaire, with reminder emails to non-respondents.
All graduates were asked to state up to three choices of long-term career, in order of preference. They were also asked to indicate whether any of the choices were of equal preference (referred to by us as ‘tied choices’). Respondents’ career choices were grouped together by us for analysis into 14 broad specialty groups based on those originally defined in the Todd Report. 6 In the subsequent sections, when we mention ‘specialty choice’ we are referring to those broad specialty groups, rather than more specific individual specialty/subspecialty choices.
List of factors for which the respondents had to answer: ‘How much has each of the following factors influenced your choice of specialty, or non-medical job?’, with response options being: ‘a great deal’, ‘a little’, and ‘not at all’.
We report percentages to describe our findings and use chi-squared tests of statistical significance. We compare the graduation cohorts of 2002 and 2008. We also divided the respondents into those who named the same specialty as their first career choice in postgraduate year 1 and year 3 (for those who gave more than one specialty choice, we allocated respondents to this group if at least one of their choices was retained between year 1 and year 3), and those who named a different specialty(ies) as their first career choice in first and third postgraduate year. We labelled the former group choice retainers and the latter choice changers. Since multiple similar analyses were performed on the same data-set, we took as evidence of a real difference p values of 0.01 or less.
Results
Response rate
After excluding doctors from the original graduation cohorts who were either not contactable, declined to participate, or were deceased, the response rates for the 2002 cohort were 65.3% (2778/4257) in year 1 and 64.8% (2748/4243) in year 3. For the 2008 cohort the response rates were 49.2% (3302/6705) in year 1 and 49.4% (3228/6540) in year 3.
In all, 2197 respondents (63% female) in the 2002 cohort and 2267 respondents (65.3% female) in the 2008 cohort replied to both first and third postgraduate year surveys. There was no significant difference between the cohorts in the proportion of female responders (
Consistency of career choice between first and third postgraduate years
In each cohort fewer respondents gave tied choices (see Method section) in their third than in their first postgraduate year. The percentage making tied first choices in year 1 was significantly higher in the graduates of 2008 than those of 2002 (19.9 and 13.9%, respectively;
Overall, in year 3, 75.3% retained a first career choice from year 1, 10.1% changed their choice to a specialty that was their second or third choice in year 1, and 14.6% changed their choice to a previously not chosen specialty. For brevity, we will refer to the 75.3% who retained at least one of their specialty choices as choice retainers, and the rest of respondents as choice changers.
Those who gave a tied first choice in year 1 were a little more likely to be choice retainers than those who gave only one first career choice in year 1 (78.3 and 74.7%, respectively, p = 0.04).
Women were as likely as men (74.6 and 76.5%, respectively, p = 0.17), and graduate entrants to medical school as likely as non-graduate entrants (74.4 and 75.1%, respectively, p = 0.72), to be choice retainers. The graduates of 2008 were a little more likely than graduates of 2002 to be choice retainers (77.3% vs. 73.3%;
Change in career choice and chosen specialty
Percentages and numbers of doctors retaining their year 1 first career choice in year 3 and the most frequent choice changes from year 1 to year 3 by specialty: UK medical graduates of 2002 and 2008.

HPS: Hospital physician specialties.
OMS – other medical specialties: includes public health, family planning, sexual health, community gynaecology, school health, alternative medicine, clinical anatomy, clinical physiology, pharmaceutical industry, medico-legal work, medical journalism, and third world medicine.
†‡§A change of choice for another specialty within the group – e.g. general medicine to cardiology, general surgery to orthopaedics, microbiology to haematology – was counted, for this analysis, as comprising the same choice for the broad specialty group.
Comparing the two cohorts (Table 2), graduates of 2008 were more likely than the 2002s to retain choices for emergency medicine, radiology and clinical oncology; graduates of 2008 were more likely than the 2002s to change choices away from the surgical specialties. There were a few other small differences between the cohorts. However, only cohort differences for radiology (
Considering the most common specialty changes (Table 2), general practice was a more frequent alternative choice across many hospital specialty choices among 2008 graduates than among 2002 graduates. However, in both cohorts, general practice was among the three most likely specialty changes from all earlier hospital specialty choices.
