
Abstract
During the COVID-19 pandemic, many countries deployed armed forces to national health care facilities to handle an overwhelming patient flow. In contrast to previous domestic military deployments, the support missions lasted for almost two years in many countries. Most research on civil–military collaboration focuses on short-term partnerships and identifies challenges and opportunities of the common effort. However, little is known about the effects of prolonged civil–military cooperation (CMC) on the involved organizations. We conducted interviews with 34 participants who were involved in CMC during the COVID-19 pandemic in the Netherlands. The study reveals the existence of organizational interests apart from the common goal of coping with the patient flow, lack of clarity in the military’s position as last resort or first responder, and competing organizational priorities causing dilemmas. Clear prioritization of military tasks and transparency in expectations are key to ensuring that prolonged CMC remains beneficial and supported by both partners.
Introduction
Infectious disease outbreaks like the West African Ebola outbreak (2014–2015) and the COVID-19 pandemic (2020–2022) have proven to pose a major threat to public health, and showed that outbreak management requires multi-sectoral involvement. Armed forces, in particular, have been increasingly supporting civilian health agencies in their efforts to prevent and respond to these outbreaks (Clarke, 2020; Michaud et al., 2019). During the COVID-19 pandemic, military support was lasting for almost 2 years in many countries (Braun & Stelzner-Doğan, 2022; Ries, 2022). Although civil–military cooperation (CMC) is an important asset in support of outbreak management, it is also difficult due to various challenges such as cultural, organizational, and operational differences and unfamiliarity between military and civilian partners (Janse et al., 2022).
Many papers on civil–military cooperation in outbreak management concentrate on interorganizational interactions and their impact on reaching a common goal (see for an overview, Janse et al., 2022). They highlight, for instance, the importance of relationship management and the integration of civilian and military activities. Although insightful, there has been limited attention for the effects of civil–military collaboration on the internal dynamics of involved organizations and their personnel. This is surprising, because civil–military partnerships, particularly when long-lasting, demand considerable adaptation and commitment from involved organizations, reduce their autonomy, and can therefore be demanding too.
The current paper reports on empirical data on experiences of personnel involved in civil–military cooperation in a Dutch hospital during COVID-19, and emphasizes the impact of the collaboration on the internal processes in each organization. While the existing literature mostly takes an interorganizational perspective, we focus on how (intra-)organizational interests and concerns influence the way in which personnel view and act toward a collaboration partner. Thus, this article addresses the internal organizational implications of civil–military cooperation by answering the research question: how does long-term civil–military cooperation during an outbreak impact the intra-organizational dynamics of involved organizations?
It is important to learn more about these intra-organizational dynamics in civil–military collaboration because they are likely to become increasingly important. Armed forces and civilian partners increasingly need to engage in long-term partnerships in the face of a broad range of crises (Michaud et al., 2019; North Atlantic Treaty Organization [NATO], 2021). For instance, many NATO countries rely on civilian partners for logistics, IT, and health care support in preparation of a potential large scale conflict. Civilian organizations, in turn, require military support to handle increasingly disruptive disasters. The COVID-19 pandemic provides a recent example of a situation in which civilian and military partners committed to a partnership for a long period of time with major consequences for each organization’s priorities, activities, and interests. A better understanding of the individual organizational motivators and distractors for this kind of CMC helps to shape future planning and deployments.
In short, it is important to understand organizational barriers to civil–military partnerships, so we can better understand and potentially mitigate these obstacles to exploit the full potential of longer-term civil–military collaborations during crises and conflicts.
Theoretical Context
Over the past decades, the domestic role of armed forces has expanded significantly in countries across the globe (Clarke, 2016; Head & Mann, 2016; Kalkman, 2019). A series of terrorist attacks in the early 2000s led to a surge in domestic anti-terrorism deployments in various countries, while major disasters overwhelmed civilian response structures and required military support to regain control (e.g., Hurricane Katrina) (Banks, 2006; Bollen & Kalkman, 2022; Canyon et al., 2017; Samaan & Verneuil, 2009). The growing domestic role of armed forces is therefore partly a response to the increase in domestic threats and the rise of large-scale disasters that have become increasingly powerful as a result of climate change. But a growing domestic role has also served military interests, because these new domestic crisis response tasks boosted the legitimacy and public image of armed forces, which were facing waning interest and endless cutbacks after the end of the Cold War (Edmunds, 2006; Malešič, 2015).
