
Abstract
Research that examines nursing staff competence that is necessary in order to provide safe community care is called for. This literature review examines Norwegian policy documents and international research with the aim to assess whether there is a match between expected and actual nursing staff competence in community care. Twelve policy documents and ten research articles were included in the review, of which key themes were identified. The Norwegian government expects a wide range of competence ranging from specific tasks in medical management to adhering to safe practice and care guidelines. Major discrepancies were identified between the advanced competence expected in policy documents and the actual competence as described by the research literature, which was mainly concerned with assistance with activities of daily living, medical knowledge, and personal abilities. There is a general lack of opportunities for competence development in the sector, implying that a general development of nursing staff competence is a pressing need in community care.
Introduction
Complexity in community care is growing. The older patient population that community carers are in charge of is sicker and frailer with more complex needs than previously, 1 and is consequently in need of multifaceted and competence-intensive nursing care. However, a common feature across community care in Europe is that a relatively large portion of employees are low qualified nursing staff. 2 Despite efforts to enhance the quality of community care, inadequate health care in terms of unmet needs, adverse events, and other threats to quality of care is reported.3,4 A Canadian study found an incidence rate of 13.2% for adverse events in home care services, of which one-third were considered preventable. 5 The trend is also present in Norway, where a recent study found inadequate care in Norwegian nursing homes to be frequent, as 87% of the nursing staff admitted to have provided inadequate care in the form of committing neglect or abuse. 6
Professional competence is described as a key issue when providing quality health care services. 7 Quality of care requires that nursing staff possess the competence needed to meet complex health care demands. 8 Internationally, studies indicate that better quality of care, improved patient outcomes and fewer adverse events are associated with higher levels of registered nurse (RN) staffing in general health care.9–12 For nursing homes in particular, higher staffing levels, especially staffing by RNs, have been associated with improved care processes and patient outcomes for functional ability, pressure ulcers and weight loss. 13 Positive relationships have also been found between staffing levels and number of deficiencies, and between staffing levels and avoidable hospitalizations. 14
However, measuring the relationship between nurse staffing levels and quality of care by focusing on numbers of staff provides only a limited explanation of the relationship between nursing staff and quality of care, as it is more a study of volume and qualifications than of the actual care and treatment that is provided. Such research reduces quality of care to indicators that are easy to measure, and excludes factors that are important to the patients and their families. 14 One issue is the number of staff and the distribution of staff groups; another is the actual competence of staff to provide the care that is needed. Thus, studies should examine the nursing staff competence needed to provide safe community care. 15 According to Eraut, 16 nursing competence is a contextual concept that, for analytical purposes, is divided into knowledge, skills, and personal attributes. We understand competence to be influenced by technical, political, and structural factors; thus, competence in community care is in a state of flux caused by the changing needs of patients and the composition of personnel. This understanding of competence is related to a holistic conceptualization of competence. 17
Consequently, a community care environment that is characterized by frail older patients with complex needs and relatively low qualified nursing staff leaves us with the following research question: does the available nursing staff competence match the competence required to meet the needs of older patients? To assess what is already known about this question, a review of policy documents and research literature was performed with the following aims: ‘identify, describe and discuss relevant policy documents in relation to expected nursing staff competence in community care’ and ‘identify, describe and discuss research in relation to actual nursing staff competence in community care’ with the overall aim to ‘compare actual and expected nursing staff competence according to available evidence: identify implications for practice and research’. The review reflects policy in Norway which follows European trends in the sector. During the past decades European health care systems have been reformed by a move away from institutional care towards home care, a move away from public provisions towards private and mixed services, and increased use of informal care.2,18 Community care is in this study defined as nursing homes and home care services. Nursing staff is defined as all staff involved in patient-related work in nursing homes and home care services, including, but not limited to, registered nurses (RNs), assistant nurses (ANs), and assistants (the latter two being referred to as support workers).
Method
The design of this study is a scoping literature review based on the framework of Rumrill, Fitzgerald and Merchant.
