
Abstract
Objective
To assess the state of national health research systems of countries in the World Health Organization (WHO) African Region.
Design
A questionnaire-based survey
Methods
Structured questionnaires were used to solicit health research systems’ relevant information from key informants in each country.
Setting
Forty-six Member States of the WHO African Region.
Participants
Key informants from the ministry of health in each country, with the support of WHO Country Offices.
Main outcome measures
Presence of national health research policy or strategy, priority setting and ethical review of research.
Results
Of the 44 responding countries, 39 (89%) reportedly had an official national health policy and 37 (84%) had a strategic health plan. A total of 16 (36%) countries reportedly had a functional national health research governance mechanism, nine of which had clear terms of reference; nine (20%) countries had a functional national health research management forum. Functional ethical review committees were reported in 33 countries (75%).
Conclusions
National health research systems were weak in the countries assessed. Significantly more resources should be allocated to strengthening these systems.
Keywords
Introduction
Developing countries face several challenges in responding to the need for knowledge to inform decision-making. Collectively, these relate to the setting-up of effective national health research systems. 1 The World Health Organization (WHO) recognises health research as a major mechanism for disease burden reduction. One of the six core functions of the WHO is stated as ‘shaping the research agenda and stimulating the generation, translation and dissemination of valuable knowledge’. 2 This important role makes it all the more essential that countries should organise health research in strong regulatory systems that enhance the creation, dissemination, use and archiving of evidence.
A functional national health research system is important to generate, disseminate, use and archive health-related knowledge and ideas in published form (in hard copy, electronic or audio formats). 3 Furthermore, the national health research system can link knowledge generation with practical concerns to improve health and health equity. 4 Although there is an increasing interest and political will in countries in the WHO African Region to develop functional national health research systems, evidence on the status of such systems is rarely available and only a few surveys can offer a very partial overview of the systems at the regional level. There is a need to develop a more global view that could also serve as a baseline for measuring progress in further national health research system developments.
The current survey of national health research system status in the Region was commissioned by the WHO Regional Office for Africa and undertaken in preparation for the 2008 Algiers Ministerial Conference on Research for Health in the African Region. The main objective of this survey was to provide a baseline for assessing and eventually refocusing the implementation of the Algiers Declaration’s recommendations, 5 as well as to measure progress in other national health research system developments. Beyond the description of national health research systems, indicating their status in the Region at the time of adoption of the Algiers Declaration, the survey enables the assessment of the compliance of national health research systems with other regional commitments and declarations.
Methods
The methods to assess the national health information systems are described in detail by Kebede et al.
6
Countries were surveyed through a questionnaire adapted from a previous survey of its kind conducted in 2005,
4
peer-reviewed by the research team from the Regional Office. Topics covered were in line with earlier recommendations and with the four operational components proposed by Pang et al.
7
for an effective national health research system stewardship function. These were:
Definition and articulation of a vision for a national health research system Identification of appropriate health research priorities, and coordination of adherence to them Setting and monitoring of ethical standards for health research and research partnerships Monitoring and evaluation of the national health research system itself
In addition to the stewardship function, we also surveyed the financing function of national health research systems, to describe how research funds were secured and if they were allocated accountably.
The questionnaire contained mostly close-ended questions and very few open-ended questions. These were grouped into seven categories inquiring on:
Health research policy – any national document that describes the national policy adopted as regards health research. Questions referred to the existence of health research policy documents, their content and settings Health research legislation – any official law or documented decision that rules the implementation of health research in the country Strategic health research plan – existence of a strategic health research plan to implement the policy and its setting Research coordination mechanisms – existence of a national health research system, national health research forum and scientific or other deontological body, and their settings Health research programme – existence of a health research programme and its setting Health research financing and budget – estimation of total budget/expenditure dedicated to health research when existing, and analysis of funding source. Respondents were asked to rank the different funding sources from the most important contributor to the least important Ethics review – existence of ethical review committees and their settings
To set the context, the first questions were on the existence of policies and strategic plans. By national health policy, we meant a national document that set the national visions and orientations of the health system development in the country. Information was also sought on the strategic health plan, another key document of the health system that describes the priority actions to be taken and the framework for implementation of the national health policy, including the activities and provisional budget to achieve it.
The questionnaire was emailed to the focal points for research at WHO Country Offices who then met with the appropriate key informant counterpart at the country’s ministry of health to introduce the questionnaire and provide explanation and guidance for its effective completion. Once the questionnaire was understood, the key informant responsible for health research at the ministry filled the questionnaire with the appropriate responses and returned it to the WHO Country Office with reference documents where applicable. After a first checking by the WHO country team, the package was forwarded to the research team at the Regional Office.