For all domestic tasks of most armed forces, civil–military cooperation is of paramount importance: civilian authorities need to request military support in the first place, civilian partners typically remain in charge throughout the deployment of military personnel and capabilities, and effective civil–military interactions are needed for a coordinated response effort (Banks, 2006; Kapucu, 2011; Zijderveld & Kalkman, 2023). Scholars and practitioners use various terms and concepts when discussing civil–military cooperation, including civil–military interactions (CMI), Defense Support to Civilian Authorities (DSCA), and Civil–Military Operations (CMO) (Bakx et al., 2021; Horne & Boland, 2022). Here, we use the term civil–military cooperation to refer to any coordination and collective effort involving civilian (health) organizations and the armed forces in response to the COVID-19 pandemic, recognizing that these efforts were civilian-led (Horne & Boland, 2022).
Civil–military cooperation is a common phenomenon in non-domestic settings too. Military organizations, for instance, also coordinate activities with civilian partners in expeditionary contexts as a means to provide essential services or win hearts and minds (Keane & Wood, 2016; Rietjens, 2008). Existing civil–military efforts are typically characterized by their relatively short timeframes, they remain low-key, and involved organizations maintain a high degree of autonomy. In short-term international relief operations, military support is often seen as a last resort option. The principle of last resort originates from the United Nations Office for the Coordination of Humanitarian Affairs (UNOCHA) and means that (1) military means are unique capabilities for which there are no civilian alternatives; (2) they are available in time to meet an urgent demand; (3) they are controlled by civilians; and (4) deployment is temporary and limited in scale (Bollen & Kalkman, 2022; UNOCHA, 2015). The principle sets clear boundaries for international military in support of civilian organizations (Boland et al., 2021). It also aims to provide clarity in the allocation of tasks by putting activities under civilian responsibility, and it gives guidance on the management of the civil–military cooperation (Bollen & Kalkman, 2022; Metcalfe et al., 2012). Although the principle refers to international CMC, the principle of last resort aligns with many countries’ domestic military support regulations.
Yet, civil–military cooperation can also take a more permanent shape, for instance in case of strategic partner programs in long-term health security projects, such as collaborative research and surveillance projects on infectious diseases (Janse et al., 2022; Michaud et al., 2019; Sanchez et al., 2011). While CMC in crisis response is challenged by ad hoc situations and unfamiliarity among collaborative partners (Bollen, 2002), longer-term projects on CMC, like these, have the advantage that organizations can get to know each other well and prepare for collective activities. In turn, these partnerships have to deal with challenges such as long-term commitments (Gibbons et al., 2013; Morgan et al., 2003; Zottig et al., 2020) and binding agreements (DiGiovanni et al., 2005; Otto et al., 2011; Snyder, 2009). It can also be hampered by high (military) personnel turnover and limited enthusiasm among the workforce (Morgan et al., 2003; Morton Hamer et al., 2019). In any case, this type of civil–military collaboration will have a far bigger influence on the organization than the more open-ended, short-term partnerships in disasters and expeditionary settings.
The existing literature on CMC often highlights in particular what kind of activities were carried out by partners in the context of a specific collaborative project or deployment (Janse et al., 2022). This can also be recognized in papers related to military support in the COVID-19 pandemic response (e.g., Gad et al., 2021; Ries, 2022) or they focus on interorganizational dynamics and interactions (Gibson-Fall, 2021). But there are a lot of internal organizational decisions and considerations that are of relevance too. For instance, an organization needs to commit to the partnership in the first place, select a preferred partner, and might try to withdraw from the collective effort at any moment. In addition, the organizational interests might be at odds with the collective goals (Keane & Wood, 2016), such as when civil support missions interfere with military exercises. This discrepancy can grow increasingly problematic over time. Such intra-organizational factors provide the preconditions for civil–military collaboration, particularly in prolonged partnerships, but our knowledge of these factors is currently very limited.
Research Methods
We answer the research question using a qualitative research design focusing on the experiences of medical personnel involved in civil–military cooperation at the Dutch University Medical Center at Utrecht (UMCU) during the COVID-19 pandemic. UMCU is a tertiary medical center providing a highly specialized level of care. This study initially aimed to clarify how partners cooperated throughout the crisis and identify barriers and facilitators. Yet, we quickly realized that the interorganizational dynamics could not be fully understood without an understanding of the internal organizational views, debates, and actions.
