
Abstract
In the early 1980s, Iraq was a middle-income and rapidly developing country with a well-developed health system. A few decades later – after wars, sanctions and a violent sectarian upsurge – child and maternal health indicators have deteriorated, its poverty headcount index is at 22.9% and diseases such as cholera have remerged. Today Iraq is beset by chronic political deadlock and a complexity of economic challenges; accordingly, all aspects of life are suffering, including health. Irrespective of the monumental investment to improve components of the health system, via national and international efforts, the health status of the population can only advance through resounding and synergistic effort in other aspects of life affecting health: the social determinants of health.
Introduction
Before the 1980 Iraqi-Iranian war, Iraq was a middle-income and rapidly developing country with a well-developed health system. The eight-year Iran–Iraq war was followed by the Kuwait invasion in 1990 and then the second Gulf war in 1991 resulted in 13 years of severe UN sanctions; the US–British Coalition military invasion in 2003 and subsequent unrest, sectarian violence and political rivalries. In that light, despite its once renowned repute for being one of the wealthiest and strongest countries in the region, Iraq and its people, over the last few decades, have suffered the penalties of a stagnant economy and restricted access to essential services due to successive wars, sanctions and sectarian conflicts.1,2
The Republic of Iraq is ranked by the World Bank as an upper middle income (UMI) country with a gross domestic product (GDP) per capita of US$3501. 3 Irrespective to the enormous amount of monetary investment over the past 10 years, the coalition and the successive Iraqi governments failed to win the hearts and minds of the Iraqi population. One reason is simply because they (successive governments) continuously fail to provide the basic needs 4 for the population: safety, shelter, food and water.
The health system in Iraq has been dissected and reviewed repeatedly, from various different approaches, and via national and international efforts,5,6 in attempts to come up with solutions that can aid the appropriate channelling of resources needed for a better functioning health system. But a health system cannot fit its purpose of serving its population, and positively affecting the health status of the people, if the social determinants of health7,8 are in the blind spot of strategists and planners. It is absolutely crucial for comprehensive and collaborative approaches, permeating all aspects of living, to see any results in the health conditions of Iraqis living in their country.
This paper aims to give an understanding of the current health and wider socioeconomic status of Iraqis living in their homeland, approximately 10 years after suffering the US-led invasion. We argue, while attempting to draw a distinctive picture, that massive efforts are needed in these areas to substantiate and support the strife for better health for all.
Methods
We adopted various approaches to objectively collect and analyse data on the living conditions in Iraq. This was done via triangulation, combining qualitative and quantitative narratives, in order to enhance confidence in our ensued findings.
The electronic online databases PubMed, Medline, Embase and PsychInfo and Google Scholar were searched using the terms ‘Iraq health’, ‘living in Iraq’ and ‘Iraq wars’, from 1980 to 2013, with no language restriction imposed. This was supplemented by iterative reviews of the reference lists of relevant published papers and searches of the grey literature, reports identified in references and reports to World Health Organization (WHO) from consultation projects. We further reviewed major international organisations documents (UN agencies, WHO, World Bank and non-governmental organisations), consulted Iraqi Government documents (including data on the economic activities provided by the Iraq Institute for Economic Reform) and WHO Iraq, as well as the UN work on Public Service Modernisation Project (which Imperial College London was part of) that focused mainly on public services such as water, electricity, education and health. Field visit by five researchers (SR, ED, SH, MR and HJ) from Imperial College London and Wayne State University to Basra in Southern Iraq (December 2011), Erbil and Suleymaniyah Northern Iraq (March 2012), Erbil (November 2012), Baghdad (5–9 December 2012) and Suleymaniyah (21–25 February 2013). Semi-structured interviews with officials and citizens from the 18 provinces of Iraq, and through observational assessments and visits to the markets, health organisations, educational institutions, citizen’s houses and recreational places.
Results
Health status
Iraq’s population is growing rapidly, today approximately reaching 32 million. 3 The population tripled between 1970 and 2007, and due to the high fertility rate (4.6 births per woman), it is forecasted that the population will reach 50 million by 2030. Approximately 50% of Iraq’s population is aged less than 19 years.9,10
The WHO estimates the average life expectancy for a male infant born in 2011 in Iraq to be 65.5 and for a female infant to be 72 years of age. 9 Although this is relatively similar to the Eastern Mediterranean regional average of 67 for men and 70 for women, the slightly lower figures can be attributed to the high death tolls due to the 2003 invasion and its consequences.11,12
The mortality and burden of disease in Iraq are not different from global trends; the epidemiological curve is shifting from communicable diseases to non-communicable diseases. However, like many countries in the region, Iraq is suffering from a double burden of disease. 13 The proportional mortality (percentage of total death in all ages) for non-communicable diseases account for 44%; communicable diseases including maternal, perinatal and nutritional causes account for 34%; and injuries account for 32%. 9
The maternal mortality ratio per 100,000 live births was 63 and the under-five mortality rate per 1000 live births was 38 in 2011. 9 Both rates are lower than the regional average of the countries of the Eastern Mediterranean, where the regional average for maternal mortality ratio per 100,000 live births is 250 and the under-five mortality rate per 1000 live births is 59.2. 10
With some geographical variations, security is the main problem Iraqis face today. Terrorist attacks, mainly targeting security forces, government buildings and markets, are regular daily features of living in Iraq. Checkpoints are present everywhere across Iraq, although this is less common in Northern Iraq – Kurdistan Regional Government (KRG).