19
Scoping reviews tend to focus on the breadth rather than the depth of coverage of literature and they tend to incorporate both research and non-research material.
19
As opposed to systematic reviews that typically focus on well-defined research questions and aim to provide answers to a narrow range of quality assessed studies, scoping studies address broader topics and research questions and many different study designs might be applicable.
20
Important requisites for both systematic and scoping reviews are, however, that the methods used throughout the different stages are applied in a rigorous and transparent way, and are documented in sufficient detail to enable the study to be replicated by others. Figure 1 is an illustration of the research design of this study.
Research design.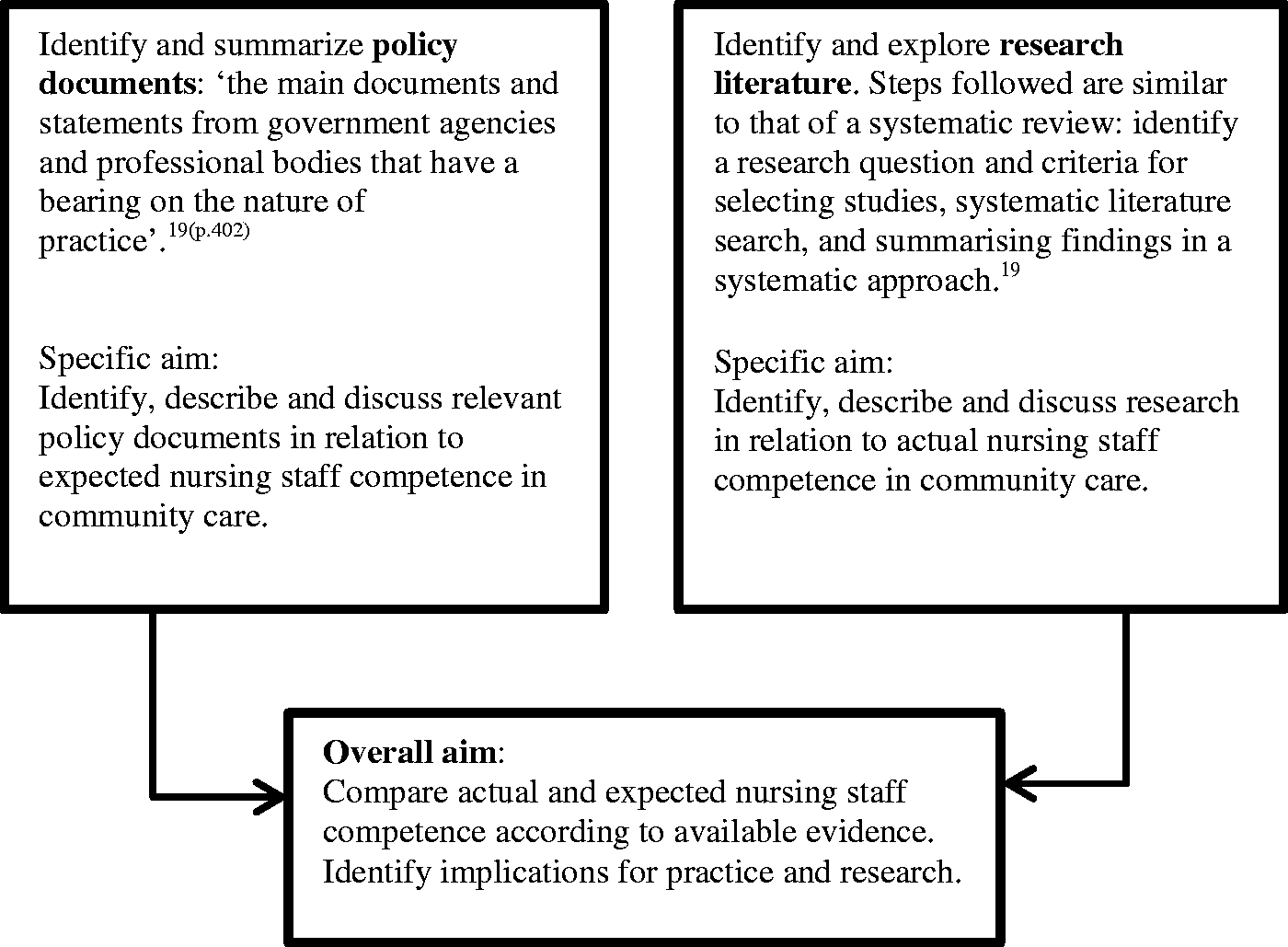
Literature search and selection
A search for relevant government policy documents was undertaken at the following Norwegian websites: www.regjeringen.no (Norwegian government), www.lovdata.no (Norwegian laws and regulations), www.ks.no (Norwegian municipalities’ organization), www.fhi.no (Norwegian Institute of Public Health), www.helsedirektoratet.no (the Health Directorate), www.ssb.no (Statistics Norway), www.helsetilsynet.no (Norwegian Board of Health Supervision), www.helfo.no (The Norwegian Health Economics Administration), and by asking for expert opinions on which documents could be relevant for this study. The search was performed in 2011 and repeated in 2014.
Eligible research articles were identified using a range of electronic health research databases, both international, Scandinavian and Norwegian: Medline, Embase, Science Direct, Academic Search Premier, CINAHL, Eric, PsychInfo, Cochrane Library (including: DARE, HTA, CDSR, CENTRAL, EED and CMR), Joanna Briggs Institute, British Nursing Index, Ovid Nursing, Web of Knowledge, Google Scholar, Svemed, Norart, Cristin, Bibsys and Idunn. Search terms used included both tesaurus/medical subject headings (MeSH) and