
Abstract
Providing access to adequate and culturally competent healthcare in the United States has been an ongoing challenge with healthcare access barriers impacting the quality of care received by racially and ethnically diverse populations. Despite the preventative measures taken to halt the spread of the COVID-19 pandemic, vulnerable populations and diverse communities were disproportionately represented in COVID-19 transmission and mortality rates. Through a review of the available literature and a quantitative analysis of COVID-19 surveillance data, this study addresses how culturally competent intervention strategies impacted COVID-19 mortality and fatality rates. This paper discusses how community leadership addressed vaccine distribution gaps and delayed government responses for diverse populations were addressed by the community leadership and provides examples of culturally competent solutions to healthcare emergencies. This cross-sectional study contributes to the current literature by exploring the impact of culturally competent healthcare interventions in North Carolina during the COVID-19 pandemic and makes the case for culturally competent practices to reduce the impact on diverse populations.
Keywords
Points for Practitioners
Racially, ethnically and gender diverse populations experience higher transmission, hospitalization, and mortality rates during pandemics and natural disasters.
Culturally competent intervention strategies may be used to address disparities and systemic barriers in healthcare access and outcomes if anticipated and prepared for in a timely manner.
Embedding social equity in policies, programs, and practices addresses healthcare disparities among vulnerable minority populations as they emphasize planning and implementation rather than reactive interventions.
As 2019 Novel Coronavirus (2019-nCoV) (COVID-19) reached the United States in December 2019 and spread across the nation (Centers for Disease Control and Prevention [CDC], 2020a), government leaders grappled with the spread of the virus. Despite social distancing guidance, travel restrictions, and other precautions, the first official deaths from COVID-19 were confirmed on February 29, 2020 (Franck, 2020). In response to concerns regarding how the virus would impact vulnerable populations, public administrators and community leaders developed intervention strategies to reduce transmission rates, mortality rates, and case fatality rates in high-risk communities (Al-Arshani, 2021; Brandt et al., 2021; Servick, 2020). Despite interventions, diverse communities have been overrepresented in both case fatality rates and mortality rates (Artiga et al., 2020; CDC, 2021b; Kaiser Family Foundation [KFF], 2021a; Martin-Howard et al., 2022; Romano et al., 2021).
The COVID-19 pandemic amplified historic barriers to healthcare access (Martin-Howard et al., 2022) with racially and ethnically diverse communities being overrepresented in transmission rates, hospitalization, and mortality rates (CDC, 2021a). The inability of leaders to develop timely Culturally Competent (CC) strategies to offset disparities and systemic barriers resulted in some diverse communities developing their own initiatives for residents (Artiga et al., 2020; Fraser et al., 2021). CC strategies are often used in the helping professions to understand differences between cultures and the unique needs of populations during cross-cultural communications (Nouman et al., 2023). Intervention strategies such as targeted information about ongoing crises and increasing access to resources during times of need are recommended for high-risk and socially vulnerable communities (Harris, 2010; Hussen et al., 2020; Valdiserri & Holtgrave, 2020). Evidence of the success of CC interventions has been seen throughout the literature in a variety of policy (Graves et al., 2007), mental health (Novacek et al., 2020), and public health contexts (Huff et al., 2023). CC testing and vaccination interventions have also been seen at the community level through the mobilization of diverse community leaders, doctors, and clergy (Leider & Wrigley-Field, 2021; Nicola et al., 2020). Risk of mortality can be decreased by developing and implementing strategies for specific high-risk communities (Hawai’i State Department of Health, 2021; Hussen et al., 2020; Valdiserri & Holtgrave, 2020). As diverse communities continue to be overrepresented in virus transmission, hospitalization, and mortality rates (CDC, 2021a; Sadeghi & Wen, 2020), CC solutions offer hope for reducing disparities in healthcare for diverse and vulnerable groups (Harris, 2010).
With the shifting political and racial landscape in the United States indicating a diversifying population (Colby & Ortman, 2015; Frey, 2018; Passel & Cohn, 2020) concerns have risen regarding how public administrators can meet the needs of diverse community residents (Rice and Matthews, 2012) and how to engage in CC pandemic preparation (Hamilton, 2019; Primo, 2013). Through a review of the available literature and a quantitative analysis of COVID-19 surveillance data, this cross-sectional study addresses how CC intervention strategies impacted COVID-19 case fatality and mortality rates in racially and ethnically diverse communities. By describing the impact of CC interventions on case fatality and mortality rates, and examining the influence of CC interventions in North Carolina, this study addresses the research question: how did culturally competent (CC) intervention strategies impact COVID-19 mortality and fatality rates?
To test the research question posed, this paper examines the available literature on CC COVID-19 intervention strategies during the COVID-19 pandemic. This cross-sectional study explores how culturally competent intervention strategies impacted COVID-19 mortality and fatality rates. North Carolina was selected as the state created a specific task force to address COVID-19 health disparities during the pandemic (Andrea Harris Social, Economic, Environmental, and Health Equity Task Force, 2020), and prioritized CC in their 2021 to 2023 strategic plan (NC Department of Health and Human Services [NC DHHS], 2021a). This study contributes to the current literature by exploring the impact of culturally competent healthcare interventions in North Carolina during the COVID-19 pandemic and makes the case for culturally competent practices to reduce the impact on diverse populations.
Literature Review
Despite the measures taken to protect communities from the impacts of the COVID-19 pandemic, the death toll of COVID-19 in the United States continues to increase (CDC, 2024). Though 61% (Figure 1) of the over 1.1 million COVID-19 deaths have been Non-Hispanic Whites/Caucasians, racially and ethnically diverse communities have disproportionately been impacted by the virus (CDC, 2024; National Center for Health Statistics [NCHS], 2021). Despite pandemic preparation anticipating limited resources during times of increased need and providing recommendations for the equitable distribution of resources (Groom et al., 2009; Hutchins et al., 2009; Liao et al., 2011), due to the increased need for Personal Protective Equipment (PPE), COVID-19 testing, and vaccinations, resources were scarce (CDC, 2021b). Though the virus itself cannot discriminate against diverse populations, these populations are considered high-risk groups due to increased social vulnerability and increased risk factors for exposure (Agency for Toxic Substances and Disease Registry (ATSDR), 2021; CDC, 2021b).