Other than the KRG area, Iraq still suffers from violent and fatal attacks. Suicide bombers in Iraq kill significantly more Iraqi civilians than coalition soldiers. Among civilians, children are more likely to die than adults when injured by suicide bombs. 14 Between January and June 2013 alone, it is reported that an estimated 2800 have been killed as a result of recent violence in the country; these atrocities are only compounded by another ‘wave of violence in the country that has reached levels not seen since 2008’ in August which has taken the lives of 800 people.5,15,16
Security for the Iraqis does not merely mean safeguarding against road side bombs, improvised explosive devices (IEDs) and random shootings; it also means, now more than ever, concerns over arbitrary kidnappings of both adults and children. 17 These kidnappings have different aims; some are meant to finance terrorist groups and some are for trafficking of human organs. 18 There is lack of information on the actual numbers of children being kidnapped or the organised criminal cells behind them; however, it was reported that Baghdad city alone had witnessed the abduction of 72 children between 1 January 2009 and 16 October 2009. 18
Social determinants of health
Housing
The housing conditions in Iraq are in a dire state for the majority of the population. Nearly 500,000 people live in squatter settlements throughout Iraq; more than 200,000 are in Baghdad alone.19,20 The figures published by The Office of the United Nations High Commissioner for Refugees (UNHCR) showed that 48% were displaced and 46% were in host communities; this indicates that to obtain an adequate shelter is a challenge for both internally displaced people and host communities alike. 19 This issue has been additionally echoed by prominent economists and politicians in the country 21 flagging up that the government is disproportionally building approximately 25,000 housing units per year for a population that currently needs three million housing units. Undoubtedly, this has resulted in overcrowding and poor housing conditions, adversely reflecting on human health, and crippling efforts to combat communicable diseases such as tuberculosis.
Water and sanitation
Although most of the housing estates are connected to water and sewage networks, the infrastructure is too old, and indeed, it is a source of illness for many people. For example, in Basra, home to over two million people and the main source of oil, the water supply is not suitable for human consumption. 16 The residents of this rich city have to purchase water (the average cost of a 20 litre jerry-can is approximately Iraqi Dinar (ID) 250, i.e. $2.5) from distribution tanks in a very unhygienic way to be used for drinking and cooking; therefore, it is of no surprise to report high rates of water-borne infections such as diarrhoeal diseases and worm infections. 22
The impact of such poor conditions for water and sanitation in the country can be further portrayed by the clear example of consequent ineffective disease control measures as the re-emergence of cholera in the form of three country-wide outbreaks within five years (September 2007, August 2008 and October 2012). 23
Electricity
Over the past 10 years, Iraq has spent over $37 billion on improving its power supply. However, the national electricity supply is still limited to 40%, at its best, with exception of KRG area.
24
This forces the public to purchase electricity privately from local dealers or to buy a domestic power generator (Figure 1). In addition to its financial burden on families (adding costs between $50 and $250 per month per household), there are significant environmental implications such as local air pollution, land contamination, increased CO2 emissions, noise pollution, widespread smell of diesel and disturbing views of large dirty generators.
25
This is compounded by the lack of regulations and poor policies to monitor the effects on human health as well as political blunders over the matter. In a recent statement, the Prime Minister accused his deputy for energy affairs of providing him with ‘false figures’ on power capacity.
26
Generators are everywhere in Iraq: majority are run on a commercial basis at heavy costs to families and businesses (Courtesy: Rawaf
11
).
Transport and road safety
Years of conflict and sanctions resulted in neglecting the transport infrastructure in Iraq; therefore, the roads are in poor condition and not well maintained. The lack of working traffic lights, pedestrian crossings, road markings, road signs and speed limits makes it unsafe to drive both within urban cities and motorways. The situation has not improved following 10 years of US-led occupation. In fact, some argue, it has worsened due to roadblocks and copious checkpoints. The locals, as well as the very few expatriates (Figure 2), we met claimed that it felt like an intentional form of psychosocial warfare. Vehicle security checkpoints, dense urban populations and presence of protective concrete blocks (which encircles 70% of Baghdad) often cause significant traffic congestion. However, despite this restriction on vehicle movement, the road traffic injury (RTI) rates are still unacceptably high.
