
Abstract
This is the fifth in a series of articles on leadership in international health. The series was coordinated by Kent Buse.
The Department for International Development (DFID) is the UK government department that manages UK assistance to poor countries. Since 1997, with the formation of the Labour government, it has been headed by a cabinet minister and has a separate identity to the UK Foreign and Commonwealth Office. In line with Labour party policy, DFID has made tackling poverty and equitable pro-poor growth the cornerstone of its organizational policy. All three White Papers (statements of government policy) that have been published since DFID came into existence place an emphasis on poverty elimination.1-3
The UK government is also a strong proponent of the Organization for Economic Cooperation and Development's (OECD) Development Assistance Committee's (DAC) views on what makes development assistance most effective. 4 In both policy and practice, DFID upholds the principles of aligning its support with the policies and plans of the countries it is assisting, and of trying to encourage all donors to harmonize their actions to reduce transaction costs for developing country governments. The most recent DFID White Paper, Eliminating World Poverty: Making Governance Work for the Poor, 5 provides a clear indication that this continues to be the main direction of travel for UK aid. One of the main pillars of DFID policy is to ‘help to build states that work for poor people.’ This means increasing the focus on good governance within these countries while also ensuring that UK aid can be channelled in more effective ways through government systems. DFID has also been a strong advocate for multilateral organizations (such as the United Nations, the European Commission and various regional bodies), and of public-private partnerships (such as the Global Fund to Fight AIDS, TB and Malaria).
The UK government has been steadily increasing its funding for development assistance over the last few years. In financial year (FY) 2005/06 DFID's budget was £4.5 billion, with plans to increase this further to £5.3 billion by FY 2007/08. In FY 2005/06 approximately £2.5 billion was spent on programmes in developing countries through DFID's bilateral aid programme: 45% of DFID's bilateral assistance was spent in Sub-Saharan African countries, with 38% spent in the Asia region. A further £1.67 billion was spent through various multilateral organizations, including the European Commission, with a particularly sharp increase over the previous year on spending for improving the effectiveness of multilateral organizations (primarily the United Nations organizations and various international financial organizations). The European Development programme received the largest part of DFID's multilateral assistance, at £917 million. 6
With regards to health and other public services, the 2006 White Paper has also stated that DFID should, ‘help people have security, incomes and public services.’ 6 The UK government proposes to ‘commit at least half of all future UK direct support for developing countries to public services, to get children into school, improve health care, fight HIV and AIDS, provide clean water and sanitation … and agree ten year commitments with developing countries to do this’ (xii). Taken together with UK government ambitions to substantially increase UK development assistance, this could be good news for public health in the developing world. Unfortunately, unlike the situation in both education and water and sanitation, where the DFID White Paper is explicit about how much each sector will receive from the UK government, it remains coy about how much will actually go to health, population and HIV and AIDS activities. Sector-specific financial information is difficult to track from the public record. A look at one version of DFID's health commitments shows that only £19 million of the Department's bilateral assistance was committed to new health programmes in FY 2005/06, with a further £2 million spent on health related work within DFID's Policy Division at its headquarters. 7 This amount does not include funding for programmes that were continuing from previous years, or health related funding that was spent through multilateral organizations or knowledge (research) programmes. However, it is worrying that there is neither a clear financial commitment towards health in the White Paper, nor a transparent means of monitoring expenditure on health-related activities year-on-year through DFID performance and expenditure reports. We hope the new health strategy paper will go some way to redressing this marked shortcoming.
Besides White Papers, DFID staff also produce sector specific ‘Target Strategy Papers’ (TSPs) to further detail DFID's strategic intent for that sector. The last TSP for health was produced in 2000 and was called Better Health for Poor People. 2 Since then, other health sub-sector strategy papers have been produced in subsequent years, including one on maternal health and one on HIV and AIDS. In early 2006 DFID decided that, with the myriad of changes in health related development assistance since 2000, it was important to review and update its health TSP. It is a statutory requirement for DFID to open its strategic planning to public consultation, which was done over during May to early July 2006. The finalized Health TSP is due to be published by the end of 2006.
DFID'S Health Sector Priorities: Discernable Directions?
