
Abstract
The aim of this study was to investigate the meaning of social adaptation among solid organ transplant recipients one year after transplantation. We analysed in-depth interviews from 16 solid organ transplant recipients by means of phenomenological hermeneutics. The informants comprised 11 men and five women with a mean age of 54 years, who had received a kidney, a liver or a heart. We found the organ recipients adjusted their everyday life in order to adapt socially and achieve a normal everyday life. The meaning of social adaptation comprised six main themes revealed by one structural analysis: being restricted, changing habits, re-evaluating one’s body image, redesigning life expectations and life goals, enjoying and expanding the social network and being disappointed in others. We conclude that the core meaning of social adaptation is living a normal life. Social support can be emotional or instrumental and is highly valued when it helps the organ recipient to adapt and achieve normality.
Introduction
The rationale behind this study was to promote the best possible long-term outcomes and self-management after solid organ transplantation (SOT) by providing an understanding of the meaning of social adaptation from the perspective of solid organ transplant recipients (SOTRs). Today, SOT is an established lifesaving treatment for patients with terminal organ failure. Surgical advances and new immunosuppressive therapies have enabled researchers to shift from focusing solely on graft and patient survival to improving important aspects of everyday life, for example social adaptation. When a person becomes seriously ill, her/his spouse or partner, children, friends and colleagues are also affected. 1 From a social health perspective, health is defined as a person’s ability to function and interact with the environment, e.g. to adapt to situations that cause stress. Solid organ transplantation is one such stress-causing situation and requires adaptation on the part of the SOTR. Prior to the present study we conducted a thorough literature search in which we identified 268 articles from seven relevant databases. A total of 49 studies were reviewed in depth based on their entire content. 2 In the literature the term used is social functioning (SF) which was often found to play a minor role as part of a quantitative analysis or as one among many other questions in a quantitative study. The vast majority of the articles were quantitative and contributed no knowledge about the in-depth meaning of SF. In 12 of the articles SF was regarded as one of the main themes. Social functioning is an important factor in health-related quality of life (HRQoL). In general, HRQoL improved after organ transplantation, and SF was part of that improvement. In summary, this extensive literature review demonstrated that the five key aspects of SF are return to work, education, daily activities and leisure, barriers to SF and, finally, social adaptation. Social adaptation involves a transition from being terminally ill, waiting for an organ and being transplanted, to the recovery process. We were unable to find any information in the literature about the transition process and its various phases. However, it was clear that adaptation takes place when returning to social participation and that support from close family members is crucial. 2 A grounded theory of social adaptation after SOT suggests that the process involves deconstruction, restriction and reconstruction. 3 However, the meaning of social adaptation was not fully revealed. Therefore, the aim of the present study was to investigate the meaning of social adaptation among solid organ transplant recipients one year after transplantation.
Social functioning refers to an individual’s interaction with the social environment, i.e., family, friends, peers and the community, as well as her/his spiritual and cultural expectations. 4 Physical and social problems persist in some SOTRs despite the fact that transplantation may enable full recovery. 5 Improving social participation for SOTRs is an important issue. 6 In the present study we viewed the social health perspective related to receiving a transplanted organ as the ability to adapt and function in everyday life. This includes life-long treatment with immunosuppressive drugs and the resulting immune deficiency in addition to the risk of graft rejection, various infections and surgical complications. When compared to the general population, some social aspects remained poorer in the SOTRs. 7 However, SF was also found to be similar or in some cases even better than that of the general population. 8 It is unclear how SF changes over time, as the results of different studies vary. Health-related quality of life, which includes SF, increased during the first six months after SOT and then remained stable for five years. 9 However, SF was also at its peak one year after transplantation and thereafter gradually decreased over a 10-year period. 10
Materials and methods
Study design
The design was qualitative, explorative and inductive. A phenomenological hermeneutic approach based on Ricoeur’s philosophy11,12 was chosen in order to capture the participants’ lived experiences as well as to gain a deeper understanding of the meaning of social adaptation and social support. The focus was on the meaning of social adaptation and social support as experienced by the SOTRs one year after solid organ transplantation.
Participants
The inclusion criteria were Swedish-speaking and cognitively adequate adult (> 18 years old) SOTRs with a follow-up of one year. The informants were recruited by a nurse at the Outpatient Clinic when they were due for their one year follow-up at the Transplant Centre. The final group comprised 16 SOTRs (11 men and 5 women) who had received a kidney (n = 5), liver (n = 4) or heart (n = 6), while one informant had received both a liver and a kidney. Their mean age was 54 years (range 22–75 years) and they all had the ability to verbally share their experiences of social adaptation and social support during their first year with a transplanted solid organ.
