
Abstract
This research aimed to explore and describe resilience qualities in Black South African families living with a family member diagnosed with schizophrenia in Bushbuckridge Local Municipality, South Africa. Through a qualitative, explorative-descriptive research design, seven purposefully sampled families were included. Data were collected through semi-structured family interviews and thematically analyzed. Three main themes were identified: experiences of living with a family member diagnosed with schizophrenia, challenges experienced by caregivers, and family strengths and resources used to cope. Findings are essentially emblematic of the general challenges experienced by family members living with a member diagnosed with schizophrenia and resilience qualities, such as family belief system, economic resources, access to disability grants, and Ubuntu. The findings highlight the need for family and community interventions and programs to address challenges faced by families caring for individuals with schizophrenia while also identifying existing resilience qualities and resources, both within and outside the family unit, that families can employ and that can help to inform the development of such programs and interventions.
Schizophrenia is one of the most complex mental health disorders and has the potential to cause significant challenges among millions of people and their families worldwide (Hahlweg & Baucom, 2022). According to Solmi et al. (2023), schizophrenia affected more than 1% of the global population and was regarded as the world’s ninth leading cause of disability based on the Global Burden of Disease study (Charlson et al., 2018). The prevalence of schizophrenia is higher in men compared to women and variations in terms of race have also been noted (Bazargan-Hejazi et al., 2023; Solmi et al., 2023). In Africa, it is estimated that about four to five million people are directly impacted by this psychiatric condition (Purgato et al., 2020). Moreover, schizophrenia is a global phenomenon with an escalating burden in low- and middle-income countries. According to the findings reported by Solmi et al. (2023), approximately 0.22%–0.26% of the South African population had a diagnosis of schizophrenia in 2019. The prevalence of schizophrenia is, therefore, relatively low compared to other mental health conditions (Charlson et al., 2018).
The diagnosis of schizophrenia is determined by two international documents, namely, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) and the World Organization’s International Statistical Classification of Diseases and Related Health Problems (ICD-11; Van Os & Kapur, 2009). According to the American Psychiatric Association (APA, 2022), the DSM-5-TR criteria for schizophrenia is based on five main key domains, which are delusions, hallucinations, disorganized thinking (speech), abnormal motor behavior, and negative symptoms. Furthermore, the DSM-5-TR specifies that hallucinations and delusions should be present for one to meet the criteria of a schizophrenia diagnosis (APA, 2022). Symptoms can be managed through lifelong treatment.
The APA (2020) provides a set of international treatment guidelines that countries should follow in the treatment of patients diagnosed with schizophrenia. These guidelines encompass integrative treatment models, including pharmacological, psychosocial, and community approaches (APA, 2020). In South Africa, the provision of care and treatment of individuals living with Schizophrenia is guided by the Mental Health Care Act no 17 of 2002 (MHCA). Patients with acute mental health conditions such as schizophrenia are admitted to the nearest designated hospital for 72 hours of observation, stabilization, and treatment (Petersen et al., 2016). Such patients may be further referred to specialized psychiatric care facilities for continuous care and treatment (Mental Health Care Act no 17, 2002). Notably, most people in low- to middle-income countries, like South Africa, do not receive optimal care and support to cope with the condition (Thela et al., 2022). Thela et al. (2022) indicate that people living with schizophrenia represent a vulnerable population due to factors such as neglect, lack of insight, socioeconomic status, and other significant social influences that reduce care and quality of life.
Perceptions and attitudes regarding schizophrenia are influenced by various factors, such as cultural values and worldviews within communities and level of education (Boti et al., 2020). Research conducted by Chong et al. (2007) shows that high-income countries perceive schizophrenia from a biopsychosocial view, while low-income countries maintain a traditional perspective. More than 40 studies conducted in eight African countries reported that most people initially considered traditional healing treatment followed by modern psychiatric treatment (Chidarikire et al., 2021). Studies conducted by Fiasorgbor and Aniah (2015) in Ghana found that 66% of the community members attributed schizophrenia to witchcraft/evil spirits and divine punishment. A study that examined the attitudes and beliefs of family members of Xhosa-speaking patients in Africa found that 67% believed that witchcraft or spiritual possession was attributed to the onset of schizophrenia (Dzokoto et al., 2023). Additionally, participants from this study believed that mental illness has a spiritual dimension, such as spiritual attacks (due to envy or jealousy) and spiritual retribution (for committing an offense against another individual or deity). Another study conducted in South Africa showed that some communities have a negative attitude toward schizophrenia given its complex nature (Botha et al., 2006). Communities around the world, therefore, hold different views about the possible causes of schizophrenia (Belayneh et al., 2019). Although the participants expressed strong beliefs in spiritual causes of mental illness, they also acknowledged other factors that could result in mental illness, such as substance abuse, family history, malformation in fetal development, and stressful life events (Dzokoto et al., 2023). Additionally, Dzokoto et al. (2023) and Monnapula-Mazabane and Petersen (2023) found that participants in their studies identified impaired brain function and disability as the driver for mental illness and behavior that deviated from the norm.
In a study conducted in Kwazulu-Natal, South Africa, researchers found that 49% of participants attributed the cause of schizophrenia to supernatural powers, while 39% of participants consulted traditional healers before they considered formal mental health services (Burns et al., 2010). Furthermore, the beliefs and perceptions held by communities and family members may influence help-seeking behavior and adherence to treatment (Agarkar, 2012; Nyanyiwa et al., 2022). Apart from the potential challenges that negative perceptions and attitudes regarding schizophrenia hold, research has focused on the impact of schizophrenia and other mental health conditions on caregivers. These studies have identified various burdens that caregivers face, including high financial expenditure, changes in family roles, and everyday life challenges for the family (Ngabeni & Davids, 2024; Ntsayagae et al., 2019). For example, families impacted by poverty are often overburdened by the responsibility to care for and support family members living with schizophrenia (Rathod et al., 2017). In low socioeconomic countries such as South Africa, the care and support for people living with schizophrenia can adversely affect the family’s financial status by reducing access to primary healthcare services (Schierenbeck et al., 2013).
Moreover, the lack of access to mental health institutions poses major challenges to most families (Thela et al., 2022). In South Africa, the shortage of mental health care practitioners, such as psychiatrists, exacerbates the challenges faced by families in rural areas (Janse van Rensburg et al., 2022). As a result, family members often spend an average of six to 9 hours a day at home providing care and support to the diagnosed family member (Addo et al., 2018; Dirik et al., 2017). Caqueo-Urizar et al. (2017) contend that family members of individuals living with schizophrenia often play a significant role during the onset of schizophrenia. The increased responsibilities associated with caregiving can prevent family members from assuming full-time employment given the responsibility of caring for and supporting people living with schizophrenia (Setlaba et al., 2020). These findings highlight that the burden attributed to being diagnosed with schizophrenia can have adverse consequences on the well-being of individual family members and the family system (Charlson et al., 2018). Shiraishi and Reilly (2019) state that caring for individuals with severe mental health disorders is associated with intense psychological stress and problems due to the complicated nature of the disorder. While some individuals are involuntarily placed in psychiatric facilities, people living with schizophrenia often receive long-term and continued care from their families, which can result in psychosocial burdens for family caregivers (Caqueo-Urizar et al., 2017; Lippi, 2016).
