
Abstract
Studies from the United States and United Kingdom have shown that Black patients are disproportionately diagnosed with psychosis and have received excess coercive medical intervention. There has been little discussion of this topic in Canada, and of how coercive interventions may have influenced Black patient attitudes towards mental health services. To address these issues, semi-structured interviews were administered to five Black men with first-episode psychosis (FEP) to (a) explore their experiences with coercive interventions and (b) describe how these experiences may have influenced help-seeking behaviours. Interpretative phenomenological analysis (IPA) was used to analyze the data. Four core themes and four additional themes emerged from the interviews. Patients described loneliness, not being heard, police contact and forced medication as influencing their attitudes towards mental health care. Further research is needed to develop reparative strategies to encourage reflection about and awareness of coercive intervention among Black FEP patients.
Coercive interventions in psychiatry refer to the use of force to ensure the safety of the patient and other persons (Kallert et al., 2011). Some coercive interventions include medical practices, such as physical restraints, seclusion and the use of chemical restraints, like intramuscular antipsychotic medication, when oral medications are refused by agitated patients or cannot be given when they are uncooperative (Tran et al., 2019). Other coercive practices include a legal component and may include court-ordered treatment, police detention leading to involuntary admission and confinement for psychiatric assessment (Knight et al., 2021). Although coercive interventions are a common practice in general psychiatric care of people with psychotic disorders (Lebenbaum et al., 2018), studies have clearly shown that certain groups, particularly ethnic minorities of African or Caribbean background, are at greater risk of a diagnosis of psychosis (Jarvis et al., 2011; Schwartz & Blankenship, 2014) and coercive psychiatric treatment (Anderson, 2019; Archie et al., 2010; Barnett et al., 2019). Further research is needed to explore the coercive experiences of these groups and their influence on attitudes towards mental health care.
Blackness and Psychosis
According to the American Psychiatric Association (APA, 2013), psychosis is the symptomatic presentation of one of the following five domains over a 1-month period: delusions (fixed false beliefs), hallucinations (sensory experiences without external stimuli), disorganized speech (loose associations, tangentiality, etc.), abnormal motor behaviour (such as disorganization, catatonic stupor or excitement) and negative symptoms (avolition, diminished expression, etc.). First-episode psychosis (FEP) refers to the first experience or reporting of these symptoms by an individual (APA, 2013).
The literature has shown that Black people are significantly more likely to be diagnosed with psychosis or schizophrenia (Schwartz & Blankenship, 2014) in the US from before the Civil War (see Jarvis, 2008), a finding that was perpetuated during the Civil Rights Movement, when some Black activists were misdiagnosed with schizophrenia and hospitalized against their will (Metzl, 2010). Findings in the United States and United Kingdom reported that Black youth experiencing first-episode psychosis were at greater risk for involuntary admission (Compton et al., 2006; Weich et al., 2017). Black FEP patients reported greater police involvement (Ajnakina et al., 2017), scored significantly higher on hallucinatory and hostility measures (Oluwoye et al., 2018) and were more likely to be referred by police or ambulance referral than other patient groups (Bhui et al., 2015).
While international studies found that those of African or Caribbean descent are at greater risk of police referral (Bhui et al., 2015), involuntary hospital admission (Barnett et al., 2019) and diagnosis of psychosis (Schwartz & Blankenship, 2014), little is known about whether these same findings hold true in Canada (Anderson et al., 2015; Jarvis et al., 2011), and even less about how these experiences may have influenced patient attitudes to psychiatric care. Hence, it is important to address how these issues affect the Black Canadian community in Montreal and how Black men with FEP experience coercive interventions in psychiatric care.
Being Black in the Canadian Mental Healthcare System
Studies in Canada showed that being Black was significantly associated with greater risk for a hospital diagnosis of psychosis (Jarvis et al., 2011), reported coercive intervention (Knight et al., 2021) and increased likelihood of police contact (Anderson et al., 2014). These discrepancies may be due to the excessive application of the “danger” criterion, which refers to those who are deemed a danger to themselves or others in the Mental Health Act (Large et al., 2008). Members of the Black Canadian community may be perceived as more dangerous compared to other ethno-racial groups due to harmful stereotypes linking Black men to criminality (Kleider-Offutt et al., 2017). In Canada, Black people are over-represented in the criminal justice system and frequently experience racial profiling (Maynard, 2017; Wortley & Owusu-Bempah, 2012). Black Canadian teens reported being excessively stopped by the police in Quebec (Dupuis-Déri, 2018), Toronto (Hayle et al., 2016) and Kingston, Ontario (Closs & McKenna, 2006). The intersection of age, race, gender, mental illness, and the law may place young Black men with FEP at high risk for medical and legal coercive interventions.
In a Canadian report conducted by Annoual and colleagues (2007), investigators found that Black Canadians were over-represented in involuntary services (e.g. detention centres) and under-represented in voluntary services (e.g. outpatient programs). African-Caribbean patients with psychosis have been found to undergo more police or ambulance referrals to the Emergency Department when psychotic (Jarvis et al., 2005), report more social coercion than members of other immigrant groups (Tran et al., 2019), have less general practitioner involvement (Anderson et al., 2015; Rotenberg et al., 2017) and have worse follow-up in comparison to other patient groups (Anderson, 2018; Nikolitch et al., 2018). There is still a paucity of research on coercive intervention, especially among FEP patients in the Canadian context where there has been an assumption of multiculturalism and tolerance for minorities (Anderson et al., 2014). Many Black Canadians reported feeling unheard by mental health professionals (Woodgate et al., 2017) and disliked the power dynamic between provider and patient based on histories of oppression (Jarvis, 2008; Medlock et al., 2018). Further research is needed to explore the coercive experiences of these groups in medico-legal settings and its influence on attitudes towards mental health services (Anderson, 2019; Valenti et al., 2014; Wood & Alsawy, 2016).
Theoretical Model of Coercion, Freedom and Control
Carroll (1991) described the theoretical framework for coercion and explained that a coercive situation occurs when there is reduced freedom and control with respect to treatment options for the patient. Specifically, coercion is present when an authority figure performs any of the following: (a) removes an alternative course of action, (b) makes the other courses of action unappealing, or (c) limits the ability of the individual to choose their treatment. Coercion is prevalent in FEP patients, especially when they are involuntarily brought to emergency psychiatric services because they are deemed a danger to self or others. This imposition is due to the fact that some patients with FEP may be unaware that they have any symptoms of psychosis, and they may not recognize that their behaviours and actions place themselves or others in potential danger. The acute state of the patient’s psychosis, in addition to the coercive practices to contain them, may mean that treatment options are not clearly explained such that patients are not fully aware of the choices available to them. For these reasons, patients with FEP who experience coercive intervention may become more vulnerable to ongoing coercive practices in a self-reinforcing feedback loop between the patient, psychiatry, and the courts.
The increased vulnerability to coercive practices among FEP patients overall may be even worse for Black FEP patients, because Black people as a group have a long history of being the victims of coercive policies and practices (Jarvis, 2008). Psychological reactance (Brehm, 1966) is a response to loss of freedom such that when personal freedom is threatened, people are driven to reinstate it. Steindl and Jonas (2012) found that some cultural groups experience greater psychological reactance than others based on self-perceived restrictions. Such is the case for Black FEP patients when they experience coercive interventions. Given the oppression Black communities have faced for centuries (Cartwright, 1851; Grier & Cobbs, 1968; Metzl, 2010; Washington, 2006), there may be even greater need for freedom and choice in actions concerning their well-being, particularly in psychiatric settings where mental health disparities are present and where there is a long history of systemic racism and mistrust. For these reasons, research is needed to explore the coercive intervention experiences of Black FEP patients and how these interventions may influence patient attitudes towards psychiatry and mental health services more generally (Knight et al., 2021; Valenti et al., 2014; Wood & Alsawy, 2016).