Data collection and analysis
A year after the SOT, one of the authors (JC) performed all the interviews, which were open-ended and lasted between 24 and 115 minutes (mean 52 minutes). The informants were allowed to decide the time and place for the interview and all chose to be interviewed at the Transplant Centre. The interviews, which were digitally recorded and transcribed verbatim, started with the question ‘Could you please tell me about your social life before the transplantation?’ After 16 interviews it was considered that the content of the interviews was sufficiently enlightening, as no new information emerged.
Data analysis
The method developed by Lindseth and Norberg 13 consists of three steps, the first being the naïve reading, in which the interviews were read several times in order to become familiar with the text and gain an initial understanding. In the next step, the structural analysis, the text was divided into meaning units in accordance with the aim of the study. The meaning units were then brought together and grouped into themes and subthemes. In the final phase, the comprehensive understanding, the text was read again, and the themes pertaining to the meaning of social adaptation and social support were reflected on. The interpretation was guided by the authors’ pre-understanding based on their extensive experience of working with and teaching the subject of SOT. This pre-understanding was constantly reflected upon and reconsidered during the data analysis and interpretation process.
Trustworthiness is important in qualitative studies, meaning that the research process as well as the final interpretation must be transparent. We adhered to the gold standard described by Lincoln and Guba. 14 The four authors agreed that the conclusive interpretation was the most reliable, even though alternative interpretations were considered.
Ethics
The study was approved by the regional ethical review board of Gothenburg (EPN 634–12).
Findings
Structural analysis of the meaning of social adaptation among 16 solid organ transplant recipients who received a kidney, heart or liver.
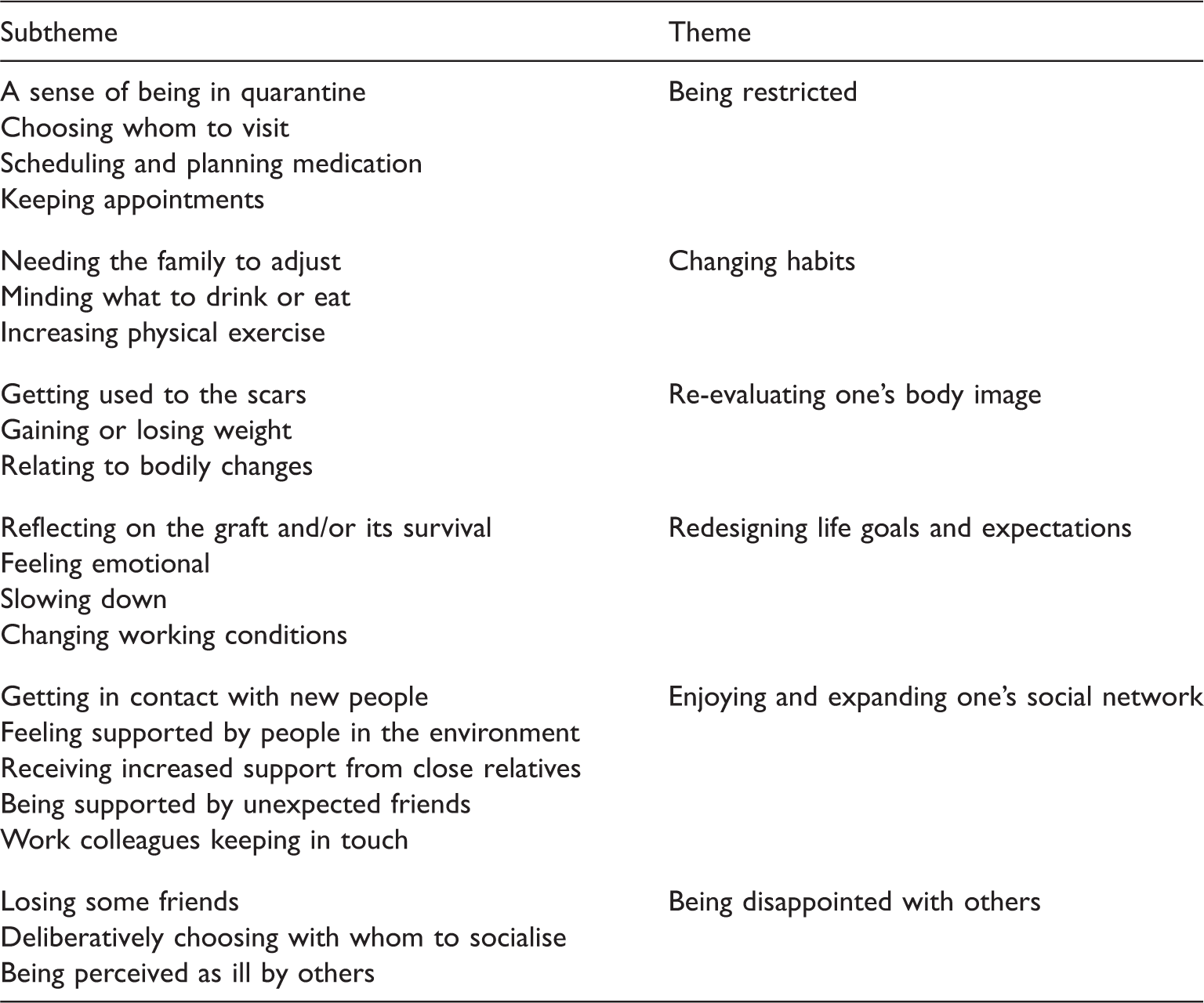
Structural analysis
Being restricted
After discharge from hospital, a period of recommended restrictions occurred, leading to undesired isolation. The informants felt they were in quarantine, carefully choosing who to meet, what to eat and trying to remember when to take their immunosuppressive medication. During this period they mostly met family members. When invited to parties they placed themselves apart from other guests to minimise the risk of infection and were first in line when a buffet was served. The informants stayed at home if they knew that young children would be present. To avoid missing any doses of medication, they set their mobile phone alarm and planned ahead to ensure that their supply of medication did not run out. At the start, I didn’t see any of my friends because I was susceptible to infections, but now I do. At that time when the results showed a low white blood cell count, it just wasn’t possible, it was like being quarantined at home. (Male liver recipient, 63 years old)
Changing habits
After the transplantation, adaptation involved changing many habits of everyday life. The informants changed their eating behaviour to become healthier and reduced their alcohol intake to zero. They exercised more in order to promote recovery and improve their general health. There was a strong need for support from the family to adjust to the new life situation. As they could no longer travel as they did before, or invite friends to dinner or parties, the lives of their close family members also became restricted. The new situation sometimes placed too much pressure on spouses, some of whom were unable to cope with the new life situation and decided to leave. It became too much for him [the spouse]. He found it a pain that everything was about me all the time, whether I would survive. And then in the autumn I also got this cancer spot and he couldn’t take it any more … well we had already had quite a lot and this was just too much. (Female heart recipient, 22 years old)
