
Abstract
This study examines vaccine allocation policy during the COVID-19 pandemic by applying a hierarchical, a negotiation, and a cultural perspective. It addresses how vaccine allocation principles under conditions of scarcity are translated into practice in the case of Norway. A main finding is that the policy was informed by instrumentalism as well as by path dependencies, but over time the issue became more salient by activating stakeholder interests, which resulted in an adaptation of established norms. The three perspectives reveal how different approaches to a “fair vaccine allocation” policy can lead to different explanations of the same phenomenon.
Introduction
This paper analyzes the vaccine allocation process under conditions of scarcity during the COVID-19 pandemic by applying three theoretical lenses (cf. Allison, 1971). Allison used three alternative and supplementary conceptual frames of reference to analyze the decision-making process around the Cuban missile crisis. The article begins with a hierarchical-instrumental perspective (cf. Allison’s Rational Actor model), examining whether the decision-making process was characterized by hierarchical control, and analyzes how clearly the goals, problems, and solutions were defined and coupled (Christensen et al., 2020). A negotiation perspective (cf. Allisons Governmental Politics model) sees vaccination policy as informed by actors with differing interests and by power struggles and coalition-building (March & Olsen, 1983). Our third perspective deviates from Allison’s models and instead applies a cultural perspective, whereby vaccination policy is informed by existing norms and values, path dependencies, and a logic of appropriateness (March & Olsen, 1989; Selznick, 1957).
In addition to all the regulatory measures adopted to combat the COVID-19 pandemic, vaccines were seen worldwide as the best way to prevent severe illness and to stop the virus spreading (Ansell et al., 2021). The roll-out of vaccination programs became a subject of major political debate in many countries (Boin et al., 2021). When supplies are limited, deciding which groups should have priority access to the vaccine becomes a pressing issue and a challenge for policymakers (Duch et al., 2021; Persad et al., 2021). It was therefore important that the reasoning underlying the decision-making process on vaccine distribution was sound, particularly in the initial phases when vaccine availability was limited (Bubar et al., 2021). Analogous to their handling of the pandemic, different countries used different combinations of a set of common principles to allocate vaccines and succeeded in speeding up the vaccination process in a variety of ways (Chapman et al., 2022; Yang et al., 2021).
Vaccine allocation is a political, administrative, scientific, and ethical process, and it is also a volatile one. Politically, the allocation and re-allocation of vaccines was a highly sensitive issue that reflected ambiguity and various trade-offs, not to mention the political aspects of gaining access to vaccines (Ferranna et al., 2021). Administratively, it was about the capacity of the government to organize the provision and administering of vaccines (Christensen et al., 2016). For scientists, vaccine allocation is complex, both because it involves balancing the different strategies and criteria underlying the vaccine programs and because of uncertainties regarding means-end relations, leading to tensions and disagreements among experts (Baekkeskov, 2016). Ethically it is challenging, since vaccine programs often need to balance different ethical allocation principles (Bell et al., 2020). But the process is also volatile, given the constantly shifting parameters of the pandemic and the resulting changes in needs and hence in vaccine allocation.
Most studies of vaccine programs are dominated by medical researchers and epidemiologists searching for optimal solutions (Liu et al., 2020). Some of the studies also take into account ethical or sociological factors, such as how vaccine programs are biased according to socio-economic or ethnic background or how the allocation to developing countries is disproportionate (Ezekiel et al., 2020; Holzer et al., 2021). Others address vaccine uptake (Wynen et al., 2022). A deficit in the literature about vaccination programs is how the vaccine allocation policy in a situation of scarce supply is informed not only by hierarchical instrumental features but also by negotiations and cultural factors. This study aims to address this gap in the literature by addressing the complexity and hybridity of decision-making in public sector organizations (Christensen et al., 2020).
The focus in this article is on the allocation of vaccines in Norway from November 2020 through September 2021. We used public documents, such as public reports, to describe the main principles of healthcare provision, as published by the Ministry of Health. Actual provision of healthcare and the criteria underlying it are outlined in reports from the National Institute of Public Health and can also be gleaned from media coverage. The decision-making process was well covered in the media and in public documents.
Theoretical Basis: Hierarchy, Negotiations, and Culture
To understand the vaccination policy process, we will apply a hierarchical-instrumental perspective supplemented by a negotiating and a cultural perspective (Christensen et al., 2020; Christensen & Lægreid, 2022; March, 1994).
A hierarchically based instrumental perspective would expect hierarchically responsible leaders to implement vaccine policy in an instrumentally rational way. It would also expect objectives and measures to be formulated through a top-down process and leaders to organize the process on the basis of unambiguous means-ends considerations based on professional expert advice (cf. Christensen et al., 2020). There is supposed to be a close connection between objectives, measurable targets, input, activities, output, and outcome. The process is informed by deliberate instrumental-structural design by leaders to bring about change (Egeberg, 2012) and policy development will be informed by experts.