Factors influencing career choice
We asked the graduates, 1 and 3 years after graduation, to rate each of 11 factors according to whether it had influenced their choice of eventual career ‘a great deal’, ‘a little’ or ‘not at all’. We compared the percentages of participants who scored each of 11 factors (Table 1) as having influenced their choice of eventual career ‘a great deal’.
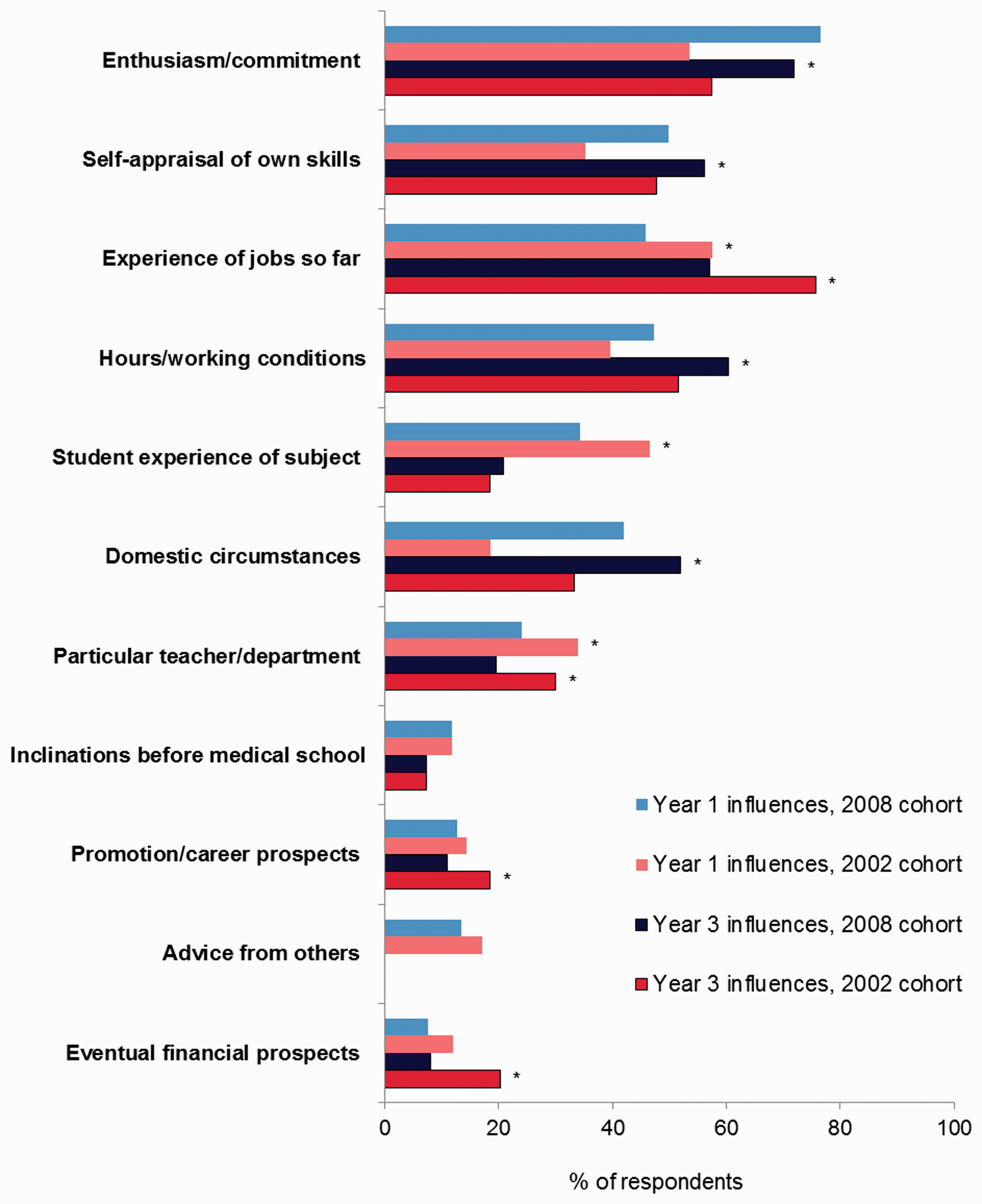
Considering the respondents who retained their first career choice between year 1 and year 3, one factor received the same response from both cohorts in both years: inclinations before medical school (Figure 1). Both in year 1 and in year 3, a higher percentage of graduates of 2008 than of 2002 reported being influenced ‘a great deal’ by enthusiasm/commitment for the specialty, self-appraisal of own skills, hours/working conditions, and domestic circumstances. Conversely, a lower percentage of 2008 than 2002 graduates were influenced ‘a great deal’, in both years, by experience of jobs so far, a particular teacher/department, and eventual financial prospects. Advice from others and student experience of subject were rated as a less important influence on career choice in year 1 by 2008 graduates than by 2002 graduates, and the same was true in year 3 for romotion/career prospects. A very similar pattern of results was observed for choice changers (Figure 2). Thus, regardless of whether the initial career choice was retained or not, some factors were more important for the graduates of 2008 and others for 2002 graduates.
