
Abstract
Drug fever is overlooked. We aim to remind clinicians to consider drug fever as a differential after eliminating other causes.
Case
A 45-year old woman presented to our hospital with one-week history of intermittent fever, left flank pain, rigours, urinary symptoms and worsening right knee pain. A month before presentation to the hospital, she had an elective revision of her right knee hemiarthroplasty with placement of new prosthesis due to worsening right knee pain. Postoperatively, she had fever on various occasions with raised inflammatory markers and neutropenia. Two out of the three perioperative tissue samples obtained at hemiarthroplasty revision grew coagulase-negative staphylococci. She was discharged with a peripherally inserted central catheter line (PICC) for a three-month course of intravenous Teicoplanin and oral Rifampicin. Her symptoms improved initially but her fever recurred 10 days later prompting referral to our department.
On examination, she was febrile (38.5℃), with a blood pressure of 131/95 and a respiratory rate of 19 and a heart rate of 90 beats per minute. She had local tenderness in the left loin, three splinter haemorrhages on her peripheries but no murmurs were heard. Her right knee was warm, swollen and tender but she was able to move her knee joint. All other examinations were normal. Her C-reactive protein level was 127 mg/L, her white cell count was 11.4 × 109/L and her neutrophil count was 2.38 × 109/L.
Chest radiograph and abdominal ultrasound showed no abnormality. Her transthoracic echocardiogram showed no evidence of vegetation. Her PICC line was removed and showed no growth. Initial urine dipstick was positive for leucocytes but negative for nitrites. Urine culture grew Escherichia coli and one of the blood cultures grew coagulase negative streptococci at 48 h. Treatment with intravenous Co-amoxiclav was started for presumed pyelonephritis. Teicoplanin and Rifampicin were continued. After 48 h, her temperature remained in the range of 37.6–38.3℃ with occasional spikes to 39℃ (Figure 1).
Graph showing the temperature and pulse rate of the patient during this admission.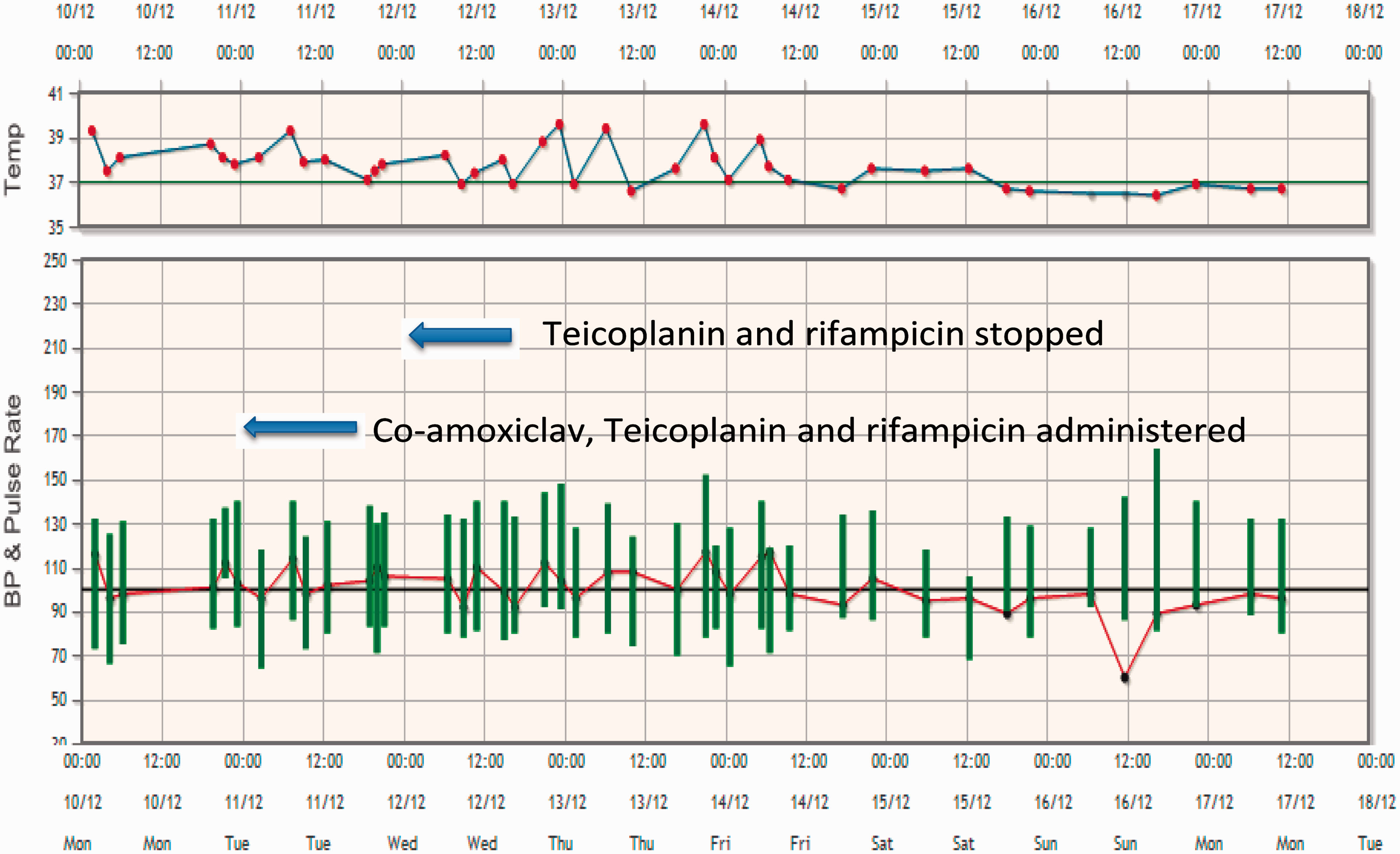
The patient was treated with Co-amoxiclav for pyelonephritis. Even though the patient looked well, her C-reactive protein level continued to rise (Figure 2). A synovial fluid aspirate showed scanty pus cells and no growth at 48 h. The orthopaedic surgeon felt that local symptoms were related only to recent surgery not to a new knee infection. Drug fever was suspected because the patient had remained febrile despite a repeat normalised midstream urine culture. This was discussed with the microbiology consultant and both Teicoplanin and Rifampicin were discontinued on day 3 of admission.
Graph showing the level of C-reactive protein (mg/L) during this admission.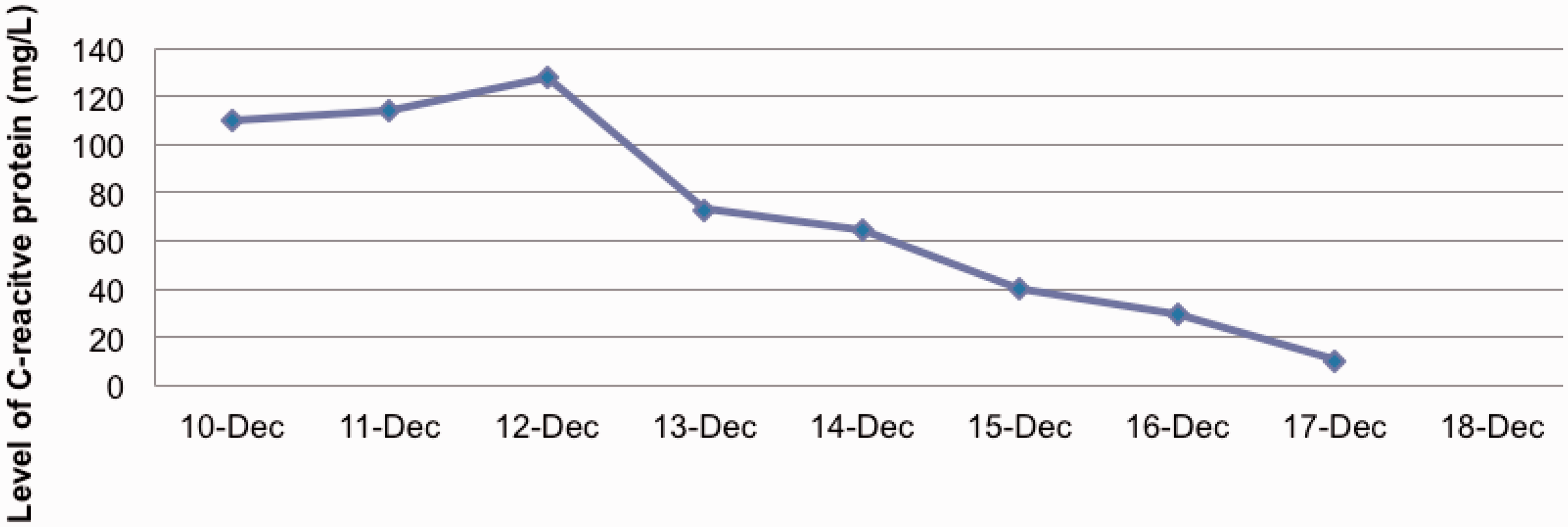
Treatment and outcome
The patient recovered when both Teicoplanin and Rifampicin were discontinued. Her inflammatory markers and white cell count started to normalise but she remained pyrexic for 3 days after discontinuation of Teicoplanin and Rifampicin (Figure 1). The patient declined further inpatient investigations and was later discharged from hospital with a 14-day course of Co-amoxiclav. She remained well.