Data were processed in a Microsoft Excel spreadsheet and basic descriptive and comparative analysis was carried out both with Microsoft Excel and IBM® SPSS® Statistics software. When required, some data were categorised. The ideal term for all strategic documents was considered to be five years. Owing to the time available to validate national financing figures, we considered ministry of health financing figures from the years 2001 and 2002. Financial amounts were given in local currencies and translated into United States dollars (US$) through the fxtop currency website. 8
Results
The results included responses from 44 of the 46 countries in the Region that were sent the survey questionnaire (response rate = 96%) (subsequent to the research described in this paper, South Sudan joined the WHO African Region by World Health Assembly Resolution WHA66.21, bringing the total number of countries to 47). For ease of analysis, the results are presented through five headings and calculated in percentage among respondents.
Health and health research policies and strategies
The availability of national strategic documents varied significantly according to the type of document (Figure 1). A total of 39 countries (89%) reportedly had an official national health policy and 37 (84%) had a strategic health plan. Furthermore, 13 countries (30%) reported the existence of an official health research policy (of which, seven had been implemented and six needed updating) and eight countries (18%) had a strategic health research plan. In 2008, most of the periods covered in the strategic plans were out of date, except for those of the Gambia (2008–2012) and Zambia (2007–2010). All of the eight countries that reported having a strategic health research plan said that they needed technical and financial support from WHO to update their plans; two of these countries (United Republic of Tanzania and Zimbabwe) did not have a health research policy.
Availability of national strategic documents relating to health research in 44 countries in the WHO African Region, 2009.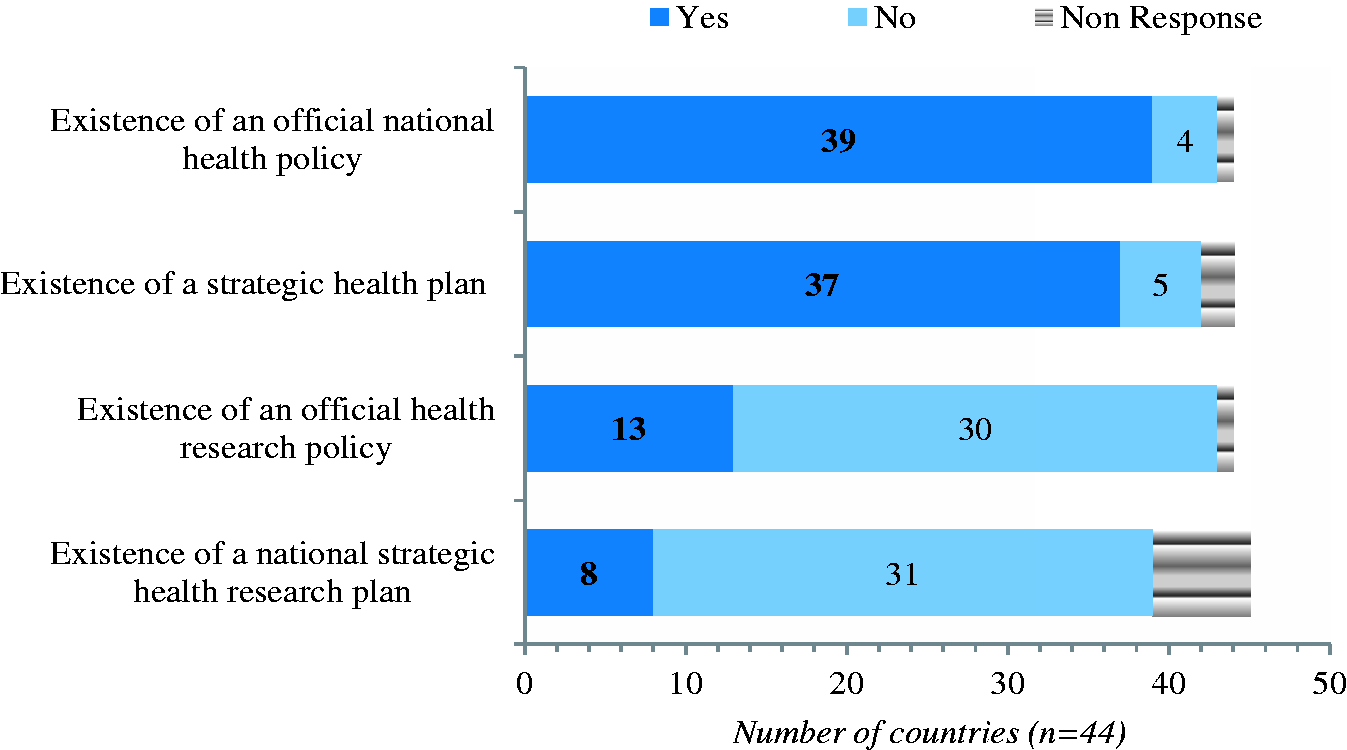
Analyses revealed that the Comoros was the only country that lacked all four of these strategic documents. Eritrea had a health research policy but no national health policy, and the United Republic of Tanzania had only a strategic health research plan but none of the other three documents. Twelve countries (27%) had only three of the documents (a national health policy, health research policy and strategic health plan), and all except Seychelles reported having complementarity between a national health policy and a national health research policy. Eight countries (18%) had developed all four documents. Ten of the 13 countries that had developed a health research policy initially formulated it between 1999 (Ghana) and 2009 (Benin, Zambia); five of these formulated theirs after 2006 (Benin, Eritrea, Lesotho, Mozambique, Zambia).