Comparison of the four priority areas
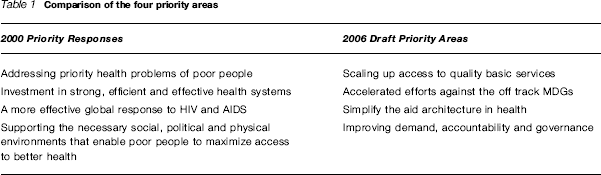
As can be seen from the above, the headlines in terms of DFID's strategy are very similar. The major shift is from a single focus on HIV and AIDS to a more general emphasis on the health related Millennium Development Goals, and an acknowledgement that the way in which health development aid is being delivered has become overly complicated and messy, with a proliferation of new organizations. For example, there are currently approximately 100 global health initiatives, funded through a mix of public and private financing, of which many have received support from DFID in the past.
When read together, DFID's health ‘priorities’ hardly seem to be priorities at all, but rather a shopping list of all the critical health-related areas that need tackling in the developing world. In many ways, the proposed priorities for the 2006 TSP are even less focused than those in 2000, especially with the shift away from a specific priority for HIV and AIDS to a more general approach to the health Millennium Development Goals. The 2006 priorities add a further priority ‘category’ on aid architecture that does not feature in the 2000 strategy. At first glance, a keen DFID observer would be justified in wondering if the organization is trying to be more ‘all things to all people’, and less about ensuring poor people benefit from increases in aid flows to the health sector.
These are valid concerns, though DFID staff have argued that these priorities represent hard choices made and are DFID's best contribution to improving aid effectiveness in the health sector. This being said, DFID can, should, and in some cases does, provide leadership in at least two critical health-related areas. These are a) ensuring that ‘upstream’ interventions at multilateral and national level are having the desired impact on poor people's lives; and b) putting sustained support into unpopular or less resourced public health areas.
Balancing Upstream Action with Downstream Impact
The primary challenge faced by DFID, and by those donors who work to the same alignment and harmonization principles of aid effectiveness, is how to ensure that supporting government policies and systems does at some point bring improvements into the lives of poor people in the countries it assists. And how can DFID persuade recipient governments to adopt genuine reforms, to set out pro-poor strategies and then to implement pro-poor programmes, especially when so much of its funding is passed indirectly through partners rather than directly to countries? At times it can feel as though we are witnessing an intricate, and not terribly harmonious, dance between partners who are trying to work out where this whole relationship is going. Each tries to steer the other towards his or her own interest, and some make the appearance of complying with the other's direction, but it isn't certain that they will end up in the same place when the music stops. With large chunks of funding also going through multilateral bodies with a view to achieving the same improvements for poor people, who leads the dance is even less certain.
DFID and its partners have influence to guide which directions receiving country strategies take, as donors often provide a significant amount of the funds to make the strategies work. While the current rhetoric puts governments in the driving seats of their own national development policies, those that are cash-strapped have limited room for manoeuvre if they wish to maintain the flow of funds from donor countries. We have witnessed some positive results during the last ten years of implementing this ‘partnership’ approach. For example, due to the sustained and joint efforts of the UN, bilaterals and the Global Fund to fight AIDS, TB and Malaria, many recipient governments do now have far larger HIV and AIDS programmes with ambitious objectives for assuring universal access to HIV and AIDS services in the near future. 8 DFID has played a leadership role in also ensuring that the health systems needed to deliver such ambitious programmes are not forgotten and that funds are invested in strengthening physical infrastructure and human resources at the same time.
DFID has found itself in a more privileged position vis-à-vis recipient governments than most of the other large donors because of the emphasis it puts on strengthening government systems and ownership. DFID also appears willing to be more innovative in how it funds programmes via government bodies. In order to ensure that the needs of poor people are not lost in some grimy part of the gap that exists between strategy and implementation, DFID staff are often involved in continual negotiation, debate and cajoling with government counterparts. This is the case even where DFID has agreed to pool its own funding for health (or other sectors) into a ‘Sector Wide Approach’ (SWAP) programme, or into a ‘pooled’ (multi-donor) funding arrangement for a sub-sector health activity. In theory, SWAPs and pooled funds help to reduce transaction costs (fewer reports, meetings, programme assessments etc.) for both governments and donors. 9 In practice these coordination arrangements can be very time consuming, especially as they are being set up. Similar effort is needed to work with multilateral bodies to help make their own internal mechanisms more efficient, and their aid more effective. DFID health staff have a key role, as critical friend, to play in these situations. Multi-laterals, government departments, DFID and other donors all need to come to an agreed understanding of how they will change the ways they will work in future, relinquishing more hands-on implementation to government staff and learning what scrutiny functions are needed for future monitoring of government programmes.
