
Abstract
The ambulance service is often summoned by a significant other. Therefore the ambulance clinician is expected to establish a trusting relationship with her/him and not focus solely on the patient. The aim of this study was to illuminate the meaning of significant others’ encounter with ambulance clinicians in a non-emergency ambulance care context, where patients were triaged to a level of care below that of the Accident and Emergency Department. The design was inductive. We used the phenomenological hermeneutic method developed by Lindseth and Norberg. Eleven significant others were interviewed using an open-ended method. A structural analysis resulted in a total of seven themes, covering the meaning of being de-burdened or the absence of de-burdening. When de-burdened, the significant other was empowered, irrespective of the outcome of the medical assessment and triage process. In the absence of de-burdening, the significant other felt inferior, petty, de-powered and not taken seriously by the ambulance clinicians. The majority of ambulance assignments are considered non-emergency care. The ambulance clinicians are the first to encounter significant others in these situations and therefore have a huge obligation to understand and handle their basic needs.
Keywords
Background
This study reports the meaning of significant others’ (SOs) encounter with ambulance clinicians in the context of non-emergency pre-hospital care (N-EAC). Significant others are defined as any person who is close and important to the patient. 1 The triage consists of a two-tier system and patients are sorted in accordance with guidelines in a triage handbook, which decides the level of care. Prioritization of patients is conducted by means of the Rapid Emergency Triage and Treatment System (RETTS), which includes five priority levels (from lowest to highest in ascending order): blue, green, yellow, orange and red. 2 With a few exceptions, RETTS is implemented nationwide in Sweden in both ambulance and intra-hospital settings.2–4 If the patient is prioritized as blue, green or yellow, she/he is characterized as N-EAC, as these levels are classified as non-life-threatening. 2 Ambulance care services around the world differ in terms of training. Even within the European Union there is a lack of uniformity concerning the role, competencies and educational requirements of clinicians. Some countries use physician based units, while others employ nurses, specialist nurses, paramedics or emergency medical technicians.5,6 In the Swedish context ambulance clinicians comprise at least one registered nurse and one emergency medical technician (EMT). However, in several counties regulations require a minimum of one registered specialist ambulance nurse per ambulance. 7 The registered nurse, or if applicable the specialist ambulance nurse, is responsible for the patient throughout her/his time in the ambulance context, including care assessments, evaluating her/his medical condition as well as providing treatment if required.
The rationale behind this study is that previous studies indicate that 47–96% of calls to the emergency medical dispatch centre (i.e. 112) are made by another on behalf of the person with a perceived illness.8–12 The ambulance is often summoned by a SO. Unfortunately, we know little about the encounter between ambulance clinicians and SOs during N-EAC, representing about 50% of all ambulance assignments. 13
However, what we already know from other care contexts is that being a relative or SO is stressful and requires various forms of support.14,15 While waiting at the Accident and Emergency Department (AED) it is common for SOs to experience anxiety 16 and to feel abandoned,14,15 due to their concern about the patient’s condition. Significant others underline the importance of being seen by staff as well as receiving adequate information about ongoing and planned care.15,16 The few existing studies in the context of ambulance care report that being related to a patient who is receiving ambulance medical treatment might be viewed as being caught between hope and despair. 17 According to Holmberg et al., 18 SOs may end up on the side line, thus not actively involved in care. Patients emphasize the importance of being taken seriously when the ambulance does not transport them to the AED, 19 which for many patients would be the obvious destination. Holmberg and Fagerberg 20 stress the interpersonal relationship with patients and their SOs as one of the most important caring aspects within the ambulance care service domain. The art of caring emphasizes the relationship with the patient.21,22 Patients experience the relationship with ambulance clinicians as both positive and negative due to surrendering and relinquishing their power, 23 which can be described as a difficult situation. Ambulance clinicians have to find a balance between viewing the patient as a subject and taking her/his life-world into account 24 on the one hand, and the acute medical care that may objectify the patient on the other. When a SO is present, ambulance clinicians are also expected to establish a trusting relationship with her/him. Engström et al. 25 found that relatives play a key role in ensuring that the specialist nurse established a better relationship with the patient by learning to know more about them and his/her wishes. In turn, this enabled the specialist nurse to see the whole person, not just the patient. In conclusion, previous research emphasizes the importance of understanding the core meaning of the SOs’ encounter with the ambulance clinicians, which is also the motive behind this study.
