
Abstract
The aim of the study is to describe the experience of psychotropic drug use among young people with mental health problems. Young people experience mental health problems, and some will need to take psychotropic drugs for either a short or a long time. Psychotropic drugs may be effective in reducing mental distress, but raise questions about increasing use, side effects, long-term treatment and off-label use. Qualitative interviews were accomplished with eight young people who had taken psychotropic drugs. Three categories were identified: ‘Effects of psychotropic drugs’, ‘Access of professional care and follow-up’ and ‘Social life and psychotropic drug use’. The young people experienced both beneficial and undesired effects from the psychotropic drugs. They experienced lack of access to professional support and follow-up. Life with family and friends was influenced negatively by psychotropic drug use and the young people were afraid of being lonely and stigmatized. The results may have implications for those who work with young people. Young people striving with mental health problems and psychotropic drug use have to have access to professional support and follow-up. Knowledge about effects of psychotropic drug use among young people is needed. The work about openness about mental health problems among young people has to continue.
Introduction
International studies have documented an increase in psychotropic drug use among young people over the past decades. The World Health Organization (WHO) recognizes that young people’s mental health is one of the most important areas concerning public health in any given year. About 20% will experience a mental health problem, most commonly depression or anxiety. 1 Some of them will be in need of psychotropic drugs for a short time, and some for a long time. In the US, this use increased two- to threefold during the last decades. 2 Different patterns have been observed in psychotropic drug use between the US and European countries, for example the level of antidepressant use among young people in the US is reported to be three times higher than in European countries. 3 However, there are also differences within the European countries which may reflect cultural beliefs, and different regulations, diagnostic classification systems and study design.3,4
Psychotropic drug use among young people in the Nordic countries seems to be low, except for Iceland, where the figures are more in line with those for other European countries and the USA. 5 However, there seems to be a trend towards increasing hypnotic drug use also among Norwegian children and young people.6,7
Unfortunately, evidence on safety and efficacy of psychotropic drug use among young people is scarce, especially that concerning long-term effects. 8 Psychotropic drugs may stimulate or sedate, alter the emotional experience of anxiety, and influence mood and concentration. They may have different side effects: some mild and others more serious, producing physiological and neurological disturbances. 9
The appropriateness of psychotropic drug use for young people is controversial and studies claim that too many psychotropic drugs are used off-label.4,10,11 These studies concern the use of drugs for an unapproved indication, age group, dosage or form of administration. Most psychotropic drugs are not tested or licensed for young people, and only a few psychotropic drugs have been approved and indicated for use among those younger than 18 years. 12
Nevertheless, psychotropic drugs may be effective in reducing mental health problems, but raise questions about increasing use, side effects, long-term treatment and off-label use among young people; this, in turn, may warrant a tight follow-up once the therapy has been started. To ensure support and follow-up, it is important to know about the different aspects of psychotropic drug use among young people. To our knowledge, few studies investigating the experience of psychotropic drug use among young people have been reported. Thus, the aim of this study was to describe the experience of psychotropic drug use among young people with mental health problems.
Methods
To gain an understanding of young people’s experience of psychotropic drug use, a descriptive and qualitative design was used. The focus in a qualitative content analytical approach is analysing explicit content of a text,13,14 and in the current study, this meant the transcribed interviews from the young people.
Participants
The participants were recruited from an association for young people with mental health problems, the Mental Health Youth (MHY). This is an interest group for young people up to 30 years of age. The organization operates through its members, and their aims are to work for openness about mental health problems, prevention of mental distress and a better health service. 15
Information about the study was made available on the MHY websites. In addition, the leaders of the MHY sent information about the study in one of their regular letters to all the members. Young people aged between 16 and 24 years with experience of psychotropic drug use were invited to participate. One reminder was sent out via the website. Ten adolescents contacted the researcher by email or SMS. One was too old and one did not respond again despite two reminders. Eight young people wanted to participate; altogether, six girls and two boys participated. All participants had experience of psychotropic drug use. They were aged 17–24 years (mean = 20.87, SD = 2.99 years). Three were high school students, two worked, two were university students and one received disability benefit. The participants all came from seven counties in Norway.
Data collection
Data was collected by means of individual interviews between December 2012 and March 2013. Six took place, in accord with the participants’ wishes, at cafeterias and restaurants, and two were telephone interviews. The interviews lasted between 45 minutes and 2.5 hours (mean 68.62, SD 38.96 minutes). They were audio-recorded and later transcribed verbatim by a translation bureau. Interviews were carried out that addressed various aspects of psychotropic drug use. Experiences related to this drug use were evoked by asking: ‘Please, tell me about your experiences with psychotropic drug use?’ Individual follow-up questions were asked to elicit more detailed information.