Doctors who retained their preference for long-term specialty: percentages who specified each factor as influencing their choice of long-term career a great deal in postgraduate year 1 and 3, comparing the graduates of 2002 and 2008. *denotes p < 0.01 (outcome of Doctors who changed their preference for long-term specialty: percentages who specified each factor as influencing their choice of long-term career a great deal in postgraduate year 1 and 3, comparing the graduates of 2002 and 2008. *denotes p < 0.01 (outcome of 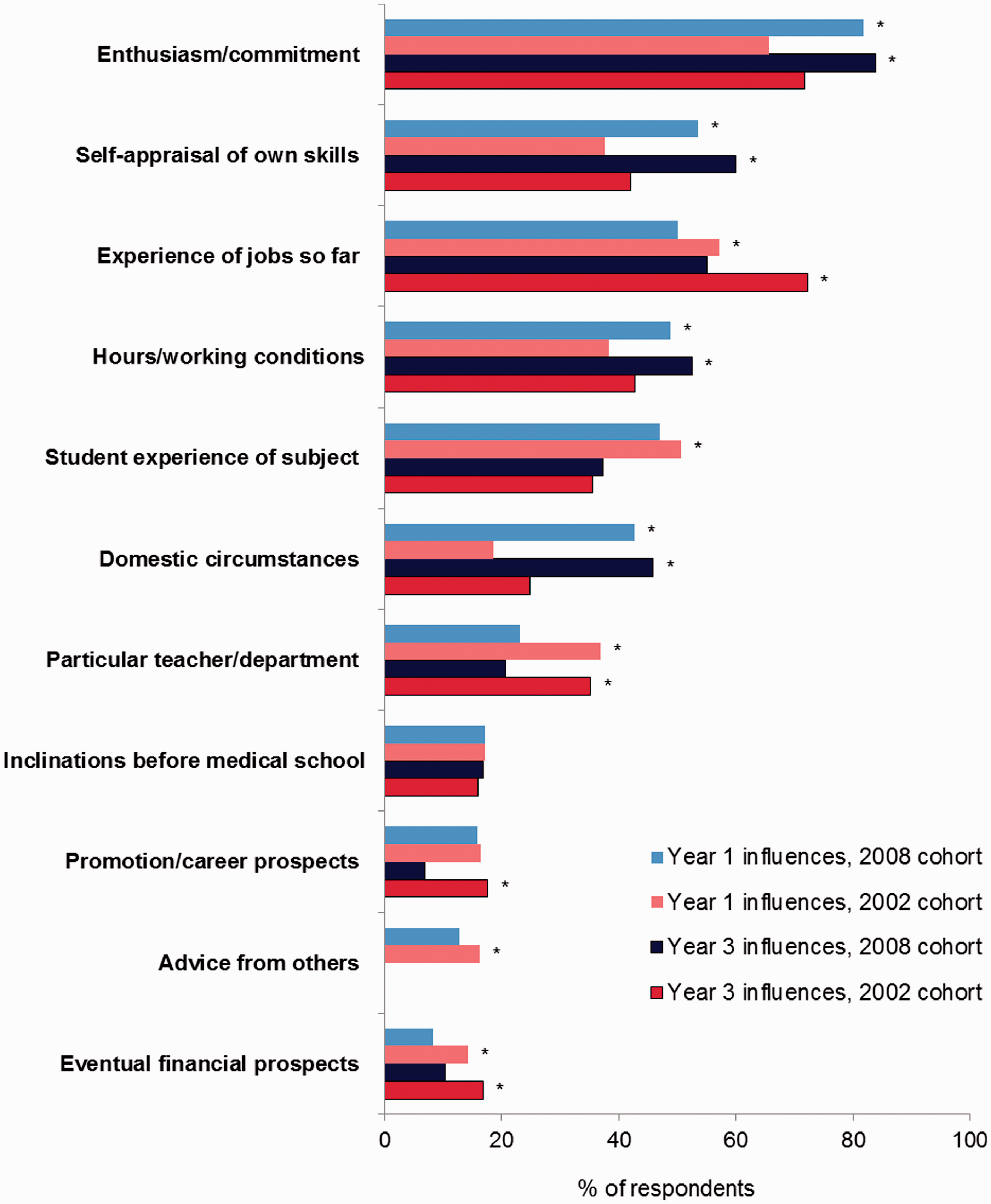
Despite cohort differences in the level to which each factor was important, the direction of change for most factors from year 1 to year 3 was the same in both cohorts. We therefore combined the cohorts and compared factor ratings in years 1 and 3 of choice changers and choice retainers (Figure 3). Those who had retained their career choice were more likely to have been influenced a great deal in both year 1 and year 3 by enthusiasm for the specialty, student experience of the specialty, and inclinations before medical school. Choice changers were more likely to have been influenced by their domestic circumstances and hours/working conditions in year 3.
Graduates of 2002 and 2008 combined: percentages who specified each factor as influencing their choice of long-term career a great deal in postgraduate year 1 and 3, comparing choice retainers and choice changers. *denotes p < 0.01 (outcome of 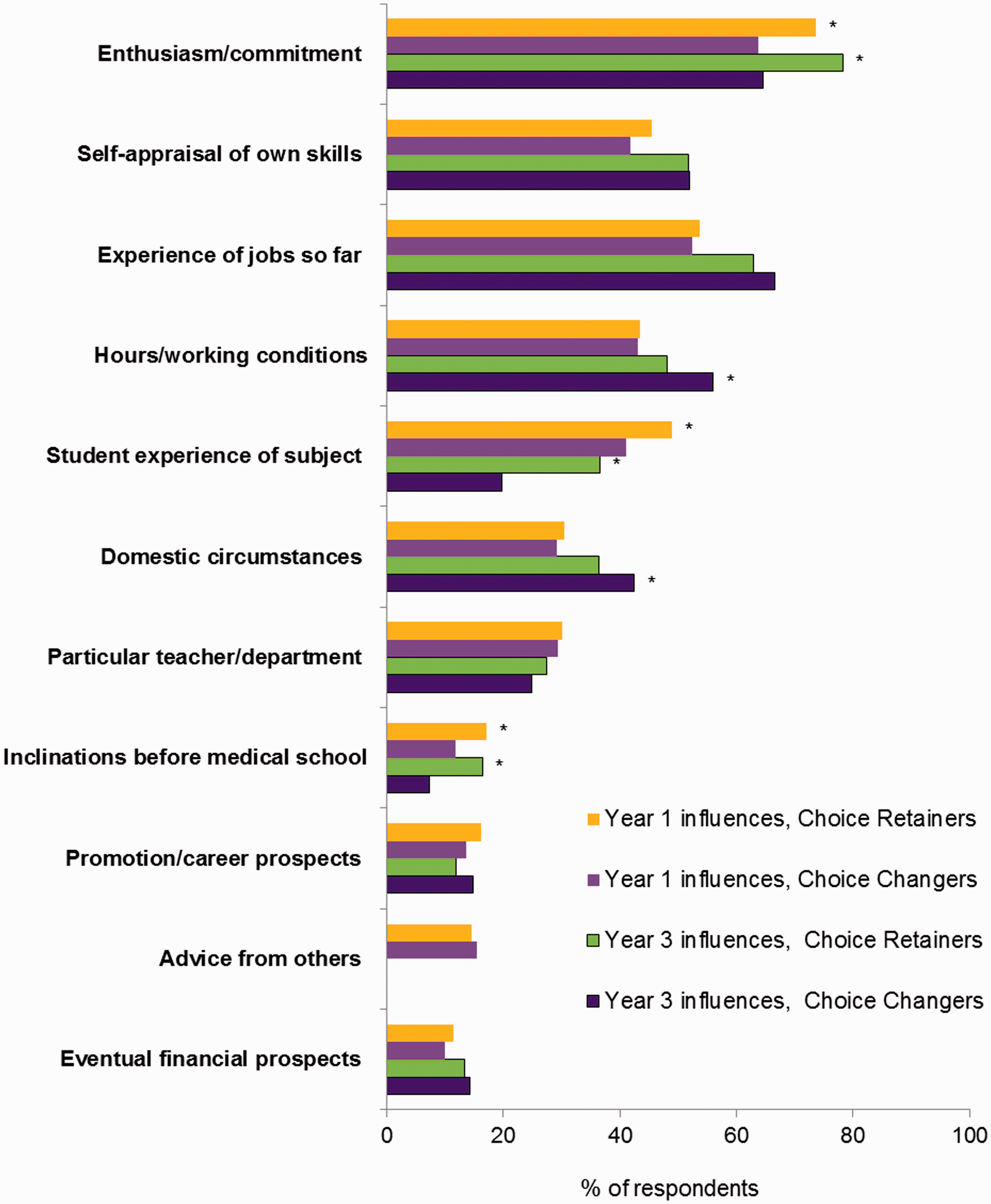
Views about careers advice and about the timing of making specialty choices