Aim
The aim of this study was to illuminate the meaning of significant others’ encounter with ambulance clinicians in a non-emergency ambulance care context, where patients were triaged to a level of care below that of the Accident and Emergency Department.
Methods
We chose a phenomenological hermeneutic approach 26 based on Ricoeur’s philosophy27,28 in order to illuminate the lived experience of SOs as well as to gain a deeper understanding of the meaning of being a SO of a person provided with non-emergency ambulance care (N-EAC). The focus was on how SOs experienced their encounter with ambulance clinicians when their sick family member was not taken to an AED.
Informants and setting
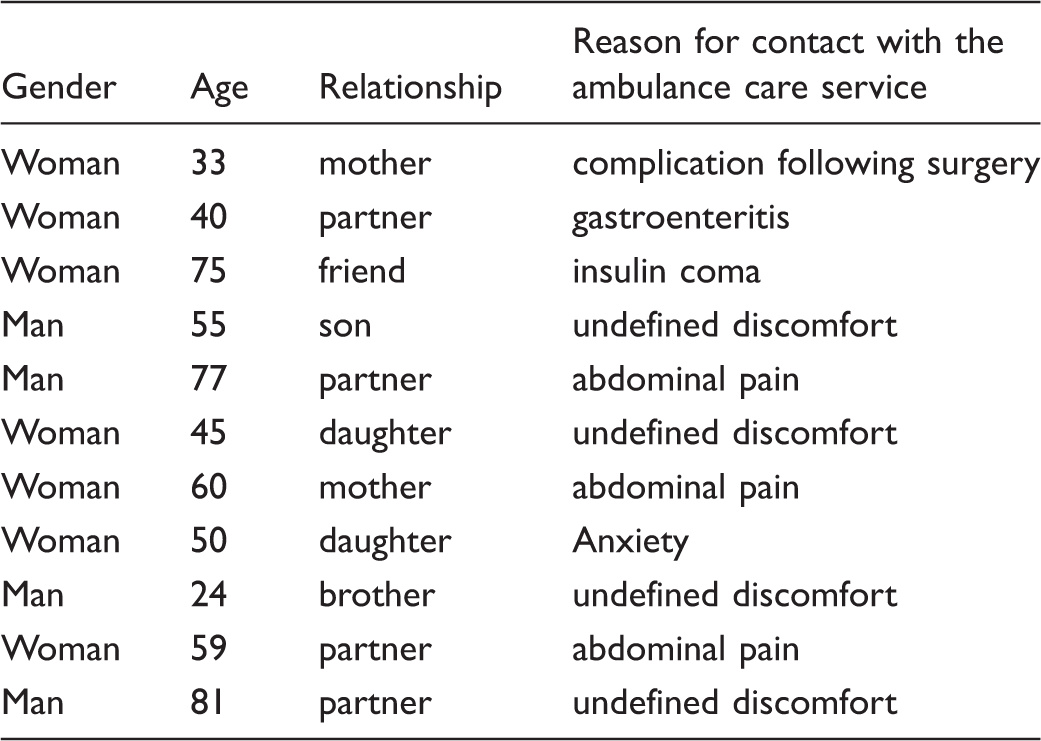
The inclusion criteria were adult (>18 years old), Swedish-speaking and cognitively adequate SOs whose sick family member received ambulance care for any reason but was not triaged to the AED by the ambulance clinicians. In conjunction with regular ambulance assignments, the ambulance clinicians recruited 21 potential informants to the study while visiting the homes of patients during late 2013 and early 2014. The catchment area for the local hospital includes approximately 250,000 inhabitants. In 2014 the emergency medical service handled about 17,000 assignments (all priority levels included) and was primarily served by three to six land-based ambulances, depending on the time of day. The potential informants agreed to the researcher contacting them by telephone, at which time they were provided with written information about the study. When the researcher contacted the informants the information was repeated verbally and the interview scheduled. Informants were excluded who were:
– Not contactable by telephone within four weeks (n = 5). – Did not respond despite having agreed a time (n = 3). – Changed their mind about participation after the initial contact (n = 2).