Persons with a diagnosis of schizophrenia may exhibit maladaptive, conspicuous behavior that could be considered unacceptable, difficult, and contradictory to the family’s social norms (Effendy et al., 2023; Ngabeni & Davids, 2024; Soni et al., 2024). In addition, schizophrenia has been associated with impairments in the social information processing abilities required to infer the mental states of others and a lack of motivation to socialize due to avolition. As a result, people with schizophrenia may face communication and socialization challenges and limited social contact with others (APA, 2022; Green et al., 2018). Moreover, families living with a member diagnosed with schizophrenia may experience social stigma, isolation, guilt, and grief that may negatively impact their physical and mental health (Effendy et al., 2023; Soni et al., 2024).
Several studies have also highlighted some of the more positive aspects of caring for a family member with a diagnosis of schizophrenia. A study by Ngabeni and Davids (2024) highlights the mitigative roles that social support, positive caregiver experiences, and interventions can have, thus serving as buffers against caregiver burden and some of the aforementioned psychological and social challenges (Kulhara et al., 2012; Peng et al., 2019). These challenges faced by families in which a family member has been diagnosed with schizophrenia highlight the value in utilizing available resources and support. By focusing on the positive aspects of caregiving, caregivers can enhance family resilience and functioning while also developing their family caregiving abilities (Bhoi & Kumari, 2024; Iswanti et al., 2023; Pan et al., 2024; Peng et al., 2019).
Resilience can be defined and categorized in three aspects: the ability to withstand stressful events, being able to bounce back from such stressors, and growth for future challenges (Baldwin et al., 2011; Bryan et al., 2019). In addition, Ungar et al. (2021) view resilience as the process which sustains human capacity by maximizing psychological, environmental, and social resources in the context of exposure to stress and adversities. Resilience should not be viewed as an independent process, but rather as an interdependent system that works together to provide protective factors and alleviate the effects of any life-threatening disaster (Masten & Narayan, 2012). A family resilience perspective recognizes parental strengths, family dynamics, interrelationships, and social milieu. It considers family stress and challenges as opportunities for fostering healing and growth rather than negative experiences (McCubbin et al., 1996; Walsh, 2012). Prominent attributes, such as having a positive outlook, spirituality, spending quality time with family, social support, and mutual recreational interests, significantly contribute to healthy families and familial resilience (Black & Lobo, 2008).
According to Walsh (2006; 2016; 2021), there are three fundamental domains and processes essential to family resilience, which include the belief system, organizational processes, and communication process. First, Walsh (2021) refers to a family belief system as an instance where the family helps each other to make meaningful experiences from adverse events and maintains a positive outlook and purpose. Walsh (2021) further postulates that in a family organization, resilience is fostered through strong leadership, stability of the structure, mutual connections, and how social and family resources are utilized. Second, family organizational patterns refer to various systems that contribute to ways in which family resilience is bolstered. Families with a high sense of mutual support and cohesion are often in the best position to be resilient during adversities (Walsh, 2016). Lastly, Walsh (2016) indicates that family resilience is fostered through communication processes, which include information clarity, sharing both positive and negative emotional experiences, and engaging in collaborative problem-solving.
The Present Study
Studies on resilience stress that resilience cannot be conceptualized solely at an individualized level but rather as an interactional multisystemic process that helps both individuals and families regain, sustain, and improve after being exposed to stress or adversity (Fletcher & Sarkar, 2013; Theron et al., 2013; Ungar & Theron, 2020). According to Bishop and Greeff (2015), studies on resilience in families in which a member has been diagnosed with schizophrenia are limited in the South African context. Most studies in this area have focused on the burden and challenges faced by families in which a member has been diagnosed with mental health conditions, such as schizophrenia. These limitations indicate that the existing research does not adequately reflect the experiences of Black South African families and highlights the need for further research in this regard, especially considering that the majority of South Africans are Black. According to the Statistics South Africa (2021) Mid-year Population Estimates report, the Black African population is in the majority (48.6 million) and constitutes approximately 81% of the total South African population. There is a growing need for research on resilience qualities that are positively attributed to family adaptation; however, there are few studies conducted in South Africa specifically examining the resilience qualities of families with a member diagnosed with schizophrenia (Bishop & Greeff, 2015; Haddad, 2008), and there is a void in research on this phenomenon specifically within Black South African families. Due to the extensive focus of the literature on the burden placed on families in which a member has been diagnosed with a mental illness, there is a great need to identify qualities that may help families be resilient while caring for a family member diagnosed with schizophrenia. Exploring and describing the resilience qualities in Black South African families living with a family member diagnosed with schizophrenia can promote understanding of the phenomenon and contribute to the knowledge base in this regard. Therefore, this qualitative study aimed to explore and describe the resilience qualities in Black South African families living with a family member diagnosed with schizophrenia in Bushbuckridge Local Municipality, South Africa.
Method
Approach and Design
A qualitative, explorative-descriptive research design, as outlined by Hunter et al. (2019) was employed. The major strength of a qualitative research approach is its ability to explore and delve deeply into a subject under investigation (Carlsen & Clenton, 2011). Exploratory studies are conducted when the researcher is exploring phenomena that are not well understood (Hunter et al., 2019; Rumnill et al., 2011). Rumnill et al. (2011) further defines the descriptive approach as studies in which the researcher is interested in documenting the salient features (e.g., events, behaviors, attitudes, processes, and beliefs) of the phenomenon of interest. This design focuses on direct, in-depth descriptions of people’s experiences, specifically the “who, what, and where” without theorization or abstraction as a focal point (Ghorbani & Matourypour, 2020; Neergaard et al., 2009). Therefore, this design was selected because it enabled the researchers to gather rich information and examine the study’s research objective.
Population and Sampling
The population comprised Black South African adult family members living with a schizophrenia-diagnosed family member, from the age of 18 years and older, as defined by the WHO (2016), who resided in Bushbuckridge Local Municipality, Mpumalanga Province. According to the latest available census data (Statistics South Africa Community Survey, 2016), Bushbuckridge Local Municipality has a population of about 548, 760; of this population 99% are Blacks. The average household size is four persons per household. Of these households, 11.9% have access to piped water, 6.8% have access to a flush toilet connected to a sewerage system, 7.5% have weekly removal of refuse, and 93.9% have electricity for lighting purposes. The area has an unemployment rate of 52.1%. Notably, there are numerous ethnic groups in Bushbuckridge, including the underrepresented Mapulana people, who speak Sepulana and are endemic to this area (Mashile et al., 2019).
