
Abstract
The way organ transplant recipients depend on social interactions to develop and experience social health and well-being is similar to that of the general population. A transplant may result in a close to full recovery of health status, but the physical and social problems can persist in some patients. The focus on improving the recipients’ social participation has therefore become an important issue. The purpose of this integrative literature review was study social function after solid organ transplantation, that is, kidney, liver, lung or heart. An integrative review was performed on studies that matched the selection criteria and published in peer-reviewed journals from January 2000 to December 2014. The information from the text was extracted and patterns of social function were categorized into different subgroups that were further looked at, and five categories emerged: 1) work, 2) education, 3) daily activities and leisure, 4) social adaption and 5) barriers. The key aspects of social functioning involve five vital domains, that is, work, education, daily activities and leisure, social adaption and barriers. Returning to work appears to be the most important for the recipients independently of the transplanted organ.
Introduction
Solid organ transplantation (SOT) is in the 21th century an established and lifesaving treatment for patients with severe organ failure. The surgical advances and new immunosuppressive therapies have opened opportunities for researchers to shift the focus from graft- and patient survival to the patient’s improved quality of life and resultant health following SOT. When a person becomes seriously ill the consequences are far wider than for just the individual concerned. The spouse or partner, children, friends and colleagues are also affected.
1
These consequences are known to affect one’s perspective on health and on quality of life. The World Health Organization (WHO) defines quality of life as: An individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns. It is a broad ranging concept affected in a complex way by the person's physical health, psychological state, personal beliefs, social relationships and their relationship to salient features of their environment.
2
Transplantation may allow full recovery of health status, but the physical, psychological and social problems persist in some patients. 5 The focus on improving the OTRs social participation has become an important issue. 6
The motive behind research in health-related quality of life (HRQoL) is to improve life and minimize the consequences of illness or certain treatments. The definition of HRQoL became an important issue in discussions during the last decade of the 20th century, as organ transplant recipients often had to endure long hospital stays directly associated with the surgery and also later due to complications related to the transplantation. 7 Quality of life is an all-encompassing target in health care and HRQoL is by definition limited to the impact on quality of life that the disease and treatment inflicts on the patient. When assessing the long term outcome for OTRs, HRQoL and life satisfaction are significant and social function is an important factor in what is defined as HRQoL. In order to promote the best possible long-term outcomes and self-management after SOT, the understanding of social functioning is vital. We therefore turned to existing literature to explore the key features of social function among solid organ transplant recipients.
The review
Aim
The purpose of this integrative literature review was to study social function after solid organ transplantation, that is, kidney, liver, lung or heart.
Design
This literature review was integrative, covering both quantitative and qualitative research. We used a methodological approach to integrative reviews that allows the inclusion of studies using different methods. To provide the review with a structured framework, whilst mitigating the risks of bias and inaccuracy, the five stages suggested by Whittemore and Knafl
8
were adopted:
Problem identification Literature search Data evaluation Data analysis Presentation
In the first stage of the review, problem identification was conducted. Solid organ transplantation offers a patient the chance to return to an active social life. After the life changing event of organ transplantation, the patients suddenly find themselves in a new and fairly demanding situation that might put a lot of pressure on their personal resources. In this review, the social health perspective in relation to receiving a transplanted organ is the ability to adapt and function in everyday life. This also includes life-long treatment of immunosuppressive drugs and immune deficiency due to this medication, and the risk of complications such as the risk of graft rejection, various infections and surgical complications.
Search methods
In the second stage, a computerized literature search was conducted to find the relevant literature published between January 2000 and December 2014 using the electronic databases CINAHL, CINAHL Complete, MEDLINE Complete, AMED, PsycINFO and Psychology and behavioral sciences collection and PubMed. The following search terms were used in different combination: health related quality of life, social function, social factors, SF36, social participation and organ transplantation. All studies that met the following criteria were considered: 1) Social function-predictors, that is, the individual’s interaction with its social environment after solid organ transplantation was examined, 2) published in the English language, 3) participants were adults, that is, 18 years and older, 4) recipients having had a kidney, liver, lung or heart transplanted, 5) peer-reviewed articles, 6) published from 2000 to 2014, and 7) abstract was available. Reference lists from the articles and dissertations, that met the criteria above, were also scanned manually.