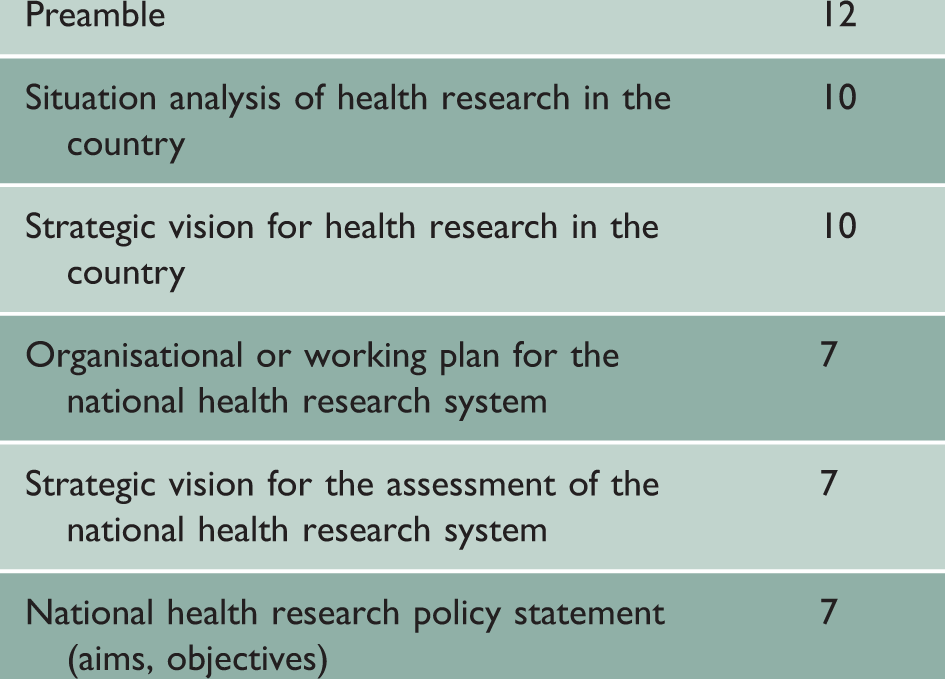
Characteristics of the health research policy documents in 13 countries of the WHO African Region, 2009.
Of the countries that did not have a health research policy, 25 were ready to develop one. Altogether, 39 countries (89%) reported needing support from WHO in developing or improving their health research policy. Of these 39 countries:
34 (87%) needed technical support to draft their health research policy 33 (85%) needed guidelines on formulating a national health research policy 33 (85%) needed financial support for undertaking a health research situation analysis 34 (87%) needed technical guidance in the development of grant proposals 31 (79%) reported needing technical support to identify evidence-based priorities 28 (72%) needed technical support for the application of health research policy.
Of the 39 countries, 35 (90%) expected WHO to help them to share experiences and lessons originating from countries with a health research policy. All of the 39 countries expressed the need for WHO support on human capacity development for implementation of health research policy.
Research coordination mechanisms
Of the 44 responding countries, 16 (36%) reportedly had a functional national health research system, nine of which had clear terms of reference; nine (20%) had a functional national health research management forum, almost all of them having clear terms of reference (Figure 2). Only eight countries (18%) had guidelines on development of collaborative agreements on health research involving health institutions and agencies outside the country, questioning the alignment of research priorities to country needs. Of the 11 countries (25%) that had a health research programme, the earliest was constituted in 1943 and the latest was just being developed. Nine of the national health research programmes had clear terms of reference, of which eight had a mission statement, a clearly defined organisational structure and a developed plan of action. Almost all of these programmes were connected to the Internet, operated using email, and were hosted within the ministry of health or an associate institution.