Both cohorts were asked to rate their level of agreement with the statement ‘Making career choices has been made difficult by inadequate careers advice’. A lower percentage of the graduates of 2008 than of 2002 agreed (36.5% vs. 42.3%;
Doctors in the 2008 cohort were asked in year 3 to specify their level of agreement with the statement ‘I had to make my career choice of specialty too soon after qualification’. This was not put to the qualifiers of 2002, but was added to the questionnaire for the 2008s because of concerns expressed that MMC was making some doctors have to choose specialties before they felt ready to do so. A total of 60.9% of 2008 graduates agreed or strongly agreed and only 21.9% disagreed or strongly disagreed with the statement. More choice changers agreed with the statement than choice retainers (26.8% vs. 17.1%;
Discussion
Main findings
Graduates of 2008 were less likely than those of 2002 to change their career choice between years 1 and 3 after graduation. However, differences between the cohorts were small. Differences between the specialties in whether or not doctors changed choice, in both cohorts, were much larger than any differences between the cohorts. General practice was the specialty with the highest level of retained choices between years 1 and 3, followed by psychiatry. General practice was, in both cohorts, the commonest year 3 alternative choice across most year 1 hospital specialty choices and was slightly more popular among 2008 than 2002 graduates. The shift away from surgery, between years 1 and 3, among 2008 graduates may reflect greater difficulty in the latter cohort in obtaining a training place or, perhaps, more realistic expectations about achieving an eventual career in surgery.
Even though the cohorts were quite similar in their retention or rejection of specialty choices, there were significant differences between them in the factors they specified as having an important influence on their choice of specialty. In both year 1 and year 3, the graduates of 2008 were more likely than the 2002s to have been influenced by enthusiasm for the specialty, self-appraisal of their own skills, working hours, and their own domestic circumstances; and less likely than the 2002s to have been strongly influenced by their experience of jobs so far, a particular teacher/department, or eventual financial prospects. There were very similar proportions of women respondents in the two cohorts, so these differences are not attributable to changing gender mix.
It appears from our findings that persistent influence of enthusiasm for the specialty, student experience of the specialty, and inclinations before medical school are associated with choice retention, while domestic circumstances and hours/working conditions may become more important later and might lead to choice change.
Strengths and limitations
The study is large scale and includes all UK medical schools. We are independent from people or organisations that might otherwise influence doctors’ responses; therefore we believe we get honest answers from them. The main limitation is that it is inherent in survey research methodology that there is a possibility of responder bias.