The ideal balancing act, then, is where DFID can support the development of international and national health strategies that favour services for poor people, and that ensure there is equitable access to health services throughout any particular country. This involves a certain leap of faith, that putting funding into the whole of the government health system, either directly or via a UN body, regional bank or partnership, will improve health in communities. It is why DFID support needs to involve not only assistance with creating national health strategies that have been elaborated through wide consultation, but also then with developing good relationships within government departments so that systems for monitoring progress, from the perspective of government, service providers and service users, are easily agreed and implemented.
Championing the Underdog Causes
DFID also has a very important leadership role to play in raising the profile of less popular public health causes. UK aid budget increases include a substantial increase for health research funding. DFID already contributes large amounts of funding for research on the so-called ‘neglected tropical diseases’ (such as schistosomiasis and lymphatic filariasis), while also funding research into new drugs for even less well known tropical diseases such as Chagas’ disease. In the area of sexual and reproductive health, DFID has advocated the need for improved family planning services, while global funding for family planning has decreased. Most controversially, DFID has championed the need for making abortions legal and safe, along with increasing the numbers of skilled birth attendants and improving emergency obstetric care, as the only ways to bring down maternal mortality rates in developing countries. DFID's stance on accessible modern contraception and safe abortion is a refreshing departure from the pro-abstinence and anti-abortion positions taken by the much more highly resourced US Agency for International Development. As such, these are all areas where DFID funding, and global advocacy, could have a real impact. We hope that these causes, and DFID's comparative advantage in promoting them, are not lost among the priorities set in the new strategy.
Leading for Change
What we are now witnessing is DFID and its like-minded partners becoming engaged in a very complex and high-stakes change process. There is little analysis in the literature of development as a change management process. Yet the radical shifts that are now being proposed within the OECD for how donor countries could make their development assistance more effective require many of the fundamentals of good change management. Donors are having to change the way they behave by agreeing to pool funding for use in implementing national strategies and by agreeing to longer term funding commitments so that governments have more assurance that their ten-year plans will still have funds in five years’ time. This will require a degree of trust that recipient governments will actively advocate and maintain pro-poor priorities, and that the governments will themselves change to allow greater transparency and accountability.
It also means not only investing in research but also using the evidence produced by research, disseminating it more widely, exploring the implications of the evidence for policy and practice, and finding novel ways of ensuring the adoption and implementation of changing policies Such a proactive approach to gathering and using evidence could be particularly powerful in advocating for greater sexual and reproduction health choice and a more reasoned debate around appropriate interventions. 10 We hope that DFID's health strategy will make explicit how as an organization it will use research evidence arising out its own programmes and others’ to help inform its future directions, and those of development and government partners.
In order for DFID to help lead the change processes inherent in the aid effectiveness agenda for health, and to be able to champion controversial causes, it needs to have knowledgeable and informed staff ‘sitting at the table’. These are not issues that can be handled by proxy but through investing a great deal of staff time, skill and often persuasive powers. While DFID's policy is to continue pushing further funding through more upstream activities, there also appears to be a trend towards reducing health advisor posts across the world as part of the Department's drive for efficiency. The arguments made for this are that, with less money going to DFID managed projects and more going to government managed programmes, or into multilateral agencies and global partnerships, there should be less need for sector specific staff to provide oversight in these areas. In other words spend more, do more (interventions), with less (people). This institutional perception runs counter to the reality of managing the change to accountable, transparent government programmes, influencing how the global health architecture works or making sure that unpopular issues remain on the international health agenda. All require a longer period of accompaniment to ensure not only that DFID funds are being used as intended but, more importantly, that the outcomes DFID signed up to are being achieved. It does not make sense to ‘downsize’ technical advisory staff at this sensitive point in the change process, but rather to bolster both the numbers and skills of those who will be needed to sit around both national and international tables. DFID health advisors will not only need to be technically proficient to maintain credibility with many of their development partners, but will also need to hone their competencies in analysing policy and political economies. They also need to work more closely with DFID's governance and social development advisors on how best to support improving partner governments’ accountability to their own citizens, and multilateral accountability systems.
When the new health TSP is eventually published we look forward to seeing not only what interventions enter into the final priority list, but also some indication of how DFID intends to support these priority areas and how it will continue to provide a leadership role at international and national levels. More importantly, we will watch with keen interest to see how DFID proposes to square its own efficiency versus effectiveness conundrum.
Footnotes
Competing interests None declared.