Availability of national coordination mechanisms related to health research in 44 countries of the WHO African Region, 2009.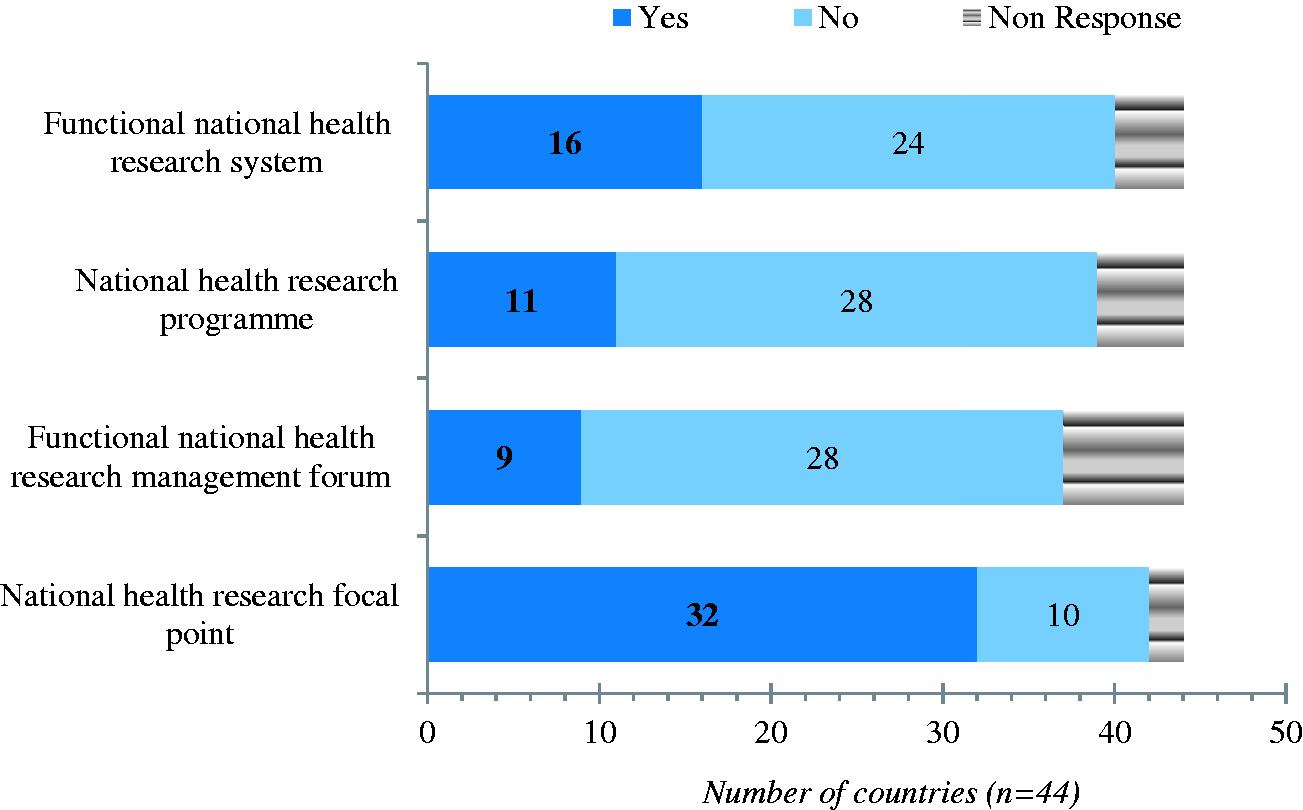
Development of health research plan
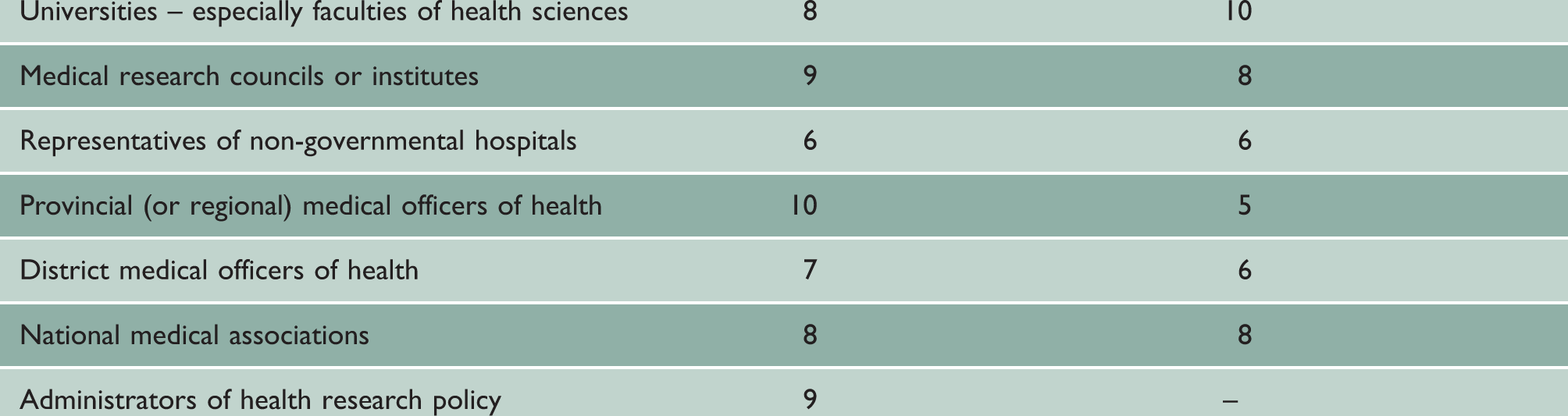
Stakeholders involved in the process of formulating a health research policy documents in 13 countries of the WHO African Region, 2009.
Health research legislation and ethics
Functional ethical review committees were reported in 33 countries (75% of the 44 countries reporting), although one-quarter of these had no written terms of reference (Figure 3). According to the survey, in only 15 countries (34%) were there hospitals with ethical review committees to review all clinical research proposals; 22 countries (50%) had a national scientific review committee, while 24 countries (55%) reported having health institutions with an institutional review committee.
Availability of national legal, ethical and scientific regulatory mechanisms in 44 countries in the WHO African Region, 2009.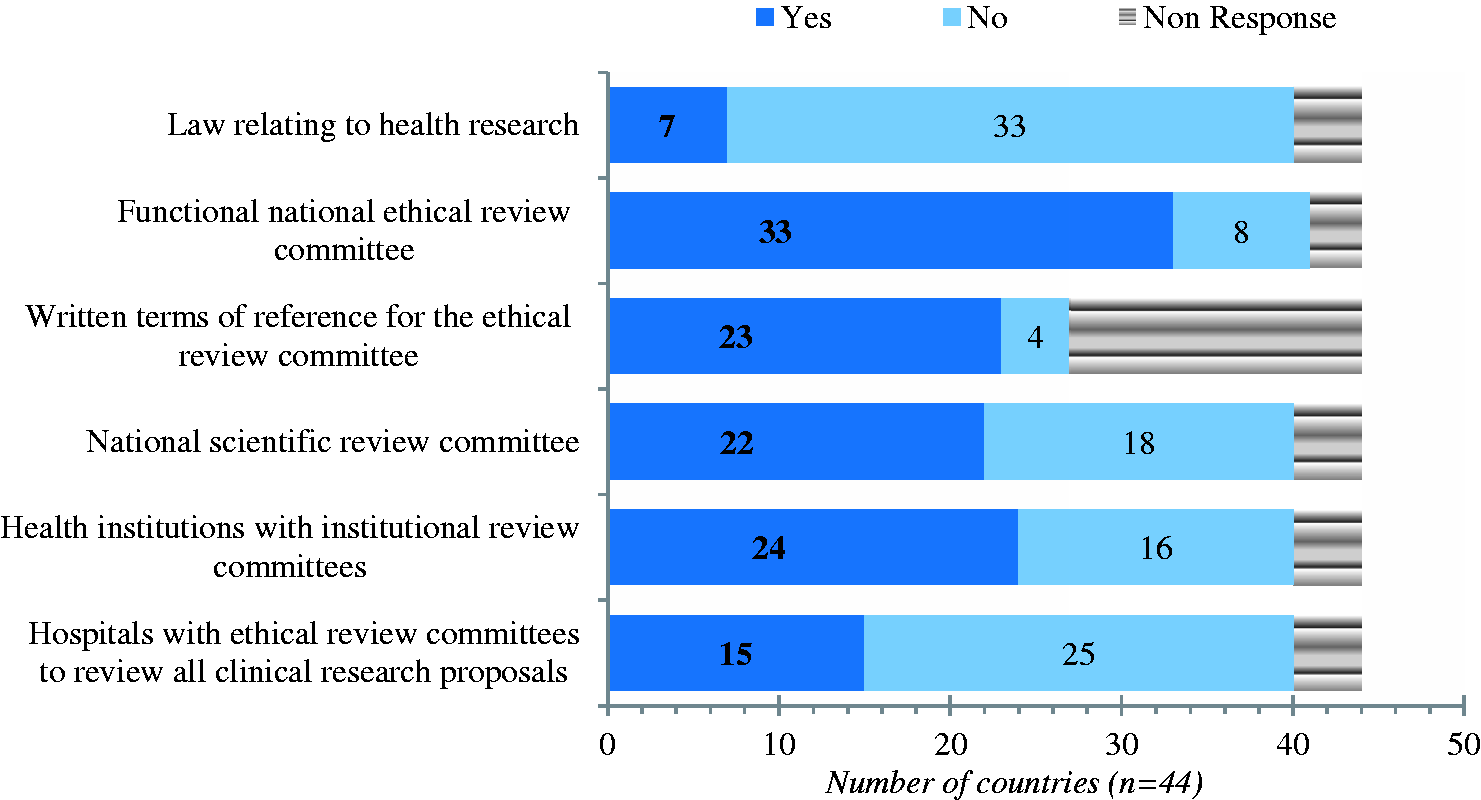