keywords, and the MeSH were ‘exploded’ where ever possible. Boolean operators (OR, AND) were used to expand and narrow searches. Single and combined search terms included: professional/clinical competence, community/primary/public/municipal health nursing/services, geriatric nursing, assessment, questionnaire, health survey, self-report, nursing evaluation research, program evaluation, validation studies, health personnel/manpower, skill mix, nurses’ role, nurses’ aides and nursing. In search engines where the option was possible, truncation was used on the search terms nurs* and competen*. The searches were limited to English or Scandinavian language, peer-reviewed articles published 2000–2014, wherever possible.
Figure 2 illustrates how the search and selection of literature was performed. The main inclusion criterion was that the literature addressed generic competence in relation to nursing staff in community care. Literature was excluded if the content was clearly irrelevant to our aim, e.g. competence regarding nursing students, general practitioners or nursing staff in hospital settings. We initially identified 14 policy documents. Careful reading of all 14 documents revealed 12 documents that included text about expected nursing staff competence in community care. We initially screened 4491 research article titles. Abstracts were read where the title did not clearly state the content of the article. All articles that did not meet the inclusion criteria were discarded. One hundred and fifty four papers went through to a second test of relevance where all abstracts were read and a further 15 papers were discarded. The remaining 139 articles were then read systematically. After this third-level screening we were left with 10 research articles to include in the study. Included literature was read carefully and text/research findings about competence of nursing staff were extracted into tables. Subsequently a narrative synthesis approach was undertaken, by which key themes and categories were identified.