Re-evaluating one’s body image
Adaptation meant SOTRs adjusting to a changed body and having to re-evaluate their body image. Scars served as a visual reminder of what they had been through. Some gained while others lost weight, which affected bodily appearance and performance. Changes in appearance ranged from hirsutism to an increase in waist girth. I have my battle scars [laughs]. I suppose I was on steroids and got rather bloated. But now I think I look more like my old self. I have noticed that I look at my face a lot more to see if I’m becoming more hairy. Someone told me that she had begun shaving her face. But I thought to myself, oh no I can’t do that. So I keep checking myself. I bruise more easily and I already had some abdominal scars. So now I think to myself, well two scars more or less don’t matter. (Female heart recipient, 27 years old)
Redesigning life goals and expectations
The informants tried hard to live a normal life, which was described as the core meaning of social adaptation. However, everyday life also included thinking a great deal about graft survival. Questions about how long the graft would last mainly occurred at the start of the recovery process and slowly diminished when their condition became stable. The only thing that bothers me is wondering how long this kidney is going to last … but no one can tell me … I know that there was some problem with the kidney at the beginning. It took five days before it began to function. Yes or no, it perhaps doesn’t nag at me like that, but the question mark is still there. (Male kidney recipient, 54 years old)
Part of adapting to being an OTR meant feeling grateful for a second opportunity in life. This feeling was not a constant reminder but more in the nature of an emotional awareness and a sense of being touched by life itself. One should be grateful for being given the chance. I must think that this was my chance. I would probably not be alive today if I hadn’t got this heart … and I have noticed that I cry very easily these days. Tears start flowing and I must say that they never did before. Now it happens quite unexpectedly and for the strangest reasons. One can say that I’m easily moved, very easily moved. (Male heart recipient, 70 years old)
Most of the informants felt a need to slow down the pace of life in general and particularly at work. One way of doing so was to consider changing working conditions in order to experience less stress and pressure. We really enjoy taking an hour over morning coffee and reading the morning paper from cover to cover. I now value such things in a way that I never did before, back then I was on my way. I value life in a different way, nothing is taken for granted any longer. (Male kidney recipient, 72 years old)
Enjoying and expanding one’s social network
The meaning of social adaptation also involved both enjoying and expanding one’s social network. After the transplantation, the informants got to know new people, often unexpectedly. These new acquaintances, e.g. people from the neighbourhood, expressed their interest and support by asking what had happened and how the informant was coping with the new situation. Overall, the informants felt supported by the people around them. Relationships with close relatives often improved and became deeper. Relatives provided support and acted in a considerate manner by checking that the SOTRs felt strong enough before inviting them to visit. Some informants experienced support from unexpected friends, who seemed to understand in a more genuine way precisely what the SOTR had been through. When old friends were not around, new ones filled the gap. Finally, colleagues from work mainly kept in touch by phone, more often after than before the transplantation. This kind of social support served as a link to the workplace and was a reminder that going back to work was actually possible. The informants reported that their core social support was provided by close relatives, friends or colleagues, all of whom facilitated the informants’ return to a normal everyday life. Having friends and peers around who help to get life back to normal as quickly as possible. (Male liver recipient, 47 years old)