Descriptive information about the 11 significant others who had a mean age of 54.5 years (range 24–81 years).
Data collection
The first author performed all the interviews two to four weeks after the initial encounter with the ambulance care service. It was assumed that the informants would have no difficulty remembering their encounter with the ambulance care service within that timeframe. The informants were allowed to decide the time and place for the interview and all opted to be interviewed by telephone.
Digitally-recorded, open-ended interviews were conducted and then transcribed verbatim. We used an interview guide that started with the question ‘Could you please tell me about your experiences of the encounter with the ambulance care service?’ This was followed by questions about what was essential in the encounter. In order to gain a deeper understanding, probing questions were posed such as: ‘You told me you felt calm and anxious at the same time. Can you tell me more about that?’
It was considered that the content of the 11 interviews was rich. However, one of the 11 informants was re-interviewed to expand on and verify the emerging comprehensive understanding. Therefore the data consist of 12 interviews in total. The audio-taped interviews lasted around 35 minutes, with the exception of one that lasted for approximately 20 minutes. The interview with the informant who was re-interviewed lasted for about 15 minutes.
Data analysis
A phenomenological hermeneutic method developed by Lindseth and Norberg 26 was applied. The method consists of three steps, the first being the naïve reading, in which the interviews were read several times in order to become familiar with the text and reach an initial understanding. 28 In the next step, the structural analysis, the text was divided into meaning units in accordance with the aim of the study. The meaning units were then brought together and grouped into themes and sub-themes. In the final phase, the comprehensive understanding, the text was read again, while reflecting on the themes pertaining to what it means to experience N-EAC. The interpretation was guided by the authors’ pre-understanding based on their extensive experience of working in and teaching the subject of pre-hospital emergency care, as well as knowledge from previous research. This pre-understanding was constantly reflected upon and reconsidered during the data analysis and interpretation process.
Ethical considerations
The Regional Ethics Board of Lund approved the study (No. 2012/253–22/5).
Results
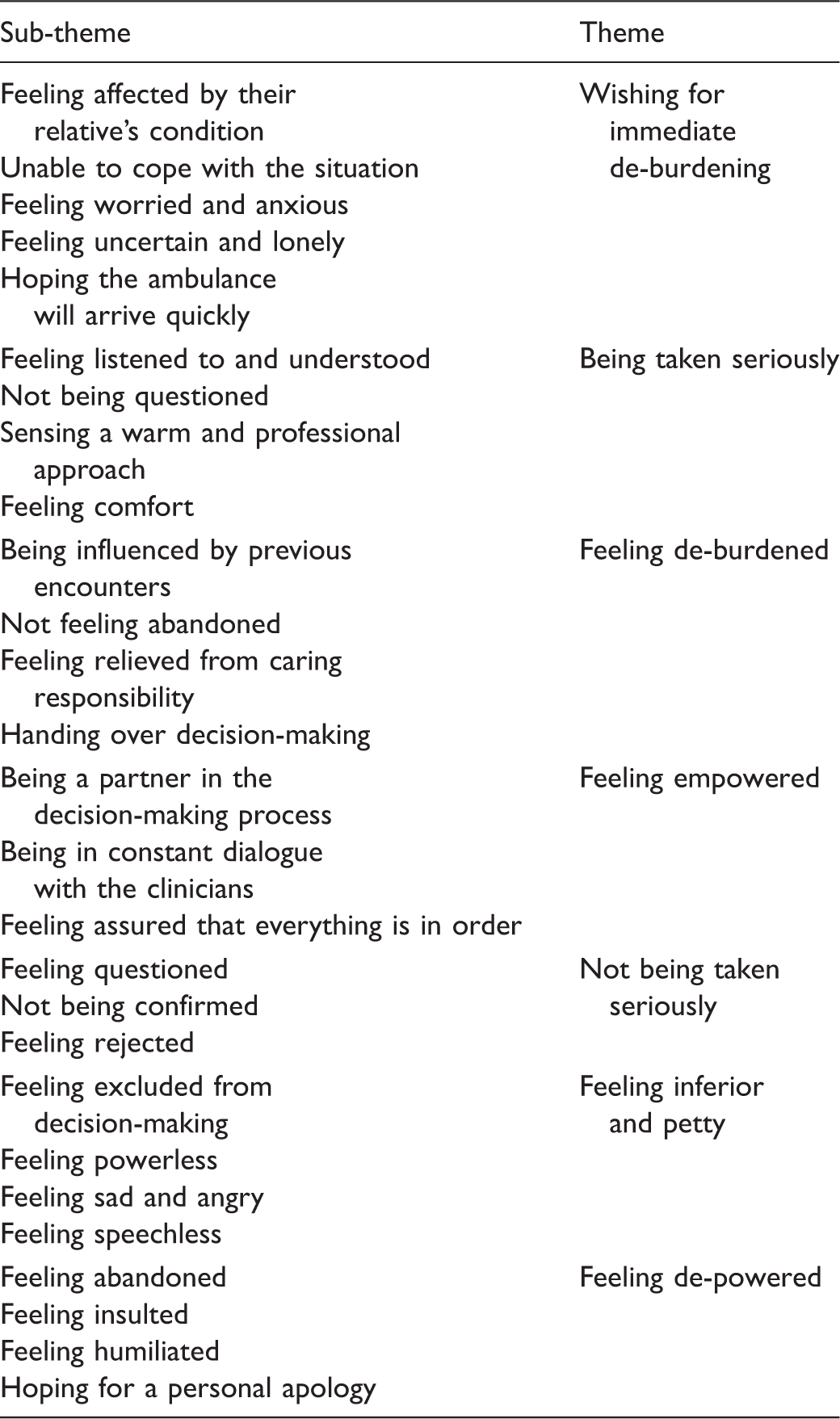
Sub-themes and themes from the structural analysis of the meaning of expecting immediate de-burdening from the ambulance clinicians during non-emergency ambulance care.
Wishing for immediate de-burdening
When the SO was distressed by the patient’s condition, a sense of insecurity emerged, which in turn triggered feelings of worry and anxiety. As a consequence the SO was unable to cope with the situation. … it can be some sort of impulse or how can I put it … phoning for an ambulance because one does not know what to do, perhaps a slight sense of panic … (woman, 45 years old) … and I can truly say that my view of the 112 [service] is very very good. They were really helpful, they were calm and … mediated a sense of calmness and knew exactly what to do … (woman, 75 years old) She knew that healthcare professionals were on the way and that alone made her calmer and a bit less worried. (man, 55 years old)
Being taken seriously