This case study focuses on the support provided by the Ministry of Defense of the Netherlands to the UMCU on three separate occasions between April 2020 and January 2022. The first deployment (April–July 2020) consisted of 92 military personnel to UMCU, with more staff being deployed to other health care facilities as well. The second deployment consisted of military support to UMCU only, with 150 persons of military personnel on site (October 2020–June 2021). The Ministry of Defense made this support conditional on the demand that the hospital served as a national patient overflow capacity. Finally, there was a third deployment of 60 personnel from December 2021 until January 2022. For all three deployments, military personnel consisted mainly of nurses, but also included physicians and support staff.
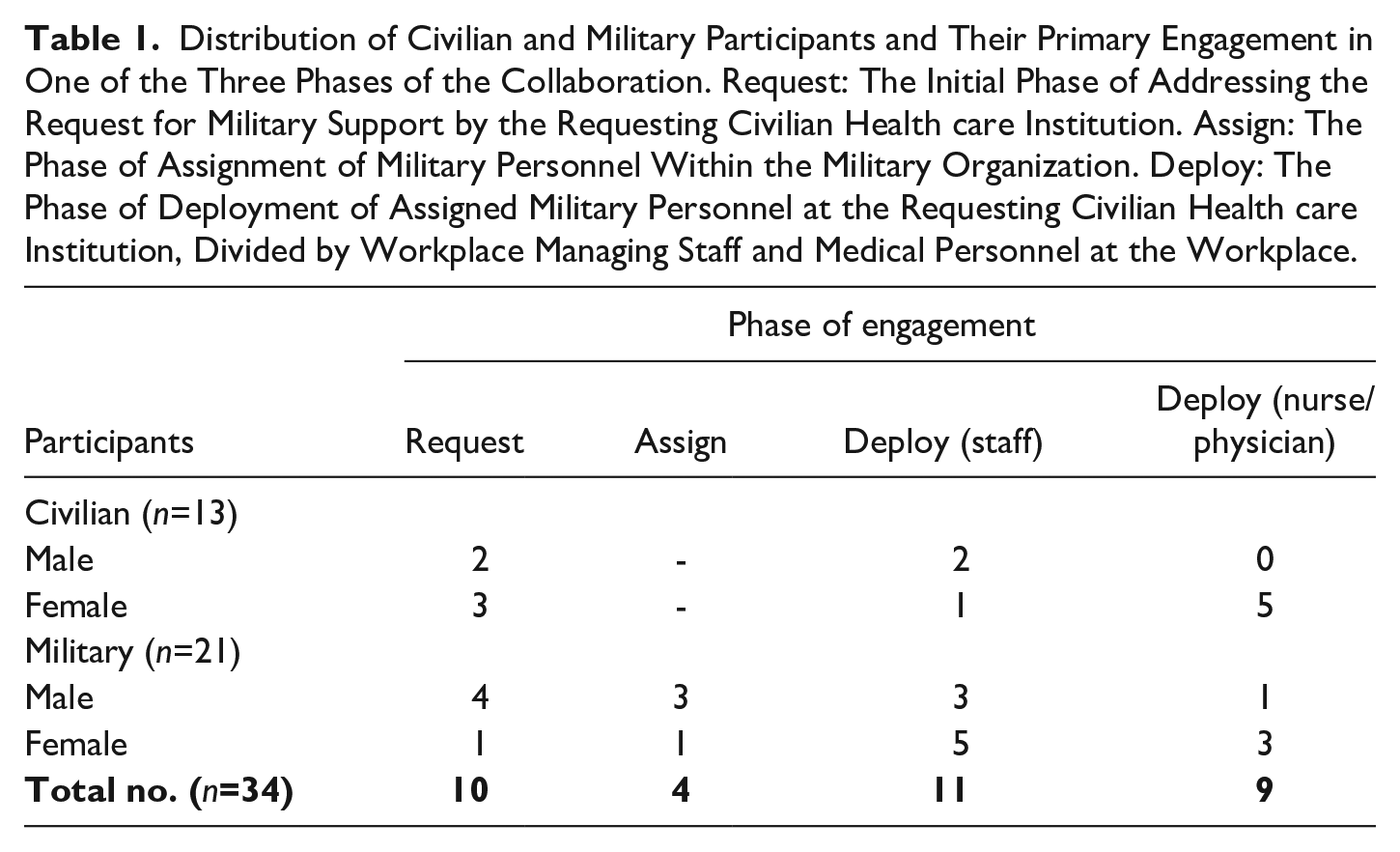
For each of the three deployments, the process of civil–military collaboration can be divided into three phases: (1) The initial request for military support by the requesting health care institution (i.e., strategic level), (2) Assignment of military personnel (i.e., tactical level), and (3) Deployment of military personnel at the requesting health care institution (i.e., operational level). The civilian and military research participants in this study represented the full cycle of phases and were involved in handling the request of military support, taking part in assigning military personnel or were working at the workplace of the requesting hospital.
