
Abstract
Sarcoidosis should always be part of the differential diagnosis when faced with a young patient with significant cardiac conduction disease.
Introduction
Sarcoidosis affects multiple organ systems, including the lung, skin, lymph node and eye. Cardiac manifestations of sarcoidosis are infrequent but are associated with increased mortality rates. 1 We present a case of symptomatic high-grade atrioventricular (AV) block in a young patient that resulted in a diagnosis of sarcoidosis as the underling pathology.
Case presentation
A 45-year-old farmer presented with a 10-week history of dyspnoea and decreased exercise tolerance. The patient was normally fit and well. No prior cardiovascular disease was noted and no symptoms of fevers or night sweats were described, although a history of systemic lethargy and malaise was noted. There were no complaints of eye problems or skin rashes. The patient was taking no medication and denied any herbal, over-the-counter or illicit drug use.
On examination, his blood pressure was 120/65 and had a heart rate of 40 b.p.m. Cardiovascular examination revealed cannon A waves at jugular venous pressure (JVP), but no audible murmurs or added sounds. There was no evidence of erythema nodosum or tick bites, and a thorough external examination revealed no peripheral lymphadenopathy. Chest auscultation was unremarkable, with good bilateral air entry. Abdominal examination revealed a palpable liver edge, but no splenomegaly, and a soft, non-tender abdomen with normal bowel sounds. A chest X-ray showed prominent hilar lymphadenopathy. A 12-lead ECG revealed complete heart block (CHB) with complete dissociation of the P waves from the narrow QRS complexes (see Figure 1). The full blood count, cardiac enzymes and inflammatory markers were within normal laboratory ranges. Echocardiography revealed a structurally normal heart. The patient was on cardiac telemetry for 48 h all of which demonstrated CHB and no other arrhythmias.
(a) Chest X-ray showing prominent peri-hilar and parenchymal nodularity; (b) ECG taken on admission, demonstrating complete heart block.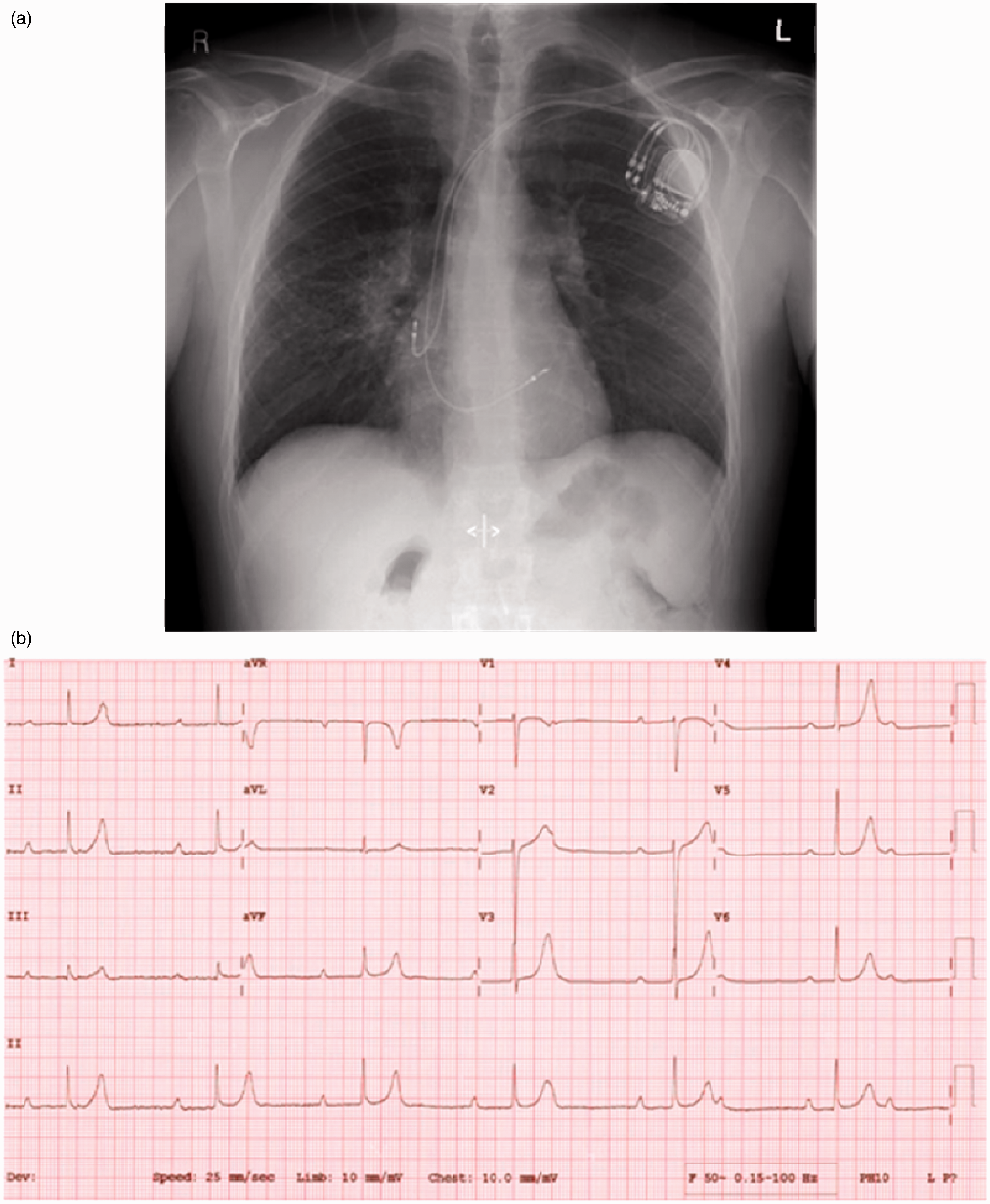