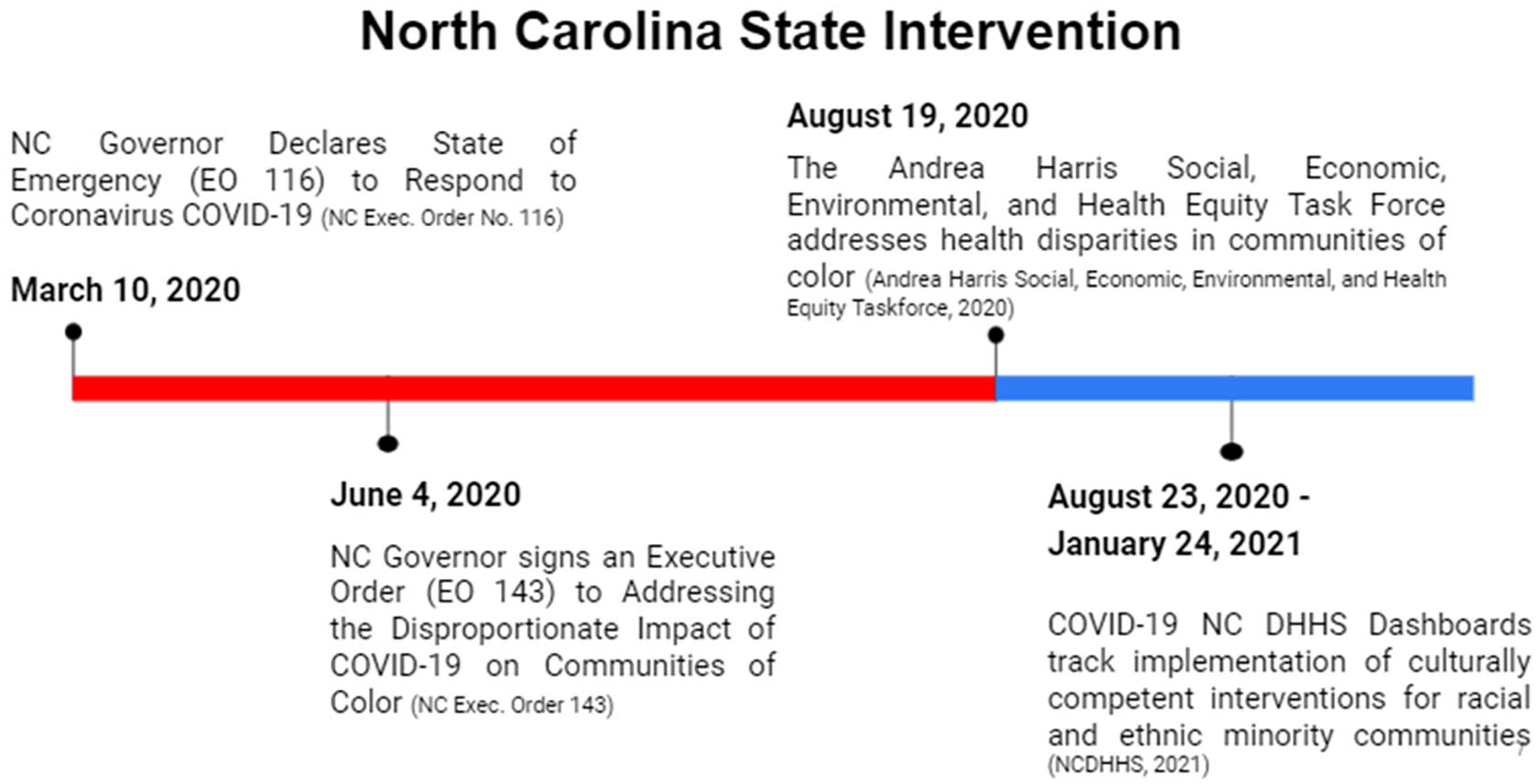
NC cultural competence intervention timeline.
Diverse communities are at an increased risk for being impacted by illness and disease due to cultural norms, socioeconomic living conditions, overrepresentation in affordable housing communities with higher population densities, and, increased likelihood of living in intergenerational households (NAS, 2020; Reyes, 2020). Barriers such as access to education and income result in increased likelihood of being employed in front-facing positions with increased interaction with the public (Bureau of Labor Statistics, 2020). These positions are more likely to lack healthcare benefits, provide benefits for preventative care, and lack sick leave to accommodate testing and vaccinations. Sick leave is crucial for many low-income individuals who cannot afford to be out of work and quarantine while awaiting COVID-19 test results. Moreover, front-facing positions are more vulnerable to incidents such as pandemics as workers do not have the ability to complete work tasks from home or lack the technological infrastructure to do so (Bureau of Labor Statistics, 2020). Individuals in these positions are at an increased risk of layoffs, unemployment, and at risk of losing limited health care benefits (ATSDR, 2021; CDC, 2020b, 2021). These factors are further exacerbated by the prioritization of white communities, their increased access to COVID-19 testing, and neglect of racially and ethnically diverse communities (NAS, 2020).
Testing and Treatment for Diverse Populations During the COVID-19 Pandemic
As communities began to mobilize and establish COVID-19 testing sites in summer 2020, sites were overwhelmingly launched in primarily white neighborhoods (Brandt et al., 2021). Despite barriers to healthcare and access to testing, many diverse individuals who were able to access a testing site were denied the opportunity for a COVID-19 test due to not meeting testing criteria, having a prescheduled appointment, or doctor’s referral being needed for an appointment (McElfish et al., 2021). These barriers created additional burdens for diverse individuals in North Carolina, specifically African American individuals who experienced higher COVID-19 infection rates in their communities (Corbie-Smith, 2021). Those who were able to overcome the obstacle of the financial and time barriers of scheduling an appointment with a physician to obtain a referral for a COVID-19 testing, doctors frequently failed to recognize early signs of COVID-19. Across the nation, African American people were repeatedly denied COVID-19 testing, treatment, and medical care (Reyes, 2020; Shamus, 2020). Barriers to testing for this group have been so widespread that 73% of Non-Hispanic African Americans in the United States reported that greater access to testing was needed, compared to 55% of Non-Hispanic whites/Caucasians (Quest Diagnostics, 2020).
These barriers have not been the only deterrents for individuals in need of COVID-19 testing. Some reported that they did not seek testing as they were afraid that leaving their homes or varying from their daily routine to get tested might result in a COVID-19 infection. With reports of people being turned away from COVID-19 testing sites, many who felt they might have contracted the virus decided the process of getting tested was too risky compared to socially distancing at home (Heard, 2021). Exposure during testing was the concern of many Hispanic individuals as well. According to a national survey, 83% of Hispanics reported having postponed or refused a necessary COVID-19 test despite believing they contracted the virus compared to 72% of both (Non-Hispanic) White and (Non-Hispanic) African American patients (Quest Diagnostics, 2020). A separate study by Zhang et al. (2022) found that African Americans and Hispanics were the most likely to report delaying healthcare during the pandemic, while Hispanics and Asians were more likely to report discrimination when receiving COVID-19 treatment. These disparities directly impacted COVID-19 testing and treatment with African Americans and Hispanics in North Carolina experiencing both higher rates of case mortality compared to White residents during the summer of 2020 (Still, 2020).