21
Literature search and selection.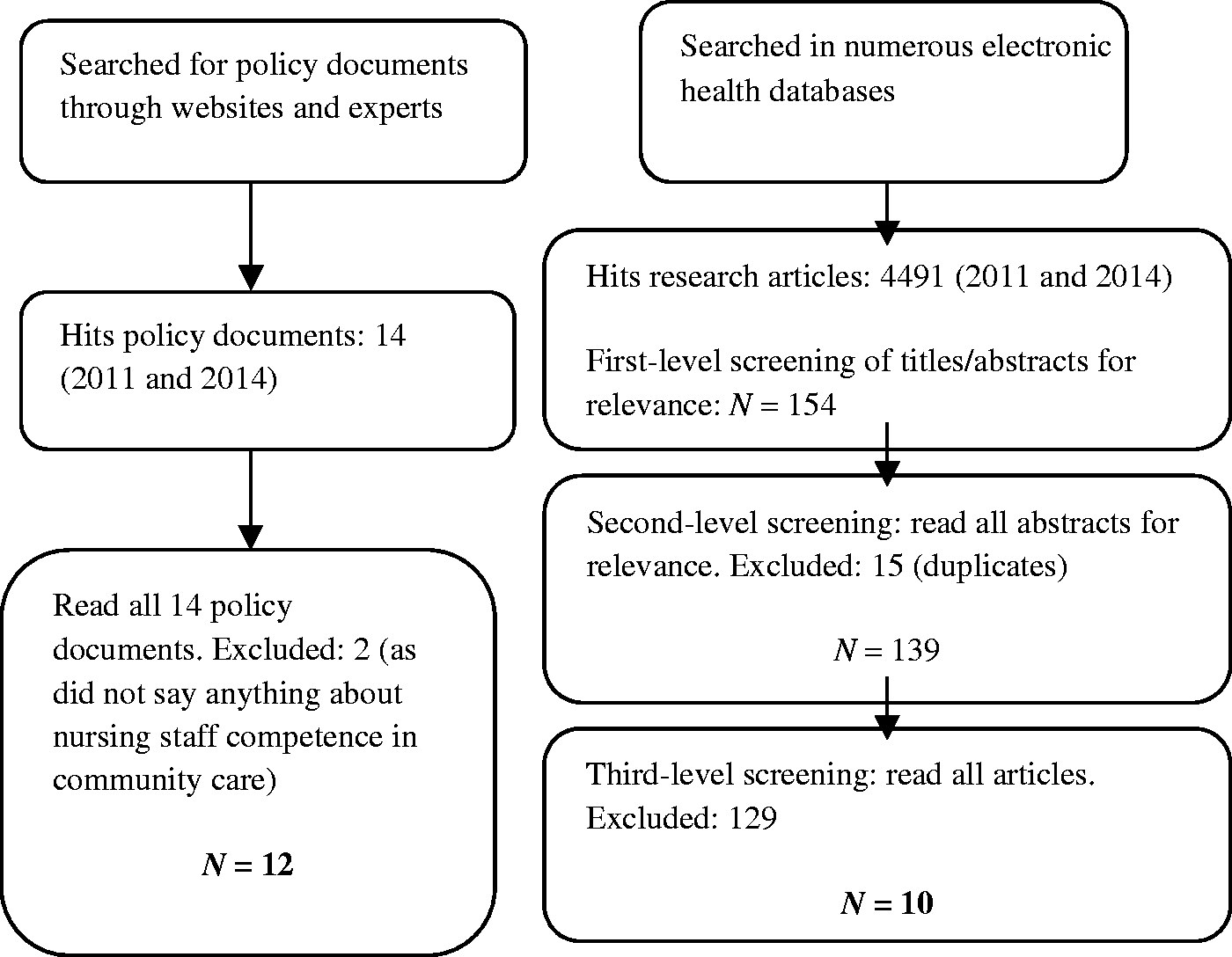
Results
Review of what policy documents say about expected competence in Norwegian community care.

RNs: Registered Nurses.
From the 12 included policy documents the following categories of expected nursing staff competence in community care were identified:
Overall principles: Sound professional practice and considerate care, patient safety and quality assurance, self-management and empowerment of patients Core competence: Public health, health promotion, disease prevention, early intervention, treatment, care, acute care and rehabilitation Competence related to cooperation and interaction: Cooperation, inter-professionalism, patient trajectory, and multicultural understanding Specific competence: Medical management including observation and reporting of effect and side effects, facilitation of research and application of evidence-based practice, application of health-related technology, knowledge of local health challenges and epidemiology22–33
Review of research on competence in community care.