6
Figures revealed that the death toll from RTIs is four times greater than that of terrorism.
27
Moreover, there remains a threat of roadside IEDs, which randomly targets Iraqis in markets, cafes and worship places, in addition to government officials, army and police.
City traffic jams due to extreme security measures (Courtesy: Rawaf
11
).
Food and agriculture
Global food security is facing increasing challenges due to many factors such as rising food prices, climate change, desertification and drought. 28 In Iraq, the challenge is even bigger, despite the presence of Euphrates and Tigris as a nourishing source for farming; the Iraqi agricultural sector is not sufficient to cover the domestic market’s needs of essential food items. 23 Ten years after the invasion, this sector still suffers desperately from lack of infrastructure, modern technology and inadequate support to local farmers. Accordingly, the Iraqi markets are heavily reliant on imported food to meet the increasing demands of the population. 28
The majority of Iraqi families receive a monthly food supplement via the public distribution system (PDS), which was adopted by Saddam’s regime in 1991 in response to the UN economic sanctions. The PDS provides almost free basic food items to almost all Iraqis; hence, there are no shortages of food across Iraq, yet, the World Food Programme still estimates that 22% of children under five years are stunted due to chronic malnutrition in Iraq. 3 The government has recently failed to reform the system due to fierce resistance from the public. 29
Education
Iraq had a well-established educational system with literacy and enrolment rates reaching its best in the 1980s. However, the system witnessed a downfall, which started after the first Gulf war and UN economic sanctions in 1990. The educational facilities suffered from widespread looting and arson attacks in 2003, 30 which was exacerbated by the rapid deterioration in the security situation and the systematic assassination of Iraqi academics, resulting in a successive brain drain from the country. 31
The UN Educational, Scientific and Cultural Organization (UNESCO) statistics show that 78.5% of adults and 82.4% of youth are literate in 2011. 32 This is relatively lower than the regional figures; hence, the UNESCO launched a literacy initiative for empowerment (LIFE) in 2010; this was followed by parliament approval of the new Literacy Law to reduce illiteracy by 50% by 2015 in Iraq. 33
In the past 10 years, the Iraqi government allocated remarkable budgets to rehabilitate the educational system; however, institutional corruption hindered (and is still hindering) these efforts. 34
Microeconomics
The annual revenue is over $100 billion
35
; however, its economy is largely dependent on international oil prices. After years of international sanctions, Iraq’s economy is slowly recovering (Figure 3). Yet, still issues such as unemployment rates are unacceptably high in a well-resourced country; youth (15–24 years) unemployment is 18% (27% of women, 17% of men). The rates are higher in urban areas in comparison with rural areas
36
as well as for those with higher education.
36