Search outcome
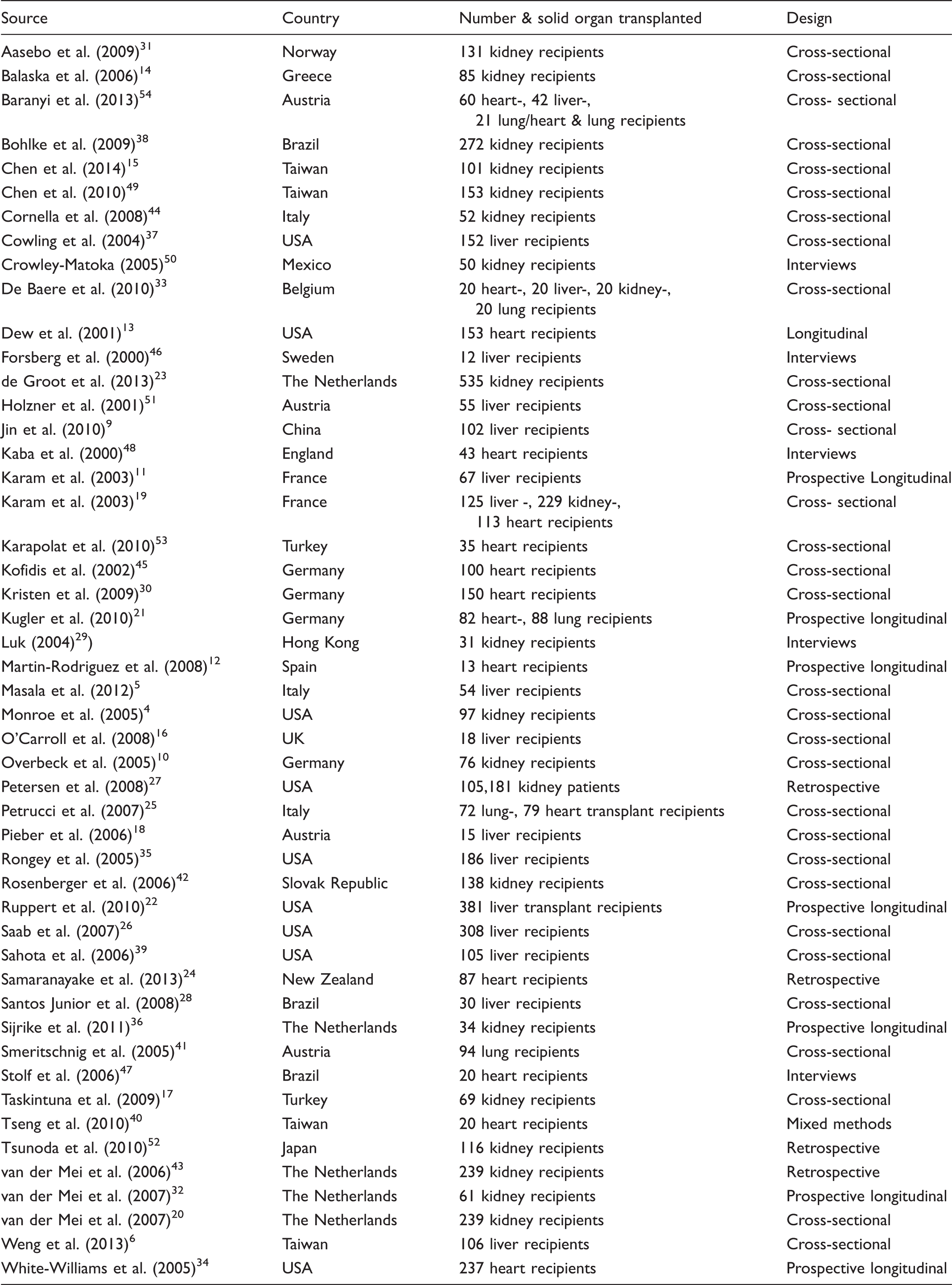
When all publications matching the keywords were included as described in Figure 1, the third stage involving data evaluation took place. Initially publications were selected using the inclusion and exclusion criteria. Then a second and a third evaluation was performed, based on the title of the study and by abstract availability. Finally, a last evaluation was made during which the full article was read. The end result was 49 articles that met the inclusion criteria and those were included in the study (Table 1).