RNs: Registered Nurses; ADL: activities of daily living; IADL: instrumental activities of daily living.
The research literature draws a fragmented picture of actual nursing staff competence in community care. The role and competence of RNs in community care is better explored than those of ANs and assistants, which are more or less unexplored, despite their importance for the care delivered to patients. In sum, the literature shows that all nursing staff in community care need, but do not have: clear job descriptions, opportunities to develop their competence and a balance between work demands and control of the work situation.
The competence of RNs was explored in six studies.34,35,37,39,42–43 The actual competence of RNs working in community care seemed to be: broad experience as a nurse, mental strength and confidence to make one’s own decisions, medical knowledge, making adequate assessments, technical skills, able to handle problematic situations (somatic, psychiatric, and palliative care), knowledge about the specifics of community care, pedagogical competence, skills in assistance with activities of daily living (ADL), collaboration with next of kin, application of evidence-based practice, computer-based documentation skills, and leadership of other nursing staff.
The competence of both RNs and other groups of nursing staff was explored in two studies.36,38 The research literature is also scarce concerning the competence of ANs and assistants in community care; only two relevant studies were found.40,41 Nursing staff as a group have been shown to have competence in assistance with ADL (meeting their patients’ physical needs), medication handling, cooperation with patients and next of kin, medical and nursing theoretical knowledge, and use of ICT. ANs were found to base their competence on standard routines, trial-and-error and situated knowledge. 40
The following categories of actual nursing staff competence in community care were identified:
All nursing staff have competence in:
Core competence: Assistance with ADL, medical and nursing theoretical knowledge Competence related to cooperation and interaction: Collaboration with patient and next of kin Specific competence: Knowledge about the specifics of community care (e.g. services and benefits available to patients) and use of ICT
In addition RNs have competence in:
Overall prerequisites: Broad experience as a nurse, mental strength and confidence to make decisions on their own, nursing assessment and technical skills Competence related to cooperation and interaction: Pedagogical competence and leadership of other nursing staff Specific competence: Application of evidenced-based practice and medical management
Discussion
Imbalance between actual and expected competence
The Norwegian government (through policy documents) is ambitious and expects a wide range of nursing staff competence ranging from specific tasks in medical management to adhering to overarching principles such as safe practice and providing considerate care. Overall, the list of competence that the Norwegian government expects, points at an advanced level of competence (e.g. facilitation of research and application of evidence-based practice) which cannot be expected to be a part of the repertoire of ANs or assistants (support workers). Much of the expected competence is also new to RNs who have an older degree. Health promotion, empowerment of patients, patient trajectory, patient safety and health-related technology are all concepts that have been given renewed content and meaning in community care. Considering the fact that few RNs have had the opportunity to enhance their competence in relation to new demands at work in Norway, 45 this list of expected competence can be seen as ambitious.
When comparing the competence described in the research literature to the competence expected through government policy documents, there are major discrepancies. The advanced and ‘new’ competence expected through policy documents does not reflect the competence described through the research literature, which is mainly concerned with assistance with ADL, medical knowledge, collaborative skills and personal abilities as mental strength and confidence. The discrepancies between what the research literature reveals of actual nursing staff competence in community care, and the nursing staff competence that the government expects, can be illustrated as in Figure 3.