Being disappointed with others
A common theme in the interviews was that after the transplantation it was easy to recognise who was a real friend and who was not. Being disappointed with others demanded adaptation, as losing some friends was a common experience leading to a lack of both emotional and instrumental social support. Some people find it easier to understand than others. People who have perhaps experienced similar things themselves may find it easier to appreciate situations like this and don’t withdraw. I have no contact with most of my old friends. (Female heart recipient, 22 years old)
As a consequence of the loss of friends and social support, some informants deliberately chose who they wanted to socialise with in order to prevent further disappointment and to rebuild their social network. One strategy was spending more time with family members. Being able to spend time with my children, grandchild and friends of course … because one notices who they [your true friends] really are [becomes silent]. (Male liver recipient, 57 years old)
Finally, a barrier to social support was a belief that others perceived the informant as still being ill. I believe that people around me see me as someone who is ill. (Male kidney recipient, 72 years old)
Discussion
Methodological considerations
We aimed to obtain variation in respect of the informants’ ages, conditions and transplanted organs. However, one limitation was that all the informants were transplanted at the same hospital. There were more male than female participants, which reflects the overall transplant population, but this aspect might have affected the findings from a gender perspective. The interviews were conducted at the same time point after transplantation (i.e. one year) at the Transplant Centre, where the informants were very familiar with the environment and felt secure. This could have been an advantage in that they were mentally prepared for the interview.
All the authors participated in the analysis process and discussed their interpretations of the meaning of social adaptation and social support, which were found to be similar. Quotations have been presented to enable the reader to follow the analysis and interpretation process. 13 According to Ricoeur’s philosophy,11,12 it is impossible to free oneself from one’s own pre-understanding. The authors handled their own pre-understanding through awareness-raising activities and by reflecting on it when reading the interview texts.
Discussion of the findings
Our comprehensive understanding is that the meaning of social adaptation is the ability to live a normal life as a SOTR. The SOTRs are motivated by a strong will to resume their daily occupation despite the recommended restrictions regarding whom to meet, what to eat, medical appointments and immunosuppressive medication. When the recommended quarantine period is over, the social adaptation process continues, involving not merely changing one’s habits in everyday life but also getting used to bodily changes where scars are visible signs of the life-changing event. When the SOTR eventually becomes accustomed to the bodily changes and a different everyday life, the emotional, social and existential re-evaluation of life goals and expectations continues. This is a journey that has just begun one year after the transplantation. A journey not always desired but instead forced by their new life role as an organ recipient. During this journey, social support is appreciated when relatives and friends support the struggle for adaptation in order to regain a normal everyday life. However, a barrier to adaptation occurs when people perceive the SOTR as someone who is merely ill, which leads to a sense of disappointment. The reactions of people around the SOTR, their expectations and how they support the adaptation process are important factors in whether or not the SOTR chooses to maintain her/his previous social network.