Limited Research
Most studies about involuntary admission and coercive treatment are quantitative and few studies have employed qualitative methodology to obtain a first-person account of patient experiences (Barnes et al., 2000; Gilburt et al., 2008; Priebe et al., 2009). In a systematic review, Katsakou and Priebe (2007) explored psychiatric patients’ experiences of perceived coercion from five qualitative studies. Thematic analysis of these studies showed that patients generally expressed (a) the need for autonomy and participation in treatment decisions, (b) concerns about the quality of care and (c) the impact of involuntary care on their sense of self-value. In other studies, findings regarding patient reactions to compulsory treatments are mixed (Seed et al., 2016). Some patients viewed involuntary care as a positive experience to maintain their safety and the safety of others (Holmes et al., 2004; Sibitz et al., 2011), whereas others viewed forced psychiatric treatment as a negative experience that was traumatic and dehumanizing (Olofsson & Jacobsson, 2001; Sibitz et al., 2011).
Similarly, in Canada, Ferrari and colleagues (2015) conducted a qualitative study among FEP patients and families to explore reasons for differential access to care. Findings revealed that internalized stigma, particularly among African and Caribbean FEP patients, played an important role in service utilization and that personal awareness of symptoms, family mental health literacy and general knowledge about psychiatric services influenced patient help-seeking behaviours. To date, there is limited data on the experiences of involuntarily admitted Black FEP patients in Canada.
Current Study
Using a qualitative design, the objectives of the study were to (1) explore the experiences of Black FEP men who have undergone coercive interventions and (2) describe their perceptions about the ways in which these experiences may have influenced help-seeking behaviours. Black FEP men were recruited to this study instead of Black FEP women for several reasons. First, the incidence of FEP is considerably higher in male patients aged 16–30 years than in female patients (Di Forti et al., 2015; Ochoa et al., 2012), so that more Black male patients were available for recruitment into the study. Second, studies showed that male patients are at greater risk for involuntary admission and coercive intervention than females (Hustoft et al., 2013; Umama-Agada et al., 2018). Third, we followed the common practice of using a homogenous sample (in terms of race, gender, etc.) to describe the in-depth qualitative experiences of a subgroup (Patton, 2002). For these reasons, this study recruited only Black FEP men.
The qualitative design of this study permitted an exploratory, phenomenological approach to capture the subjective experiences of Black FEP patients who had undergone coercive interventions in a Canadian health setting (in Montreal). The literature showed that Black FEP patients were more likely to experience coercive interventions (Barnett et al., 2019; Knight et al., 2021). Black patients are more likely to be diagnosed with psychosis (Schwartz & Blankenship, 2014) and brought to mental health services via police or ambulance referral (Jarvis et al., 2005; Oduola et al., 2019).
In addition to adding to the nascent Canadian literature on these topics, the current study addressed the gap in the clinical and research literature by documenting and exploring the reported coercive experiences of Black FEP patients with respect to their treatment for psychosis. There is limited research on this topic in Canada, and how coercive interventions may have influenced Black Canadian patient attitudes towards mental health services. Participant interviews shed light on the influence that coercive practices may have on help-seeking behaviours and attitudes to mental health services. Information from this study can be used in the hopes of improving treatment decisions for Black FEP patients and offering insight into the contemporary Canadian medical context.
Method
Research Design Overview
A phenomenological, qualitative, research design was used to explore the in-depth experiences of coercive interventions among Black men with FEP and to describe their perceptions about the ways in which these experiences may have influenced their personal, help-seeking behaviours. Interpretative phenomenological analysis (IPA) offers insight into how a given person, in each context, makes sense of complex and subjective phenomena (Smith & Shinebourne, 2012). This type of qualitative analysis focuses on the way individuals understand and describe their experience and allows the researcher to interpret how the individual makes sense of phenomena in a larger social context (Smith et al., 2009). Doing so is especially important for this study as it focuses on the experiences of members of the Black community who, as a group, have a documented history of problematic interactions with the healthcare system and consistent reports of unmet needs by primary care providers (Jarvis, 2008; Woodgate et al., 2017). Given that this form of analysis focuses on the personal lived experiences of participants rather than objective outcomes (Eatough & Smith, 2008), this detailed, in-depth approach was selected to identify themes related to the study objectives. Furthermore, given that IPA is ideal for small numbers of research participants (i.e. less than 10; Smith et al., 2009), it was selected to analyze the qualitative data for this study.
Recruitment Process
The first author, a Black Canadian woman, was a student and research assistant in the First Episode Psychosis Program (FEPP). She introduced the study to the FEPP clinical team. She attended weekly FEPP meetings and reminded the psychiatrists and case managers to check if they had any Black FEP patients who could be referred to the study. Patients were recruited for the study if they were (a) male, (b) English-speaking, (c) aged 18 and older at the time of referral, (d) self-identified as a Black Canadian, (e) experienced medical and/or legal coercive intervention based on their hospital chart, and (f) were still in active FEPP follow-up. Only clinically stable Black men approved by the FEPP clinician were invited to participate in the study. A patient was deemed clinically stable by the FEPP psychiatrist if (a) the patient could tolerate the interview, (b) symptoms were sufficiently under control and (c) the patient had the capacity to concentrate, be reflective and provide coherent answers. If a patient met the recruitment criteria, the case manager introduced the study to the patient. If the patient gave verbal consent to the case manager to participate in the study, the first author met with the patient after the next scheduled follow-up appointment. On the day of the interview, the case manager brought the patient to meet with the first author once the clinical appointment was finished; the research interview took place in a nearby office if the patient agreed.
Participants
Summary of Demographic Information.