The imbalance between actual and expected nursing staff competence in community care.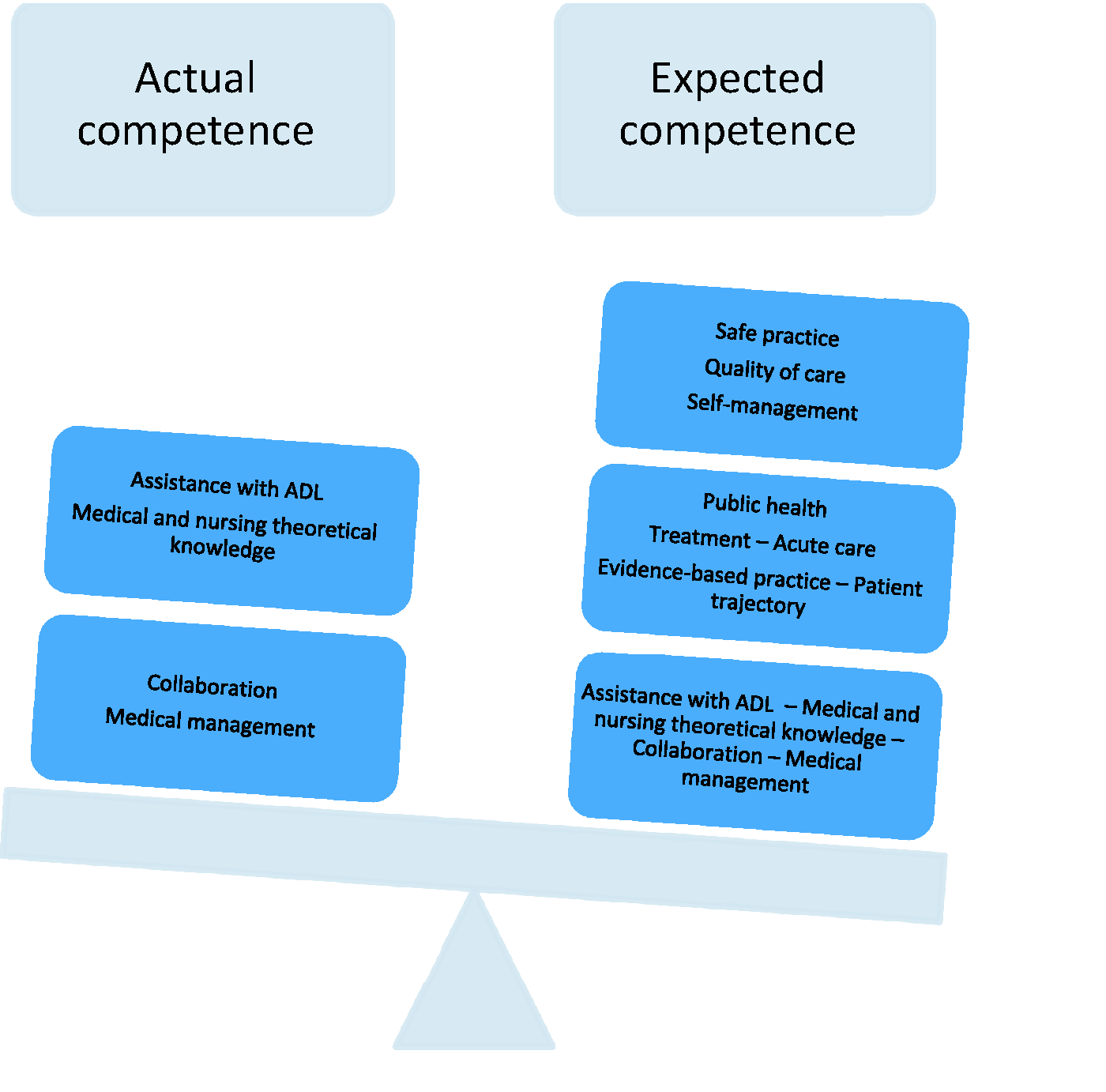
Following the example of several other European countries, 46 the Norwegian government implemented dramatic changes in the structure of Norwegian health care in 2012.22,24 An important consequence of these reforms across Europe is that people in need of health care are mainly meant to be treated in the municipalities in which they live, i.e. community care. As the largest population group in need of health care is older people, the reforms affect this group the most. All over Europe, fewer hospital beds and shorter hospitalizations mean that community care, across home care and nursing homes, currently encompasses follow-up of medical treatment from hospital stays and rehabilitation in addition to traditional older people care,47,48 again implying that nursing staff are meant to perform quite advanced nursing care and medical treatment. 49 The ambitious governmental expectations do therefore seem necessary in order for the older patient population to receive safe, high-quality community care. A shift is also evident in the research literature, which demonstrates an awareness of the current complexity in community care. Research published after 2012 emphasizes that advanced nursing care is now needed in community care to meet the needs of frail, older patients.42,43 Finnbakk et al. 42 describe a future scenario where we not only require multidisciplinary and advanced nursing competence in the fields of gerontology and geriatrics, but also the ability to integrate advanced health care technology into care. If the imbalance identified in the literature is indicative of an actual competence gap in practice, there is indeed a need for a strong focus on competence development in community care, as is emphasized in most of the research literature reviewed. Although most countries have their own unique health care system, there is a European trend of pushing more health care responsibilities into community care. 50 Assuming that the older patient populations across Nordic countries have similar health care needs, the findings from this study could therefore have transferability to other Nordic countries.