A purposive sampling technique was used to sample participants (Clark et al., 2021). Purposive sampling refers to the deliberate selection of participants based on their pertinent characteristics (Etikan et al., 2016). The participants had to comply with the following inclusion criteria: (1) willingness to participate as participation was voluntary, (2) be an adult family member of a Black South African family living with a family member diagnosed with schizophrenia for at least 36 months, (3) reside within the Bushbuckridge Local Municipality, and (4) be fluent in English, Xitsonga, Isiswati, and Sepedi as interviews were conducted in these languages.
Sample
Demographic Profile of Participants From Family Interviews.
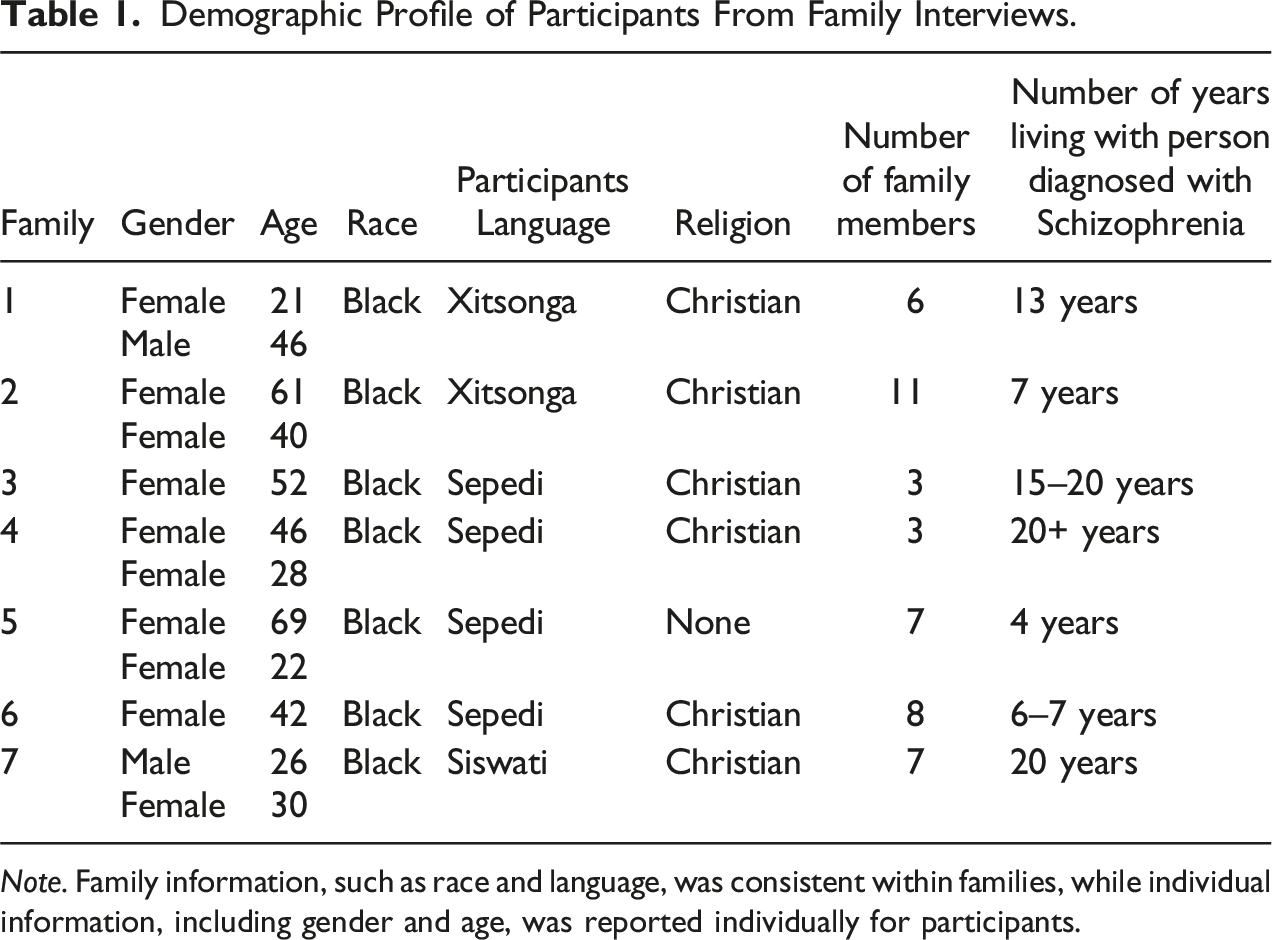
Note. Family information, such as race and language, was consistent within families, while individual information, including gender and age, was reported individually for participants.
Procedures
The study received institutional approval from the Health Research Ethics Committee of the North-West University (NWU-00222-22-A1). The researcher recruited the participants through the assistance of the Mpumalanga Mental Health Society (MMHS), which is one of the leading organizations in mental health services in the Mpumalanga Province. The MMHS agreed to act as both the gatekeeper, providing researchers with access to potential participants, and as a mediator, facilitating contact between the researchers and potential participants (Kristensen & Ravn, 2015).
Potential participants were contacted telephonically by MMHS, on behalf of the researcher, and determined their willingness to participate in the study. An independent person who was not involved in the study facilitated the informed consent process. All the participants who had indicated willingness to be part of the study were contacted by the independent person to facilitate the informed consent process. The study only commenced after participants agreed, signed, and returned the informed consent forms. Once the informed consent process was concluded, the independent person provided the researcher with participants’ contact information. The researcher then contacted participants to make appointments for family interviews to begin the data collection process.
Data Collection
Data collection involved using a demographic information form, semi-structured family interviews, and field notes.
Demographic Information Form
Participants were requested to complete a demographic information form before the start of the interview. The form included age, gender, number of family members, period spent living with a family member diagnosed with schizophrenia, and religion. The demographic data provides a general profile of the research participants as outlined in Table 1. Data were anonymized to protect the identity and privacy of the participants.
Semi-Structured Family Interviews
Eggenberger and Nelms (2007) state that family interviews are useful for collecting rich, family-level data on family experiences and meanings, as well as for uncovering hidden phenomena. Based on Eggenberger and Nelms’s (2007) descriptions of family interviews, the researcher conducted semi-structured family interviews to collect data from adult family members living with a family member diagnosed with schizophrenia. Participant convenience was ensured by allowing each family to indicate their preference for interviews to be conducted at their homes or other appropriate locations for data collection (private, quiet, available seating, etc.).