Despite the reported avoidance of testing sites and healthcare, many Hispanics and African Americans did seek testing only to discover that they were unable to travel to a testing location due to not owning a vehicle or inoperable public transportation. For those who attempted to seek walk-up testing in North Carolina and other states, many were denied a COVID-19 test due to walk-up testing being considered hazardous for healthcare workers (Brandt et al., 2021). Hispanic individuals working in the trade industry and at high-risk of infection (Bui et al., 2020) found that they were unable to complete a COVID-19 test due lack of language accommodations. Wait times for testing averaged between one and two hours resulting in healthcare workers and testing volunteers being overrun with individuals in need. English-speaking testing staff were unable to assist non-English speaking individuals as “calling for a translator [was] logistically impossible” (Behbahani et al., 2020). Furthermore, Trump-era changes in immigration policy resulted in Hispanic individuals being wary of messaging from government agencies and wary of their immigration status being threatened if they sought medical treatment (Behbahani et al., 2020). This discouraged those with vulnerable immigration statuses from seeking COVID-19 treatment, testing, and vaccinations (Heard, 2021).
Communication and messaging with minority populations has been a challenge for government agencies. In North Carolina and other states, CC public health strategies like government-created education materials for the public during the pandemic were not readily available in Spanish, nor were education materials in Spanish reaching the intended populations (Robinson, 2021; Wagner & Sanchez-Guerra, 2021). CC solutions for Spanish-Speaking populations were implemented in a few locations throughout North Carolina as government, health, and legal professionals developed partnerships for distributing translated information about the ongoing pandemic to Spanish-Speaking communities. These efforts included not only translated information, but connecting with Spanish-Speaking community leaders, and providing cultural humility training to healthcare providers (Robinson, 2021).
Spanish-speaking residents in North Carolina who traveled to testing sites and had overcome logistical, language, and transportation barriers were surprised to find police officers working at testing sites to assist healthcare workers by directing traffic and providing other police services (Fisher & Harden, 2020). The presence of police officers combined with a mistrust of government agencies and fear of being targeted for immigration related questioning, resulted in many leaving testing sites out of fear. A feeling that African Americans share having experienced historical discrimination and targeting from police officers and living during the heightened political unrest in the wake of the murder of George Floyd (Stolberg, 2020).
While police presence may have deterred Hispanics and African Americans from testing sites, the presence of police officers may have been a welcome sight for Asian populations who experienced increased discrimination due to the COVID-19 virus having originated in the Wuhan Province, China. Studies have found that since the beginning of the pandemic, there has been an increase in xenophobic and cynophobic comments across social media (Litam, 2020; Yang et al., 2020). Sentiments which increased after former President Trump used Twitter to condemn the “Chinese Virus,” igniting a wave of anti-Asian sentiments on social media and sparking the viral hashtag “#chinese virus,” and “#china virus,” among others (Hswen et al., 2021). A study conducted by the Center for the Study of Hate and Extremism, reported that there was a 179% increase in reported hate crimes against Asian Americans in the first quarter of 2021 compared to the first quarter of 2020 (Yam, 2021). While discrimination and prejudiced hashtags surfaced across social media, incidents of bias crimes and hate crimes increased with 80% of physical and verbal assaults occurring in public places (e.g., grocery stores, businesses, on public transportation, etc.) making being in public unsafe for Asian Americans (Tessler et al., 2020; Yam, 2021).
Discrimination against Asian Americans became so widespread that congress passed the COVID-19 Hate Crimes Act (S.937) to expedite reviews of reported hate crimes against Asian Americans, and to memorialize Asian victims of hate crimes. Despite scholars estimating that the number of hate crimes and bias incidents against Asian Americans have been underreported, 33% of Asian respondents to a Kaiser Family Foundation (KFF) survey about Asian experiences during the COVID-19 pandemic “report[ed] that they have personally felt more discrimination based on their racial/ethnic background since the COVID-19 pandemic began in the U.S.” (Artiga et al., 2021). As such, many Asian Americans were hesitant to venture out of their homes during this time due to a fear of harassment and discrimination, impacting the safety felt at COVID-19 testing locations and likelihood of getting tested for the virus.
As federal, state, and local governments provided access to testing and other resources for communities in need, indigenous/First Nations populations residing on tribal lands found themselves 3.5 times more likely to contract COVID-19 compared to Non-Hispanic Whites/Caucasians (Horse & Huyser, 2022). As tribal governing bodies maintain sovereignty on tribal lands, these populations are frequently disproportionately impacted by pandemics due to legal barriers for tribes in need of emergency assistance. This is because each tribe has a unique agreement with the United States government and often must wait for an emergency declaration or must specifically request funding to aid tribe members (Federal Emergency Management Agency [FEMA], 2021). Due to the historical implications of viral infections having been used as the first recorded instance of biological warfare against First Nations Peoples in the United States, Native American populations are fully aware of the devastating impact that infectious diseases can have on their communities (Galassi, 2015).
Due to this reality and higher levels of chronic conditions, Native American populations are uniquely vulnerable to COVID-19. Though the Indian Health Service (IHS) provides resources for populations living on tribal lands, testing, treatment centers, and healthcare providers are frequently inaccessible and under-resourced due to travel distances from remote locations to the healthcare site. Additionally, reporting concerns have been a barrier for Native populations as some tribes report cases by zip code, as part of Asian case numbers, refuse to provide case data, and/or provide case data without the consent of tribal leaders (Leggat-Barr et al., 2021). This has led to Native populations being disproportionately impacted by COVID-19 in states like Arizona, New Mexico, North Carolina, and Oklahoma where Native American populations contribute to less than 10% of the state’s total population but have accounted for 40% to 50.8% of COVID cases (Gopi & Nair, 2020; Horse & Huyser, 2022).
CC Interventions During the Pandemic
African American Communities
As the pandemic worsened over the summer of 2020, testing sites began to be established in diverse communities by community residents themselves and/or municipal leaders due to evidence of disproportionate impact of COVID-19 on diverse neighborhoods (Brandt et al., 2021; Servick, 2020). Rates of disease and chronic illness (primarily Diabetes, heart disease, Nephritis, HIV, and homicide) have historically been higher in African American communities (NC DHHS, 2023) due to a variety of environmental and nutritional factors (Gaskins et al., 2007). Higher rates of chronic illness and disease in these communities not only result in increased vulnerability to COVID-19 but social distancing and reduced treatment options have negative health impacts for individuals with co-occurring diagnoses (Saqib et al., 2023).