The presence of a high-grade AV block in a young patient prompted further investigation. Biochemical investigation revealed an elevated serum ACE level but normal calcium levels. Renal, liver and thyroid function tests were normal, as was Lyme serology. Given the abnormal chest X-ray, a thoracic and abdominal CT scan was performed which revealed peri-hilar and mediastinal lymphadenopathy, with extensive nodularity across the right middle and lower lobes, and further scattered nodules throughout the lungs (see Figure 2). The differential diagnosis included sarcoidosis or potentially lymphoma.
(a) CT thorax/abdomen, demonstrating peri-hilar and mediastinal lymphadenopathy and extensive nodularity; (b) Mediastinal lymph node biopsy demonstrating extensive replacement of lymph node tissue with non-caseating granulomas.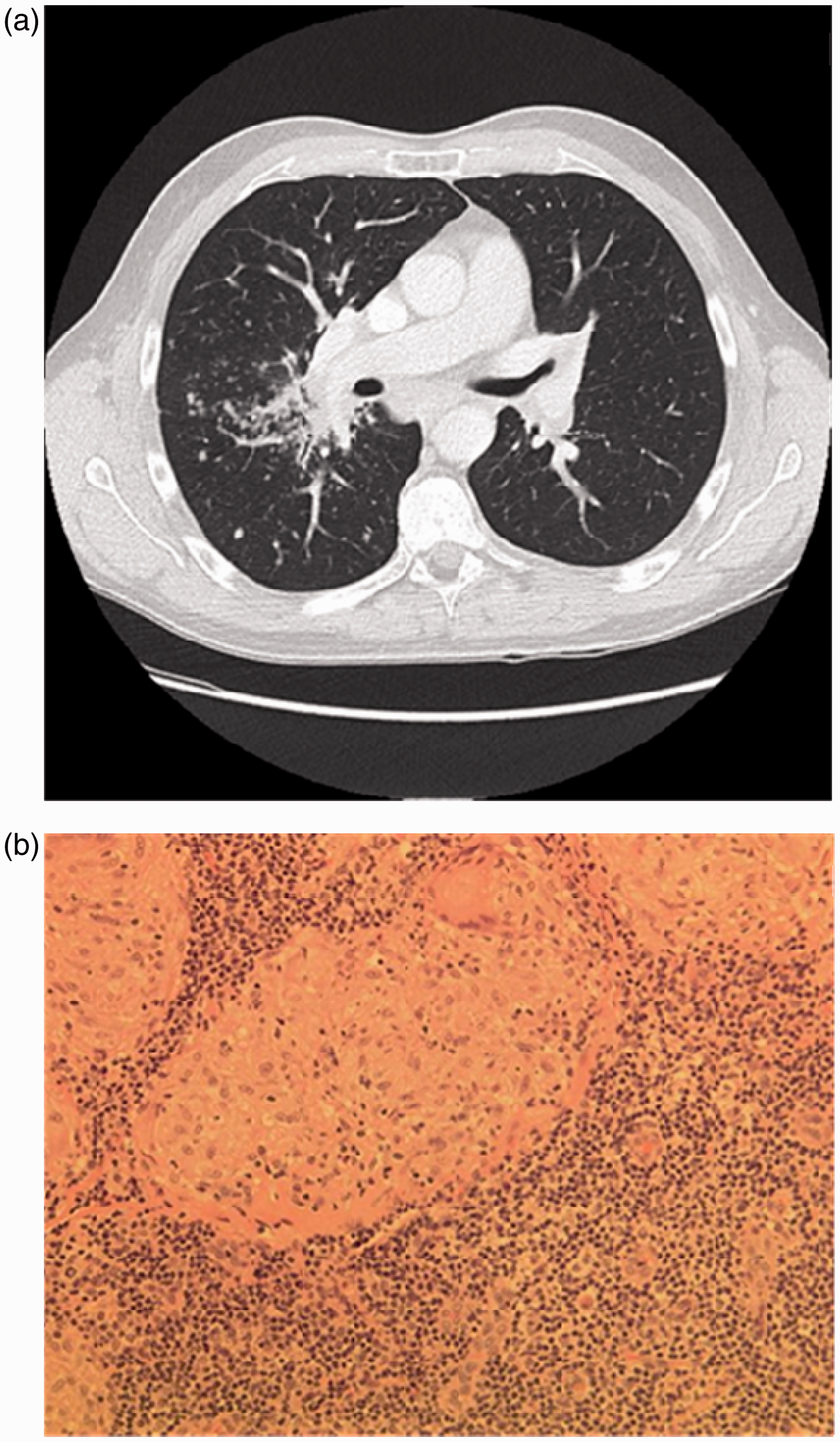
The patient was transferred to the regional cardiothoracic unit. The patient had a permanent pacemaker implanted for the CHB. Subsequently, he underwent a video-assisted thoracoscopic surgery mediastinoscopy with lymph node biopsy. Histology of the lymphoid tissue showed almost complete replacement by granulomas, with no caseation (see Figure 2). These features were consistent with a granulomatous lymphadenopathy and confirmed sarcoidosis.
Discussion
Sarcoidosis is a multi-system granulomatous disorder that exhibits non-caseating granulomas in involved organs. 2 Pulmonary, skin, eye and central nervous system and lymph node manifestations are well documented, but cardiac involvement in sarcoidosis is less recognized. 1 Only 40–50% of patients with cardiac sarcoidosis at autopsy are diagnosed ante mortem. 3 Clinically detectable manifestations of cardiac sarcoidosis are present in only 5% of patients. 3 Making an early diagnosis of cardiac sarcoidosis can lead to better clinical outcomes, but this is often quite difficult. In 2006, the Japanese Society of Sarcoidosis and Other Granulomatous Disorders published revised guidelines for the diagnosis of cardiac sarcoidosis to aid our diagnostic approach. 4 Cardiac magnetic resonance imaging (MRI) is becoming more available and has become the imaging of choice for the evaluation and diagnosis of cardiac sarcoidosis because of its high spatial and soft tissue resolution. 5 Cardiac MRI, with use of gadolinium, can demonstrate area of scar and/or myocardial oedema, particularly in the active stage of cardiac sarcoidosis.