The hierarchical-instrumental perspective is used to understand the rational calculation of central political and administrative actors as well as to analyze the organization of the process and the actor and influence pattern (Christensen et al., 2020; Egeberg & Trondal, 2018). The focus is on how these actors defined the problems and came up with solutions for vaccine allocation. A bounded rationality approach (March & Simon, 1958) assumes that the actions of decision-makers are informed by the logic of consequentiality (March & Olsen, 1989), but at the same time constrained by the complexity of the situation, the lack of complete information, and decision-making routines. For these reasons, actors will tend to make decisions that are regarded as satisfactory rather than completely rational.
According to this perspective, the formal structure around the vaccination process is assumed to be important, meaning both how the relationship between political executives and expert bodies is structured and how the process of vaccine allocation is organized and what rules are applied and how. Seen from this perspective, one might expect vaccine policy to be based on analytical planning, the growing role of science in policy, and the drive for global, evidence-based policymaking (cf. Drori & Meyer, 2006). Vaccine allocation would be decided by the top leadership, with either politicians or experts scoring relatively high on means-end knowledge, consistency, and unambiguous criteria. One would accordingly expect a tight linkage between overall goals, options, and consequences.
Viewed from a negotiation-based instrumental perspective, deficiencies in developing and implementing vaccination policy may occur owing to resistance to leaders’ vaccination policy from actors inside or outside the government organization who have different interests and different perceptions of problems and solutions. There might be interest articulations, power struggles, winning coalitions or compromises alluding to what March and Olsen (1983) label Realpolitik and to the government politics model of Allison (1971). Various actors have different vested interests and may act strategically to influence how vaccination policy works in practice. The actual vaccination policy may therefore create tensions, conflicts, and compromises, and the winning coalitions might change over time. According to this perspective, the government is not a group of unified actors but a collection of heterogenous organizations operating as coalitions in which each actor acts in an instrumentally rational way informed by his or her interests and enters into coalitions with external actors with similar interests (Christensen et al., 2020). Thus, the expectation is that different ministries and central agencies might defend various special interests in vaccination policy.
Seen from this perspective, political rationality is less about means-end knowledge than about the quest for collective agreement on political and policy action. It is the art of coalition—building and not scientifically generated, conclusive knowledge about one best way of achieving a particular end (Donadelli & Gregory, 2022). In contrast to the hierarchical-instrumental perspective, it is less about centralized information-based decision-making and more about negotiation and bargaining among groups promoting and protecting different interests and values (Gregory, 1997; March & Olsen, 1983).
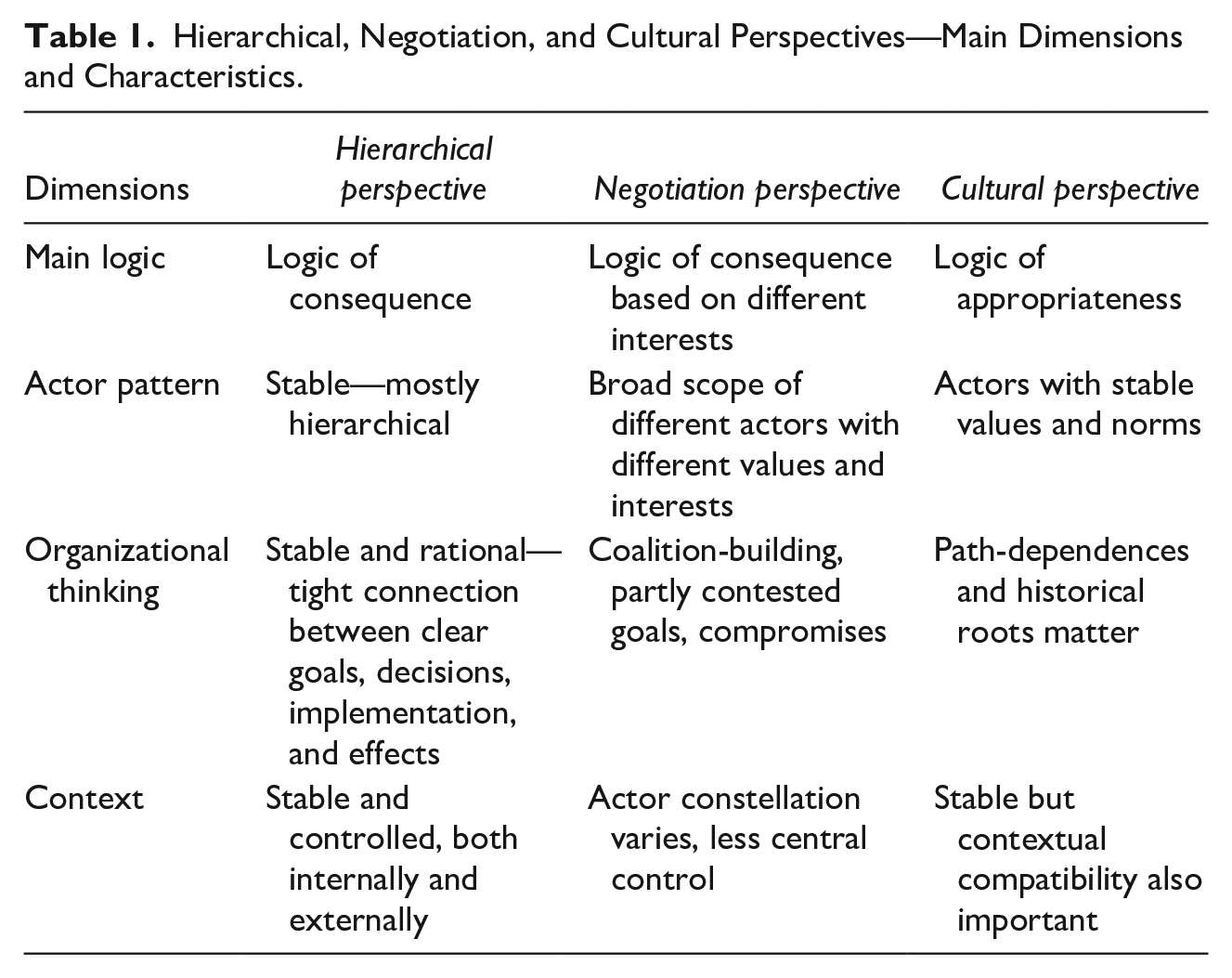