Iraq: poverty line and distribution of average monthly expenditure (Adapted from Iraq National Strategy for Poverty Reduction).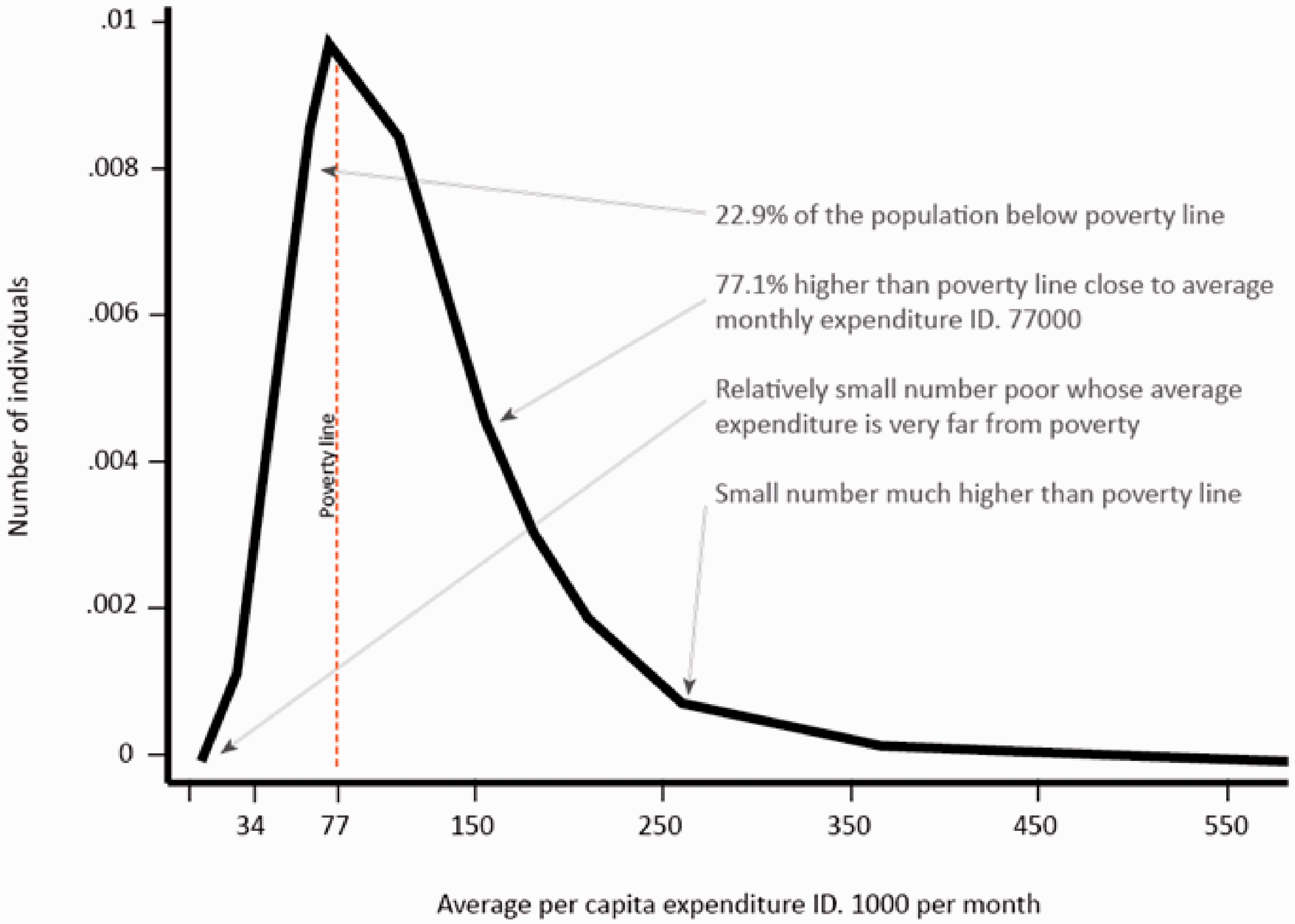
Iraq’s poverty headcount index is relatively high at 22.9% with a poverty gap of 4.5%. 37 The poverty levels vary considerably by governorate, with the highest poverty headcount index observed in rural Al-Muthanna at 74.7%.37,38
Consumer price index – Iraq 2009–2010 (Ministry of Planning and Central Statistical Organisation 2012).
In May 2013, Iraqi diplomacy successfully reached a resolution to remove Iraq from UN chapter VII mandate which is seen as a step forward to build a stronger economy; however, a relatively stable macro economy is not sufficient to ensure continued prosperity. 40 The lack of economic diversification makes Iraq’s economic growth vulnerable to oil price and volume shocks. This undermines its ability to conduct viable and sustainable fiscal policy. Economic diversification is, therefore, a challenge for the Iraqi government – both to create jobs and to promote income-creating opportunities for a majority of the Iraqi population. 41
Discussion
Marti Ahtessari, the UN Under-Secretary General, described Iraq in 1991 after the Gulf war as a rather highly urbanised and mechanised society. Now, most means of modern life support have been destroyed or rendered tenuous. Iraq has, for some time to come, been relegated to a pre-industrial age, but with all the disabilities of post-industrial dependency on an intensive use of energy and technology.
42
Living in Iraq today is not easy; nonetheless, it is not all doom and gloom. The monumental investment to improve the health system, via national and international efforts, is very promising but needs significant and equal contribution in other aspects of life affecting health and quality of living. Housing, water and sanitation, electricity, transport and road safety, food and agriculture, education and the economic stronghold of the country integrally affect people’s lives as has been demonstrated in our results, and so require multidisciplinary and multi-institutional cohesive effort to positively impact the population’s health.
Apart from the literature review, this work presents subjective findings of the day-to-day living in Iraq today. The researchers, to the best of their knowledge, attempted to reflect as clear of a picture as possible of the living conditions from their multiple visits and semi-structured interviews inside and outside Iraq. However, due to the descriptive nature of this work, we acknowledge that other aspects of living in Iraq today may have not been discussed.
Conclusion
The investment in health services is crucial to elevate the health status of the population. However, such an outcome will not be possible without similarly heavily investing to enhance the conditions of the social determinants of health; health and its status can only advance through mirrored efforts to improve the social determinants of health. And thus, through sustained sensible management and robust policies, Iraq’s abundant natural and human resource base can be a valuable source for the revival of its economy and coherent social structure. Iraq’s contribution to the regional development will be significant.