CC community and municipal interventions differed across the nation with the largest examples of community mobilization being in southeastern African American communities. Considered an essential element to interacting with African American communities during the pandemic, across the United States countless church clergy members used their position of influence to reach community members (Al-Arshani, 2021; Brandt et al., 2021). With CC interventions such as mobilization of African American clergy members, many houses of worship became hubs for COVID-19 related information and services (Clasen-Kelly, 2023; Moore et al., 2022). Community churches began to be used as testing sites, clergy/volunteers provided educational materials about the importance of testing and vaccinations, and government partners and doctors were able to reach African American communities in a CC way using the existing community framework (Van et al., 2020).
Though there are many barriers to healthcare access in African American communities, individuals reported avoiding COVID-19 testing due to the history of maltreatment and oppression, and a cultural fear of discrimination and maltreatment from White healthcare providers. According to Al-Arshani, many African Americans were concerned that COVID-19 testing, and vaccine distribution was the equivalent of the infamous Tuskegee experiment (2021) where the federal government experimented on, infected, and withheld treatment from African Americans in the name of medical research (Heintzelman, 2015). With African Americans considering the lack of testing to be a continuation of past injustices by White service providers and the medical community, those who were able to access COVID-19 testing and vaccinations were hesitant to do so.
Hispanic Communities
African American and Hispanic populations have been found to be uniquely vulnerable to the COVID-19 pandemic. The two groups account for over 25% of service workers, and 16% of transportation workers making them more likely to be considered essential workers and being forced to remain in their positions not qualified for remote work (Bureau of Labor Statistics, 2020). Hispanic individuals have been disproportionately impacted by COVID-19 (Carrion et al., 2021; Vilar-Compte et al., 2021) due to systemic barriers, and avoidance of seeking medical treatment (Czeisler et al., 2020) due to mistrust, fear, and lack of appropriate language accommodations (Behbahani et al., 2020; Fisher & Harden, 2020; Heard, 2021). As a result, Hispanics and Latino COVID-19 cases are one of the most under-diagnosed racial/ethnic groups that also suffer from “provider bias and less access to culturally appropriate health care services” (Rodriguez-Diaz et al., 2020).
To combat this disproportionate impact, organizations serving Hispanic communities and other community leaders organized to close the gap for Hispanic populations. While some initiatives were launched by academics and local governments and highlighted the strengths and benefits of engaging communities directly (Epps et al., 2021), impacted communities were already at work due to delayed government response. Organizations in different states such as the Latino Community Fund Georgia and El Centro Hispano (North Carolina), began raising funds for services such as COVID-19 testing, vaccinations (El Centro Hispano, 2020; Pratt, 2021), and for to provide food for families impacted by COVID-19 (Lazo et al., 2021). Successful strategies included connecting with church and community leaders, or with respected members of Hispanic communities such as pastors or “abuelas” (the Spanish word for grandmother) (Pratt, 2021). By utilizing a CC community-based approaches where mobile clinics provide language-appropriate services to communities in need and utilizing CC imaging for information such as cartoon abuelas for nervous children (Pratt, 2021) communities have been able to provide CC interventions which are necessary for survival (Hooper et al., 2020).
Asian Communities
For Asian communities (including Pacific Islanders/Native Hawaiians), outside of the physical and verbal assaults that have occurred because of discriminatory rhetoric, is the failure of governments to identify individual communities within this identified racial and ethnic category as unique. As a result, individuals with ancestors from East Asian nations are all provided with the same information regardless of country of origin therefore relying on the community to provide necessary resources such as translation services. This creates an additional barrier during pandemics with Asian subpopulations. Classifying distinct populations as Asian/Pacific Islander/Native Hawaiian does not accurately describe individuals resulting in some groups being categorized as Asian and/or other interchangeably (Wang et al., 2020). As a result, studies by Yan et al (2020) indicate that “Asians are four times more likely to die after contracting COVID-19 than white individuals while failing to depict the true impact of the virus on specific populations.” Despite these data and reporting concerns, successful COVID-19 interventions for “Asian” communities have been documented by identifying unique subpopulations and providing CC responses for those communities in their primary language (Leider & Wrigley-Field, 2021). CC solutions for Asian subpopulations also include factoring in cultural norms such as multi-generational households and including community leaders in planning strategies through representation and community engagement (Carrion et al., 2021; Hawai’i State Department of Health, 2021).
Native American Communities
With Native American populations becoming infected at 3.5 times the rate of non-Hispanic Whites (Hatcher et al., 2020), tribes worked to provide their own CC COVID-19 response. In North Carolina, the Lumbee Tribe in collaboration with two local universities developed a CC intervention for tribal members consisting of free COVID-19 testing and education for the Lumbee community. The initiative worked to spread information about COVID-19 in an accessible way to tribal members in remote locations (UNC Pembroke News, 2020) and provided reliable information to communities wary of information from the government due to mistrust (Shi et al., 2023).
Similar CC testing and vaccination intervention strategies were seen in the Cherokee Nation, Oklahoma. Compared to surrounding non-Hispanic White communities, the Cherokee Nation’s elders successfully mobilized free drive-up COVID-19 testing, PPE, and other resources for those in need (McFarling, 2020). The success of the Cherokee COVID-19 response has been well documented (Hathaway et al., 2021; Kaur, 2021; Kelley, 2020; McFarling, 2020) and commended for having succeeded where federal agencies have failed. By “following the science,” responding quickly and implementing mask and social distancing mandates, creating a Cherokee Nation COVID-19 Dashboard, providing information about the pandemic in Cherokee and English, and gaining support from the Chief; the Cherokee’s CC solutions saved thousands of lives (Cherokee Nation, 2021; McFarling, 2020). Due to these CC strategies demonstrated by the Lumbee, Cherokee, and other tribes, Native American populations were able to provide information, testing, and vaccinations to vulnerable and vaccine-hesitant communities (Chumburidze, 2021; Locklear et al., 2021).
Importance of Timely CC Vaccination and Testing Interventions
Practices that specifically target high-risk communities are essential to decrease the disproportionate impact on vulnerable communities (Schneider, 2013). CC Interventions such as testing in diverse neighborhoods must be embedded into pandemic planning to reduce disparities. When testing sites were established in diverse neighborhoods with low socioeconomic status, studies found that these sites lacked staffing, resources, and, had longer wait times compared to testing sites in predominantly White and high income neighborhoods. After these sites were established as a CC intervention in minority neighborhoods, the demographics of those being tested at the sites were not representative of the populations residing in those communities. White residents from neighboring communities had traveled to minority neighborhoods to take advantage of decreased wait times (Linly, 2020; Servick, 2020). To prevent this disproportionate impact, public administrators working across states in emergency management and sustainability must both anticipate and prepare for the unique needs of vulnerable populations to engage in equitable and ethical pandemic response and ensure the survivability of minority communities (Schneider, 2013).