An important aspect of de-burdening was that the ambulance clinicians provided the SO with a sense of being listened to and understood. When the SO experienced the situation as untenable and decided to call 112, it was important to be taken seriously and not questioned about having summoned an ambulance. Another essential part of the experience for SOs was a sense of warmth and a professional approach towards the ill person, which resulted in a feeling of comfort. Both the SOs and the patients hereby experienced that the ambulance clinicians took the situation seriously. … they definitely took responsibility for the examination as soon as they came in. And they first and foremost addressed their questions to my mum … (man, 55 years old)
Feeling de-burdened
Significant others’ experiences of previous encounters with healthcare professionals influenced their attitude to the most recent situation. If their previous experiences had been positive, they also perceived the most recent situation as de-burdening. … it’s a question of confidence and trust in the ambulance crew. And as I had positive experiences … I find that it was really very helpful … (woman, 75 years old) Of course, that’s exactly what you want, that somebody else will also assume responsibility. (woman, 75 years old) But those who arrived now, the ambulance, how can I put it, they took over in a way, I mean, in a very good way, not negative, and they sort of explained a little. (woman, 50 years old)
Feeling empowered
When the SO felt confident that everything was in order, she/he was empowered to continue the care of the patient and accepted that the patient was well enough to stay at home. A feeling of being a partner in the decision-making emerged. Yes, one wants to have a knowledgeable person who says that it’s OK. They checked his values, listened to his breathing, pressed and examined certain parts of his body and such like // … one wants assurance that it really is OK. (woman, 40 years old) It felt extra safe for me, as they made certain that he [the sick family member] seemed to be alright before they left us. //So … you feel secure due to the fact that they really made sure he was OK. (woman, 40 years old) They never left me, or us, until we understood that the crisis was over. (woman, 77 years old)
Not being taken seriously
Previous uncaring encounters that influenced the most recent situation included the need to accompany the patient during transportation to hospital. The SOs tried to convince the ambulance clinicians to permit them to accompany their sick family member. They wanted to make sure that the ambulance clinicians did everything possible for her/him, in addition to providing AED staff with relevant information. But I reacted strongly to family members not being allowed to travel in the ambulance//It would have felt better for me … if I had been allowed to come and could see what they did and all those things. (woman, 59 years old) I would never forgive myself if something happened and I had ignored it and not phoned. That’s what happened on one occasion and my Dad died. (woman, 45 years old) … it feels a bit as if we are always phoning for an ambulance, that’s the feeling we had when they did not take her with them. (woman, 45 years old)
Feeling inferior and petty