From a cultural perspective on political-administrative relations, it will be important to clarify how an organization’s established cultural features will influence the course and outcome of the vaccination policy processes (Selznick, 1957). Informal norms and values and the appropriate organizational solutions will be relatively stable over time. Rather than a logic of consequentiality, a logic of appropriateness will inform how vaccination policy is developed and implemented and there will path dependencies as well as a compatibility test of the policy (Christensen & Lægreid, 2021; March & Olsen, 1989). The vaccination policy might run into trouble if it deviates too much from existing traditions, procedures, and processes. There might be a layering process in which the vaccine policy as well as its implementation are edited and supplement existing arrangements owing to internal as well as external pressure rather than replacing them, resulting in hybrid solutions (Mahoney & Thelen, 2010).
Table 1 sums up some of the main dimensions and characteristics based on the two perspectives.
Hierarchical, Negotiation, and Cultural Perspectives—Main Dimensions and Characteristics.
Context
Until October 2021, Norway had a minority center-right coalition government. As the largest coalition partner, the Conservative Party was allocated the offices of Prime Minister and the Ministry of Health and Care Services (MHC), which were the two main political actors involved in the management of the COVID-19 pandemic (Christensen & Lægreid, 2021). The Norwegian Directorate of Health (NDH) and the Norwegian Institute of Public Health (NIPH) are subordinate central agencies under the MHC and were the main administrative and expert bodies dealing with the pandemic.
Norway received vaccines through agreements with the EU. The Pfizer/BioNTech vaccine was approved for use on December 21, 2020, and the Moderna vaccine on January 6, 2021. The first citizen was vaccinated on December 28, 2020, followed by vaccination of the oldest and most vulnerable citizens, but mass vaccination did not start until May 2021. The political executives said early in the process that they had put the NIPH in charge of the vaccination program because of its expertise.
The vaccination program had to be adjusted several times owing to new developments in the pandemic, changes in allocation principles, delays in deliveries of vaccines, and restrictions on approved vaccine suppliers (NIPH, 2020, 2021). Overall, vaccines were scarce until August 2021. Patients in nursing homes were vaccinated by mid-February and all over 85-year-olds by mid-March. By October 9, 78% of Norwegian citizens had received one vaccine dose and 68% were fully vaccinated, which was above the European average. In Norway, vaccination is voluntary and free, trust in the health authorities is high, and vaccine hesitancy and resistance are low. By the end of November 2021, 92% of all citizens over 18 years had been vaccinated with one dose and 88% were fully vaccinated
Vaccine Allocation Principles
According to the WHO (2020a, 2020b), vaccines should be equitably and justly distributed, targeting individuals at highest risk of serious disease or death (see also DeRoo et al., 2020). As effective vaccines became available for COVID-19, demand was shown to outstrip supply, making it urgent to develop a strategy to prioritize their use to ensure maximum public health and societal benefits. The recommendation followed all over the world was that people over 65 years, those in shielded groups, and healthcare workers should be given priority (Hassan-Smith et al., 2020).
In Norway, the NIPH established its own external expert ethics group to decide priority based on these principles. The group’s report (NIPH, 2020) stated that decisions on priority should be influenced by the following factors: the societal groups for whom the vaccines had been approved; the effectiveness of the vaccine; the safety of the vaccine for different age groups; the ability of the vaccine to prevent infection and transmission; the level of risk of severe disease and death in the various groups; the occupational infection risk; the epidemiological and clinical characteristics of COVID-19; and the development of the pandemic. The report also pointed out that the availability of different types of vaccines at various points in time was important, underlining that the development of the pandemic might make it necessary to adjust the priorities.