North Carolina Context
One of the most highly populated states in the nation, North Carolina is home to over ten million residents with an average population growth rate during the last ten years at around 9.5% (US Census Bureau, 2023a). The state boasts both growing urban areas and declining rural cities where communities have experienced widespread hospital closures (Brandt et al., 2021). A survey of adults across 12 rural counties in North Carolina in 2005 (Arcury et al., 2005) found that individuals in rural communities were not only significantly poorer than their urban counterparts, but also had increased difficulties accessing healthcare in addition to not being able to afford treatments and medical services. Prior to and during the pandemic, North Carolina residents in rural areas struggled to access medical care due to the lack of provider availability (Arcury et al., 2006) and higher out of pocket costs. The cost of healthcare for residents continues to increase annually with healthcare expenditures per capita in North Carolina in 2020 being $8,917 (KFF, 2022). Total expenditures on healthcare vary among residents in the state with urban residents spending less on individual deductibles, copayments or cost sharing amounts (Less than $7,000) compared to individuals in rural areas. Residents in counties such as Bladen, Lenior, Jones, Bertie, and Chowan pay the highest out of pocket costs, with annual averages totaling over $10,000 (Karen, 2020).
North Carolina has one of the highest rates of Medicaid use in the nation with 1.8 million enrolled during June 2020 and 2.3 million (or one in four) being enrolled in August 2023 (KFF, 2021a). Vulnerable populations such as those with chronic illnesses are considered high-risk not only for contracting the COVID-19 virus, but are also more likely to experience the lingering impacts of COVID-19 referred to as long-COVID (Muratori Holanda et al., 2021). As low-income individuals in North Carolina are more likely to contract the virus and an estimated one third of individuals who contract COVID-19 will develop long-COVID, low-income individuals are at an increased risk for experiencing negative health impacts in the long term (Murator Holanda et al., 2021). With 39% of adults considered high-risk in North Carolina due to chronic illness and 19.4% reporting being in poor health (KFF, 2021b), a large percentage of the population is extremely vulnerable to pandemics and healthcare emergencies.
COVID-19 Response in North Carolina
On June 4th NC Governor Roy Cooper signed an Executive Order (EO 143) called addressing the Disproportionate Impact of COVID-19 on Communities of Color (NC Exec. Order 143, 2021). This Executive Order resulted in the development of the Andrea Harris Social, Economic, Environmental, and Health Equity Taskforce (AHSEEHETF), whose mission was to investigate widespread health disparities in diverse areas (AHSEEHETF, 2020). The task force developed many recommendations and intervention strategies, however, not all the proposed suggestions were implemented. One recommendation was the creation of the COVID-19 Dashboard to track impact on communities and implementation of CC interventions. The NC DHHS Dashboard was created and began tracking demographic impact data on August 23, 2020 (NC DHHS, 2021b). A Patient Engagement Subcommittee (PES) was developed at this time to investigate and provide a plan for meeting short-term goals by December 2020. As not all recommendations were implemented or provided an intervention, this study explores the impact of CC intervention strategies implemented between August 23, 2020, through January 24, 2021.
In response to the rising mortality rate of North Carolinians, and the high rates of transmission between racial and ethnic minority groups, North Carolina (NC) developed a task force to address systemic barriers prohibiting the access to healthcare (Andrea Harris Social, Economic, Environmental, and Health Equity Taskforce, 2020). This task force provided recommendations for strategies designed to reduce mortality rates and to close the vaccination gap between racial and ethnic groups (NC DHHS, 2021c). After North Carolina Governor Roy Cooper signed Executive Order (EO 143), Addressing the Disproportionate Impact of COVID-19 on Communities of Color (NC Exec. Order 143), the AHSEEHETF was created to encourage medical professionals to engage communities of color to gather information and provide a platform for transparency and inclusion; support and identify opportunities to increase the number of minority health professionals servicing communities of color; and encourage increased cultural competence in the provision of care for communities of color (AHSEEHETF, 2020).
As one of the intervention recommendations of the task force was to develop a dashboard to track impact on communities and implementation of CC interventions, the COVID-19 Dashboard was developed by the NC DHHS and began tracking demographic impact data on August 23, 2020 (Andrea Harris Social, Economic, Environmental, and Health Equity Taskforce, 2020). The committee then created a Patient Engagement Subcommittee (PES) to set short-term goals that should be completed no later than December 2020.
The PES met for the first time on August 19, 2020 (see Figure 1) and developed four short-term goals to address rising mortality rates. First, the creation of a data collection initiative to track demographic data of those impacted by COVID-19 and making the data accessible to the public. Data collection included information on race, ethnicity, gender identity, sexual orientation, and other identifying attributes to accurately determine the impact of the virus, assess impact, and address barriers through policy recommendations (Andrea Harris Social, Economic, Environmental, and Health Equity Taskforce, 2020). Second, the PES conducted research into the practices of health agencies to determine how agencies were engaging vulnerable populations and educating them about the ongoing health crisis. This was for the purpose of creating guides for agencies to assist them with informing diverse populations about the pandemic (Andrea Harris Social, Economic, Environmental, and Health Equity Taskforce, 2020). The PES’s third goal was to question the necessity of police presence at testing sites, provide recommendations for alternatives to police officers, and encourage community representatives to engage at testing sites to build community trust. The final goal of the PES was to conduct research into the best practices of patient engagement to make equitable policy recommendations.
In addition to these goals, the PES implemented additional intervention strategies including developing relationships at the state and local level to provide telehealth services to individuals in quarantine or others whose movement was restricted. The NC DHHS also created vaccination awareness programs for diverse communities, specifically Spanish-speaking communities to ensure the delivery of accurate pandemic-related information. NC DHHS further contracted community health workers and behavioral health specialists to support patients in quarantine. Additional funding was also allocated for NC Office of Rural Health’s Information Technology Program to assist with providing technical support for telehealth services. As a result, federal Health and Human Services guidelines were temporarily lifted to allow for “noncompliance with the regulatory requirements for telehealth communication technologies under the Health Insurance Portability and Accountability Act of 1996 (HIPAA), meaning that providers would not be penalized for providing telehealth services via HIPAA-non compliant platforms such as FaceTime, Facebook messenger, and Skype” in addition, controlled substances were permitted to be prescribed after telehealth visits (AHSEEHETF, 2020). These relaxed policy guidelines directly impacted the care received by low-income individuals in rural areas benefited from this change in policy the most, with 29.3% of telehealth users being Medicaid beneficiaries (Assistant Secretary for Planning and Evaluation, 2022).