In the event that the visit by the ambulance clinicians did not lead to de-burdening, feelings of being excluded from the decision-making process emerged. The ambulance clinicians often adopted a professional, outsider perspective, and thus failed to take the insider perspective of the patient and SO into account. Some of the encounters with the ambulance care service were characterized as stressful, i.e. being abandoned with a sick family member and not receiving the necessary support. This initially resulted in feelings of powerlessness and being stunned by what had happened in the encounter with the ambulance clinicians. The long-term consequence was that the SOs were left with a sense of sadness and anger. Mum was not in danger of death but nevertheless the situation was unbearable. (woman, 45 years old)
Feeling de-powered
When the sick family member was left at home it generated concerns, and the SOs’ primary need for de-burdening from the often self-imposed caregiving responsibility remained unmet. As a consequence, they felt abandoned and insulted. In addition to the fear of having to shoulder responsibility for continuing the care of the patient, there was a sense of humiliation due to not having one’s needs met. Thus, the informants stated that they felt the need to receive a personal apology. … she [the sick family member] has no strength, cannot cope any longer and I feared what could happen and dared not leave her alone because she was so totally exhausted … //I had no choice but to ‘like’ the situation. (woman, 45 years old)
Comprehensive understanding and reflections
When an ambulance is summoned by a SO, it is because she/he can no longer handle the situation with her/his ill relative, i.e. the patient. The SO expects that her/his ill relative will be taken seriously by the ambulance clinicians, thus providing immediate de-burdening. Is this need reasonable or too great for the ambulance care service to fulfill? We believe that this need is reasonable, basic and urgent and should be confirmed by the ambulance clinicians in order to provide comfort, establish trustworthiness and relieve suffering, all of which are considered to be at the core of caring. 21 Being cared for depends on the ambulance clinicians’ awareness of and attentiveness to the needs of SOs. 17 The ambulance clinicians’ approach should be characterized by consideration, presence and composure. 17 Andersson et al. 14 illuminate that elementary things such as being received kindly and being acknowledged and listened to help SOs to feel strengthened and to endure the situation. When the ambulance clinician confirms the expectation of de-burdening, the SO feels established in her/his dignity and thus her/his suffering is alleviated in the moment. 29 Consequently, when the SO is not taken seriously and not de-burdened in the moment, her/his dignity is violated 29 and feelings of suffering are increased. The absence of relief and support gives rise to a sense of powerlessness. 15 The SOs were positioned in a delicate situation. On one hand, they wanted to be de-burdened immediately, as presented in our study. On the other, they often felt totally responsible for the patient, which made it difficult for them to hand over responsibility to the professionals. 17
Significant others provide social support in different ways for persons with illness. In Sweden, out of the total population of about 9,800,000, 30 as many as 1,300,000 help or support an ill family member. At least 900,000 of these carers are of working age. 31 Finfgeld-Connett 32 argues that social support consists of two entities: emotional and instrumental support. Emotional support comprises consoling signs, which are intended to ease uncertainty, concerns, worry, hopelessness and depression. Physical presence is not always necessary for social support, as the provision of information may be sufficient. 32 When SOs lack the ability, confidence or skills to provide social support on their own, the need for relief, i.e. de-burdening, occurs. Relief can involve either emotional or instrumental support or both.