Data analysis
The audio-recorded interviews were analysed based on the qualitative content analysis of Graneheim and Lundman.13,14 The manifest content analysis was made by the first author. The interviews were read through several times to get a sense of the whole picture, then the whole text about the experience of the young people’s use of psychotropic drugs was divided into meaning units, which were then condensed. These condensed units were abstracted and coded. The various codes were compared, based on differences and similarities, and sorted into seven subcategories and three categories; these constitute the manifest content.13,14
The tentative categories were discussed by the four authors and revised when necessary until a consensus had been reached. A process of reflection and discussion resulted in agreement about how to sort the codes. Quotes were chosen to illustrate the category in question.
Ethics
The young people were given written and verbal information about the voluntary nature of participation and the right to withdraw at any time with no need to explain. Informed consent was obtained from all the participants before the study, and confidentiality was assured. All the participants were urged to contact their therapist or physician if problems emerged after the interviews. They were also given the opportunity to call the first author, although none of them did.
Results
All the participants had used psychotropic drugs for a short or a long time. The psychotropic drugs described the most were antidepressants, antipsychotics and hypnotics. The young people did not start this medication without consideration, and had thought about addiction problems and undesired effects. Usually, a general practitioner prescribed the drug.
Categories and subcategories related to the experience of psychotropic drug use among young people with mental health problems.
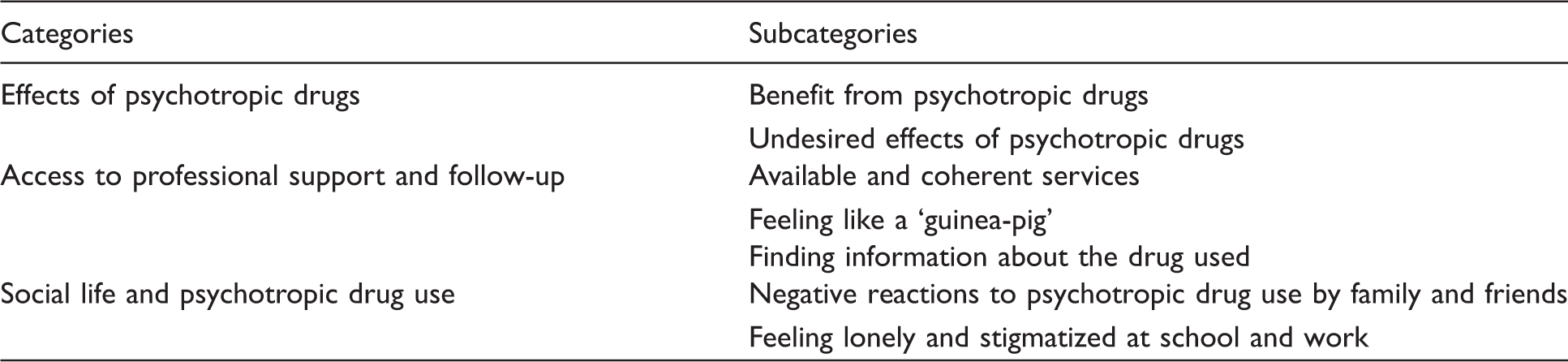
Effects of psychotropic drugs
The psychotropic drugs benefited the young people, and made it possible to be part of society, although there were undesired effects, of both a mental and a physical nature.
Benefit of psychotropic drugs
For those individuals with depression, psychotropic drugs provided quite good mood stability. The medication gave the person a life with emotions and an easier daily life. I am depressed; I cannot go outside my door. The antidepressant gives me the opportunity to walk out and go to physical training. I do like to train, it gives me pleasure.
A young woman told that her psychotropic drug enabled her: ‘… to break her heavy chains and do other things, dare to try and have a cosy time together with friends’. When she did not use her psychotropic drug, such normal things were hard to do.
Undesired effects of psychotropic drugs
In contrast to the benefits of psychotropic drugs, the young people also described some undesired effects or no effects at all. When I was about 15 years of age I had some strenuous periods. One moment I was singing, everything was great. The next moment I felt terrible, cried and could not do a thing. Some periods were like this every day. The physician gave me a psychotropic drug, but it did not help at all. Some of the drugs made me confused. I could be dangerous and do things I usually do not dare to do. I tried to commit suicide. I was too apathetic to bother. I had taken my morning medication. After a while I had to sit down, but could not rise again. All the energy had gone. The psychotropic drug was phased down after several episodes like this, but then I become more depressed and indifferent.