A total of seven semi-structured family interviews, each lasting between 45 minutes and one hour, were conducted at participants’ homes, as per their preference. Two families were Xitsonga-speaking, four were Sepedi-speaking, and one was a Siswati-speaking family. The researcher is fluent in all the languages spoken in Bushbuckridge; however, a translator, who had to sign a confidentiality agreement, was present in all the interviews to provide correct substitution of words and prevent the misinterpretation of words. Only the participating family members, first author, and translator were present during the interviews.
The following questions were included in the interview schedule and were evaluated by qualitative experts prior to use: (1) Please tell me about your experience of living with a family member diagnosed with schizophrenia. Can you share some examples of what you’ve experienced? (2) What kind of difficulties have you faced while living with a family member diagnosed with schizophrenia? Can you share some examples of difficulties you’ve experienced? (3) What resources and strengths do you think your family uses to deal with the difficulties of living with a family member diagnosed with schizophrenia? Can you share examples of how your family uses these resources or strengths?
An electronic voice recording device was utilized during the interviews. The first author transcribed the interviews to immerse himself in the data and prepare the data for analysis. Transcripts were sent to the co-coder for independent analysis.
Field notes
Field notes were taken during interviews to capture important information useful during data analysis that was not captured on the audio recording, such as non-verbal communication. Sutton and Austin (2015) contend that handwritten field notes can assist researchers in capturing behaviors, non-verbal cues, and impressions that may not be adequately captured through audio recording. The notes were kept for audit trail purposes and included in the data for analysis. These notes were scanned and stored in the researcher’s passworded encrypted computer.
Data Analysis
The data were inductively analyzed using six steps of thematic analysis developed by Braun and Clark (2021): (1) familiarizing yourself with the data; (2) generating initial codes; (3) searching for themes and codes to identify patterns; (4) reviewing themes; (5) defining and naming themes; and (6) producing the report in a systematic report format. Data were manually and independently analyzed by the first author and an experienced co-coder. The co-coder had to sign a confidentiality agreement prior to receiving data and was instructed to delete all data when data analysis concluded. Once the analysis was completed, the first author and the co-coder converged to compare their themes and determine that consensus had been reached to ensure trustworthiness regarding analysis.
Trustworthiness
To ensure trustworthiness, the authors considered the criteria for credibility, dependability, transferability, and confirmability as identified by Guba and Lincoln (1985). Credibility refers to confidence in the truth of the findings (Guba & Lincoln, 1985). To ensure credibility, the authors employed researcher reflexivity through active and critical reflections on processes, enhancing awareness of their own beliefs, and bracketing any biases. Furthermore, a literature integration was conducted to compare the findings with sources of evidence. Moreover, the use of a co-coder, a proper audit trail, and the provision of in-depth descriptions of the processes contribute to the study’s dependability, which can be understood as the consistency of findings (Guba & Lincoln, 1985). Confirmability, which Guba and Lincoln (1985) associate with the neutrality of findings, was ensured through reflexivity and a proper audit trail, as described above. Finally, transferability refers to a comprehensive description of the sample and context (Guba & Lincoln, 1985). Therefore, thick descriptions of the study sample and context are provided to facilitate judgments of the findings’ potential applicability to other contexts.
Results
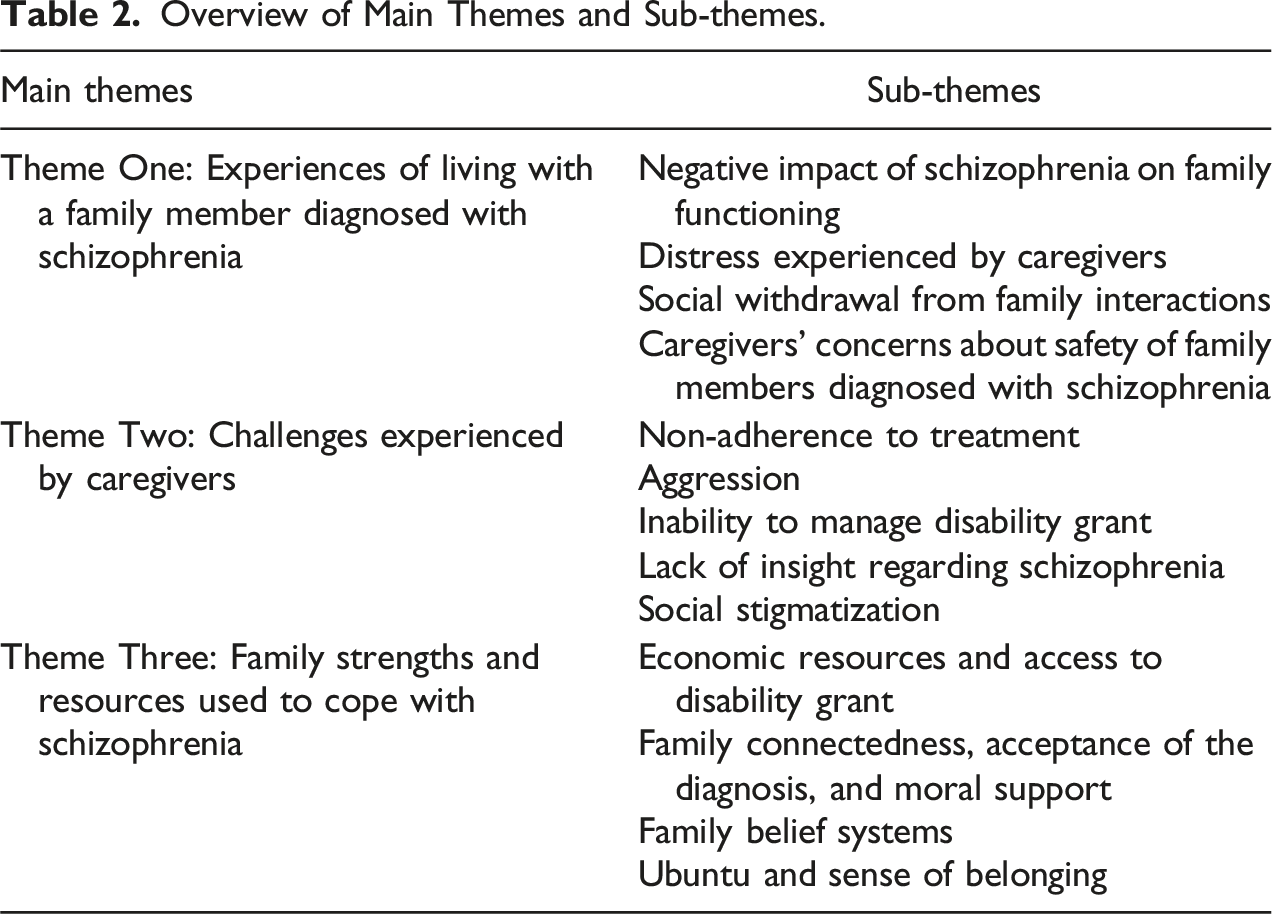
Overview of Main Themes and Sub-themes.