Holmberg et al. 23 argue that SOs have their own suffering, especially as the ambulance clinicians focus on the patient. They revealed that SOs may be both comfortable and uncomfortable with the idea of no longer being able to influence the caring situation. The SOs feel respected and acknowledged when the ambulance clinicians listen to them, 23 which corresponds with our results. Confirming the suffering of the SO should therefore be considered a necessity.
Söderlund 33 defines care from a SO’s perspective as ‘a struggle’ against or with others to relieve her/his own and the patient’s suffering. In other words, there is a tripartite relationship between the ambulance clinician, the ill person and the SO, which is interdependent. When the ambulance clinicians arrive and confirm SOs’ need for help and support, the SOs view it as de-burdening and are strengthened, which enables them to continue to shoulder the responsibility for care, making it possible for the patient to remain at home. It was essential for the SO to feel that the ambulance clinicians viewed the situation as being as serious as it really was. 14 It is of great importance to acknowledge that confirming and empowering SOs may profoundly affect future healthcare encounters. De-burdening enables SOs to feel confident that future healthcare contacts will have a positive outcome. Nevertheless, when the responsibility for the patient becomes overwhelming, SOs need help to deal with the situation. This is expressed as a desire to be de-burdened by the ambulance transporting the patient to the AED and allowing the SO to accompany her/him. Absence of de-burdening occurs when the ambulance clinicians do not confirm the SO’s desire to be relieved from caring responsibilities and also implies failure to take the patient and the SO seriously. In this situation the SO feels violated; a feeling that can continue long into the future and potentially overshadow subsequent healthcare contacts. The only way for the SO to reconcile her/himself with what happened in such an encounter is to be offered a personal apology from the ambulance clinicians who violated her/his sense of dignity.
As human beings we take care of and watch over ourselves until it is no longer possible. Ricoeur argues that a person is characterized as being capable, i.e. of talking, acting, narrating and above all taking responsibility. 34 When our ability to watch is gone we hand over this task and responsibility to someone close, a relative or a SO. 35 This mostly results in a sense of comfort, knowing that someone we trust and love is protecting us from harm and watching when we are too sick to manage. 35 Significant others believed that being present with the patient was vital for the patient’s comfort. 15 For those who are watching, the focus is on being attentive, checking and guarding in order to prevent negative events. This task sometimes requires being awake around the clock and being prepared to intervene whenever needed. Watching means waiting, preserving and worrying. 35 In the context of N-EAC, the patient surrenders to the SO, who watches until she/he can no longer handle the situation. At this point the ambulance care service is contacted due to a fundamental wish to be de-burdened from watching. This situation demands a professional and confirming approach from the ambulance clinicians, i.e. taking the patient and her/his SO seriously. If this does not happen the SO becomes uncomfortable and cannot let go.