Discussion
Drug fever is characterised by a febrile response coinciding temporally with the administration of drug in the absence of any other conditions that may cause fever. 1 The single consistent characteristic of drug fever is the resolution of the febrile reaction when the responsible agent is stopped. It is frequently misdiagnosed since temperature is one of the parameters we associate with infectious disorder.2,3 The fever may arise from the drug's pharmacologic action, its effects on thermoregulation, a local complication following parenteral administration or an idiosyncratic response. 1
The key to diagnosing drug fever in any patient is to consider it in situations when fever does not correspond with the likely infection. The median time from the initiation of a causal agent to the onset of fever ranges between 5 and 10 days.4,5 Longer interval times were seen with other agents. The clinician must not assume that the patient will not develop fever just because he has taken the medication for more than a month.4,5 Drug fever may have any pattern; with fever that typically resolves within 48–72 h; depending on the type of agent, its elimination rate and the patient’s co-morbidities.1–3 Patients are usually disproportionately well and may lack the tachycardia that typically accompanies an elevated temperature. Individual reaction ranges from maculopapular rash, bronchospasm to facial swelling. Other findings include normocytic anaemia and an elevated erythrocyte sedimentation rate that are not helpful in narrowing the differential diagnosis.1,4
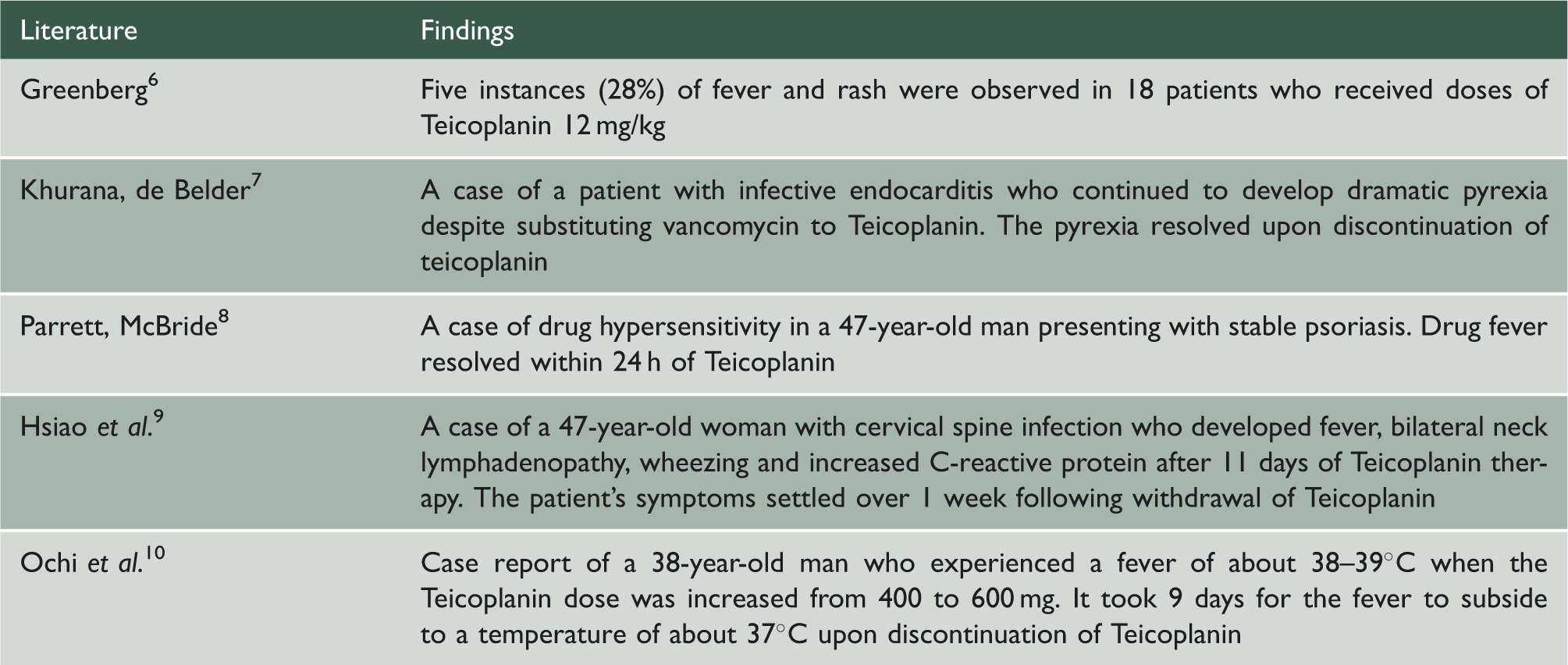
A summary of the various case reports.
Learning points
In our case, while we cannot say for sure if infection is responsible for the patient’s symptoms, drug fever is certainly one differential that we should not exclude. We want to remind clinicians to keep this diagnosis in mind after elimination of other potential causes of fever of unknown origin.