Methodology
To assess the impact of culturally competent healthcare interventions in North Carolina during the COVID-19 pandemic, this cross-sectional study utilizes data collected from the NC DHHS Dashboard to compare the impact of strategies prior to and after implementation of CC interventions. A cross-sectional study was selected as these observational studies measure both outcomes and the prevalence of diseases in populations (Setia, 2016). Limitations of this design are that cross-sectional studies, being that they examine a snapshot in time, cannot establish causality (De & Singh, 2019). This study will analyze changes in crude case fatality rate, crude mortality rate, and percentage of total deaths by race and ethnicity in NC prior to CC Intervention (March 15, 2020–August 22, 2020) and after (August 23, 2020–January 24, 2021). This timeframe was selected as August 23, 2020, is the first day that the NC DHHS Dashboards began tracking the implementation of CC interventions in diverse communities. Additionally, the Andrea Harris Social, Economic, Environmental, and Health Equity Task Force’s goals were to have been implemented by December 2020 (AHSEEHETF, 2020).
Data Collection
The NC DHHS Dashboard was created to track COVID-19 transmission rates, mortality rates, and case fatality in various communities across all 100 counties. This resource was utilized to collect COVID-19 cases and deaths by week, per county, and, by race and ethnicity. As the COVID-19 dashboard provided a weekly time frame, data was divided into two-time frames following the NC state intervention timeline: (1) before CC intervention (23-week period) and (2) after CC intervention (23-week period). While interventions may have been implemented after January 24th, 2020, this date was selected to allow for any interventions implemented in December 2020 to be included in the analysis and to compare two 23-week timeframes.
The dashboard included COVID-19 data by race and ethnicity but did not include data about the racial and ethnic populations in each county. Population data were compiled from the United States Census Bureau’s 2019 population survey, and the Census Reporter to gather information about COVID-19 cases, and deaths by race and ethnicity per county as well as total population of racial and ethnic groups per county. For COVID-19 reporting and for the United States Census, ethnicity is reported as either Hispanic or Non-Hispanic, and is not a racial category. To assess impact, intervention data was compiled to create separate comparisons of cases and deaths by race and ethnicity.
Sampling
Using the NC DHHS COVID-19 Dashboard data, as well as data from the 2019 United States Census and Census Reporter, the sample included all individuals of all racial and ethnic backgrounds in NC. COVID-19 case data included positive COVID-19 cases and deaths for NC, positive COVID-19 cases and deaths by race and ethnicity for all 100 counties during March 15, 2020–August 22, 2020 (Pre-CC Intervention), and August 23, 2020–January 24, 2021 (Post-CC Intervention). The sample included five racial groups: (1) African American, (2) American Indian/Alaska Native, (3) Asian/Pacific Islander/Native Hawaiian, (4) White, and (5) Multiple/Other (biracial individuals or those who do not fit into another racial category). Data on ethnicity included two categories: (1) Hispanic, and (2) non-Hispanic. As the COVID-19 Dashboard categorizes individuals from east Asian countries as Asian/Pacific Islander, compared to the United States Census’ separate distinctions between Asian and Native Hawaiian/Other Pacific Islander, these individuals were grouped together for the purpose of this study. Since the literature indicates that individuals from Asian/Pacific Islander/Native Hawaiian subgroups are frequently categorized as being Asian despite Pacific Islander ancestry and vice versa (Wang et al., 2020), these categories were combined to capture the impact of COVID-19 on these racial groups. Since data obtained from the NC DHHS Dashboard included racial and ethnicity data categorized as “suppressed” (indicators removed confidentiality) or “missing” (where racial/ethnicity was not reported), this data was not included in the report.
Instrumentation
To explore the research question posed, case fatality rates (deaths by number of COVID-19 cases), mortality rates (deaths by population per 10,000 people), and percent of total deaths (deaths by population as a percentage of total deaths) were calculated using NC DHHS COVID-19 data and United States Census population data. As case by race and case by ethnicity were reported separately, mortality by racial group and mortality by ethnic group were also calculated separately. Racial and ethnic case fatality and mortality rates were calculated using the following formulas (Figure 2): Case Fatality (deaths by number of cases) Calculation: deaths / total cases Mortality Rates (deaths by population) Calculation: deaths / per specific population (per 10,000) (Figure 2)
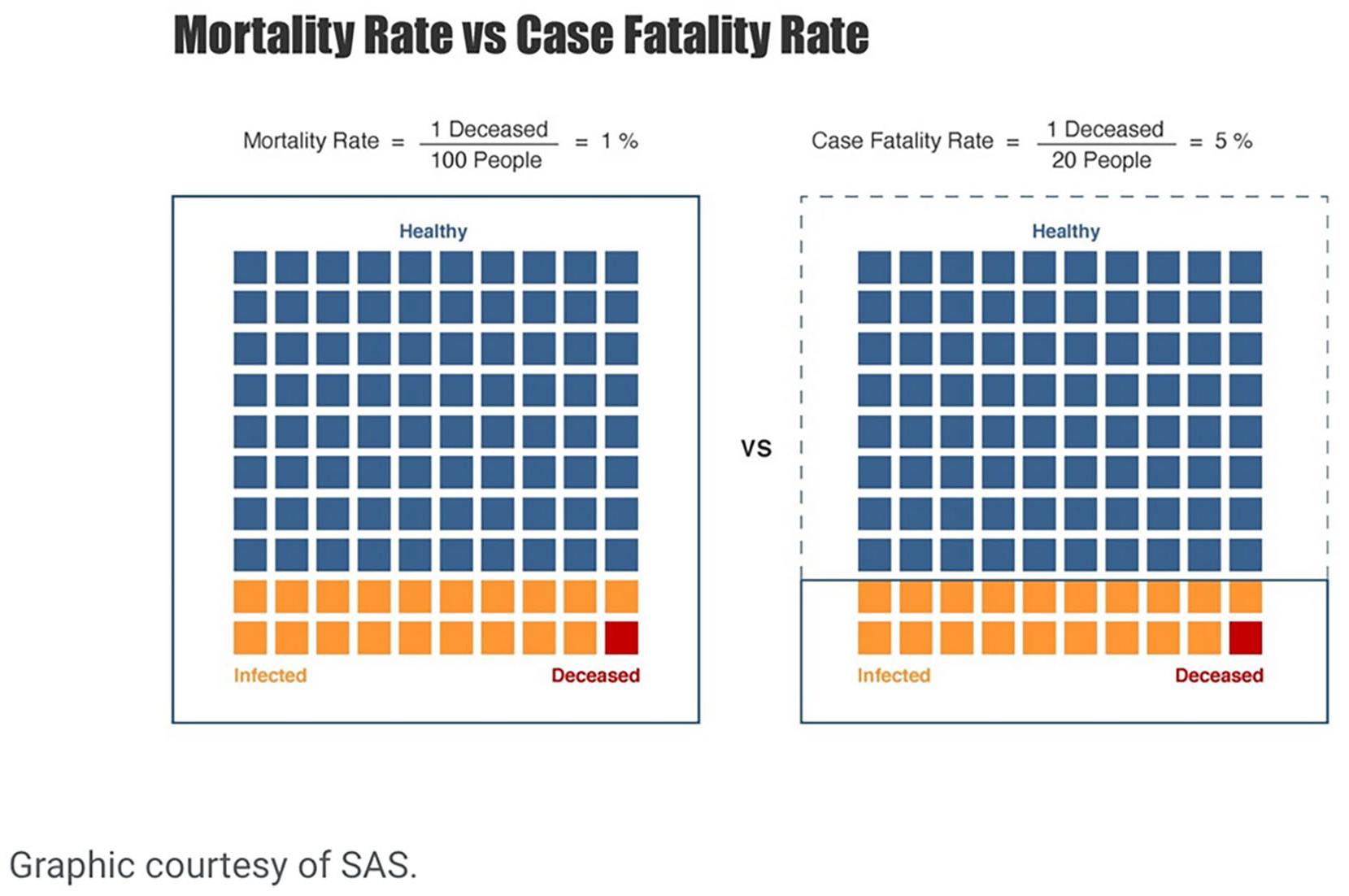
Explanation of mortality rate vs case fatality rate.