Theme One: Experiences of Living with a Family Member Diagnosed with Schizophrenia
Participants shared various experiences of living with a family member diagnosed with schizophrenia. They gave an account of the impact of schizophrenia on their family functioning and the daily emotional and financial distress that is accompanied by caring for family members with the illness. Sub-themes include the following:
Negative Impact of Schizophrenia on Family Functioning
Participants indicated that they often experienced disruption of family well-being when family members experienced psychotic episodes because of schizophrenia: “There are times where things are normal and smooth but once it starts, everyone at home will be disturbed by the instability” (P 6); “When the illness starts, he insults all of us including neighbours” (P 3); “There are days when things are hard…” (P 3); “…he claims that there are things hurting him at night and sometimes he talks alone” (P 5); “Sometimes when he sleeps, he makes noisy sounds at nights of which when we check him, he does not know what is happening” (P 5).
Distress Experienced by Caregivers
Participants experienced various forms of distress, such as feeling helpless or experiencing stress, due to living and caring for a family member diagnosed with schizophrenia: “…it is sometimes depressing for the whole family because of his condition” (P 1); “I am always stressed and emotionally overwhelmed because I don’t know what else to do to help him” (P 5); “As a family sometimes we don’t know what to do to help him” (P 1); “Sometimes we can struggle to sleep at night because of the noises he makes” (P 1); We live in fear because he threatens us and tells us that the house belongs to his father” (P 5); “…sometimes it is emotionally overwhelming” (P 4).
Social Withdrawal from Family Interactions
This sub-theme of social withdrawal from family interactions represents participants accounts of social disconnection from family members diagnosed with schizophrenia. This was evident through several quotes demonstrating a lack of engagement in family interactions: “Basically, when you are with him, he doesn’t usually talk much at our place of residence” (P 1); and he seems to be afraid to talk but when he is outside there in the village with other people, he does talk a lot” (P 1); “He is always quiet and does not like talking to us. At time he locks himself in the room” (P 6); “We do not have a healthy relationship with him” and “It seems like he lives in his own world” (P 5); “Sometimes he sits the whole day without having interest and energy to interact with any of us” (P 2).
Caregivers’ Concerns About Safety of Family Members Diagnosed with Schizophrenia
The sub-theme emanates from the participants’ continuing concerns and uncertainty about the personal safety of family members diagnosed with schizophrenia, especially outside of the home environment or in the absence of caregivers. They shared the following: “Every day early in the morning around 6 am, he goes out” (P 1); “He travels by foot for long distances without knowing where he is going” (P 2); “There will be a disaster if he is left alone in the house” (P 4); “I cannot go to school, I do not have social life as I am always caring for them” (P 4); “My concern is that he always escapes from the hospital when he is admitted” (P 5); “The other challenge is that he does not want to stay at home and we are always worried about his safety” (P 6).
Theme Two: Challenges Experienced by Caregivers
The theme of challenges experienced by caregivers, along with its sub-themes, unpacks challenges shared by the participants during the interviews. It covers a wide range of challenges faced by caregivers while caring for family members diagnosed with schizophrenia which include non-adherence to treatment, aggression, misuse of disability grant, lack of insight regarding schizophrenia, and social stigmatization.
Non-adherence to Treatment
Most of the participants characterized non-adherence to treatment by their family member with schizophrenia as a daily struggle: “At first, he refused to be refused to be injected…” (P 7); “The problem is that he is on treatment which he receives from the clinic, but he does not adhere to it” (P 2); “Sometimes we even go to an extent of running after him to take treatment”. (P2); “He does not want to take his medication and leaves home early in the morning” (P 1); “My son does not adhere to his treatment and at the hospital, they think I do not give him treatment, sometimes I go to the extent of mixing food with treatment” (P 5).
Aggression
Many participants reported that they experienced aggression, violent behavior, and destruction of property perpetuated by the family member living with schizophrenia: “…he is always aggressive and violent at home.” (P 2); “…becomes angry and aggressive when he defaults his medication…He once physically assaulted our late brother with a weapon” (P 3); “My brother often threatens to stab us with a knife when he is angry, sometimes he appears to be a danger to the family” (P 4); Life is difficult, he does not want to understand, he often burns his own clothes, blankets and beds” (P 5); “…he goes around the community and destroy other people’s properties” (P 5).
Inability to manage disability grant
The sub-theme emerged from what participants shared about the financial difficulties emanating from an inability to manage disability grant received by the relatives with schizophrenia: “The main challenge is that when his grant is paid, he does not want to buy anything essential for himself, and we have never seen money, his disability grant card is with the loan shark” (P 3); “My son used to receive disability grant, but he did not want us to manage it for him. He always demands money from us and if I do not have, he forcefully goes to my bedroom to search for it” (P 5); “The grant is being managed by his daughter because [he] does have capacity to handle money” (P 2).
Lack of insight regarding schizophrenia
Many participants observed a lack of insight into the mental health condition of relatives diagnosed with schizophrenia. The following quotes highlight how this lack of awareness and insight impairs functioning, especially in the social domain. Participants said: “The main challenge is that he never acknowledges that he has a mental problem” (P 6); “He wears very dirty female clothes without any problem” (P 7); “He seems to be confused and lack understanding of what is happening with him, especially at night” (P 1).
Social stigmatization
The sub-theme of social stigmatization emerged from families’ experiences of negative perceptions directed towards them because of living with a family member diagnosed with schizophrenia. The following quotes demonstrate participants accounts of social judgments, and lack of social support: “People will call you names because we live with someone who is mentally challenged” (P 1); “At the hospital they think I do not give him treatment” (P 5); “His own family of origin neglected him because of the mental health condition” (P 7); People judge us based on his mental status” (P 2).
Theme Three: Family Strengths and Resources Used to Cope
Regarding strengths, resources, and resilience qualities which families apply to cope with schizophrenia, the following sub-themes emerged during the interviews: economic resources and access to disability grant, family connectedness, moral support, family belief systems, and Ubuntu and sense of belonging.
Economic resources and access to disability grant
Participants shared their views on the importance of access to a disability grant and other financial resources. Most indicated that the grant served as the resource they used to mitigate economic challenges associated with caring for their family member: “There are certain periods where he needs to be transported to the clinic and one of the family members is able to pay for the costs because she is employed, and the grant also helps a lot” (P 1); “The grant is helpful towards the needs of the family” (P 2); “My sister recently got a job which also contributes to the groceries that covers him” (P 3); “Access to the grant serves as a resource that the family uses to thrive” (P 4).