For this empirical research, semi-structured, face-to-face interviews with a mean duration of 90 minutes were carried out with military and civilian personnel. Recruitment was done by snowball sampling, starting with key military actors involved in the collaboration. They were asked to recommend civilian counterparts or other relevant civilian or military personnel involved. Inclusion of participants proceeded until saturation was reached, defined by referring to identical key players and to the moment that no new insights emerged from the interviews. Prior to the data collection, all participants received an information brochure and signed an informed consent form. An ethical review and approval was obtained from the Research Ethics Review Committee Faculty of Science of the VU University Amsterdam (BETCHIE 2022.038). After a pilot interview in September 2021, data were collected between May and December 2022. Table 1 offers an overview of civilian and military participants and the phase of their primary engagement during the collaboration.
Distribution of Civilian and Military Participants and Their Primary Engagement in One of the Three Phases of the Collaboration. Request: The Initial Phase of Addressing the Request for Military Support by the Requesting Civilian Health care Institution. Assign: The Phase of Assignment of Military Personnel Within the Military Organization. Deploy: The Phase of Deployment of Assigned Military Personnel at the Requesting Civilian Health care Institution, Divided by Workplace Managing Staff and Medical Personnel at the Workplace.
Data were coded and analyzed according to the guidelines of abductive thematic analysis method (Thompson, 2022). The ATLAS.ti 23.3.4 program was used to assist in the coding process. The first author performed the coding of data in close consultation with the second author.
Results
Saturation was reached after interviews with 34 participants. During the coding process, themes related to the intra-organizational consequences of collaboration emerged from the data, resulting in three main themes: (1) reasons for civil–military collaboration, (2) organizational interests at stake during the long-term collaboration, and (3) the military’s position in the collaboration.
Reasons for Civil–Military Collaboration
Benefits of Cooperation
Most study participants acknowledge that both organizations benefited from the collaboration. UMCU relied on the cooperation when it urgently needed external support to cope with the crisis situation, while the military had the ability to provide medical personnel on a short notice, which also improved the public image of the armed forces. For military personnel, involvement in the UMCU provided valuable working experience and contributed to the development of their (clinical) skills: We have many young and new staff who have now gained experience in their own positions that they would otherwise never have gained. [R25-mil-deploy/staff]
It was also acknowledged by most interviewees on strategic level and also some at operational staff level that the COVID-19 collaboration enabled further cooperation and strengthened their resolve to formalize commitments for future joint activities. The Ministry of Defense now benefits from this partnership by the consolidation of new in-hospital training opportunities, while UMCU officially partnered with Defense as one of the 14 partnering hospitals (IDR) to expand its activities toward military medicine: I think the collaboration during COVID has accelerated and strengthened a lot. [R14-civ-request]
Developing Doubts on the Distribution of Benefits
Mainly military respondents throughout strategic, tactical, and operational levels had their doubts if the effects of the collaboration were proportional beneficial for UMCU. The longer the collaboration lasted, the higher the degree of unease that was reported by these military respondents, but this was also recognized by a few civilian colleagues. For some, including an UMCU participant, the decision of UMCU to cooperate with the armed forces for extra personnel was perceived as a low-cost opportunity for UMCU: We [UMCU] have benefited from that. Considerable financial benefit. If we should have hired people, regardless of where they would have come from. Or we should have spent money to have the part-timers work extra, or bonuses, or-. Now Defense has simply solved a very large personnel problem. [. . .]. The policy level was very happy with that of course. [R10-civ-deploy/staff]
This also raised the question on military tactical and strategic level if military support in the long term created false competition by disrupting the health care market at a moment on which there were possibly other options to scale up personnel capacity: My other concern was: Defense is only there to absorb the initial blow, and after that, the institution has to take care of itself. [. . .] that’s just the non-compete clause for the initial emergency response. We’re there when there are real shortages, but once that’s resolved, despite the fact that there are still concerns. [R11-mil-request]