To calculate the case fatality and mortality rates by racial and ethnic group, United States Census data was used to obtain the number of individuals in each racial and ethnic group in all 100 counties in the State of NC. Using CDC data on the number of COVID-19 cases and deaths by week, racial, and ethnic group were calculated for the State of NC and per county before the CC Intervention period (March 15, 2020, through August 22, 2020) and after the CC Intervention period (beginning August 23, 2020, through January 24, 2021). Then, using the case fatality and mortality rate formulas provided above, the case fatality and mortality rates were calculated for the State of NC, racial group, and ethnic group before and after CC Intervention. Afterwards, the percentage of case fatalities by racial and ethnic group as a percentage of total case fatalities was calculated. Finally, the Before CC Intervention and After CC Intervention case fatality rates, mortality rates and percent of total deaths by racial and ethnic groups were compared as a percent change Before CC Intervention and After CC Intervention.
Discussion and Results
Between March 15, 2020, and August 22, 2020, a total of 169,768 North Carolina residents whose racial data had been reported, and 171,278 people whose ethnic data had been reported had been diagnosed with COVID-19. This number increased to 659,605 COVID-19 cases by race and 659,874 COVID-19 cases reported by ethnicity by the end of the post-intervention period on January 24, 2021, resulting in a 288.53% increase in total cases by race and a 285.26% increase in total cases by ethnicity. During that same time frame, between March 15, 2020, and August 22, 2020, a total of 3,328 people who had been diagnosed with COVID-19 by race and 3,327 people who had been diagnosed with COVID-19 by ethnicity compared to 8,186/8,263(race/ethnicity) COVID-19 deaths after CC Intervention (see Appendices A and B for full data tables). Across all racial and ethnic groups, the crude mortality rate increased from the Before CC Intervention period to After CC Intervention period, except for the Multiple (Multiracial)/Other racial group where mortality rates were seen to decrease (Table 1).
Case Fatality & Mortality by Racial Group.

Source. Created with NC DHHS COVID-19 data and United States Census population data.
The results in Table 1 show that for all racial groups decrease in case fatality from the Before to After CC Intervention period, showing that fewer people diagnosed with COVID-19 overall died in NC due to COVID-19 after the CC Intervention with the greatest decreases being seen in American Indian/Alaska Native (decrease of 1.27%) and African American populations (decrease of 1.11%). All minority racial groups (African American, American Indian/Alaska Native, Asian/Pacific Islander/Native Hawaiian, Asian/Pacific Islander/Native Hawaiian, and Multiple/Other) were seen to have a decrease in percentage of total deaths with the greatest decrease being seen in African American (decrease of 5.23%) and Multiple/Other (decrease of 4.09%). Whereas the White case fatality was seen to decrease along with all racial groups, the percentage of White total deaths was seen to increase by 13.69%. Crude mortality rate increased After CC Intervention in NC (4.64 deaths per 10,000) among all racial groups except Multiple/Other with 1.67 per 10,000 Multiple/Other people dying After CC Intervention compared to 5.86 per 10,000 Multiple/Other people dying Before CC Intervention. This shows that fewer people died across racial groups after being diagnosed with COVID-19, and African American benefited more from CC Intervention than other racial groups.