Seven countries (16%) had a law relating to health research, of which the oldest was enacted in 1965 (Lesotho) and the most recent in 1993 (Eritrea). Six of these countries’ laws included ethical concerns. Where no ethical review committee existed, there was some form of regulatory body. This was embodied either through the scientific review committee or through ministerial, institutional or hospital ethical committees, which met whenever there were projects to review. However, four countries had no ethical or scientific regulatory body at all, while two countries (Liberia, Mauritania) had independent mechanisms in place for clearing ethical issues in research.
Most of the countries’ ethical review committees met either on a monthly basis or just whenever there were projects to review (Figure 4). Where there was only an institutional regulatory body or just an independent mechanism for ethical concerns, a committee was organised whenever there were projects to review. In addition, in some of the countries where ethical review committees met on a regular basis (e.g. Angola, Mali), they also met on demand. In the year preceding the survey, the national ethical bodies in 22 countries met on average 6.8 times (almost bimonthly), the frequency of meetings varying from zero meetings in the whole year to monthly meetings.
Annual frequency of ethical review committee and scientific review committee meetings in 44 countries of the WHO African Region, 2009.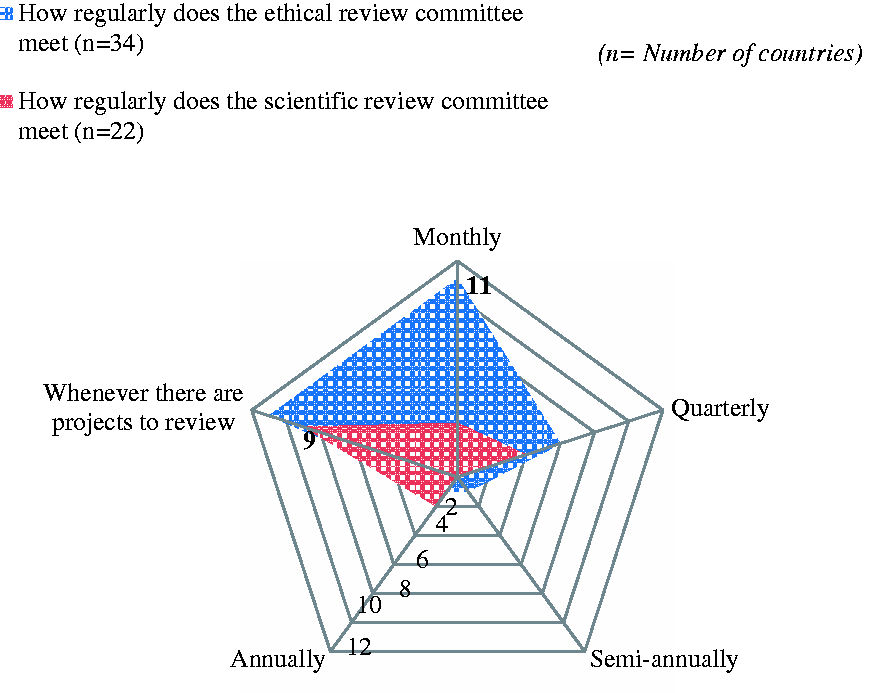
A total of about 1455 reviews and proposals were reported by 20 countries as being considered each year by the national ethical review committees, which corresponds to an average of 72 reviews or proposals per country per year, ranging from a minimum of three reviews or proposals per year in Seychelles to a maximum of 600 in Kenya. Six of these countries (30%) considered less than 10 reviews and proposals each year, while 14 countries (70%) considered 10 or more. The percentage of repeats or resubmissions of reviews and proposals averaged nearly 35% per country (0–100) (n = 17 countries).