However, this sentiment related to the risk of financial exploitation was not recognized by all: No, there is no competition. Because we did that already from a military tasking related to one of our core responsibilities. So in other words, there is not really any state aid. So there is also no Defense personnel deployed for elective care. [R33-mil-request] We’ve always been very mindful of whether there’s a much higher return on this than what we’d normally do. That’s obviously not the case, because there’s also significantly less return on the care we’re not providing, because we were actually doing more than our fair share. So we did look into that, and we do monitor ourselves to see if there might accidentally be a positive business case for us. Because, of course, we simply didn’t want that from a societal perspective. [R18-civ-request]
Among study participants there was also a perception that apart from the common goal to cope with the patient flow, other organizational interests led UMCU to choose for civil–military collaboration too. A substantial part of mainly military respondents were increasingly convinced that, besides a strict financial advantage, deployed military personnel were used to solve a more common and already existing organizational problem of shortage of civilian medical personnel, rather than an acute problem, and an easy way to get extra personnel into the hospital. This observation was also made by an UMCU participant: But in practice, everyone could manage it in their own region, but we still had support from Defense. So that did indeed give a bit of the feeling of, is that actually still for the country or is that for the UMCU? I can remember those conversations well, yes. At a certain point, it is also a bit over. And certainly in the departments, I think, you are just supporting care. Not solving the crisis. [R29-civ-deploy/nurse_physician]
Organizational Interests at Stake in Long-Term Collaboration
Competing Priorities
During the ongoing collaboration, tension arose regarding competing organizational priorities. Initially, COVID-19 overwhelmed the hospital capacity, for which military support was brought in. UMCU agreed to the condition that the hospital would function as a national overflow capacity, which justified the extra military support to this hospital. It was also agreed that there would be no upscaling of regular care as long as military personnel was deployed at the hospital. At the same time, the military adhered to the agreement that the support would be available as long the numbers of COVID-patients were above a certain threshold. Over time, the situation became more manageable, but military support was still needed, because the hospital was not yet able to manage the situation without support. In fact, because of the remaining military support, referral of patients to the UMCU continued, maintaining its pressure on the hospital organization. While other hospitals started to upscale their regular care, UMCU was not able to do so because of the military presence at their hospital. The hospital was caught between conflicting types of interests. Despite the felt urgency to restart delayed medical care and a financial incentive to start treating regular patients, it was held back by an operational imperative to maintain military assistance: And you gradually noticed, at a certain point it decreased again, that need for a national overflow capacity. But of course, we were still there. [. . .] I know that it really hurt a lot, those operating rooms down [in numbers]. Operations on children were cancelled, there were people sitting at that table of the senior management in the morning just crying about how distressing it was. And all hospitals in the region had that scaling down. And when the rest started scaling up again, the UMCU waited with that, because they had to do the national overflow. I also kept saying: pay attention, guys, keep doing that national overflow, because we are gone from here, this is the only justification for us being here. So if you wanted to stop that national overflow, that is not possible. Yes, that is possible, but then we are gone with those 150 people. [R12-mil-deploy/staff]
At the same time, the military faced its own competing priorities. At the beginning of the pandemic, military personnel was available, but military activities, such as training exercises and deployments, restarted over time. Medical personnel was needed for these military operational activities and military readiness was expected for international military commitments. The additional tasks of COVID-19 support caused a competition of priorities. Several military respondents stated that the COVID-19 support harmed the military operational readiness status and was felt long after the completion of the collaboration: These are the same people who have been appointed to the VJTF [NATO commitment], which means that, when deployed, they lack the necessary knowledge to properly support their comrades in the forward area or to provide the care they deserve. So that long deployment has really been fatal for the ability and deployability of this unit. [R15-mil-deploy/staff]
However, some military interviewees also acknowledged that COVID-19 stretched the already existing challenges of military units due to years of financial cutbacks and reorganizations. Nevertheless, it shows that both organizations struggled with internal challenges as a result of the collaboration.