Family Connectedness, Acceptance of the Diagnosis, and Moral Support
This sub-theme emerged from multiple participant responses affirming family communication, acceptance of the diagnosis, and moral support as means to coping with difficulties associated with schizophrenia. Participants’ quotes especially focused on the importance of these aspects within the family and toward the person diagnosed with schizophrenia. Participants said: “We always try to support each other” (P 3); His condition requires his family hence we think other people may get tired” (P 3); “I have learned that [I] must accept their current mental condition” (P 4); “We communicate with my children about ways to deal with his condition” (P 5); “We believe that caring for him is way of expressing love and support” (P 6); “All family members show love, concern and ensures that he has been eaten food” (P 7).
Family Belief Systems
Several participants indicated that they engaged in various religious practices to cope with the responsibility of caring for family members diagnosed with schizophrenia. The practices included performing ancestral rituals and praying to God: “God is the one that keeps me to continue helping him and sometimes I consult the ancestors to ask for guidance and strength” (P 5); “We receive emotional and spiritual support from the church” (P 1); “Trusting in God makes us feel pity for him and we pray for him for improvement of the mental health condition” (P 7); “Also receives spiritual support from the pastor, they come to offer support at home” (P 4).
Ubuntu and Sense of Belonging
The majority of the participants mentioned the concept of Ubuntu as a factor which fosters family resilience when they are faced with the challenges of caring for a family member with schizophrenia. Central to African psychology is the tenet of Ubuntu, which is defined by humanness epitomized by the phrase: “a person is a person through other people” (Chitindingu & Mkhize, 2016). Participants shared: “We continue to look after him because he is part of the family, and being unwell does not mean we should leave him” (P 1); “To be honest, we continue care for him because he is our uncle and family” (P 2); “It requires a heart and resilience” (P 3); “Your child is your child there is nothing you can do” (P 5); “The way our late mother used to care for all of us encourages us continue caring for him” (P 6).
Discussion
The aim of this study was to explore and describe resilience qualities in Black South African families living with a family member diagnosed with schizophrenia in Bushbuckridge Local Municipality. The goal was to promote a better understanding of family resilience in this context and contribute to the existing knowledge on this phenomenon. Existing literature highlights challenges faced by family caregivers of individuals with mental health conditions, underscoring the need for research on the experiences and resilience qualities of Black South African families caring for persons with schizophrenia. The thematic analysis of family interview data revealed three main themes, reflecting participants’ experiences of living with a family member diagnosed with schizophrenia, caregiving challenges, and the family strengths and resources they used to cope. Our findings serve as supporting evidence for prior research on family resilience in caring for a family member with a diagnosis of schizophrenia, while also offering some novel insights into this phenomenon, specifically among Black families in South Africa. Our findings may, therefore, be utilized to expand cultural understandings of caregiver adversity, coping, and resilience and encourage the development of family and community interventions focused on assisting those affected by schizophrenia in rural South Africa to better understand the complexities of the condition.
Family resilience appears to be a key focus area of schizophrenia research within cultural contexts, and several studies report on the experiences of family caregivers in this regard (Belo Fernandes et al., 2021; Bishop & Greeff, 2015). Our findings provide valuable insights into family caregivers’ negative experiences of schizophrenia’s impact on family functioning, distress, social withdrawal, and concerns about the safety of the family members diagnosed with schizophrenia. The negative impact that schizophrenia has on family functioning has been supported by Pan et al. (2024). The presence of psychosis among family members can also lead to substantial burden, disrupted family social functioning, and poor family interactions, possibly due to a lack of cooperation in caregiving responsibilities and insufficient involvement in professional care (Fusar-Poli et al., 2022; Pan et al., 2024). In connection with the findings by Hodgins (2017) that the behaviors associated with schizophrenia may have negative consequences for family functioning, our participants’ experiences predominantly centered on the impact these behaviors have on family functioning. Furthermore, Effendy et al. (2023) report that these behaviors may result in caregivers experiencing psychological burden and stress.
Families from our study experienced various forms of distress because of the dynamics of living with a relative with severe mental illness and felt unsure about what to do or how to handle certain situations. Similarly, Pan et al. (2024) contend that family members caring for a relative diagnosed with schizophrenia experience psychological distress and initially may experience a sense of feeling unprepared and helpless. The experiences of emotional distress and burden in caring for a family member with a diagnosis of schizophrenia have also been reported by Soni et al. (2024) and Effendy et al. (2023). Effendy et al. (2023) found experiences of guilt, sadness, anger, and despair among the participants of their study, while Viertiö et al. (2021) found that families caring for relatives with mental health conditions are likely to experience depression, anxiety, and other mental health challenges because of the everyday stresses. It was evident from this study that schizophrenia negatively impacts both patients and their families’ psychological well-being, which may in turn result in fear, overwhelming stress, and depression. In addition to emotional and psychological distress, participants from the study conducted by Effendy et al. (2023), as well as studies by Soni et al. (2024) and Bhoi and Kumari (2024), mention physical exhaustion and burdens among participants caring for a family member with a diagnosis of schizophrenia. While Bhoi and Kumari (2024) note that caregiver resilience plays an important role in managing psychological distress, Ntsayagae et al. (2019) suggest that distress may result from caregiving demands and may be exacerbated by the social impairments associated with schizophrenia, given that schizophrenia causes social withdrawal from interacting with people (Green et al., 2018; Lippi, 2016; Ntsayagae et al., 2019).
Our findings highlight that caregivers observed the family member diagnosed with schizophrenia withdrawing from social family interactions. These findings are consistent with the findings of the study conducted by Effendy et al. (2023) in Indonesia, which noted that caregivers experienced withdrawal by the family member diagnosed with schizophrenia. According to Effendy et al. (2023), participants from their study did not realize that self-withdrawal, the inability to take care of themselves, and lack of motivation, talking, and socialization were also part of the symptoms of schizophrenia. Similarly, the narratives of participants from our study suggest that they were better at identifying positive symptoms of the disorder. As people diagnosed with schizophrenia may prefer solitary activities, the family’s ability to communicate and establish meaningful communication and relationships with the affected family members may be compromised (Estradé et al., 2023; Lysaker et al., 2022). From our study’s findings, it was evident that social withdrawal by a diagnosed family member negatively impacted the family’s communication networks, resulting in social disconnection, poor interaction, and social isolation, as also noted by Fulford and Holt (2023).