The report proposed five main goals as a framework for the vaccination program, ranked in the following order: reduce the risk of death, reduce the risk of serious disease, keep essential services and critical infrastructure operating, protect employment and the economy, and open up society. It recommended focusing more on a reduction in deaths than on lost years of life, because the indirect effect of avoiding deaths was greater for society and would strongly affect the other goals.
More specifically, the report discussed three categories as a basis for the proposals regarding priority: risk of serious disease and death, the infection situation, and occupation. The first risk category was of direct medical relevance, where the evidence suggests that elderly people are most likely to become seriously ill and/or die of COVID-19, as are younger people with underlying diseases. Therefore, focusing on these two groups would also ease the risk of overburdening the health service. The report also pointed out that underprivileged social groups were overrepresented among people with COVID-19; however, it merely warned that the vaccination program should not cause more inequality without proposing active measures to reduce it, which later became a problem.
Geographical variations in the infection rate were the next criterion. Since the infection rate differed widely from one region to another in Norway, a geographical bias became one a criterion for allocation, because this could reduce the number of deaths and cases of serious disease, avoid overloading the health service, and contribute to a lifting of severe restrictions. Despite this emphasis, geography was not initially a main priority in the allocation process. This later became a major challenge. The third category—occupation—implied giving priority to health personnel and people with critical societal functions, because they had an increased risk of death and disease, were at high risk of infecting others, and were critical for health and other important services.
The Allocation and Re-Allocation of Vaccines in Practice—Changing Priorities
In the fall of 2020, the MHC instructed the NIPH to develop a national plan for COVID-19 vaccination. The plan mainly followed the advice of the COVID-19 expert group and the general government prioritization principles for healthcare (GOV, 2016; NIPH, 2020). The NIPH’s changing advice was mainly followed by the government.
Norway began vaccinating in the first week of 2021; its vaccination program got off to a slightly slower start than those of many other European countries (Sølhusvik, 2021). The original sequence of priorities was to first save lives and then reduce the risk of serious disease. The elderly and the sick in nursing homes were therefore vaccinated first, followed by all those aged 88 years and older. Thereafter, each age group, in descending order, became eligible for vaccination until all those over 18 years had been vaccinated. These allocation priorities were the same as those used by most other European countries (Hunziker, 2021); the only difference was that vaccination of health personnel became the next priority after protecting the most vulnerable groups (Sølhusvik, 2021). Protecting jobs and re-opening the economy were not high priorities.
The crucial question then was how to adjust the vaccine program along the way. The first demands came from front line health personnel who were caring for COVID-19 patients. Four days after the vaccination program started it was adjusted by the NIPH and 15,000 extra doses were allocated for healthcare personnel (Sølhusvik, 2021).
Another controversial aspect that only came to light after some time was that Norway started out with a geographical allocation system based on the proportion of people over the age of 65 years in a given municipality. This implied that small municipalities on the periphery with few infected people received relatively more vaccines because they had the highest share of elderly people, while Oslo, which had by far the most infections, received a disproportionately low share of vaccine, which ran counter to the advice of the WHO. This lack of sensitivity to the actual pattern of infections was reflected in the reluctance of the expert group to base priority on geography and social inequality.
Since Norway is a sparsely populated country with long distances between settlements, small batches of vaccine were initially sent around to many small municipalities, which aggravated the already slow pace of distribution caused by the smaller than expected supply of vaccine from January through March 2021. The allocation principle chosen seems to have been rather ineffective and inefficient, but it had a ring of democracy to it in a country where geo-politics is important.
There was an intensive media debate in February about potential changes in the vaccination program, and a survey among citizens showed that 62% were in favor of prioritizing areas with high infection rates, while 24% agreed with the strategy used. This gave some basic backing to reallocation.
The NIPH argued that the plan had always been to adjust the vaccination program along the way, but this had not been clearly stated at the outset. However, in March 2021, the NIPH stated that the mutation of the virus into variants that spread more quickly, especially in the Oslo area, meant that the focus should be there. This was only partly true since Oslo had had a high infection rate throughout the pandemic irrespective of mutants. The political leadership in Oslo requested more vaccine for the capital several times, and support for this grew based on the argument that “more vaccines in Oslo are a gain for the whole country.” Oslo was the epicenter of infections and it was argued that the government should “extinguish the fire where it burns.” The issue became an increasing focus of media debate, which also stepped up the political pressure; more actors became engaged, and the level of conflict rose. The vaccine allocation program became a hot political issue. Sixty-four mayors from the area around Oslo asked the parliament to intervene and change the vaccine strategy.
The debate became even more heated in late February when the mayor of Molde, a rather small regional city, accused Oslo of not managing the pandemic well and potentially endangering the rest of the country. The subtext to this was that Oslo did not deserve to be given vaccination priority. Several aspects of this statement were interesting. First, until then, there had been few conflicts between different parts of the country, but his arguments indicated a center-periphery conflict. Second, big cities have more potential to spread COVID-19, virtually regardless of what action they take, making criticism of this kind problematic. Third, the mayor of Molde was from the Conservative Party, while Oslo was run by the Labor Party. This triggered a political conflict that would continue in the run-up to the parliamentary elections in the fall of 2021. The prime minister apologized for the incident, because one of her under-secretaries of state had colluded with the mayor without informing her. Through this act she both managed to disagree with the mayor and, more importantly, tried to depoliticize the question; but she was also left with few alternatives to geographical re-allocation.