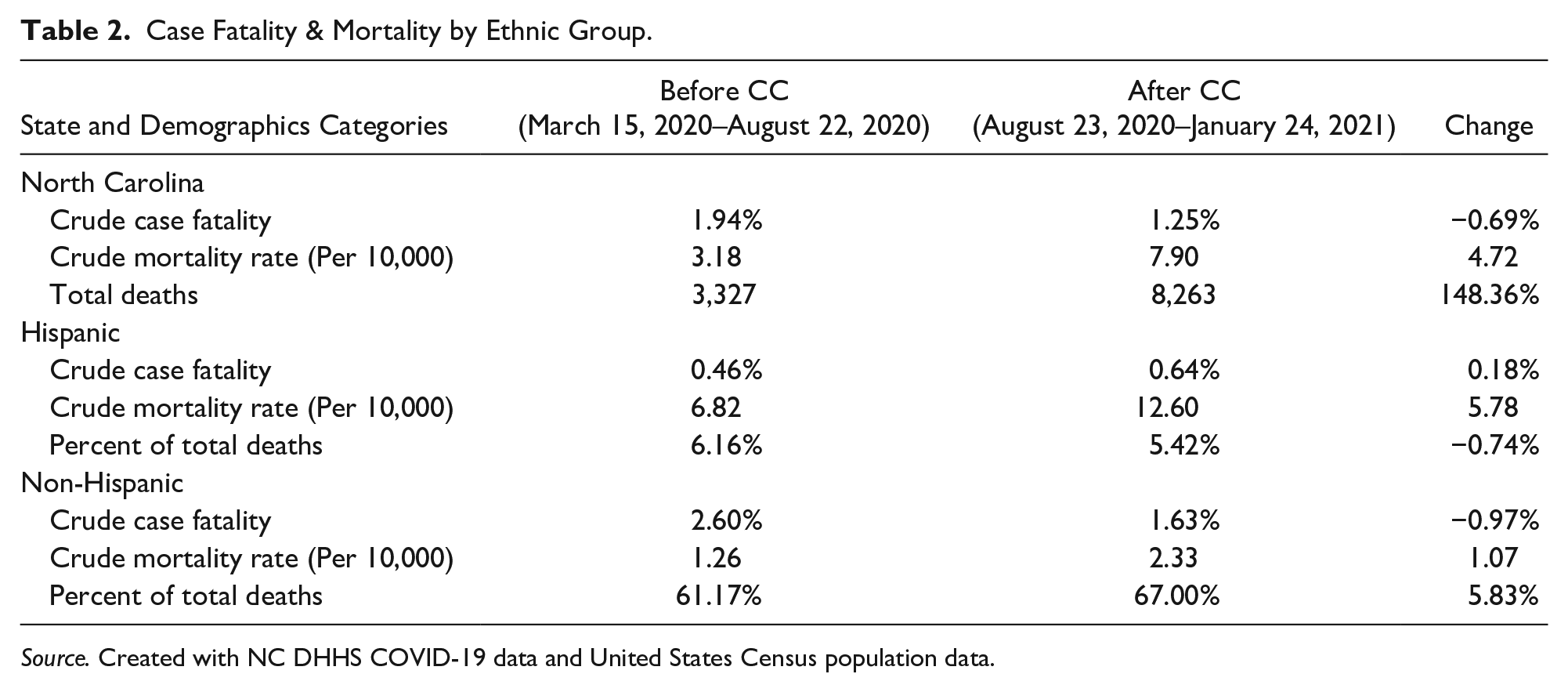
Results in Table 2 show that case fatality decreased from Before CC Intervention to After CC Intervention in NC (decrease of −0.69%) and for non-Hispanic populations (decrease of −0.97%) compared to an increase in Hispanic case fatalities (0.18%). Percent of total deaths was seen to increase for non-Hispanics by 5.83% compared to a decrease for Hispanic population by 0.74%. Finally, crude mortality rate increased across all groups with NC increasing by 4.72 deaths per 10,000, non-Hispanic populations increasing to with 2.33 deaths per 10,000 people After CC Intervention compared to 1.26 deaths per 10,000 people dying Before CC Intervention, and Hispanic populations with the greatest increase with 12.60 deaths per 10,000 people After CC Intervention compared to 6.82 deaths per 10,000 people dying Before CC Intervention. Showing that though fewer Hispanics died after being diagnosed with COVID-19, the number of Hispanics who died as a proportion of the Hispanic population increased.
Case Fatality & Mortality by Ethnic Group.
Source. Created with NC DHHS COVID-19 data and United States Census population data.
Analysis & Discussion
As has been seen by the disproportionate number of deaths of racial and ethnic minority individuals, CC Interventions that specifically target high-risk communities are essential to decrease the disproportionate impact on vulnerable communities (Schneider, 2013). In this study, the case fatality rates, mortality rates, and deaths per 10,000 by racial and ethnic population were compared across racial and ethnic groups and compared to the overall case fatality and mortality rates for the State of NC. Based on the results of the study, CC Interventions in the State of NC is associated with a decrease in the mortality rates of Multiple/Other communities, but an increase in mortality rates across other racial and ethnic groups. Additionally, CC Interventions are associated with decreased fatality rates across all racial groups but are associated with an increase in ethnically Hispanic communities. The findings support that after CC Interventions, the percentage of total COVID-19 deaths across all racial and ethnic groups decreases after the implementation of a CC Intervention. Though the percentage of White deaths as a total of all COVID-19 deaths increased, this is not to be associated with a racial disadvantage for White populations as CC Interventions for minority communities do not disadvantage racial and ethnic majority communities.
Limitations
Limitations of this study concern the transmission of COVID-19. In looking at the findings of this study, it may seem that CC interventions may have had little to no impact on fatality and mortality rates due to the increases seen across racial and ethnic groups. This is a reflection of the larger trends in COVID-19 transmission where individuals, religious groups, and others who have characteristics associated with a decreased likelihood to comply with health directives (men, lower levels of education, perception of lower risk, lack of government trust, and lack of moral obligation for compliance) (Leal et al., 2021, p. 524) or who violated stay-at-home orders. Though stay-at-home orders and phases were put in place by the Office of the Governor, the COVID-19 pandemic was plagued with legal challenges to his authority to issue such orders (Crumpler, 2021) and challenges with law enforcement (Brooks & Lopez, 2020). A misinterpretation of this study may lead the reader to believe that the increase in mortality rate for Non-Hispanic Whites compared to other racial groups might be indicative of CC solutions resulting in higher mortality rates among Non-Hispanic Whites. As Whites are less likely than other racial groups to be charged with violating stay-at-home orders (Michener et al., 2022), and less likely to have COVID-19 public health orders enforced on them while openly defying directives (Dunbar & Jones, 2021; Hopkins, 2022); further research is needed to examine the role of defiance of public health orders and COVID transmission, case fatality, and mortality rates by race and ethnicity. Additional limitations for this study included the death rates by racial and ethnic group and suppressed cases. Large groups such as Non-Hispanic Asian/Pacific Islander/Native Hawaiian and Non-Hispanic American Indian/Alaska Native serve to combine unique groups of individuals into singular racial categories. Further, designating individuals as Hispanic/Non-Hispanic complicates data analysis processes with the same individuals being categorized into different racial/ethnic groups. These limitations speak to the larger challenges of racial and ethnic designation for the United States Census and local public health reporting (U.S. Census Bureau, 2023b).
Conclusion
In conclusion, further research is needed on CC Interventions among racial and ethnic minority communities. There is vast amount of literature supporting the adoption and implementation of CC policies and CC Intervention practices (Groom et al. 2009; Hawai’i State Department of Health, 2021; Hussen et al., 2020; Hutchins et al., 2009; NAS, 2020; Quest Diagnostics, 2020; Schneider, 2013; Valdiserri & Holtgrave, 2020; Sadeghi & Wen, 2020), however, as has been seen during the COVID-19 pandemic leadership matters, race matters, and timely implementation matters. Despite the support of CC Interventions, implementing intervention strategies after communities have been ravaged by an infectious disease (NC DHHS, 2021a) is not a CC strategy, nor is it good leadership practices. During crises and pandemics, social vulnerability matters and unless public administrators embed equity in policies, programs, and practices in vulnerable communities, children and families will continue to experience healthcare disparities. As such, planning and implementation rather than interventions are essential to reducing inequities among vulnerable minority populations.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.