The selection process of articles for the integrative review. Characteristics of the 49 articles reviewed for social function.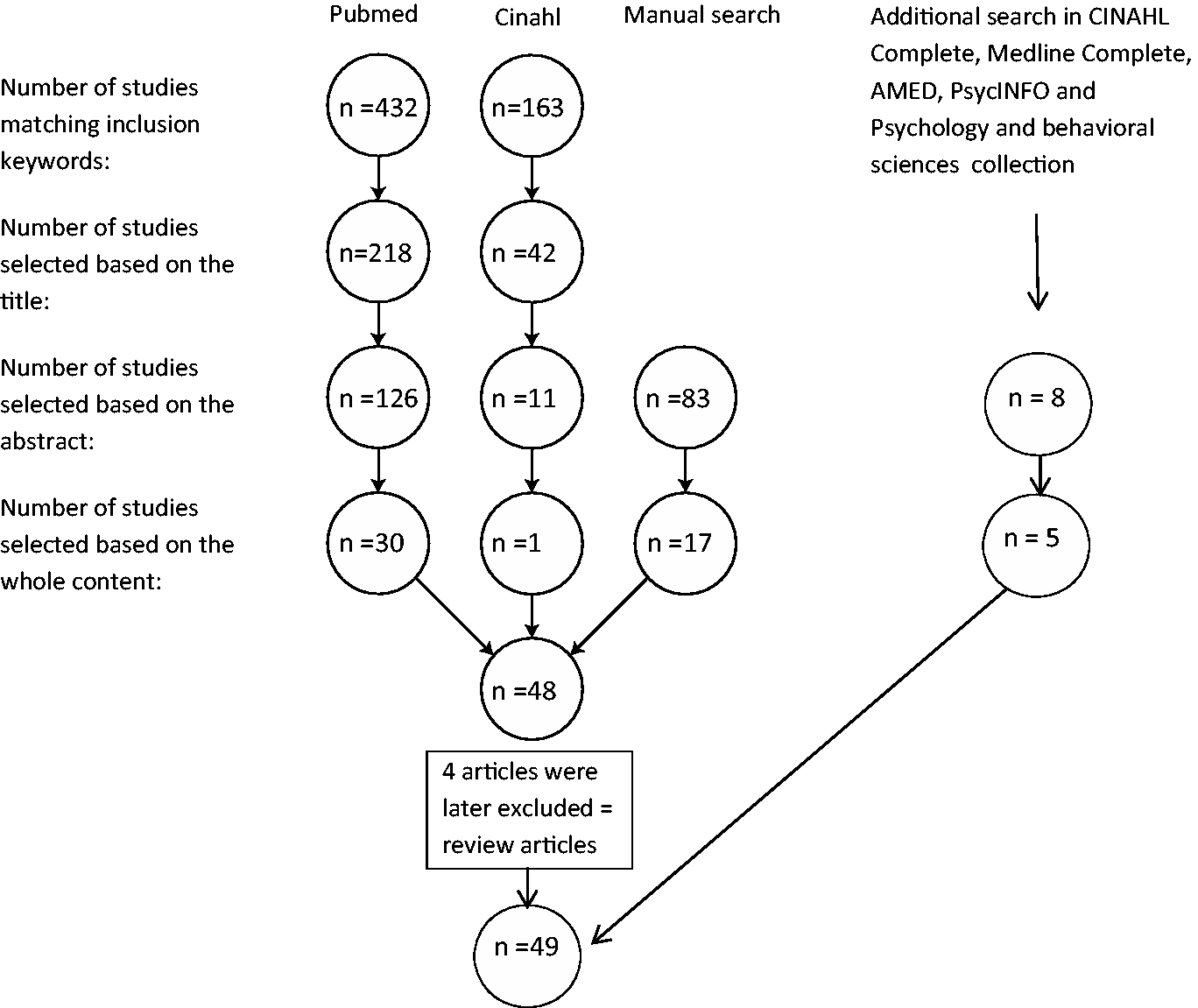
Quality appraisal
Evaluating the quality of sources in an integrative review is complex according to Whittemore and Knafl. 8 All papers in this review were published in peer-reviewed journals and the quality was evaluated based on the theoretical and methodological quality, informational value and representativeness. Papers of low informational value or lack of representativeness were excluded. However, we did not exclude any studies on methodological quality grounds, since the purpose of our review was to look at the literature broadly and synthesize all findings describing social function after SOT.