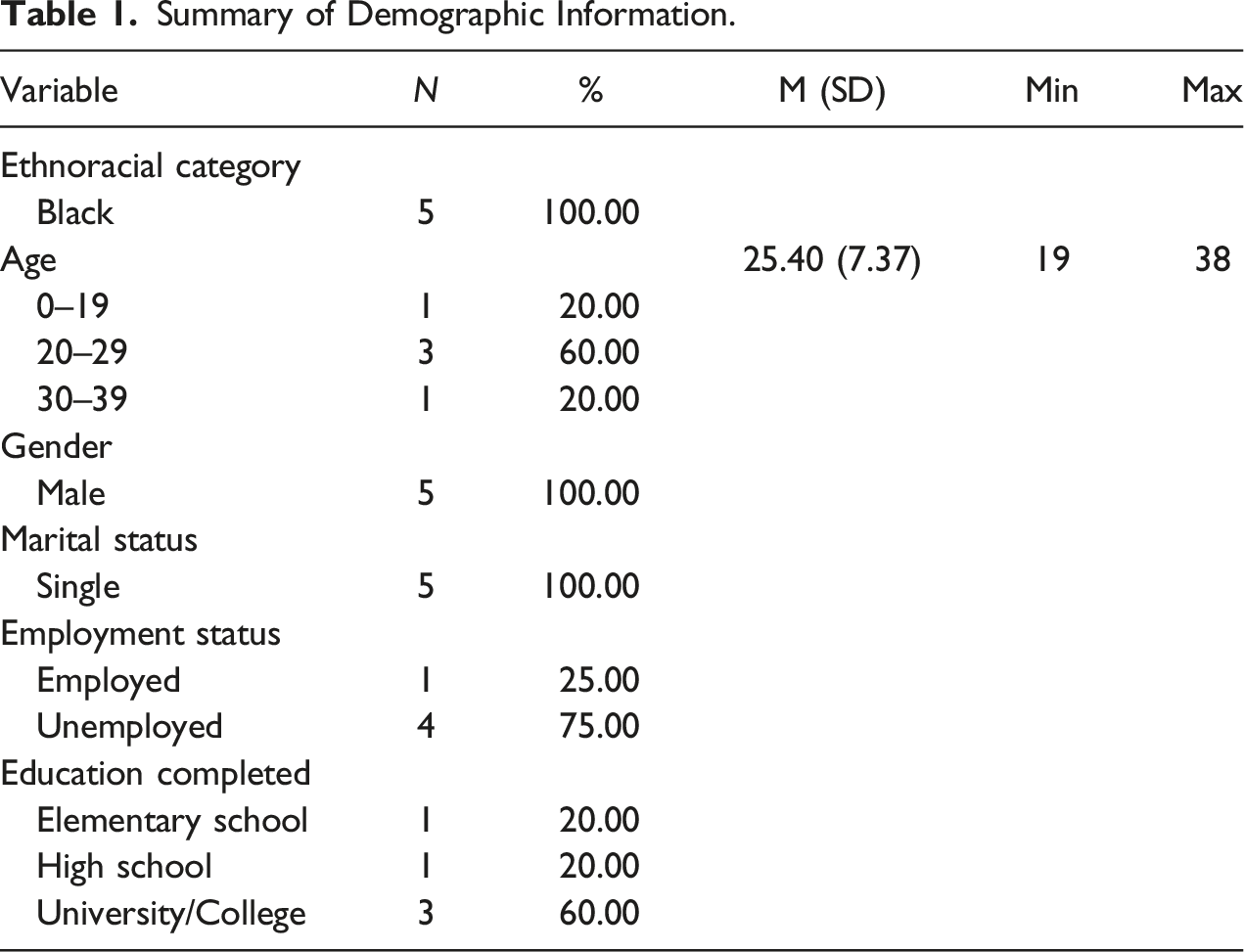
In this study, the operational definition of “Black Canadians” denotes people of African descent in Canada and are composed of the following subgroups: (1) Canadian-born descendants of Black people who came from Africa during the slave trade; (2) descendants of Black loyalists, refugees, fugitives and settlers who immigrated during the American civil war, and (3) those who immigrated from the Caribbean and Africa to Canada after World War 2 (Mensah, 2002). Participants who self-identified as a Black Canadian, in which the participant described themselves as belonging to or identifies with the Black community, participated in the study.
Initially, an approximate sample size of 10 participants was planned for this study based on the balance between (a) reaching the point of data saturation, in which no new themes or codes are developed (Vasileiou et al., 2018), (b) the relative burden of the study for a hard to reach population and (c) the feasibility given the in-depth analysis required within a phenomenological approach (Green & Thorgood, 2004; Hennink & Kaiser, 2019). This practice is consistent with the literature: Katsakou and Priebe (2007) argued, based on a review of the literature, that sample sizes ranging from five to 10 were fruitful and sufficient to address the research question at hand using a phenomenological approach. However, due to the difficulties to interview patients in-person during the COVID-19 pandemic and the obstacles associated with virtual encounters of distrustful patients, only five FEP patients were interviewed.
Measures
Socio-Demographic Questionnaire
For descriptive purposes, a socio-demographic questionnaire was given to participants to complete in pencil-paper format to obtain a description of the sample. Information was collected on participant age, gender, marital status, ethnoracial category, country of birth, education level, and employment status.
Interview Questions
A series of 17 open-ended questions was asked of each participant. Questions were based on objectives of the present study and were developed in consultation with four members of the advisory committee. Members of the committee identified as being from racialized communities and/or had expertise in working with racialized groups. Some questions were adapted from the McGill Illness Narrative Interview (Groleau et al., 2006; e.g., “What other therapy, treatment, help or care would you like to receive?”) and the Cultural Formulation Interview (Lewis-Fernandez et al., 2015; e.g., “Why do you think this is happening to you?”) to promote a person-centred approach with consideration of the interviewee’s sociocultural context. All interview questions were agreed upon by the advisory committee after discussion and reflection. The interview was structured into six main sections. The purpose of the divisions was to allow the participant to share his story in the order that the events occurred – from referral, to initial emergency room assessment, to hospital admission, and finally to discharge from the hospital to the outpatient FEPP. The first section asked questions to allow participants to initiate their narrative however they wish (e.g., How were you referred to FEPP?). The second section explored how the participant was admitted to the hospital (e.g., How did you feel about your experience coming to the hospital?). The third section elicited the perception of treatment during the hospitalization (e.g. How do you feel about the treatment suggested by your doctor?). The fourth section explored whether the participants felt that any part of their identity (race, age, gender, etc.) played a role in the medical care they received (e.g., What do you think about this statement? Based on my background or identity, my quality of care is worse). The fifth section explored participants’ attitudes towards mental health services and their influence on help-seeking behaviours (e.g., How has your past experience influenced how you obtain care?). The sixth and last section sought insight into how participants felt about their outpatient treatment and what could be improved, if anything (e.g., How has your care been so far by the FEPP team?).
Procedure
The study was conducted in compliance with the Ethics Review Board of the CIUSSS du Centre-Ouest-de-l’Île de Montréal. Interviews took place at the FEPP which is an outpatient treatment program in a Montreal hospital for patients with first-episode psychosis. The First Episode Psychosis Program has been receiving referrals since 2008. Approximately 40% of the patients are from racial and ethnic minority populations and a considerable proportion are involved in the judicial system. Of note, none of the FEPP clinicians were Black and only one was from an ethnic minority.
Interviews were conducted from January 2020 to March 2020. The first author explained the study to potential participants and obtained written consent from those who agreed to take part. Participants were informed that they had been invited to participate in the study because they were receiving care from the FEPP. Consent forms were written in plain, simple language and participants were encouraged to ask questions if anything was unclear. Participants were told that the researcher wanted to better understand their experiences in accessing mental health services and how these experiences may have influenced patient attitudes so that care could be improved, if necessary, for future FEP patients. Participants were notified that they could withdraw from the study at any time with no consequence to their current treatment.
For those who did not wish to be audio-recorded, field notes were taken. Of the five interviews, four interviews were audio-recorded and field notes were taken for one participant. Interviews were conducted one-on-one between the researcher and the participant in a private office setting and participants were advised to disclose only information they wished to share. The length of interviews varied from 40 to 60 minutes and were completed in one session. At the end of the interview, participants were compensated for their time with a $10 gift card and given the research team’s contact information.
Data Analysis
Phases of the IPA Process.