After discussing a more radical redistribution model that allegedly could save many lives, the NIPH (2021) recommended a clearly more moderate re-allocation of the vaccine in favor of Oslo. The government followed the advice of the agency, deciding that 3% of the vaccines should be re-allocated to those geographical areas that had had 50 or more people admitted to hospital with COVID-19 during a specifically defined period. According to this criterion, which focused on healthcare capacity, six districts of Oslo, most of them less affluent ones with large immigrant populations, and four other cities close to Oslo received 20% more vaccine. What was not communicated so clearly was that this re-allocation decision changed the basic criterion from share of the population over 65 years in a municipality to share of people over 18 years, which favored municipalities with a younger population—that is, the big cities.
The re-allocation generated a lot of complaints from mayors in municipalities on the periphery, who argued that it was unfair, because it treated people differently, and some alluded to the argument that the re-allocation gave unfair advantage to Oslo, which in their view had not been successful in combating the pandemic. Even the minister of children and families said that Oslo’s claim to more vaccine was indefensible. What these actors did not say was that the original allocation had in fact valued elderly people more than younger people, so it had already treated people differently, but with a different profile.
After the re-allocation decision, many groups came forward and demanded that they should receive a larger share of the vaccine. These groups included kindergarten and schoolteachers, supported by their unions and the Labor Party, but also taxi drivers, bar and restaurant personnel, students, and police. In general, their demands were not met at this point in time. Another interesting development was that municipalities were supposed to use 20% of their quota for health workers, but in fact they used 34%, indicating that they had made inappropriate use of their local discretion. The government decided on March 23 to allocate 24,000 extra vaccine doses to health personnel in hospitals, especially in areas with strong infection pressure, such as central hospitals with capacity problems.
A report by an expert group of economists, commissioned by the NDH and published in April 2021, proposed that geography and infection rates should carry much more weight, meaning that the most affected areas should get far more vaccines than the less affected ones (Holden, 2021). Such measures would allegedly save more lives, result in less serious disease, lessen the burden on health capacity and create more opportunities for opening up. The report recommended not only radical geographical reallocation of the vaccines, but also that employees in kindergartens and elementary schools should be prioritized.
On April 30, the government decided to pursue a more comprehensive geographical redistribution of vaccine doses to 24 municipalities in the central part of eastern Norway (the epicenter of infection) on the grounds that these areas were experiencing particularly high infection pressure. This meant that these municipalities received 60% more doses from the beginning of June, while 309 municipalities were allocated 35% fewer vaccine doses.
This change was in line with the advice from the NIPH, which criticized the government for being slow to decide and initially recommended more radical redistribution. The municipalities receiving fewer vaccine doses were again very critical, because it was seen as unfair and caused capacity problems. In late May the government decided to reduce the geographical redistribution somewhat.
On May 22, the government decided to vaccinate members of parliament, cabinet ministers, the Supreme Court, and key personnel in ministries and some central agencies. This decision was rather bad timing and was heavily criticized by health personnel and the medical association. Many of the prioritized key personnel including the minister of health refused to accept this offer.
During the summer of 2021, the situation changed as sufficient vaccines became available and the rate of vaccination speeded up. School teachers were eventually prioritized from July. The Delta variant triggered a surge in cases from mid-August. The focus now was on younger adults and teenagers; vaccinations for 16- and 17-year-olds began on August 18 and for 12 to 15-year-olds on September 2. The authorities now asserted that vaccination was more important than contact tracing.
Summing up, the use of allocation principles in the Norwegian vaccination program changed several times in a rather confusing pattern. Initially the government prioritized municipalities with older populations, which were overrepresented in the periphery, but which had fewer cases of infection. However, the infection pressure was higher in the capital area with its younger population and eventually led to changes in the vaccine allocation policy. This led initially to a slight geographical reallocation, which later became somewhat more radical combined with a stronger focus on young people, which took infection pressure more into consideration. All these changes added up to a rather complex vaccination program.
The second report from the COVID-19 investigation commission (NOU, 2022:5) in late April 2022 criticized the government for not carrying out stronger geographical re-allocation earlier, which could have reduced the number of hospitalized COVID-19 patients. It also criticized the government for not prioritizing teachers earlier. The report revealed some of the processes behind the fact that geographical re-allocation had occurred so late. In interviews with the commission, the minister of health said that he had been against such a re-allocation, but eventually lost out. He argued that the estimates from the NIPH were unreliable, even though they pointed in one direction. The interviews also revealed that the minister of finance had repeatedly supported more re-allocation but had not been listened to. One reason was obviously that the PM was reluctant to support re-allocation, probably for geo-political reasons, and in view of the upcoming national election and fear of reduced public support for the vaccination program.