Data extraction and synthesis
In the final two stages, data analysis and presentation, the information was extracted and patterns, as well as differences, became apparent. The results were further examined and categorized into different subgroups, where quantitative and qualitative data each formed a subgroup. The analysis process continued and finally resulted in five categories that when linked together, present a picture of social function after SOT, as described in the literature.
Results
Of the 49 studies finally included in this review (Table 1), social function (SF) often played a minor role as part of a quantitative analysis or as one out of many other questions in a qualitative study. The absolute majority of the articles were quantitative. In 16 of the articles, SF was regarded as one of the main themes. In general, HRQoL improved after organ transplantation and SF was included in that improvement. Several studies showed that SF was improved when compared to how it was prior to transplantation.9–15 When compared to the healthy population, some social aspects remained poorer in the SOT recipients. 16 In one study, kidney recipients scored social function in the patient-reported questionnaire The Short Form (36) Health Survey (SF-36) lower than their donors but the same as the control group. 17 However, SF was also found to be similar or in some cases, even better than the general population.18–20 It is unclear how SF changes over time. Results from various studies are disparate. HRQoL increased the first six months after SOT and then became stable for five years. 21 However, SF was also at its peak one year after transplantation and thereafter slowly deteriorated during a period of 10 years. 22 Another study showed that kidney recipients having had a transplant from a living donor participated more socially and were more satisfied with their participation the first five years after transplantation than recipients having had a kidney transplant from a deceased donor. 23
Work
The majority of the studies examined employment status. Employment is considered an important indicator of social function and can be viewed as a benchmark to evaluate the patient’s ability to reintegrate into society in the post-transplantation process.9,24–26 It is also widely recognized as an important factor of quality of life.21,25,27 Employment and return to work is also a central wish and highly prioritized by those waiting for transplantation. 28 After transplantation, the recipients had renewed hope of a return to work. They were also able to make plans on how to best achieve this. 29 The prevalence of those who manage to achieve their goal and return to work after SOT varies extremely in the literature, ranging from 12% to 83%.4,6,10,14,15,24–26,29–36 There were no studies showing that SOT recipients work to the same extent as the general population.
A return to work after SOT was associated with a decrease in depression and presents opportunities to create social contacts, which increased well-being.10,33 Another advantage of working again was increased income, which made it possible for the recipients to influence social participation, and to do the things in life they once enjoyed. 37 Bohlke et al. 38 found that employed recipients had better social functioning than those not working.
Many predictors for returning to work are cited in the literature. Patients that experienced the ability and had the motivation returned to work more often.21,30,34 Other predictors were educational level, 30 younger age21,25,27,30,34,35 or a financial need.27,30 Disease-related factors21,27,30,34 such as duration of unemployment before transplantation were a predictor were the latter was a negative factor. Poor health status among liver transplant recipients was also a reason for unemployment. 35
There seems to be a consensus that the ability to return to work is connected to employment prior to transplantation.24,25,28,29,32,39 Also, the type of work before SOT seems to matter. Returning to work was lower amongst blue-collar workers, whose work is physically more demanding. 34 White-collar jobs were associated with returning to work.6,30
For those with previous employment, a reduction in missed working days could be observed. They also felt that work was less problematic. However, lack of employment prior to transplantation made it harder to reintegrate into the labour-market due to an experience of being outdated.29,39 The possibility to acquire a job was reduced over time after transplantation. 26 Having been off work for less than 24 months was viewed as a positive predictor of returning to work. 25 Those not being able to work 24 month after transplantation, experienced troublesome stress. 26 Psychological factors e.g. fear, play an important role. 40 These factors can also lead to self-inflicted isolation.