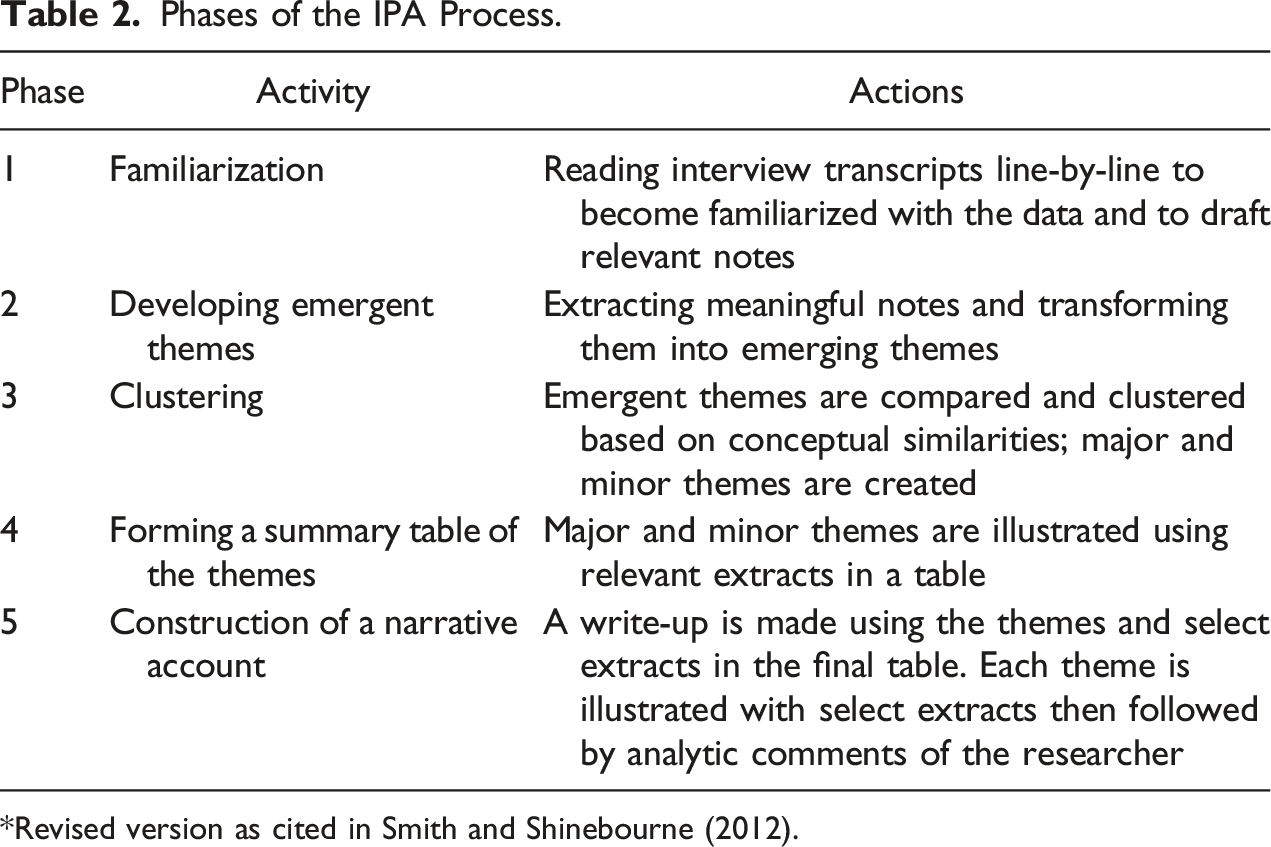
*Revised version as cited in Smith and Shinebourne (2012).
Methodological Integrity
To ensure study findings were warranted and upheld methodological integrity, several measures were taken. First, interview questions were objectively reviewed by committee members and a Research Ethics Board to reduce potential bias and capture diversity within the study sample (Meyrick, 2006). Second, the first author, to the best of her ability, tried to support the patient voice using open-ended encouragements throughout the study to establish a climate of safety around treatment narratives and limit possible bias of social desirability. The first author engaged in reflexivity by taking into consideration how her professional identity (as a research assistant and student at FEPP) and cultural identity (as a Black Canadian) could influence data collection (Dodgson, 2019). She purposefully only asked open-ended questions to not introduce bias during interviews (Reid et al., 2018). Third, themes that emerged from the interview transcripts were grounded in evidence using excerpts, so that findings were derived specifically from the participants’ experiences (Smith & Shinebourne, 2012). Fourth, member-checking was performed in which information gathered from the interviews was reviewed with participants to validate the findings and to check for accuracy (Birt et al., 2016). Similarly, the advisory committee, composed of members with expertise in working with racialized groups and/or are members of racialized communities, reviewed the identified themes to enhance credibility of the results.
Results
Summary of Themes by Participant.
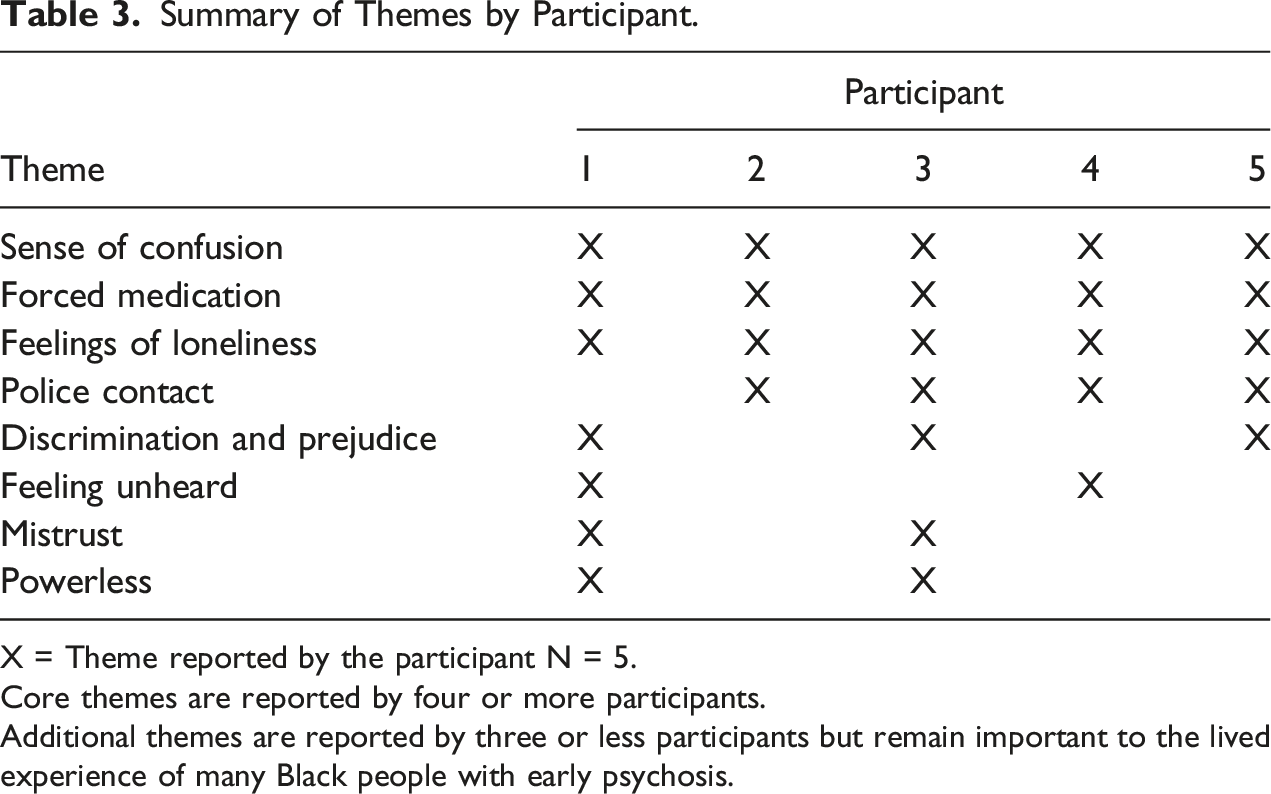
X = Theme reported by the participant N = 5.
Core themes are reported by four or more participants.
Additional themes are reported by three or less participants but remain important to the lived experience of many Black people with early psychosis.
Four Core Themes
For study objective 1, four core themes emerged from the data: sense of confusion, forced medication, feelings of loneliness and police contact.
Sense of Confusion
The first core theme to emerge from qualitative data analyses was a sense of confusion. All participants mentioned how they did not understand what was going on and wished that someone had explained things to them once they were referred to the hospital or before undergoing coercive measures. Participant 4 stated, “It was very confusing because I didn’t know what that [medication] means. Even now, I don’t know what it means.” Participants reported in their own words a sense of confusion that they associated to a variety of reasons. Participant 1 believed it was due to his lack of education, but also psychoeducation to interpret the diagnosis: “You drop out of school and end up in the hospital that’s the double wammy, you know? Cause you’re uneducated, and you’re sick, sick to the knowledge that you don’t understand.” Participant 3 associated a sense of confusion to his feeling of being exposed to contradictory statements made by the court and psychiatrist: The thing is they said I’m not guilty, but I still did the time. How am I not guilty, but I still did the time? If I’m not guilty, I’m supposed to leave the hospital as soon as I get not guilty.