Access to professional support and follow-up
The young people described a lack of coherence between the different levels of the health services and in the period when they were students they found it difficult to find the school’s health service. When prescribed psychotropic drugs they could ‘feel like a guinea-pig’ and they had to find out information about the drug for themselves.
Available and coherent services
The young people did not find the school health service to be easily accessible. The public health nurse’s (PHN) office was often hidden in a back entrance and not publicized on the school’s notice board. The young people found it difficult to walk through the corridors to the office, feeling that they were being looked at. Those who managed to visit the school health service and talk to a PHN were resigned to this feeling. There was a PHN at our school, perhaps an hour a week. She was not interested to talk about that kind of problem – mental health problems.
The young people were followed up within different health services, and before reaching the age of 18 years it was within the child and youth psychiatry services, from which they reported several good experiences. The health service providers asked about the psychotropic drug use and took the relevant blood tests. As they got older, the young people were offered treatment through the regional psychiatric services for adults. The transition from child and youth psychiatry to adult psychiatry services could take a long time to settle. But finally, when they did get treatment, the young people felt that it was adequate. When they improved and stopped taking the psychotropic drug, the trouble started again if there was a relapse of the mental distress and they were no longer a patient on a high-priority list, because then they had to wait a long time for treatment. I am afraid of telling the therapist that I feel well. I cannot stop the treatment. If I do so it is impossible to have contact again when I need them. I will be placed on a new waiting list. In the period when starting with a psychotropic drug I talked to my family doctor every other week. I had frequent agreements with her until I got a psychologist. Then I saw her more seldom, merely when we had to make a change concerning the psychotropic drug. However, some physicians would give a prescription without a new appointment.
Feeling like a ‘guinea-pig’
Hypnotics for sleeping problems were described as helpful at the start, but often their effect decreases. This may cause physicians to choose to stop the drug treatment, increase the dose or try another drug. The young people felt insecure about physicians or other health professionals’ knowledge of psychotropic drug use. The physician said: I do not know if this drug is good for you, but I think so. Good effects have been seen in other people. We will give the drug another chance; perhaps it will have an effect later. He just said: we have experience! I cannot understand the ethics here. I wonder if physicians really know what they are talking about. I feel like a “guinea-pig”. It’s a pity they do not know more about the effect of the psychotropic drugs. The patients become ‘guinea-pigs’. I have to have the psychotropic drugs, so of two evils …
Finding information about the drug used
Information about the drug, its effect and side effect, how to take it and for how long was insufficient. In addition, the young people had to find the information themselves. The young people used friends, parents, the Physicians’ Desk Reference and websites to access information.
When asking health professionals about the drugs, the young people were often dissatisfied with the answers. The young people were sceptical of professionals’ knowledge about psychotropic drugs and used the internet and other sources of information after the consultation. He only prescribed the psychotropic drug. Back at home, I searched on the internet and found the Physicians’ Desk Reference. The reference said that the physicians should have regular checks with the patients who used that drug and another said that research showed a danger of suicide attempts among persons using that drug.
Social life and psychotropic drug use
The young people experienced negative reactions from their family and friends and felt that the family was ashamed. They felt alone and stigmatized at school and work because of their mental health problems. Friends disappeared when they became ill. Information was retained about the drug use.
Negative reactions to psychotropic drug use by family and friends
The young people described negative reactions from their families regarding their psychotropic drug use. Some families were considerate and the young people described worried parents who were concerned about their child’s psychotropic drug use. Other parents did not want their daughter or son to be a psychotropic drug user and were afraid that other people would find out about it. My parents? No, they do not understand the mental health problems and drug use. They tell me to find a job because that will make me better. When I got treatment and was prescribed a psychotropic drug I could not tell them. When I needed money for the psychotropic drug I told them I needed new trousers.
It was uncommon for the young people to tell others about their mental health problems and psychotropic drug use. If they did they needed to defend its use. Everybody, family and friends has an opinion about psychotropic drug use. There is a lot of scepticism. I feel people become sceptical towards me as a user of that kind of drug. They ask about a lot of things, especially side effects. They tell me to stop using the drugs. I meet a number of opinions.
Feeling lonely and stigmatized at school and work
The young people felt alone with their mental distress and psychotropic drug use. They did not dare make contact with other people. One reason was that they were afraid to be confronted with other people’s opinions on mental distress and drug use. They felt that they were not accepted as equal human beings, and that they were different from other people. Generally the young people tried to hide their mental health problems and drug use from school and employers. I have to have tablets in my pocket in case I get a panic-attack. If people at my work had seen me taking the psychotropic drug I may not have been allowed to work with that special work that I love or I may lose my job.