Several studies point out that most of the recipients were medically able to resume work after the transplantation from a medical point of view, but abstain to do so.4,6,25,30,33,41 Clinical factors due to transplantation and socioeconomic factors affect their decision. 39 Financially independent patients more often regarded themselves as incapable of working. 30 Some patients restrained from work due to re-prioritizing in favour of family and leisure activities. 33 The major reason for not resuming work was physically related.33,35,36,40 In contrast, Sahota et al. 39 found that the ones who returned to work reported inferior physical capacity.
Education
Education can in many cases be delayed due to the onset of the disease of origin and the subsequent transplantation. 31 Getting an education is highly valued. To initiate an education is associated with several factors, e.g. difficulties getting an employment due to prolonged absence from the labour-market and trouble finding a suitable occupation due to reduced physical ability.29,31
Aasebo 31 presented in a study about ‘the life situation of kidney recipients’ that kidney recipients had a higher education compared to the general population. Similar studies by Karam et al. 11 and Van Der Mei et al. 32 showed the opposite, that fewer liver- as well as kidney recipients had a higher education than the general population. Karam et al. 19 also showed that higher education is associated with higher social participation.
Daily activities and leisure
One of the main reasons for organ transplantation is to allow the recipient to resume their normal daily activities. 26 Being able to carry out normal daily activities and tasks was perceived as a measure of wellbeing by the patients. 42 Previous research confirms that recipients to a high extent resumed most daily tasks and perceived daily activities as encouraging.19,41,43 The patients experienced wellbeing from being able to carry out daily activities due to an increased physical capacity as compared to before the transplantation. 39
The patients had a positive attitude towards restarting hobbies and a return to daily life.29,33 Participation in leisure activities during a four-week period ranged between 22% and 98%. Activities were diverging and included everything from going out for a coffee to visiting an exhibition. A total of 44% reported resuming the same hobby as before transplantation. 31 Participating and resuming leisure time and hobbies increased during the first year following transplantation.20,43 However, 28% described having problems carrying out leisure activities one year after transplantation. 22 When comparing time spent on leisure activities with that of the general population, disparate results were shown ranging from recipients spending less time, to recipients spending more time than the general population.30,32,44
One part of finding the way back to a ‘normal’ lifestyle could be to resume travelling. Travelling for cultural and social reasons is regarded as a typical activity in daily life in Western countries. 45 Recipients who travelled reported this to be a positive experience that favorably improved their QoL as it brought a sense of wellbeing. 45
Social adaptation
Organ transplantation necessitates changes to daily life that demand adaptation. 19 Social support and social reintegration are two very important factors for adapting successfully. 10 Social adaptation is gradual as and continues to improve over time.12,28 Social adaptation and participation in daily activities is generally perceived as being successful.29,31,33 Also factors that had a negative impact on the social adaptation were brought to light. Such factors included limited physical ability, post-surgical complications and experienced current health.9,28,29,40,43 These led to direct consequences for the recipients: 22% reported reduced time spent with friends due to physical limitations and 34% perceived worsening relations with friends. 40 Three qualitative studies pointed out the importance of family and friends.46–48 When support was sought and given, it gave the participants socially strengthened, but when friends disappeared when the support was needed it gave the recipients a feeling of a lost social life. 48 Stolf and Sadala 47 found that families had a central part in the process of social adaptation. Spouses were often present and encouraging and the children represented a stimulus in the struggle to socially adapt. The positive effect and importance of support from both spouses and children was confirmed by Forsberg et al., 46 who also described how SOT could bring broken families back together. However, for one patient with a previous history of substance abuse, the transplantation lead to complete isolation and loneliness since the previous social network was built entirely around drug abuse. 46
Barriers for social function
Some recipients perceived a negative change of their body. 31 Chen et al. 49 found that the perceived notion of one’s body can affect relationships and create self-imposed isolation. Reduced social interaction could also be the result of a previous disease. 37 Reduced cognitive function due to an illness could directly and negatively affect social function also after an organ transplantation. 13 Recipients described limitations in their daily life and difficulties in resuming prior roles and responsibilities. 50 They expressed a wish to being able to resume ‘a normal life’.32,47,50 While one study reported that the majority of the recipients believed that they had regained their health; now they were normal people, 47 other studies described a feeling of being stuck somewhere in between healthy and ill.32,50 In a study by Holzner et al., 51 those whose expectation of a return to a normal life following transplantation was not realized rated their quality of life significantly lower than those who had accepted that life would not be completely ‘back to normal’. It can therefore be assumed that unmet lifestyle expectations may lead to an increased stress and adverse effect on patients’ HRQoL.