Methodological considerations
Data collection took several years due to the fact that a nursing research culture was not implemented in the emergency context where the study took place. That is, the ambulance care services were not organized in a manner that promoted research, including recruiting potential informants. Most of the data were gathered in 2013 and 2014, and both SOs and patients were asked to participate by specialist ambulance clinicians. The patients’ experiences are presented in another study.19 Trustworthiness is important in qualitative studies, meaning that the research process as well as the final interpretation must be transparent. We adhered to the gold standard described by Lincoln and Guba. 36 Credibility was ensured by each member of the research team independently evaluating the interview guide. The interviews, which were conducted as a dialogue with open-ended questions, provided rich data about the phenomenon. The author who conducted the interviews (AR) has several years of clinical experience in the ambulance care service, thus has an extensive pre-understanding. Great efforts were made to bridle the pre-understanding throughout the study. To some extent the results were surprising to the research team, thus it can be assumed that the pre-understanding did not influence objectivity, especially as the context was unfamiliar to the other researchers (AK, AF). All three authors agreed that the final understanding was the most reasonable, although various interpretations were considered. As the informants were recruited in both rural and urban areas of southern Sweden, we believe that representativeness was good. The informants comprised daughters, sons, spouses, friends and parents, thus representing various perspectives of being a SO. Based on the logistic organization of the local ambulance care service, the research team saw no other alternative than to allow the ambulance clinicians to recruit the informants. Although we are well aware that this could lead to a potential problem in the recruitment process in terms of who was recruited, in our view the results indicate that the ambulance clinicians did not only ask informants to participate who they believed would be advantageous for the members of the ambulance care service. All informants opted to be interviewed by telephone. A probable reason for this might be that the encounter with the ambulance care service was fairly distressing and of an unplanned nature. Thus, it is possible that the informants had put the situation behind them and did not want to be reminded of it. Telephone interviews can carry a potential risk of missing data, as, unlike face-to-face interviews, it is not possible to observe visual information such as facial expression and other implicit nuances. According to a study by Hewison and Haines, 37 there are several reasons for difficulty in recruiting research informants, including their belief that they have nothing to contribute and their unwillingness to allow a research nurse to visit them in their homes, which was also a problem in the present study.
Finally, if the ambulance clinicians or another caregiver responded inadequately to the informants’ unique requirements and feelings, it could also constitute a reason for declining to meet personally.
Conclusion and clinical implications
The results reveal that the key mission of the ambulance care service in this context is to empower the SO to continue to act as a social support provider. A pre-requisite is to understand that the desire to be de-burdened and relieved of responsibility for care is a basic human need in the given situation. The majority of ambulance assignments are considered non-emergency care. The ambulance clinicians are the first to encounter SOs in these situations and therefore they have a huge responsibility to understand and handle the SOs’ basic needs. It is encouraging to know that there is a simple solution whereby the ambulance care service can fulfill these needs, thus enabling the SO to continue to provide support. The solution is to:
– confirm the expectation of being de-burdened; – provide immediate de-burdening; – take the ill person (patient) seriously; and – ensure that the SO can handle the situation before leaving the scene.
As first impressions are lasting, this approach could be implemented as a four-point checklist in every phase of the ambulance care service, which would also make it possible to evaluate the caring encounter. The results of this study raise questions about how ambulance clinicians interpret encounters with SOs and what needs are identified, especially within the N-EAC context. For this reason further research is necessary.
Footnotes
Author contributions
Andreas Rantala was involved in the study concept and design, collection and analysis of the data, as well as the drafting and revision of the manuscript. Anna Ekwall participated in the study concept and design, as well as the revision of the manuscript, while Anna Forsberg acted as the main supervisor and was thus involved in the study concept and design, data analysis, as well as the drafting and revision of the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.