Similarly, Participant 4 reported feeling confused due to the lack of communication between medical and legal authorities during the referral process. Participant 4 explained, “I spent many time travelling from place to place and I didn’t know very well what was happening, and what was going to happen.”
Other participants indicated that they did not understand their illness or the clinical procedures they underwent. Participant 5 noted being initially confused about his diagnosis: “It wasn’t until like long time after that, that I understood that there was a problem in the way I was thinking.” Participant 2 explained he was in denial about his diagnosis because he felt his symptoms were due to spiritual reasons. His cousin experienced a psychotic episode 1 week after him, so he was not sure if his psychosis was medical or if it was because some people “wished” to harm him and his family. According to him, this incident explained why the antipsychotic treatment was not helpful, even if he saw it as a “placebo” as did his African friends who were in Canada. Similarly, Participant 1 expressed additional confusion due to differences in service provision between Canada and their country of origin: “Some Black people haven’t gone to the hospital since they were in my country, then they travel here and it’s the first time they’re in the hospital, so it’s a new form of adaptation, you know?” It is not clear from this utterance if the participant thought hospitalization was warranted or not.
Forced Medication
The second core theme discovered from patient interviews was the concept of forced medication and treatment. All participants expressed initial negative attitudes towards intramuscular (IM) injections and oral antipsychotic medications. Some participants expressed the fear that the medication would change some aspects of their identity: “My fears were like it would alter the way I was thinking. It would interfere with the natural, my natural state of mind” (Participant 5). Others expressed the belief it would make them more ill: “I keep thinking that if you take too much of the meds, maybe you can get the sickness even more” (Participant 1). Similarly, Participant 3 felt he had no say or control over his body: “She put me away and made me take pills out nowhere. I never used to take pills.” Participant 4 expressed that the lack of communication with professionals contributed to the initial reluctance: It was like very confusing because at first the doctor tried to give me some medication that at first I wasn’t really into take it. So we had to go in front of the judge to take an ordinance. A prescription for treatment.
He further added, “They just told me here is the medication, you have to take it. But no one really explained it to me how it was going to affect me.” However, some participants over time reported growing comfortable with medication once it reduced their symptoms. Participant 2 expressed that he was okay with the monthly intramuscular injections but did not like the side effects of weight gain. Participant 4 stated the injections reduced his symptoms despite his initial confusion: “In the beginning, I didn’t know what it was, what it was going to do to me. Right now, I think it’s helpful because I don’t have that type of disconnection anymore.”
Feelings of Loneliness
The third core theme derived from the data was feelings of loneliness. All participants felt they were alone due to the lack of social support among family members or due to their illness making their mind “different” from others. A majority of the participants reported having an absent father figure. Participant 2, who explained that he experienced auditory hallucinations because he wanted to hear his father’s voice, considered that this directly affected him. Participant 2 expressed feelings of loneliness after his father’s passing, saying that it was hard on him. Similarly, Participant 3 mentioned the loss of his father, “After two months I did in the hospital, my dad was gone after two months.” Participant 3 expressed further feelings of isolation when he discussed moments he felt alone at school: “When I meet new people, I just don’t know how to make friends,” and at court, “I had nobody in court. My parents weren’t in court. It was only me.” Feelings of loneliness also emerged when participants discussed their experience of being diagnosed with psychosis or schizophrenia. Participant 4 explained that he felt alone in his illness because he could not talk to others about it: “I don’t understand me, myself! I don’t understand it at the level that I feel like I could talk to someone about it.” Similarly, Participant 1 expressed the experience of stigma from family members: I feel kind of like the stigma on me because I don’t want to tell too much of my family member because the closer you are to your family especially Caribbean family, and they don’t know the situation, they will not only have you, not console you, but they will just laugh sometimes...I would feel shy, and go more in the box and that’s the reason why I didn’t want to tell them.
On the other hand, Participant 5 felt his friends and family were supportive, but still felt alone in that his mind was “different.” He explains, “I feel like I’m different as my doctor put it…I have different moods than my surroundings, my friends, or my family or something. I know there’s something different, but I just try to not to think about it too much.”
Police Contact
The fourth core theme elicited from patient interviews was police contact. For 4 out of 5 participants, someone called 911, which led to a coercive referral to the hospital via police, ambulance or court-order. Participant 4 reported being hit with a police car and tasered while he was sick: The police told me to drop the knife, but I didn’t realize what was happening. The situation escalated very quickly, and I end up walking and the police just hit me with the car, and I dropped the knife at that moment, and they handcuffed me.
Participant 3 was also brought to the hospital by police officers after his high school signalled the police. Participant 3 exclaims: The school was trying to suspend me so I just okay, forget my suspension, so I just left the office, cause if I stayed, I would’ve got arrested anyways. But I felt like something was going to happen. I felt like they were going to call the police on me. It’s like I know why White people like to call the police so much. So, I just left and got home, and when I reached home my door started getting knocked down and when I looked, I saw the police.
Participants 2 and 5 recalled being brought to the hospital via ambulance. Participant 2 explained that he was standing in front of a police station when he experienced an episode and was brought to the hospital. Participant 5 explained that he was at home when 911 was called: “I was at work and on lunch time. I just went back home because I couldn’t stand it and from there I went to the ambulance. My father was there and I wasn’t acting normal so he called an ambulance.”
Four Additional Themes
For study objective 1, four additional themes that emerged in three or less of the study participants were discrimination and prejudice, feeling unheard, mistrust and feeling powerless (see Table 2 for themes).
Discrimination and Prejudice
The first additional theme was discrimination and prejudice. Some FEP patients related their experience in the hospital to the experience of African American men in jail. Participant 3 stated: I really find nothing was wrong. I feel like they were just trying to send me to the jail. If I was in the States, they’d probably send me to a jail for no reason. You know how they say school bring you to jail sometimes? If I was in the States, they’d send me to jail but I guess here, they send me to a hospital because they have nothing on me.
Participant 3 expressed throughout his interview that he felt the hospital was a “lock-up” and that his endpoint was jail: “I still feel like a jail cell. I don’t know how to explain it. It’s a hospital. If I keep switching from hospital, to hospital, to hospital, then eventually I will switch to a jail cell.” Participant 1 also echoed this sentiment when discussing his experiences growing up as a Black man: “I’ll think it’s because I’m Black but it’s not that, you know? It’s just me. It’s just me, how I grew up blackish with American state of mind, think everyone is out to get me sometimes.” He further explained his experience growing up and how stigma from others leads him to feel judged: “Not for myself, but from others. If it takes a community to grow a child, it feels like that community had the power already to judge the child before it is even born, you know?” This stigma was also expressed by Participant 3 in which he stressed during his interview that he was not being violent and that he was simply listening to music minutes before he was referred to the hospital: I didn’t even start a fight in the school. I was in no fight. I was in no argument with no teachers, I wasn’t doing none of that. I just hit the table one time, and everybody was talking. The teacher wasn’t even in class. The teacher gave us something to do, but I finished it. And I was listening to my music and I hit the table once.