Apart from withdrawal, the current study found that caregivers were often concerned about the safety of their family members. Studies indicate that caregivers living with a family member diagnosed with schizophrenia are often concerned for the well-being, whereabouts, and personal safety of family members (Bhoi & Kumari, 2024; Commey et al., 2022; Ngabeni & Davids, 2024). Dzokoto et al. (2023) found that from participants’ perspective, mental illness could be associated with dangerous physical behavior and mentally ill individuals were subjectively viewed to be more prone to violence and tendencies to harm themselves and those around them. People with schizophrenia may lack insight into the importance of safety and often leave their homes without the knowledge of their caregivers (Long et al., 2022). Furthermore, Pan et al. (2024), Soni et al. (2024), and Ngabeni and Davids (2024) reported that caregivers also experience concerns regarding the future care of family members with a diagnosis of schizophrenia, should something happen to them; however, this sentiment was not evident in the experiences shared by the participants in our study. Although social withdrawal and non-treatment adherence emerged as two distinct sub-themes in our study, Estradé et al. (2023) and Dzokoto et al. (2023) further highlighted that communication challenges caused by social withdrawal may also impact adherence to the treatment of schizophrenia.
The caregivers that participated in our study reported experiencing several challenges, including non-adherence to treatment, aggression, inability to manage disability grants, lack of insight regarding schizophrenia, and social stigmatization. Overall, these caregiver challenges serve as supporting evidence to findings reported by Soni et al. (2024), Ngabeni et al. (2024), and Effendy et al. (2023). Our findings concerning challenges with treatment adherence are consistent with findings from the study by Soni et al. (2024). Although Ntsayagae et al. (2019) emphasize the role of family members in administering, monitoring, and ensuring treatment adherence, as well as avoiding relapse, most families in our study experienced challenges in ensuring treatment adherence, as persons diagnosed with schizophrenia refused or resisted treatment and did not understand the importance of treatment adherence. While Soni et al. (2024) link findings from their study to the lack of insight and compromised judgment associated with schizophrenia, Semahegn et al. (2020) suggest that non-adherence to medication is prevalent among patients with major psychiatric disorders. Poor treatment adherence for schizophrenia may, however, be further compounded by healthcare facility limitations, financial constraints, family religion, and communication challenges (Dzokoto et al., 2023; Effendy et al., 2023; Estradé et al., 2023; Ngabeni & Davids, 2024; Soni et al., 2024). Chen et al. (2024) noted that family knowledge about treatment may be associated with increased family resilience. However, negative attitudes and poor adherence are common treatment challenges that may lead to relapse, which have been associated with aggressive and violent behaviors (Chen et al., 2024; Monyaluoe et al., 2014).
Although context-dependent aggression emerged among the caregiver challenges identified in our findings, it was not exclusively mentioned in relation to treatment adherence. Nonetheless, our findings corroborate with research suggesting that the subjective experience of aggression and violent behaviors has been indicated by family members caring for a relative with schizophrenia in South Africa (Ngabeni et al., 2024). Our findings also align with the work of Monyaluoe et al. (2014), indicating that persons with schizophrenia may exhibit violent threats and acts, as well as destruction of property, causing harm not only to their families but also to people in their communities. Moreover, Effendy et al. (2023) noted that family caregivers were terrified when these individuals became agitated. It seems reasonable to argue that family members may struggle to express concerns, negotiate treatment adherence, and set boundaries with these individuals, which was reflected in our participants’ accounts of challenges in managing grant funds (Green et al., 2018; Monyaluoe et al., 2014; Ntsayaga et al., 2019).
Our findings provide valuable insights into the challenges that caregivers experience with people living with schizophrenia in managing disability grants. While Soni et al. (2024) and Effendy et al. (2023) emphasize the financial challenges and concerns in caring for a family member with schizophrenia, our findings provide novel insights regarding the challenges caregivers experience regarding grant fund management, as grant recipients did not utilize these funds effectively consequently demanding more financial support from families. In South Africa, applicants can receive up to R2, 180 per month on a permanent basis if their disability lasts longer than 12 months or for a temporary basis for a disability lasting between 6–12 months (South African Government, 2002). Our findings regarding financial challenges are supported by existing concerns regarding the ability and skills of persons with schizophrenia to manage their money independently, and findings stating that some caregivers do not feel comfortable letting persons with schizophrenia make their own financial decisions due to the lack of insight and compromised judgment associated with schizophrenia (Soni et al., 2024).
Interestingly, concerns regarding the lack of insight were also identified as one of the challenges faced by the participants in our study; however, participants’ responses suggested that family members with schizophrenia denied their condition and its impact on their functioning. While our participants appear to have emphasized the impact that this lack of insight has primarily on social functioning, findings from existing studies highlight challenges associated with safety, decision-making, and treatment adherence (Long et al., 2022; Soni et al., 2024). Participants in our study also elaborated on their experiences of social stigmatization, highlighting the social implications of living with a family member diagnosed with schizophrenia.
Our findings regarding caregiver challenges with social stigmatization corroborate with the findings of studies by Bhoi and Kumari (2024), Chen et al. (2024), Effendy et al. (2023), Iswanti et al. (2023), Pan et al. (2024), and Soni et al. (2024). Stigmatization influences how families perceive themselves, the person living with the illness, and the community and may result in feelings of shame, guilt, and social isolation (Pan et al., 2024; Sadock & Sadock, 2014). Research has shown that social stigma not only affects people who experience severe mental illness but also their relatives, close friends, and the entire family, who often experience discrimination and prejudice associated with caring for a member with a chronic mental health condition (Buizza et al., 2007; Effendy et al. 2023). Aside from the stressors and adversities faced by the participants in our study, as well as family caregivers globally, familial strengths and external resources used to cope with the caregiving role and care for a family member with schizophrenia have also emerged.
Our findings highlight the importance of economic resources and access to disability grants, family connectedness, acceptance of the diagnosis, moral support, family belief systems, and Ubuntu and sense of belonging as salient family strengths and resources used to cope when caring for a family member with schizophrenia. Overall, these findings serve as supporting evidence to existing literature on family resilience and coping in caring for a person diagnosed with schizophrenia (Bhoi & Kumari, 2024; Chen et al., 2024; Effendy et al., 2023; Iswanti et al., 2023; Pan et al., 2024; Soni et al., 2024). While strengths and resources emerged as separate themes in our study, Bhoi and Kumari (2024) note similar aspects among the process of developing family resilience, which entails: (1) surviving the current situation, (2) changes in family structure, (3) attempting to accept the family member, (4) seeking positive meaning, and (5) supporting others in the family. Interestingly, our primary themes and sub-themes share significant overlap with nearly every stage of this resilience development process. Similar to the experiences reported by our participants, Effendy et al. (2023) notes that financial resources play an important role in family resilience. These findings are also supported by the results from a South African study by Zwane et al. (2022), which suggests that access to grants can strengthen families and improve livelihoods in rural areas, thereby enhancing their resilience.