Eleven countries (n = 22) had another national body (e.g. university or government agency) reviewing the proposals before or after the national ethical review committee, and mechanisms for clearing ethical issues in research were in place in three of the 10 countries where no ethical review existed (Chad, Liberia, Mauritania).
Analysis of ethical review committees in 24 countries showed that the number of committee members varied from 5 to 37, with an average of 12 members per committee. In most of these countries, membership included representatives from the health professions (with a minimum of one physician), legal or professional ethics associations, religious bodies and the scientific community (research institutions, universities). Some committees also included representatives from civil society, human rights associations and non-governmental organisations.
Health research funding
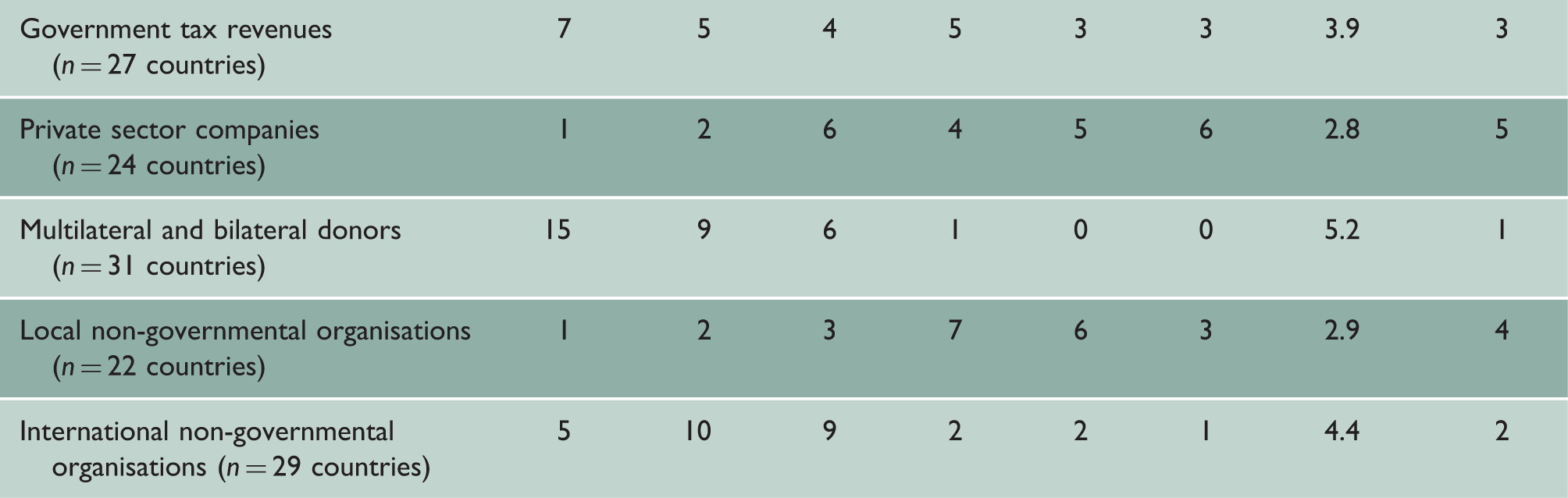
Relative importance of the source of health research funding in 44 countries of the WHO African Region, 2009.
Only 16 countries provided information regarding the amounts of money allocated to health research in 2001 and 2002. Seven of these countries provided figures, four countries reported no funds allocated, and five countries lacked data in this regard. Of the seven countries that provided figures, one reported to have allocated 5% and 7% of the overall ministry of health budget to health research in 2001 and 2002, respectively, while another allocated 2% in both years. The other five countries showed very low percentages (<1%) allocated.
The total amount of the ministry of health budget reportedly increased in six countries. The global percentage allocated to health research for these six countries was 3% in 2001 and 3.6% in 2002. A comparative analysis of figures from these six countries in 2001 and 2002 revealed that the total amount of money allocated to health research increased by 52% (from US$ 14,941,995 to US$ 22,750,179), while the total budget of the ministry of health of these countries increased by 27% (from US$ 498,708,619 to US$ 635,491,313).