Discussion
The focus of this study was young people aged between 16 and 24 years, with experience of psychotropic drug use. The young people had experienced the effects of psychotropic drug use, both good and bad. The beneficial effects allowed them the possibility of a life, but the side effects included both emotional and physical complaints. A lack of professional support and follow-up from health services was experienced, including professionals who made them insecure about the drug used. They experienced loneliness in relation to family and friends and were afraid of stigmatization.
The young people described beneficial effects of the prescribed psychotropic drugs, which made them feel better and helped maintain their level of health so that they could be part of society. Generally, they described a feeling of well-being and having more energy. On the other hand, they described undesired effects. Although clinical studies of psychotropic drugs in young people are scarce, the beneficial and adverse experiences reported by the young people in this study are in accord with the literature. For example, antidepressants are documented to be useful and well tolerated for acute treatment of anxiety among young people, 16 recommended for distressed mood and reported to be prescribed a lot for young people. 17 Adverse effects such as fatigue and feelings of losing consciousness are reported by young people taking antidepressants. 18 Furthermore, in a recent review among young people, hallucinations and somatic symptoms such as weight gain, fatigue, trembling and loss of cessation of periods for the females are described as adverse effects. 10
The small number of clinical studies and lack of evidence-based guidelines for psychotropic drug use among young people may explain the differences in prescribing patterns and use in this population.19,20 This absence may further underpin the experience of the prescriber relying on and referring to their own clinical experience as a basis for initiating psychotropic drug treatment; this, in turn, may explain a young person’s insecurity about a professional’s knowledge of the drug used and the treatment.
Although antidepressant drug treatment may be a valuable part of treating young people with mental health problems, it is important that the physicians and other professionals facilitating the correct treatment for them. A careful selection of patients, choice of drugs with a potentially lower risk for adverse effects, as well as close health monitoring and healthy lifestyle counselling, are a way of maximizing effectiveness and safety. 21
The young people in the current study were usually prescribed a psychotropic drug by physician in the municipality’s health service. Merikangas et al. report that appropriate drug use is significantly more frequent among young people being treated within the mental health service rather than in a general medical or other settings. 22 The young people in the current study were most often prescribed a psychotropic drug by a physician in the municipality, and experienced that they often did not get any support and follow-up.
There have been reports of attention and concerns about psychotropic drug use among the youngest group of young people.20,23 Off-label use of drugs is in general common and treatment of young people with psychotropic drugs is mainly based on evidence from adults. Too little is known about its safety, especially the long-term effects on growth, and cognitive, emotional and sexual development. 24 In any case, psychotropic drug use among young people is increasing,7,25
Relevant to this, young people may be seen as more biologically vulnerable to exogenous drugs than older people, because of physical, psychological and emotional development. The research, so far, does not reveal any information on the effect of psychotropic drugs on the developing brain or the burden of their side effects on quality of life and on metabolic complications; 26 this may be seen as not beneficial to a developing body and brain. Thus, Byrne et al. emphasize that professionals have to monitor closely young people who are taking psychotropic drugs, and maintain vigilance for those who use drugs for an extended period. 27 Physicians and other professionals involved in the care of young people with mental health problems must pay special attention to the potentially adverse effects of psychotropic drugs when used in this population. 21
In the current study, the young people were aged between 16 and 24 years, and thus seen as young adults; on this basis they could tolerate doses estimated for adults. However, their experience of psychotropic drug use was also from previous years when they were much younger and the side effects were potentially more harmful to their developmental process.