Cardiac manifestations of sarcoidosis can be a significant cause of mortality being responsible for about 85% of deaths in such patients. 6 CHB, bundle branch block, ventricular tachyarrhythmia and congestive heart failure are among the clinical manifestations, and sudden cardiac death can be the first presentation. 7 Granulomatous deposition and the resultant cardiac fibrosis can also lead to significant mitral regurgitation secondary to papillary muscle involvement and dysfunction. Pericardial involvement is often found at autopsy but clinical pericarditis however is not. CHB has been found in 23–30% of patients with myocardial sarcoidosis, with bundle branch block in 12–32%. 7 Early identification and intervention in such patients is important. Often, however, sarcoidosis is not considered in patients presenting with CHB therefore causing a delay in the management of the underlying pathology.
Sarcoidosis should be considered in patients presenting with significant AV block, particularly in younger patients. Lenegre-Lev syndrome can cause idiopathic fibrosis and calcification of the conduction system and valves, leading to CHB. 6 The European Society of Cardiology (ESC) recommends permanent pacemaker implantation for symptomatic and asymptomatic patient with CHB which has prognostic benefits. 8 It is important to treat reversible causes of AV block before the decision for permanent pacing is made. Finally, there are a number of small uncontrolled trials demonstrating the some benefits of glucocorticoids in the treatment of cardiac sarcoidosis.9,10 However, because many patients present with congestive heart failure, the usual side-effects of steroids (weight gain, increase risk of infection and possible exacerbation of heart failure) may preclude its use. The prognosis of cardiac involvement is worse compared to other manifestation of sarcoidosis. About 80% of deaths due to sarcoidosis is from cardiac involvement either from congestive heart failure or sudden cardiac death.