Discussion
Despite the recommendations of several meetings and summits, endorsed by the 58th World Health Assembly 9 in 2005, urging countries to develop health research policies and plans, very few countries had developed such policies by 2008, although most of them had national health policies and plans. An explanatory assumption is that most of the national health policies and plan documents included a section on health research. The concern raised by this pattern is the difficulty in covering such a vast and important area as health research in only a section in a document, although most of the health research policies covered important areas of health research systems. Nevertheless, an encouraging finding is the strong will of most of the countries to develop or update their health research policies and their expressed need for support from WHO in this area.
Given this absence of guiding documents for national health research systems, it is not surprising that only one-third of the countries had a functional national health research system and only 20% of countries had national health research management forums. It illustrates the weakness of countries in putting in place concrete mechanisms to identify appropriate health research priorities. Moreover, the absence of guidelines on the development of collaborative agreements on health research involving health institutions and international agencies in 31 countries may imply that research priorities would be less in line with the needs of these countries and more influenced by the demands of external agencies or countries.
Health research legislation can provide a conduit for attention to research ethics and is a key component of research ethics governance. According to the survey, only a very few countries have legislation relating to health research, almost all including attention to ethics. This finding is similar to an earlier report by Kirigia and Wambebe 4 in 2006, in which only one out of 10 countries had legislation related to health research, and reflects the challenge in this area.
Health research at both national and international levels should be guided by clear, ethical principles. 10 Health research ethics has been acknowledged as a major concern for countries in the Region, as expressed during the 51st session of the WHO regional committee for Africa in 2001. 11 Showing efforts made by countries to address that issue, some recent surveys revealed an increasing number of national ethical review committees. While in 2003, 10 out of 28 countries in the Region (36%) reportedly had a research ethics committee, 12 six out of 10 countries reported a functional national ethical review committee in 2006. The present findings confirm the upward trends in establishing national ethical review committees. A regularly updated list of regional ethical review committees and scientific review committees is now available online. 12
Ethical review committees need to meet regularly to update their requirements according to the constantly changing scientific environment. However, our finding showed that ethical review committees met on a monthly basis in only 11 countries (32%). Moreover, some countries had ‘decentralised’ structures of ethics review, with no national ethics committee but ethical review committees located at the institutional level. This pattern is also found in countries in other regions, such as Japan. 13 However, important considerations with this type of model are whether these committees operate in a ‘stand-alone’ capacity without overarching guidelines or regulations, and how consistent their operating procedures are. Incidentally, most of the countries that reported not having a national ethics review committee appear to have an ethical or scientific regulatory body, except for four countries.
Monitoring and evaluation mechanisms of health research system are missing in many countries. Although 50% of the countries have national scientific review committees, these are less prevalent in countries than ethical review committees. A total of 13 countries that reported an ethical review committee did not have a national scientific review committee. Seven countries (16%) had a policy document that included a strategic vision for the assessment of the national health research system.
Public authorities in many countries are increasingly funding research and show interest in what comes from their funding. 14 However, health research funding in countries in the Region is still mostly provided by multinational or binational donors and international non-governmental organisations, which may sometimes create an influential and conflicting environment with national strategic orientations. Although 18 countries recognised the importance of having a budget line for health research in the ministry of health budget document, and 11 countries provided the amount of money allocated by the ministry of health to research in 2001 and 2002, only two of them aligned with the recommendation by the Commission on Health Research for Development to allocate at least 2% of national health expenditure on research and research capacity strengthening. 15 Nevertheless, results show an increase in the budget allocated to health research over the years.
Although this study is one of the few that has attempted to include most of countries of sub-Saharan Africa, it has some limitations that warrant caution in the interpretation of the results. The findings are based on a key informant study and not on a quantitative survey. The responses are dependent on the subjective opinion of the key informant, rather than based on actual interviews of institutions using standardised questionnaires. Thus, comparison of results between countries could be problematic. The study did not address issues related to the physical and human resources available to research, or the outcome and use of research results – two important components of the health research system.
Conclusions
The difficulty in gathering data and the unavailability of some key national health research system data clearly show how the vision of health research as a system is less developed in African countries. Indeed, a functioning system cannot exist without a clear definition of the vision, strategies, financing and ethics; this thus asserts the importance of developing national strategic documents. It clearly appears from this survey that additional efforts are required to develop or improve health research policies, plans and systems. Mobilisation and harmonisation of international partners to support countries will certainly be an asset.