The young people missed available and coherent services. The problems with access to mental health services seem to pose an enduring challenge. The young people missed professionals who had the knowledge and competence to provide support and follow-up. Mental health care within school and the community health service is described as fragmented and inaccessible. Often, PHNs have an office far away in the school building and the young people did not know when they were available. PHNs who work within the school health service are in a position to prevent mental health problems and identify psychotropic drug use among young people. The awareness the PHNs have to this position and responsibility are described in other studies.28,29 In addition, Borup reports that PHNs (school nurses) may reduce students’ proneness to drug use when they experience complaints. 30
The PHNs at the school health service is described not accessible – the young people could not find the office and did not know when she was there. When they had the courage to visit the PHN and present their problem, they felt that she did not want to talk about mental health problems. The experience of a PHN, who talks about a problem unrelated to what the young person needs, could be seen as making her both professionally unpredictable and invisible. Similar barriers are reported McCann et al. in a study among 26 Australian young people with depression. 31 Clancy (p. 73) says ‘The PHNs must be accessible, predictable and visible’ – visible practically and as a professional – in order to offer help. 32 In the Norwegian municipalities, the PHN are responsible for intercepting the signals from young people with mental health problems and referring them for examination and further treatment within specialist health care. 33 Young people have the right to health care as stated in the Act of Patients’ Rights 34 and the UN Convention on the Rights of the Child. 35
Experience of the transition from mental health services designed for children and young people to the specialist adult health service was an inadequate, long and unpredictable process. Cooperation and coherence have been recognized as a problem in the Norwegian Health Services. According to the Coordination Reform, achieving better cooperation and coordinating services is a goal for the central authorities. 36 The Act of Patients’ Rights gives the population the right to equal access to medical treatment of good quality, to help safeguard prevention of illness, and diagnosis, treatment and rehabilitation. 34 The young people in the current study did not feel they received the necessary support and follow-up such as safeguarding the prevention of illness and treatment of good quality. The young people experienced physicians who were unsure which psychotropic drug to use and said that they felt like ‘guinea-pigs’. The young people experienced physicians and health-care personnel who lacked knowledge about the psychotropic drugs prescribed. The absence of evidence and guidelines about psychotropic drug medication for young people may have made the prescribers insecure. Mehler-Wex et al. report a lack of knowledge among the professionals in the municipality about psychotropic drug use among young people. 4 That may have a risk of under- or overdosing and a delayed risk of long-term effects. The most of the psychotropic drug used to young people have been developed and assessed to adults.
The young people described a problematic social life linked to negative reactions to psychotropic drug use from family and friends. Family members indicated their shame at having a child with mental health problems in need of psychotropic drugs. This reaction from significant others as family members is a burden to the young people and adds to their mental health problems. Elkington et al. confirm that, in families with a young person who has mental health problems, this is communicated as a negative trait and the communication occurs via rejection or denial of the young person’s problems. 37 They have reported that young people experience stigma in the form of individual discrimination and rejection within their families and social networks. The stigma associated with mental health problems may remain as a significant barrier to treatment. 38
The young people in this study found friends among others who also had mental health problems. Old friends disappeared when they became ill and new acquaintances were not told about their mental health problems, because they were afraid of their reactions. Negative views of psychotropic drug use are reported to be common in many countries. An overall belief in the harmfulness of antidepressants is particularly seen among young people and those with a lower level of education, although such opinions have decreased over the past decades. 39 Young people who avoid being open about their mental health problems and psychotropic drug use may lose the possibility of treatment and a life at school adjusted to their problems or treatment.
Strengths and limitations of the study
The results of qualitative research are evaluated in terms of trustworthiness, that is, credibility, dependability and transferability.13,14
Credibility involves the evaluation of two aspects: how the investigation was carried out and how credibility was demonstrated. The young people were interviewed individually and their experience showed a rich variety of mental health problems and the need for psychotropic drugs. They represented seven counties, were aged between 16 and 24 years, both females and males, from different backgrounds and with various experiences of psychotropic drug use. This could increase the possibility of shedding light on different aspects of psychotropic drug use. During the analytical process, the interpretations were compared and discussed by the authors until a consensus was reached.
Dependability refers to the stability of data over time.13,14 The data collection was extended to a period of barely four months. The young people were asked the same open-ended question as an introduction, followed by individually adapted follow-up questions.
The descriptions of context, selection and characteristic of participants, data collection and analytical process make possible the reader’s assessment of transferability to other groups and contexts. As a result of the nature of the sample, only eight participants, the transferability of the results could be questioned. It is debatable to what degree the current results can be transferred to other settings or groups of young people using psychotropic drugs. The question is how well the young people in the present study represent or differ from other young people who have used psychotropic drugs. Transferability is enhanced by comprehensive presentation of the subcategories, categories, results and quotations from the transcribed text.
Conclusion
Due to the unfortunate consequences with mental health problems, attention has to be paid to poor mental health among young people and advances are necessary for treatment, care and support of these conditions. The results from the current study have implications for those who work with young people struggling with mental health problems and psychotropic drug use, for example PHNs in the school health service. Further studies are needed to investigate young people’s experiences of psychotropic drug use and why individuals and society do not accept mental health problems among young people. Intervention studies are needed with regard to health promotion programmes aimed at fortifying young people’s mental health.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.
Acknowledgements
We wish to thank you the young people who generously shared their experience with us. The study was approved by the Norwegian Social Science data Service.