Emotional distress such as depression could complicate social interaction and daily tasks,28,52–54 and Chen et al. found that stress and depressive symptoms were significantly negatively correlated with social function. 15 Physical activity, social relations and working after having undergone organ transplantation was often associated with emotional stress. In difficult cases, the stress could become pathological. Some kidney transplant patients experienced that the stress prior to surgery had not diminished afterwards and they wished that they could return to dialysis. 49 A study of Baranyi et al., with heart, lung and liver recipients participating, showed that a consequence of physical insufficiency giving a feeling of low self-confidence could result in withdrawal from social life. 54
Methodological considerations
In this review, the five stages by Whittemore and Knafl 8 were considered useful in giving a comprehensive understanding of the field. Though 49 articles were included in the review, other papers may certainly exist and would be found if using different key-words in different combinations during the search. Since the vast majority of the quantitative studies were using SF-36 to explore social functioning or HRQoL in particular, the search outcome might have been different if this keyword was excluded or changed. The inconsistent results in the different studies could be the effect of different selection criteria when choosing the sample population.
Discussion of the findings
As a result of this study, we know that the key aspects of social functioning after solid organ transplantation involve 1) work, 2) education, 3) daily activities and leisure, 4) social adaption and 5) barriers. These five domains all affect social function in various ways.
Employment prior to transplantation is decisive for resuming work.24,25,28,29,32,39 Being off work for less than two years prior to transplantation was a positive predictor for going back to work. 25 The type of work also seemed to matter.6,30,34 Psychological factors and physical limitations were barriers for resuming work.33,35,36,40 Also financial independence might act as a deterrent to prevent from returning to work after transplantation. 30 Most countries have different insurances and social security systems. This makes it very difficult to discuss how contacts with employers could be promoted and resumed in general terms. Solutions have to be found in each country. It is probably very useful to consider this when the patient is assessed and put on the waiting list for transplantation. For some OTRs, retraining or re-education may be a solution. Social workers have a key role here.
Daily activities and leisure are important aspects for many healthy individuals and subsequently also for OTRs. 42 Interest and hobbies should be supported and encouraged to improve the societal participation after transplantation.29,33 To be able to travel seems to be one of the most important things for the recipients, as well as partaking in cultural activities, at least in the Western world. 45 This also requires the recipient to have a stable financial situation.
It is self-evident that various symptoms and complications negatively affect social functioning. The key issue might be how to prevent these complications or how to limit symptoms affecting everyday life. As health-care professionals we need to support symptom management and put strong efforts into limiting the impact of side-effects and complications and consider this as unwanted outcomes after SOT.
The social adaption demands a transition from being terminally ill, the wait for an organ, have the transplant and thereafter the recovery process. How the transition process proceeds cannot be found in the literature. Research is therefore needed in this field. However, it is clear that there is an adaptation when returning to social participation where support from the close family is crucial,46–48 and that could mean that persons without a close family or friends are at a potential risk for a worse outcome. 54 Professional support may be required for patients with a poor or non-existent social network. This should be considered when the patient is put on a waiting list to receive an organ.
In conclusion, this integrative review has pin pointed five vital domains of social function, that is, 1) work, 2) education, 3) daily activities and leisure, 4) social adaption, and 5) barriers. These domains are necessary in order to support a restored social functioning and thereby also a good health related quality of life for patients who have received a kidney, liver, heart or lung transplantation.
Further research is needed regarding a basic understanding of the process of transition of social functioning after SOT and what social function actually means from the perspective of the OTR. A transplant specific instrument of social functioning would be a useful tool to assess important aspect of long-term outcome after a solid organ transplantation.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.