Analysis—Instrumentalism, Negotiation, and Culture Revisited
How can one understand the vaccine allocation process in Norway, including the main principles used in practice and the actions of and conflicts between actors, in terms of hierarchical, negotiation, and cultural perspectives (cf. Christensen et al., 2020)? First, the vaccine principles were very general and mainly concerned health losses and gains and making the best use of resources. They were potentially inconsistent and conflicting and left a lot of leeway for discretion on the part of decision-makers (NIPH, 2020; WHO, 2020b). The first expert group operationalized these principles to make recommendations about the allocation of COVID-19 vaccines in practice. It also ranked the goals of the vaccine program according to the main handling of the pandemic by the government. The priority was to reduce the risk of death and severe disease and to keep essential services and infrastructure operating; these goals took priority over protecting employment and re-opening society, and it defocused vulnerable groups like children and young people (Christensen & Lægreid, 2020). The recommendations downplayed the social inequality inherent in the spread of infection and thereby also the possibility that the vaccination program would aggravate this inequality. Similarly, it did not focus much on the uneven geographical spread of the disease in setting priorities. Some considerations were defocused or organized out, while others were made more central in their discretionary coupling between general principles and actual allocation (cf. Schattschneider, 1960). This led to biases that did not do much to slow down the pandemic.
When it was decided to reallocate the vaccines and then change the criteria for allocation with a focus on specific areas within the epicenters, the vaccine allocation began to mirror more closely the characteristics of the pandemic. This re-allocation responded to the fact that the epicenters had a disproportionately low share of vaccine. But the re-allocation was cautious and could have been much more radical (Holden, 2021). The second re-allocation sought to further re-adjust the principles in a complex combination of geography and age that was more geared to ending the pandemic, but it came rather late. The re-allocations reflected the fact that in the first phase, expert-dominated vaccine allocation clashed with the political context, which led to an increasingly fierce public debate over vaccine allocation. This had features of “arena shifting” and politicization (Flinders & Buller, 2006). Once Norway had a sufficient supply of vaccines, their allocation became a less politicized issue.
Using a hierarchical-instrumental perspective, one can focus on both the actors and the related patterns of influence and organizational thinking (Christensen et al., 2020). The decision-making process regarding the vaccination program differs somewhat from the main decision-making pattern behind the pandemic regulations, in the sense that the political leadership explicitly “handed over” decision-making power to the NIPH (Christensen & Lægreid, 2020a). On the one hand, this is understandable; most other countries adopted a similar strategy since this is a very specialized issue. On the other hand, the government has the final say on the recommendations, even though it mostly followed and certified expert advice during the first vaccination phase. The re-allocation nonetheless became a hot political issue.
If one looks at the definitional aspects of the process, the original criteria for vaccination priorities and the actual allocation seem to be rational in a rather bounded way, in the sense that not all the decision-making criteria were attended to but only a few selected ones (cf. March & Simon, 1958). The procedure delegated responsibility for formulating a COVID-19 vaccination plan to epidemiological experts in the NIPH who, in turn, based it on the general guidelines for prioritization in healthcare—in other words, standard operating procedures were followed (cf. Cyert & March, 1992). In doing this, it basically followed some of the WHO’s guidelines and allocated vaccine in a similar way to many other Western countries.
The two re-allocation decisions and the criteria connected with them attended more closely to the actual spread of the virus. In that respect they were more rational, but their impact with respect to stopping the pandemic was rather limited. Two types of rationality were present: the first based on principles and traditional criteria for allocation; the second much more context-related and pragmatic (Boin & Lodge, 2021). But even after the last re-allocation, this was criticized as “too little too late,” so combining the two had features of limited rationality.
Exploring the process more from a negotiation perspective, we can identify a development from means-end thinking based on analyses of comprehensive information provided mainly by sector-specific experts toward the increased involvement of different stakeholders trying to defend their own interests and values. Trial-and-error intervention as well as bargaining, negotiation, and coalition-building supplemented rational means-end thinking (cf. Christensen et al., 2020). There was increasing pressure to adjust the allocation policy but the changes in this policy differed only marginally from the status quo, even though the politicization of the issue made the changes look larger than they were in reality. Somewhat paradoxically, the increased features of negotiations over time resulted in more incrementalism and “muddling through” than radical change (cf. Lindblom, 1959). One could also say that it was a case of delegation but also politicization combined with hierarchy, meaning that the negotiation process was characterized more by mutual adjustment between central actors (cf. Boin et al., 2021). As the issue became increasingly salient, the definition of the problems and solutions became more varied and contested, making rational action more difficult.