Policy implications
System of training
Under MMC, UK medical graduates make their specialty choices earlier than they did in the past. We found no evidence that their specialty choices are less stable now, at least between years 1 and 3, than they were in the past. It is possible that improvements in the provision of careers advice have negated any uncertainties associated with having to make earlier career decisions. We intend to check that no adverse effects of earlier career decisions emerge during later career stages by following up these two graduation cohorts in future.
For general practice, our results suggest that it became more popular post-MMC both as the initial career choice and a backup choice to which respondents switched. This trend should be encouraging to workforce planners, as general practice remains an undersubscribed specialty in the UK. 7
Despite an overall positive picture, the majority of the post-MMC cohort said that they had to make their specialty choice too early. Others have reported that there is a rise in the percentage of medical graduates not entering specialty training immediately after their two foundation years, and this may be attributable to the increase in the number of doctors who take a career break. 8 Checkley et al. 9 from the North Western Foundation School surveyed foundation trainees who did not go straight into specialty training. One of the most common reasons these trainees gave for this decision was uncertainty about future career specialty choice.
Time out can be beneficial for many reasons, but it would be lamentable if a sizable proportion of junior doctors marked time in their training solely because they needed more time to make their specialty choices. Changes to UK medical training that are currently being considered will hopefully ensure that this does not occur. The Shape of Training review has suggested that the structure of medical training needs to be more flexible to allow doctors to transfer their learning and experience between specialties and care settings. 10 This has particularly been argued for specialties such as emergency medicine, which experience specialist trainee shortages and tend to be chosen quite late. 11
In 2012, the Academy of Medical Royal Colleges developed a new 2-year structured core training programme called Broad Based Training (BBT), which consists of 6-month placements in four specialties and thus aims to provide broader experience before applying for specialty training. 12 Seven deaneries ran a pilot for BBT in 2013 and will have another round of recruitment to posts starting in August 2014. 13 Provided the pilot is successful, this might become a nation-wide scheme.
With more flexibility in training between specialties, and availability of more generalist training schemes, those who feel they cannot make their final choice of specialty by 18 months after graduation would not have to do so.
Career advice provision
Over one-third of 2008 graduates agreed that making career choices has been made difficult by inadequate careers advice. This is a surprising finding, as since the introduction of the foundation programme, medical schools have made considerable efforts to ensure that career planning resources are available to junior doctors. Each deanery or foundation school has career advisors who offer personal advice, general career advice, and access to online career planning tools. Deaneries also run ‘taster’ sessions of 2–5 days spent in a specialty in which the foundation trainee has not previously worked. Also in July 2009 the NHS medical careers website (www.medicalcareers.nhs.uk) was re-launched to address the need for medical careers advice: the site is still running and appears to be regularly updated.
There have been some indications that, despite feeling that career advice is important, 5 junior doctors have not been taking advantage of all the career planning resources provided for them.14,15 Thus the next challenge, in this respect, for the medical schools and foundation trusts is to get juniors to utilize a wider variety of formal resources.
Changes in expectations
We found an increase in the influence on career choice of working hours/working conditions and domestic circumstances. This observation is not limited to UK doctors. Sondheimer, Association of American Medical Colleges’ senior director of medical education projects, wrote ‘The millennials seem to be more inclined than previous generations of physicians to trade some of their income for more control of their hours and an improved lifestyle’. 16 The importance of factors synonymous with our use of the terms ‘domestic circumstances’ and ‘work–life balance’ for the new generation of doctors has also been highlighted by research in Australia17,18 and Canada.19,20 These are unlikely to be incidental trends which will soon disappear. New generations of graduates do want it all – a successful career in medicine and time for personal life. Medical educators and workforce planners need to take into account this shift in medical students’ and junior doctors’ priorities and expectations. The implementation of the European Working Time Directive has already reduced the number of hours doctors can work. For the NHS, offering more part-time and flexible work and training opportunities is likely to be the way forward. There was some indication from our results that, when factors summarised as hours/working conditions and domestic circumstances become important influences to an individual after year 1, this might lead to change in specialty choice. Thus, finding solutions for allowing acceptable working hours and time for domestic commitments in all specialties is likely to result in fewer late choice changes.