According to participants, experiences with discrimination and prejudice not only emerged from interactions with authorities but also through interactions with family and friends. Participant 5 explained the challenges he faced as a bi-racial child in Montreal and feeling excluded because of it. He stated: I’m not Black, I’m not White, I’m in between the two so I was, and I didn’t really know what to say or what to do so I was, I didn’t ask myself questions but I don’t have so much problem, like it’s hard for me to find the right type of friends because some friends will, well some people won’t include me in the group so much because I’m always different. There’s not a lot of biracial people in Montreal. (Participant 5)
Feeling Unheard
The second additional theme that emerged from the data was feeling unheard. Participants expressed how they felt ignored by mental health professionals and that their mental health needs were unmet. Participant 1 explained: Most of the time you don’t get back the feedback that you, that will…I don’t know, motivate you? You just get back a blank answer …you know? And you don’t get to be heard all the time. It’s mostly by schedule if you don’t finish telling all of the story within the half an hour someone else comes in and tells their story, you know?
Participant 1 also expressed the need for a Black mental health professional to feel fully understood: I was thinking I should be sent back home when my sickness arose, when I had my first episode. I always think I should do that, that I should have a Black doctor or nurse, someone who connects with me from the island and checks and explain.”
Similarly, Participant 4 expressed the need for someone to address his needs and listen to his medication inquiries prior to treatment: “Maybe if they explain to me what was going on and what was going to happen because at the beginning when the doctor just said me, here is the medication they didn’t explain to me why I have to take the medication.”
Mistrust
The third additional theme elicited from the transcripts was mistrust, specifically towards mental health professionals. Some FEP patients reported a sense of mistrust regarding their psychiatric care: “I don’t know, at the core of everything, I really don’t trust being in a hospital. Because of the forced treatment, and all these things, being poked with needles and still going on, it just feels like an invasion sometimes” (Participant 1). Participant 1 shared that he initially opened up and explained himself to the emergency room physician but felt the physician betrayed him by forcing him to stay in the hospital: “It depended on that explanation. I didn’t know that. I just thought I had to explain myself to the doctor and that was the deciding doctor that would seal my fate, you know? I didn’t know that.” Even when the clinical team was supportive at times, he still felt the need to “police his mind” because trust was not established: “I’m here sick and so much people are taking care of me but none of my family, and it’s not a family member you’re sitting down to and talking to, so anytime you’re feeling stuff about the family, just it feels like an invasion” (Participant 1). Additionally, when Participant 1 was diagnosed, he felt that the providers were trying to control him: “They say I’m schizoaffective and I’m not too sure what that means…I’m kind of like ‘woah, woah, stay back, this is my mind’, you know?” Participant 3 also expressed feelings of mistrust not only towards mental health providers but even towards his family: “That’s my mom, that’s the police. That’s why I don’t trust her too much. To me, she’s the police.”
Powerlessness
The last additional theme that emerged from the qualitative data was feelings of powerlessness. FEP patients reported a sense of powerlessness with respect to the coercive dimension of their psychiatric treatment. Participant 3 reported feeling stuck and unable to escape given that his treatment at the FEPP is under the jurisdiction of the court: “I cannot escape it. I cannot escape the government…I don’t have a choice. The only thing I can do is just survive though.” Similarly, Participant 1 reported feelings of powerlessness as a sick patient, “I feel like I’m weak because I’m in the hospital and it beats your judgement sometimes.” He also felt powerless as a man by not managing the household: “I was partly responsible for it because I was the man of the house and nothing was going good.”
Help-Seeking Behaviours
To address study objective 2, participants described their subjective perceptions about how these coercive experiences may have influenced their personal help-seeking behaviours. Responses varied among the 5 participants. Participant 1, who experienced 7 years of psychiatric treatment, stated, “I don’t think it will change too much. I feel like it could, but I would just be putting myself out there for some crazy stuff.” Participant 1 expressed how he had no social support, and it was hard to come to appointments: “It feels like I have no one there to come with me to the appointments and it just feels like I’m alone.” Furthermore, feeling unheard and unseen in medical settings contributed to sombre attitudes towards treatment: “Well coming from my standpoint that I’m Black, and it’s like I wanted to be heard more a little bit” (Participant 1). Similarly, Participant 3, who was referred to FEPP 2 years ago, responded: “It’s scary. If I came here some other time bro, I wouldn’t. If they keep me here for another time, they better have some weed for me because I wouldn’t even stay.” When Participant 3 was asked what part of his experience could be associated with his position, he further explained that he disliked the police contact: “There’s nothing that can change it unless they stop. The police stop harassing me and stop coming and picking me up and just dropping me to the hospital that would be good.”
Participants 2, 4 and 5 were more open to receiving further mental health services. Participant 2, who was diagnosed with schizophrenia 3 years ago, expressed initial hesitancy due to his first negative experience with medication side effects. However, Participant 2 felt cared for by the FEPP team and found the doctors helpful. Participant 4, who was recently referred in the last year, simply stated he was open to mental health services. In the beginning, Participant 4 mentioned that he did not understand what was going on leading to great confusion, but after the medication reduced his symptoms, he started feeling better, so he became more open to receiving other services available. Likewise, Participant 5 responded, “I’d be willing to see what services and if it works better than what I have so far, it would be good.” Like Participants 2 and 4, Participant 5 felt confused at first but reported that his perception of FEPP services changed after the medication improved his condition and the FEPP team addressed his concerns.
Discussion
The purpose of this study was to (a) explore the experiences of Black FEP men who underwent coercive interventions and (b) describe how these experiences may have influenced help-seeking behaviours. Semi-structured patient interviews were analyzed using IPA. Four core themes (sense of confusion, feelings of loneliness, forced medication and police contact) and four additional themes (discrimination and prejudice, feeling unheard, mistrust and powerlessness) emerged from the qualitative interviews. Participant responses varied on their attitudes towards mental health care after experiencing coercive treatment. Some participants were open to receive further mental health services after having experienced a coercive intervention, whereas others were not. Patients reported that themes of loneliness, not being heard, police contact and forced medication influenced their attitudes towards mental health care.
Study findings support the theoretical framework of coercion by Carroll (1991) in which coercion is present when FEP patients have limited opportunities to participate in their treatment as they are involuntarily admitted and are deemed unable to make sane decisions. Thus, patients with FEP who experience coercive treatment are more vulnerable to coercive interventions. This finding can be reflected in coercive situations with Black FEP patients. Prior Canadian studies have shown that Black FEP patients are at greater risk for diagnosis of psychosis (Anderson, 2019), coercive referral (Jarvis et al., 2005) and coercive treatment (Jarvis et al., 2011). Based on the theory of psychological reactance by Brehm (1966), which describes the response to reduction in freedom, reported themes of mistrust demonstrate that Black FEP patients have a greater need for freedom and choice in actions concerning their well-being, especially in psychiatric settings where health disparities are prevalent for these groups.
The first core theme was a sense of confusion. Participants described how inadequate communication by healthcare providers, different explanatory models of illness and poor understanding of mental health services as newcomers to Canada all contributed to a sense of confusion. Poor medical communication, cultural insensitivity, lack of trust, and use of coercion are known barriers to therapeutic relationships and lead to poor patient attitudes to care (Gilburt et al., 2008). These findings suggest the need for improved medical communication in clinical encounters between practitioners and patients. This recommendation would usually take the form of longer appointment duration, especially in the initial evaluation and subsequent appointments. Other interventions could include family psychoeducation seminars and invitations to family members of patients to follow up appointments with case managers and psychiatrists. Ample time must be given to answer questions, negotiate treatment and resolve diagnostic concerns.