Previous research describes how organ transplantation necessitates changes in daily life. 8 Social support and social reintegration are two very important factors for successful adaptation. 10 Compared to physical recovery, social adaptation is gradual and continues to improve over time. 15 Social adaptation and participation in daily activities after SOT are generally perceived as successful. 16 Factors that have a negative impact on adaptation are limited physical ability, post-surgical complications and current health status.17,18 Three qualitative studies highlight the importance of family and friends.19–21 When support was sought and provided, it gave the informants the strength to pull through, but when friends disappeared despite the need for support, the SOTRs had a feeling of a lost social life, 21 which is supported by our findings. Families play a central role in the adaptation process. 20 Spouses are often present and encouraging. We should acknowledge that the adaptation process places a great deal of strain on spouses and that children represent a stimulus in the struggle. The positive effect and importance of support from both spouse and children was confirmed by Forsberg et al., 19 who described how SOT could bring broken families back together again.
In her excellent discussion of social support, Finfgeld-Connett 22 claims that it is an advocative, interpersonal and context-specific process. Social support can be either emotional or instrumental. Emotional support consists of comforting gestures intended to alleviate uncertainty, anxiety, stress, hopelessness and depression. Physical presence is not always required. The SOTRs stated that simply knowing that someone is available if needed can be comforting. Receiving cards or flowers or knowing that others are praying for you can provide emotional support. Other ways of providing support are through use of the internet or telephone. 22 In our findings the informants felt supported when friends phoned to check up on them, even if not paying any visits. Phone calls from work were also appreciated. Due to the risk of infection, physical presence was initially confined to close family members or relatives. Social support can be provided simply by being present. Thus, in general, the emotional type of social support seemed to work well and was appreciated, although there were exceptions. Finfgeld-Connett 22 also argues that emotional support includes normalising situations by diverting attention from the problems at hand. Among our informants, social support was appreciated when it strengthened the process of adjustment to a normal life.
Instrumental support involves providing tangible goods such as child care supplies, furniture and food as well as various services, e.g. transportation, physical care or assistance with household tasks. In our study, instrumental support was mainly provided during the first period of recommended restrictions by spouses or close family members, which placed a great deal of pressure on them.
We believe it is vital to acknowledge that social support is an interpersonal, context-specific process involving the exchange of information. The information consists of facts, advice, words of reassurance, positive affirmation, empathy or similar expressions of support. The social support process is dynamic and changes in response to challenging circumstances such as SOT. Support providers are believed to be reliable, available and willing to provide help at challenging times. 22 However, our informants often found that former friends often withdrew after SOT. Perhaps SOT appears frightening to those not involved, thus continued support is not self-evident. When experiencing the loss of former friends, the SOTRs protected themselves by deliberately choosing with whom to socialise. An important attribute of social support is advocacy. Social support providers serve as advocates by motivating and empowering SOTRs to act on their own behalf and maintain as much control as possible. Without social support, there is the risk of lack of motivation, empowerment and control.
In order for social support to be initiated, the SOTRs must recognise their need for support and be willing to accept assistance, which is influenced by their own coping abilities and expectations of others. In turn, potential support providers must recognise the need for assistance and be willing to offer help. When this is not the case, the SOTR is painfully reminded of the need to redesign her/his life expectations and find new support providers with an inside perspective and experience of life changing events. Because circumstances are context specific, support after SOT is probably enhanced when providers and recipients have experienced similar challenges. 22 Solid organ transplant recipients only turn to healthcare professionals (e.g. transplant nurses) when others cannot provide the required support. It is worth noting that in our study healthcare professionals were not mentioned as possible support providers. The role of the professionals might be supporting the SOTR to maintain or re-design the social network rather than acting as providers themselves.
In conclusion, the meaning of social adaptation after SOT is the ability to adjust and regain normality, as perceived by the SOTR. Social adaptation necessitates changed habits, re-evaluation of body image and re-designing life goals and expectations. Both emotional and instrumental social support are needed after SOT and are appreciated when they facilitate adaptation to a normal everyday life.
Further research
A transplant-specific instrument covering social adaptation would be a useful tool for assessing important aspects of the long-term outcome after SOT.
Footnotes
Acknowledgements
This study was performed within the Swedish nursing research organ donation and organ transplantation network. The authors are grateful to Gullvi Nilsson and Monique Federsel for reviewing the English language.
Funding
We gratefully acknowledge funding from the Swedish Research Council for Health, Working Life and Welfare (Grant/Award Number: 2013–1766), The Local Research and Development Board for Gothenburg and Södra Bohuslän and from the Hainska foundation.
Conflict of interest
The authors declare that there is no conflict of interest.