When the government took the first decision to re-allocate the vaccine, it decided on a very moderate re-allocation as a compromise in order to enhance its legitimacy, which had been called into question by the crisis (Christensen et al., 2016). When the NIPH was pressured to recommend a less radical re-allocation, the decision-making process that had initially been characterized by delegation to the experts now became more of an open negotiation process with diverse stakeholders (cf. March & Olsen, 1983), as revealed by the Corona Commission (NOU, 2022:5).This feature was even stronger in the second re-allocation when it became more of a “sounding-out” process as the government sought to “please” opposing actors both inside and outside the cabinet (cf. March & Olsen, 1976). The pressure on the Conservative government to re-allocate vaccine to the epicenter in Oslo, which was run by the Labor Party, was balanced out by pressure from the periphery, partly from its own supporters. It was accused of giving too much priority to the first demands, even though this would have been the most rational way to stop the pandemic; this was additionally politically difficult because of the coming local election.
From a cultural perspective the vaccine allocation policy started out with strong path dependency informed by principles developed by the WHO and followed up by the NIPH based on recommendations from an external expert ethics group about how to prioritize, meaning that the roots influenced the routes taken (Christensen et al., 2021). This followed a long national tradition regarding healthcare priorities, which was operationalized in giving the elderly, the sick, and healthcare personnel vaccination priority. Traditional norms and values constrained instrumental action, whether hierarchical or negotiational. But the problem with this was that the pandemic in some ways was unique, so more account needed to be taken of contextual features of the pandemic and its actual development as well as the increased politicization of the issue. Yet despite this lack of compatibility between the cultural path and the actual pattern of the pandemic, the change process was more incremental than abrupt or sudden and the resulting change was characterized by continuity more than discontinuity. This resulted in what Streek and Thelen (2005) label “reproduction by adaptation.” (p. 9) Thus, the vaccine decision-making process did not result in a dramatic new path. From the start it was characterized by what one might label “local rationality” on the part of epidemiological experts (cf. Allison, 1971; Cyert & March, 1992). The re-allocations brought about by a more open and politically controversial process did not in the end result in much deviation from the path originally chosen.
Taken together, what we see is more a complex mixture rather than pure ideal-models. The hierarchical-instrumental perspective does not rule out policy adjustments, a negotiation perspective cannot operate without some sort of informed means-end analysis, and to understand the process and outcome one also needs to take cultural constraints and path dependencies into consideration (cf. Christensen et al., 2020). Overall, the study illustrates how these different theoretical perspectives on a “fair vaccine allocation” policy can produce different explanations of the same phenomenon. However, it also illustrates that different perspectives demand different types of data. In this respect it is right out of Allison’s (1971) playbook.
A Comparative Note
Norway was in many respects a high performer regarding the management of the COVID-19 pandemic (Christensen & Lægreid, 2021). The death rate was very low. The trust in government as well as in experts was high. There was no mass polarization and both society and the political elite showed a willingness to cooperate. Vaccination hesitation was low, and the vaccination rate was high. There was no attempt to introduce mandatory vaccination, and the idea of a domestic vaccination passport was not implemented. Thus, the vaccination policy can be seen as a social contract between government and citizens. In this context one would expect the vaccine allocation policy to have been smooth and informed mainly by expert advice based on evidence-based knowledge and expert path-dependency. However, this was only one part of the story. Vaccination allocation policy in Norway was originally delegated to a great extent to epidemiological health experts and their advice was informed by norms and values embedded in the public health community. However, over time the issue became more politically salient and a broader set of actors with different interests succeeded in getting the vaccine allocation policy changed; nevertheless, the hierarchically positioned political executives still had the final say (Christensen & Lægreid, 2022).
Most of the literature on vaccine allocation amid conditions of scarcity revolves around epidemiological issues that arise when developing predictable and optimal prioritization strategies (Matrajt et al., 2021), rather than addressing the political issues and cultural features. However, in practice, implementation of optimal strategies must also take account of other factors such as ethical, political, societal, and contextual aspects. This study adds to our knowledge about the politics of vaccination and how the vaccine allocation policy changed as the pandemic progressed.
Since few countries had sufficient vaccine in the first year of vaccination, governments faced the tough task of determining and defining priority groups for vaccination (Forman et al., 2021). Most countries had guidelines prioritizing individuals at high risk during the early stages of vaccine allocation (Ferranna et al., 2021). Across most countries, high-risk sectors of the population such as older adults, vulnerable people, and frontline health and social care workers were high on prioritization guidance lists (Duch et al., 2021). However, there were still differences: for example, the UK’s prioritization was strictly age-based, while the WHO’s prioritization guidance was occupational group-based.
Most vaccine prioritization analyses have only considered variations in the risk of infection and death by age. But there are also studies that take other factors into consideration (Chapman et al., 2022; Yang et al., 2021). Even when considering top priority groups, equity across and within priority groups must be considered. A challenging problem is also how to allocate vaccines to the remaining population and how to allocate limited vaccines to different groups of people as they become more available over time (Chen et al., 2020). There is a trade-off between prioritizing high-risk groups versus high transmission groups (Bubar et al., 2021). A highly debated issue was whether essential workers should be prioritized over older adults and individuals with serious medical conditions, even though the latter groups were at much higher risk of severe COVID-19-related illness and death (Ferranna et al., 2021).