The second core theme that emerged was feelings of loneliness. All participants expressed feeling alone due to lack of social support from relatives or due to their diagnosis making them feel “different” and isolated from others. These findings are consistent with a previously reported link between loneliness and psychosis (Michalska da Rocha et al., 2018). Some of the participants mentioned having an absent father figure. This information is consistent with the literature showing that Black men are often raised in homes without fathers (Cartwright & Henriksen, 2012), resulting in feelings of loneliness and abandonment (Earl & Lohmann, 1978). These findings suggest that strong social networks are important, and interventions to increase family involvement could prevent treatment discontinuation and reduce feelings of loneliness in patients with psychosis (Taylor et al., 2017). Referral to Black community programs and standard interventions like school classes, employment training, and group therapies and activities could go a long way towards mitigating these concerns, especially in the context of ample family support. Most importantly for young Black men with FEP, intervention programs that reach out to fathers to specifically encourage their involvement in their sons’ prescribed activities will likely be of most benefit.
The third core theme was forced medication. All of the participants expressed initial fears and negative attitudes towards their prescribed medications. Some participants feared the side effects of their oral antipsychotic pills, and some felt that the injections were too invasive, whereas others felt that the clinicians did not provide enough explanation regarding how the medication would work or why it needed to be taken. These findings are consistent with the current literature (Demjaha et al., 2017). Hickling and colleagues (2018) found that patients were more likely to adhere to antipsychotic medications if they were satisfied with the medical information provided by practitioners. Some authors have attributed the unwillingness of Black patients to take medication to general mistrust of medicine due to past experimentation on African Americans (Chaitoff et al., 2014; Jarvis, 2012). These findings suggest the need for physicians to be aware of the historical and cultural factors that impact the Black community and that may undermine medication adherence. In addition, these findings highlight the need for clinicians to be more transparent with patients and provide better information about antipsychotics to facilitate recovery. It may be good practice to spend extra time with Black patients and their families to discuss medication and to be patient with the kinds of questions that may be asked. Although time intensive, such interventions are likely to improve the therapeutic relationship, understanding of psychosis and its treatments, and overall outcome.
The last core theme that was elicited from the data was police contact. As shown in the literature, Black patients are more likely to be referred to emergency services by the police than are patients from other ethnic groups (Anderson et al., 2014; Archie et al., 2010), and this pattern was evident in the present study as well. All participants reported experiences with the police in which some were handcuffed, tasered, hit with a police car, or brought to the hospital via ambulance after 911 was contacted. However, these are not isolated events. In April 2020, a 26-year-old Black man diagnosed with schizophrenia was shot to death in Brampton, Ontario, after he called 911 for help (Nassar, 2020). In August 2018, a 23-year-old Black man with ongoing mental health issues was fatally shot by police in the city of Montreal (CTV Montreal, 2018). Similarly, in Montreal, Quebec, a 58-year-old Black man with a history of mental illness was shot outside his apartment after police arrived (Shingler, 2019). These tragic examples, among others, suggest that there may be enduring stereotypes or racial bias in which Black people, particularly Black men, are deemed more dangerous than members of other ethnioracial groups (Metzl, 2010; Kleider-Offutt et al., 2017; Oliver & Fonash, 2002). Those who are diagnosed with severe mental illness are often seen as a public threat (Corrigan & Watson, 2005); thus, the intersection of race, gender and mental illness may place Black FEP men at greater risk for coercive measures. Training in basic mental health principles is needed for police officers to learn how to better handle patients during a psychotic episode. Also, officials must assess their own potential bias to prevent further stereotyping of racial minorities, and research should contribute to learning how racial stereotypes continue to inform public opinion. Community outreach and education efforts with Black communities, and enlisting the participation of Black community partners, could sensitize families of youth to the symptoms of psychosis. This approach might encourage early referral to psychiatric services via family doctors rather than allowing symptoms to escalate until police and ambulance intervention are necessary.
Along with the core themes, four additional themes emerged from data analyses. The first additional theme was discrimination and prejudice. After conducting the participant interviews, it was evident that contemporary issues affecting the Black community, such as racial profiling (Closs & McKenna, 2006), over-representation in jails (Wortley & Owusu-Bempah, 2012), and police brutality (Taylor, 2016), influenced the attitudes of young Black FEP men. Racial socialization refers to a process in which shared beliefs about race and racism are taught and transmitted by family, communities, and society-at-large to youth (Boykin & Toms, 1985; Thomas & Speight, 1999). Racial socialization patterns regarding Black Canadian men were evident as some participants expressed how they expected to be sent to jail and that the hospital was a form of unlawful confinement. Participants also mentioned the prejudice they experienced growing up as a Black person and how they constantly felt judged, excluded, and targeted by others. These feelings expressed by participants are also mentioned in the literature, in which Black men reported, feeling targeted not only by police (Taylor, 2016), but also schools (Ellis et al., 2018; Nasir et al., 2017), media (Dukes & Gaither, 2017), sports (Comeaux, 2018), and the workplace (Bell, 2017). Thus, mental health professionals must be sensitized to these matters and future research urgently needs to explore the impact of racial discrimination on the mental health status of Black people and other ethnic minorities. The priority of any clinical intervention is to make a culturally safe space for the work to unfold. Topics of concern, such as racism and discrimination, need to be given priority when patients are ready to discuss them in a culturally safe and appropriate manner (Williams, 1999).
The second additional theme that emerged from patient interviews was feeling unheard. This theme is commonly reported by Black patients in the literature, who often expressed unmet mental health needs and the feeling of being ignored, unheard, and unseen in healthcare settings (Brown, 2016; Woodgate et al., 2017). In this study, Black FEP men wished to be heard but felt dismissed when their medical concerns were not addressed. One participant even expressed the need to be legally represented in order to have his voice fully heard. He also requested the presence of a Black mental health professional as he felt they would be more attentive. The preference for racial concordance was also shown in a study conducted by Chaitoff and colleagues (2014), who found that Black participants preferred health institutions with diverse staff, but particularly Black healthcare workers. These findings suggested that it is important for mental health professionals to recognize the challenges that ethnic minorities experience in clinical settings and to actively promote patient welfare, and patient engagement, in all medical matters. It also points to an urgent need for universities to train more students from diverse backgrounds and for hospitals and other health institutions to hire qualified Black candidates to clinical and administrative positions. In some settings ethnoracial matching of patients and clinicians will not be possible, especially when services are highly specialized with limited numbers of trained staff. In these situations, clinicians need to be aware of how to work with diverse patients and to openly discuss what the patient’s preference would be – the gender and ethnicity of the ideal clinician – and how not having access to their preference will affect the treatment. Such a discussion gives permission to raise problems of communication and increases the likelihood that a patient will feel respected and heard in the clinical interaction.
The third additional theme was mistrust. A few participants expressed mistrust towards mental health professionals as a result of practitioners dismissing their concerns, being referred to the hospital via police contact and being forced to take medication they initially refused. Negative attitudes towards medication have also been shown in the literature about Black patients, in which they are reluctant to participate in healthcare services due to the belief that experiments like those at Tuskegee (Washington, 2006) could happen again, that misdiagnosis and clinician bias will prevail in clinical interactions, and due to their own personal misgivings as a result of cultural mistrust (Chaitoff et al., 2014; Hankerson et al., 2015).
Cultural mistrust refers to the belief held by some African Americans that White people cannot be trusted due to daily occurrences of racism, such as microaggressions, or the results of centuries of mistreatment ensuing from slavery (Terrell et al., 1981). For example, during the COVID-19 pandemic, the history of harmful experiments led by medical institutions in Black communities seemed to have an impact on vaccination hesitancy (Bajaj & Stanford, 2021). Cultural mistrust is an understandable response by Black people to a long history of pervasive racial discrimination in US society (Terrell et al., 2009). While it may be protective in some situations, cultural mistrust has negative consequences, such as complicating the diagnosis of psychosis when clinicians may mistake legitimate mistrust for psychotic paranoia (Whaley, 2001). It may be difficult in some cases to differentiate between cultural mistrust and paranoid mistrust among Black patients with FEP – in fact, the two may coexist (Terrell et al., 2009; Whaley, 2001). This is evident in how participants expressed mistrust not only towards medical staff but also family.