Gap in the research literature
As only two Norwegian studies concerning competence in community care were found, of which one is a study of poor working conditions and the other revealed that community-based nursing staff competence is unexplored,35,41 we do not know if the competence expected through policy documents can be found in Norwegian community care as research on community-based nursing staff competence is lacking. However, results from competence measurements in Sweden and Finland36,38,39,43,44,51 support our proposed competence imbalance, and since Sweden and Finland are similar to Norway in how they organize community care, results can be assumed to be transferable to Norway, meaning we can assume a competence imbalance in Norway. Moreover, the rapid change in and growth of community care are also reasons to call for new studies of nursing staff competence in community care, both in Norway and other Nordic countries. Most studies available concern only one group of nursing staff (mostly RNs), which is problematic when such a large proportion of community care nursing staff consists of relatively low qualified or untrained personnel. Research on community-based nursing staff should preferably include all groups, as all nursing staff groups have influence on the quality of care, but with the possibility to assess differences in competence levels between groups and whether these levels meet the needs of patients. Finally, the research on competence in community care is limited, consisting of several qualitative studies that are not necessarily transferable to other settings and several questionnaire surveys which lack vital information about the validity and reliability of the questionnaires used. Future studies of competence in community care should aim for methodological rigor and generalizability in order to increase the legitimacy of nursing science in this field.
Methodological considerations
A limitation to this scoping review is that it only identifies and reviews policy documents from one Nordic country, whereas it reviews research on competence from several Nordic countries. The transferability of the assumed competence gap to other Nordic countries could therefore be further explored and strengthened in a review of all Nordic policy documents. Scoping reviews aim to provide an overview of the literature and evidence available in a field, 19 and may be enhanced by including as much literature as possible. We did, however, restrict our inclusion of policy documents to Norway with the limitations that this involves.
Strengths of this and other scoping reviews are that, as opposed to systematic literature reviews, scoping reviews focus on the breadth rather than the depth of coverage of literature and they incorporate both research and non-research material. First, this scoping review provides us with an overview of the literature and evidence available, which is a good starting point before exploring the field empirically. Second, this review incorporates policy documents, which are often omitted from scientific articles. Policy documents, defined in Figure 1 as ‘the main documents and statements from government agencies and professional bodies that have a bearing on the nature of practice’,19(p.420) lay the ground for what thresholds of quality we can and should expect from community care and are therefore important benchmarks against which to compare the actual nature of practice.
Conclusion
As quality of care requires that nursing staff possess the competence needed to meet complex health care demands, evaluation of quality of care should involve evaluation of nursing staff competence. This is particularly important in community care which is expanding in most European countries but which still makes use of relatively low competent staff. This study, a scoping review of Norwegian policy documents and Nordic research regarding nursing staff competence in community care, found a substantial imbalance between ambitious governmental competence expectations and the actual nursing staff competence that is available. All research studies emphasize a general lack of opportunities for competence development in the sector, and that general development of nursing staff competence is a pressing need in community care. Rigorous research with a focus on all nursing staff groups involved in care and treatment of patients in community care is needed.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.