Family connectedness, acceptance of diagnosis, and moral support were identified as resilience qualities in Black South African families living with a family member diagnosed with schizophrenia. Positive communication and information-seeking among family members are noted along with social support, open communication, spiritual and/or religious resources, and optimal family functioning as some key resilience qualities that support family members in dealing with the complexities of caring for a family member with schizophrenia (Martinez et al., 2023; Parks et al., 2018). Family connectedness can be seen as a strength that binds the family together in times of disruptions, such as those caused by mental health challenges (Danhouse & Erasmus, 2020). In addition, acceptance of the diagnosis and seeking moral support from other family members are strengths for most participating families in this study. Acceptance, which appears to be a central theme of caregiver coping, aligns with research by Pan et al. (2024), Bhoi and Kumari (2024), Soni et al. (2024, and Iswanti et al. (2023). In addition, studies conducted in Turkey by Ata and Doğan (2018) found that seeking social support and information serves as a coping mechanism for families caring for a person with a mental health condition. Taken together, these findings highlight the need for effective family communication, acceptance, and social support to empower families, as well as equip them with the skills, strengths and resources needed when caring for a member with a diagnosis of schizophrenia.
Family belief systems were also identified as a potentially useful resource. Family studies conducted in various African countries found that the family belief system plays a significant role in the understanding and treatment of schizophrenia given that they adopt both a traditional/faith-based model and a biomedical model of treatment (Van der Zeijst et al., 2023). Most participants from our study mentioned that they prayed to God, asking for the strength to heal their family members. Modise et al. (2021) found that praying and spiritual support from faith-based institutions are deemed the most reliable coping mechanisms by families caring for relatives with schizophrenia. Thus, prayer and belief in God appear to play an important role in helping families cope with challenges posed by living with a relative with schizophrenia (Monama & Basson, 2017). Another study, conducted in the Mpumalanga Province by Ngobe et al. (2021), suggests that it is common for Black indigenous families living with a relative diagnosed with a psychotic disorder to consult ancestors and traditional healers (Christian & Barbarin, 2001).
Lastly, the findings in this research suggest that most families cope with the dynamics of living with a relative diagnosed with schizophrenia due to the deeply embedded concept of humanity (Ubuntu). Coetzee and Roux (2003) refer to Ubuntu as African humanism, which involves sympathy, care, support, respect for others, consideration, kindness, and sensitivity to the needs of others. The above sentiments were echoed by all participants’ understanding of the importance of being present for their family members during difficult times of mental health challenges and were evident in all participants’ reasons for continuous care and support of their families despite the everyday complex difficulties.
Notably, taken together, our three themes include stressors and adversities as well as resources and familial strengths, which aligns with the notion that resilience is a process that exists in the context of exposure to stress and adversity (Ungar et al., 2021). Furthermore, the findings support the view that resilience is an interactional, multisystemic process that facilitates individual and familial improvement when exposed to stress or adversity (Fletcher & Sarkar, 2013; Ungar & Theron, 2020). These findings also align with the family resilience framework by Walsh (2006), as the family belief system (specifically regarding transcendence and spirituality), family organizational patterns (reflected in participants’ response to changing circumstances, roles and responsibilities, connectedness, and making use of social and economic resources), and family communication processes (represented culturally in the form of Ubuntu) were identified as prominent resilience qualities. However, the findings provide a unique cultural contribution from the perspective of Black South Africans, which is clearly reflected in the themes and sub-themes.
Limitations and Recommendations
The study was conducted in Bushbuckridge Local Municipality and is limited to this geographical context. However, the description of the procedures regarding the research process should allow other researchers to replicate the study in other similar contexts. The study identified a need for research regarding Black families in South Africa; however, the sample is not representative of all Black cultures in South Africa. Children were not included as participants; however, their input could provide a more holistic understanding of family experiences regarding the phenomenon and could add value to data gathering by providing a different perspective. Most of the sample (92%) in this study was Christian, which limits the diversity of perspectives in relation to spirituality and religion. It should also be noted that the findings provide a snapshot of the experiences of participants during a specific point in time.
The inclusion of diverse belief systems can also provide other perspectives related to resilience qualities. Longitudinal research will be valuable in providing insight into the phenomenon over a longer time period. There is a need for studies to develop family and community interventions focused on assisting those affected by schizophrenia in rural South Africa to better understand the complexities of the condition. Specifically, interventions targeted at empowering family caregivers appear promising (Iswanti et al., 2023). Furthermore, as our overall findings largely overlap with the family resilience development process described by Pan et al. (2024), it may be valuable to explore the extent to which this process may be transferable to other contexts, especially in terms of chronology, which could help to tailor interventions to equip families with the skills required when they need it most. Finally, community psycho-education programs may also help to reduce the social stigmatization experienced by families caring for members diagnosed with schizophrenia in rural areas.
Conclusion
This study provides insight by contributing to the limited existing body of knowledge on family resilience qualities among Black South African families living with members diagnosed with schizophrenia. Similarities and differences from our findings are clearly in the literature, as reflected in the discussion above. A noteworthy example is that the findings allude to stressors and adversities, underscoring the need to develop and/or employ familial strengths while also utilizing available external resources to handle stressors and adversities. This supports the view that resilience is a process initiated by exposure to stress and adversities (Ungar et al., 2021). Another interesting example is that the findings align with the family resilience framework of Walsh (2006) regarding prominent familial resilience qualities. Our overall findings also align with the family resilience development process described by Pan et al. (2024) and highlight the need for interventions aimed at empowering families (Iswanti et al., 2023). In addition, the findings provide a unique insight into culture- and context-specific experiences, stressors, adversities, and familial resilience qualities regarding the phenomenon. Examples of this include the role of traditional beliefs in social stigmatization, context-specific economic challenges and resources, and the importance of Ubuntu. With this in mind, the findings highlight the importance of guarding against “one-size-fits-all” approaches to interventions and programs for families residing with a family member diagnosed with schizophrenia and shed light on the need for context-specific and culturally appropriate family and community interventions and programs. Taken together, our findings along with the supporting literature suggest that the development of interventions may be guided by principles that promote a better understanding of schizophrenia, address challenges faced by families caring for individuals with schizophrenia, identify and maximize existing resilience qualities and resources, engage social support by addressing stigma, and strengthening social support networks.
Footnotes
Acknowledgments
The authors wish to thank Mr Ryan du Toit for editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This study was approved by the Health Research Ethics Committee, Faculty of Health Sciences, North-West University, South Africa with the ethics number “NWU-00222-22-A1”.
Consent to Participate
All participants had to give voluntary written informed consent to participate.
Data Availability Statement
Data can be made available upon reasonable request from the authors.