In addition to being over diagnosed with psychosis (Schwartz & Blankenship, 2014), cultural mistrust may predispose Black patients to be involuntarily admitted to the hospital (Oduola et al., 2019) and referred to psychiatric services via police (Anderson et al., 2015; Bhui et al., 2015) due to delayed help-seeking until symptoms are severe. As in the US, anti-Black racism is systemic in Canada (Maynard, 2017), which may contribute to Black people being less trusting of White clinicians (Mensah, 2002; Woodgate et al., 2017). These findings suggest that mental health professionals must work to acknowledge that mistrust is legitimate and reflect collective experiences of abuse. It is a delicate task to address these disparities in mental health frameworks, and it requires professionals to establish safe rapport with the families of patients, and the wider Black community, to unweave the mistrust that has developed over centuries.
Suggestions for increasing trust in Black patients may include having cultural brokers present in evaluations and follow-up meetings, increasing family involvement, encouraging cultural sensitivity in clinical practice, openly acknowledging racial differences and making an effort to ensure that Black patients feel heard and seen in clinical sessions (Medlock et al., 2018; Whaley, 2001). The participants of this study advocated for this as well: “I should have a Black doctor or nurse, someone who connects with me from the [Caribbean] island and checks and explains” (Participant 1).
The last additional theme was powerlessness. Some participants expressed a sense of powerlessness as a result of their coercive experiences or due to being unable to fulfil personal obligations because they were sick in the hospital. These feelings of powerlessness were also mentioned in the medical literature about the dynamics of clinical interactions. Patients felt the most powerless when they were approached by clinical staff uniquely as a sick patient such that their subjective lifeworld was ignored or neglected (Verbeke et al., 2019). These findings suggest the need to promote patient autonomy in clinical settings to enhance the therapeutic alliance and improve attitudes towards psychiatric care. Clinicians need to take the time to listen to their patients, especially those from backgrounds with histories of discrimination and marginalization, given that the care setting may act as a traumatic reminder of previous adversity.
Qualitative data were also collected to determine the influence of coercion, when it occurred, on help-seeking behaviours. Of the eight identified themes, four played a greater role in influencing patients’ attitudes to care and help-seeking behaviours: loneliness, feeling unheard, police contact and forced medication. Participants 1 and 3 were less open to mental health services and associated this with lack of social support, feeling unheard in clinical settings and the initial contact with emergency psychiatric services via police referral. In contrast, Participants 2, 4 and 5 were more open to mental health services after the medication reduced their psychotic symptoms, despite their initial reluctance to accept their prescription. These findings are consistent with past literature in which Black Canadian patients reported feeling unheard in medical settings (Woodgate et al., 2017), and FEP patients reported that lack of knowledge about psychiatric services negatively influenced help-seeking behaviours (Ferrari et al., 2015).
The difference between participants and their attitudes towards treatment may involve social support and education. Participants 1 and 3 had little to no family support throughout the course of treatment, so they found participating in mental health programs difficult because they had no one to support their progress. Participants 2, 4 and 5 had more social support, potentially making it easier to benefit from hospitalization or adhere to court-ordered treatment.
Another difference between the patients was education. Participants 1 and 3 dropped out of high school, whereas Participants 2, 4 and 5 were enrolled in university or college studies. It is possible that those with higher education may have been exposed to material in their studies that may have helped them process information they received concerning their illness, improving attitudes to treatment and services. Education may also have equipped these participants to better understand the language of psychiatry and issues regarding mental health and recovery. In a Canadian study, Ferrari and colleagues (2015) found that as patient awareness of symptoms and general knowledge of mental health services increased, so did help-seeking behaviours among African and Caribbean origin groups with psychosis. The current study findings suggest an urgent need to take the time to teach Black FEP patients and their families about psychosis diagnoses, symptoms, treatments and outcomes.
Research and Practice Implications
Results from this study contribute to the clinical literature, especially in the Canadian context, and highlight the importance of research on healthcare disparities to address the challenges lived by members of ethnoracial minorities. To date, there are limited data on the experiences of involuntarily admitted patients and patients that are coercively treated by the mental health system, in general, and specifically among the Black FEP population in Canada. This study provides preliminary data on these issues. The results of this study can also be used to improve clinical interventions and triage procedures so that patients can participate more fully in treatment decisions. Professionals need to be trained to ensure that their patients are culturally safe, which includes an awareness of the privileges of the clinician and of the legitimacy of cultural mistrust. This study also calls for clinicians to become aware of common stereotypes of Black male patients under the age of 30 who have been perceived by clinicians to be more threatening, incoherent and disturbed, requiring coercive measures to contain extreme behaviours (Pipe et al., 1991). The results of this study may inform policymakers on how to promote patient welfare and autonomy in future hospital policies and mental healthcare programs. Further study will determine how decisions are made and which implicit racial stereotypes are contributing to excess coercive measures in Black people. Beyond the world of psychiatry, the study also points to the urgent need to train police officers, lawyers and judges as they make key decisions regarding the implementation of coercive measures in patients with mental health problems.
Limitations
Only five Black FEP patients were interviewed for the study. The small sample size was due to the outbreak of COVID-19, which abruptly halted study recruitment midway through the process. A larger sample size would have offered more insight into the marginalized and stigmatized experiences of Black FEP patients who undergo coercive interventions. This study nonetheless provided descriptive information on the experiences of coercion in Black FEP men and the implications of these experiences on help-seeking behaviours. In any case, the small sample size was acceptable, given the qualitative methodology. The qualitative sample was also limited to the experiences of young, Black, English-speaking men in Montreal, who were diagnosed with early psychosis. In addition, the experiences of FEP patients were limited to the interview questions. The findings cannot be generalized to other sites or settings. The use of field notes did not contain the same level of detail as audio recordings, so data analyses may have been impacted. While the researchers acknowledged and, as much as possible, set aside their own beliefs throughout the study, it is possible that some implicit bias was present. To minimize this, semi-structured interview questions were reviewed by the Research Ethics Board to maintain objectivity and ensure that questions were not ambiguous or leading. Despite these limitations, this study contributes to the literature on FEP patients and coercion in Canada, which has been limited.
Future directions
Future research could use data triangulation (Jentoft & Olsen, 2019), in which data are gathered from multiple sources, such as mental health practitioners, families and patients, to explore the topic of coercion. Research could carefully evaluate intervention strategies to encourage family involvement with young Black FEP patients and to assess the influence of family involvement, on mental health outcomes. Information could also be collected on police attitudes towards urgent referrals to emergency services to detail the encounters that patients experience prior to coming to the hospital. Given that many FEP patients are involved with the judicial system, future research should also investigate the court process and how it determines outcomes for young Black men with psychosis. Studies will need to focus on psychiatry, the police and the law to unravel the web of interactions that lead to the use of excess coercion in young Black men with psychosis.
Conclusion
Past studies have shown that there is differential treatment in psychiatric care across ethnoracial groups. The scientific literature shows that Black patients are disproportionately referred via police to mental health services (Bhui et al., 2015; Oduola et al., 2019). There is limited research on this topic in Canada. This study addressed this gap in the clinical and research literature by qualitatively exploring the lived experience of coercive interventions in a treated sample of Black FEP men. Results showed that themes of loneliness, feeling unheard, police contact and forced medication negatively influenced Black FEP patient attitudes towards mental health services. More research is needed to document and contextualize the role of ethnoracial status in coercive mental health care of early psychosis and to outline reparative strategies for members of Black communities.
Footnotes
Acknowledgement
We thank the FEPP clinical team and patients for partaking in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the First Episode Psychosis Program (FEPP), Institute of Community and Family Psychiatry, Jewish General Hospital.