From an ethical point of view, it is a mistake just to assume that prioritizing the most vulnerable is the best strategy (Giubilini et al., 2021). When large quantities of vaccine are available, a feasible solution could involve first vaccinating the high-risk groups and then allocating the remaining vaccine to the high-transmission groups (Chen et al., 2020). It has also been argued that decisions on who to vaccinate should be highly contextualized. In some settings, the elderly may be prioritized, in others, it may be the population most likely to become infected and hence cause community spread (Russell & Greenwood, 2020).
In a rather under-researched field, one important goal of this study was to focus on the challenges and conflicts related to the allocation program, features that were seen in most other countries (Duch et al., 2021). Even in a well-performing COVID-19 crisis management country like Norway, the allocation of vaccines produced challenges, tensions, and conflicts. At the crossroads between attempts to allocate vaccines rationally and negotiations and path dependencies, features ensue that combine international recommendations for vaccine allocation with unilateral and domestic responses (Christensen & Lægreid, 2021).
Even high trust countries such as Norway need to have a proper crisis response strategy regarding allocation of vaccines to perform well (NOU, 2022:5). It could be seen as a paradox that a high degree of support for the vaccine program was combined with quite a lot of internal allocation conflicts. Quite a few countries in Europe, including France and the UK, encountered resistance to both pandemic regulatory measures and to vaccination, without necessarily experiencing internal conflicts over the allocation of vaccines. The United States seems to have been different from most other countries in that it experienced conflicts over both regulatory measures and vaccines related to deep conflicts between the parties, with vaccine rates having geopolitical features (Palm et al., 2021). Israel used broad criteria for prioritization—that is, dividing the population into fewer groups and having a lower age threshold, which had several beneficial effects (Cylus et al., 2021). Overall, our argument is that a hierarchical-instrumental approach to vaccine allocation needs to be supplemented by a negotiation approach as well as a consideration of domestic path dependencies to understand the complexity of how this policy developed and was implemented across countries.
Conclusion
Summing up, the decision-making process related to vaccination policy in Norway can be seen as an incomplete rational allocation process (jf. Allison, 1971). It was informed by negotiation as different actors and stakeholders tried to defend their own interests and values, but in the shadow of hierarchy. Furthermore, the vaccine allocation policy was constrained by established cultural norms and values which came under pressure over time. The issue of vaccine allocation was not only a question of governance capacity and means-end knowledge, but also involved governance legitimacy and gaining the acceptance of different groups of citizens (Christensen et al., 2016).
The public would favor people for vaccination based on a broad range of factors (cf. Duch et al., 2021). How the government obtained scientific advice and whether it listened to it mattered, but so did the strength and scope of public pressure, while the preferences of government officials influenced the criteria for assessing and managing regulation of vaccine allocation (Forsena et al., 2021). This finding has added value to the politics of regulation and risk assessments in areas of scientific uncertainty that go beyond vaccination (Vogel, 2012).
This study has shown that an intended rational allocation process was constrained by several contextual issues (cf. Pollitt, 2013). One was the infection pattern, which was only partly addressed by the main priority principles in the vaccination program; this was somewhat unexpected. Another was the supply of vaccines, which changed from vaccine scarcity and delayed supplies to an adequate supply. This had a significant influence on allocation policy. In addition, the side-effects of vaccines and virus mutations also played a role in evolving expectations. Thus, an instrumental approach following the WHO’s recommendation of giving top priority to individuals at highest risk of serious disease and death was over time supplemented by negotiations as well as adaptations, whereby measures were adjusted to feedback from vested interests and emerging evidence.
Vaccination was clearly an important measure in countering the pandemic, but it also attended to some extent to other concerns. Moreover, shifts in attention and agenda-setting as well as political opportunities shaped the process (Flinders & Buller, 2006). The challenge was to balance competition for resources and attention, scarcity of vaccines, urgency, long-term planning, expertise, pragmatic adjustments, politicization, governance capacity and governance legitimacy.
A main lesson is that there is an overlap between hierarchical-instrumental, negotiation, and cultural perspectives in interpretating the process of vaccine allocation (cf. Christensen et al., 2020). The implication of this is that rather than seeing the three perspectives as alternatives it might be more fruitful for our understanding vaccination policy and politics to see them as supplementary perspectives. Over time hierarchical control has increasingly been supplemented by negotiations and modification of a traditional cultural path.
Another lesson is that expert bodies, such as the NIPH, not only have a managerial role but also a constitutive one, actively participating in shaping their own purpose (Roberts, 2013). There is a more normative and democratic issue at stake here, begging a discussion of the question of how much should be left to such expert bodies in making the case for a specific vaccine allocation. After all, vaccine allocation involves difficult trade-offs between competing values that cannot be delegated to experts alone (Christensen & Lægreid, 2021).
Challenges for future vaccine allocation policy include increased transparency and communication around why some groups are given higher priority than others and more focus on equity considerations across and within prioritized groups (Forman et al., 2021). Also important for the debate are the trade-offs between different prioritized groups and knowledge about how the allocation of vaccines is affected by the political salience of vaccine policy and the supply of vaccines, and how infection patterns develop in the course of the pandemic.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.