Integration-Distance Paradox
Another effect of long-term collaboration was managers’ fear that lower-level personnel at the workplace would overly identify with the collaboration partner. This could be a result of “too much integration” over time. This fear was particularly perceived at the military assigning level. There were concerns that, after a long period of collaboration, military personnel at UMCU felt responsible for the (negative) consequences when the decision was made to end the collaboration and leave the hospital. They worried that personnel would question the military decision and hinder a decisive exit. This concern was mainly countered by rotation of personnel, so personnel would be deployed for shorter periods of time. High rotation means that personnel had less chance to get fully acquainted with civilian partners and get attached to the collaboration. This policy was not explained by senior military decision-makers and therefore not understood at the workplace, where it caused frustration at the civilian side of the collaboration: What you also see, is that your own staff, if you are somewhere for more than four weeks, then you also start to have an opinion about it. For more than two months, then you really start to get into the swing of things and after three months, your own coffee mug is in the department. And you just participate fully. And who do you work for here then? So yes, that took way too long. [. . .] And it’s not just at the decision-making level: OK, we’ll wait a bit. It’s also at the executive level that people are so involved and don’t want to get out of it either. [R28-mil-assign]
Moreover, a military manager explained that the military “is there to help, not to rescue” [R1-mil-assign]. This reflects some degree of conscious distance toward the collaboration and civilian concerns. The military, from this perspective, would not just blindly deliver what was asked for, but would deliver based on what problem needed to be solved and what the military had to offer in response, regardless of the initial request.
The Position of the Armed Forces in the Collaboration
Military Support as a Last Resort
At the start of the crisis, the military was considered to be the only possible option to support the overwhelmed health care system (last resort). Because most military operational activities were canceled, a relatively large, well-trained source of medical skilled personnel became available on short notice: And the advantage is that you [Defense] have trained healthcare personnel that are available, from that availability function. I think that is different from other places in the country, you don’t just have that. So you do have a contingent of professionals that can be deployed more freely than all kinds of other constructions that you had. [R18-civ-request]
But at the same time, mostly military respondents on tactical and operational level did question if the military was the only available and possible option. But even at strategic level, a military manager suggested that a request for military support was too much a default option: Yes, you know, and that is also, a lot of unfamiliarity with other options that are there. But the first default response is: Defense. [R11-mil-request]
As the pandemic continued, the opinion grew that continuation of the collaboration was a result of path-dependency and previous success, rather than the military still being a last resort and the only available option: But yes, what did you do yourselves to arrange it in the meantime? There were some options, VWS [Ministry of Health] volunteers for example. But for the rest, yes ok: if it happens then we [UMCU] press [the button] and they [Defense] will come. Because that is what they [UMCU] were used to. [R28-mil-assign]
Positioning, Priorities and Expectations
Among the military interviewees, there were different opinions on how the military should position itself in the face of this kind of collaboration. Most military respondents adhered to the concept of last resort for military involvement, although this principle was questioned by study participants throughout the collaboration at UMCU. Respondents also stated that this concept of last resort is not necessarily in conflict with a position of a strategic partner: So you can sit and wait until you are the last resort, but then you are surprised, while otherwise you can be very prepared in where you intervene, or do not intervene, [. . .]. So I think that certainly at a strategic level, perhaps also at a high tactical level, you have to have those contacts very closely. And that you perhaps have a staff element that can contribute interdepartmentally. But I think it is different when you deploy [military] units for two years to do the execution. [R15-mil-deploy/staff]
Military respondents reflected also on the task of domestic support to civil authorities and the risk of competition with the two other military core responsibilities: (1) to protect national and allied territory, and (2) protection of the international rule of law. As emphasized by respondents from the request, assign, and deployment phase, it is a necessity for the military to be a strategic partner for civilian authorities in times of crisis. It should be able to deliver support as part of statutory obligations, at the request of civilian authorities. However, at the start of the pandemic, military resources were available due to downscaling of regular military activities. But what if this was not the case? A few respondents stated that expectations should be managed among civilian partners regarding the availability of military assets. Partners should always take into account that the military can also be deployed in the interest of these other core responsibilities. This means that in case of a next health crisis, military support might not be guaranteed: With the size of our armed forces and what is happening in the world, we have to be able to do all three tasks at the same time. And the situation at that moment requires where the priority lies. Where in the pandemic, when there was no Ukraine yet, we also looked at whether we should consider stopping the other missions, to provide national support. But for example, if a pandemic breaks out again now, with no doubts we would ever think of immediately withdrawing that entire eastern flank again. [R11-mil-request]
Finally, both partners acknowledged the military’s added value in crisis support. But while the hospital was in urgent need of clinical support, the military regularly stated their expertise in crisis management, not primarily on COVID-19-related clinical skills. This reveals a difference in perspectives between the two partners concerning the perceived military’s optimal added value in this crisis collaboration: You just notice that we as military personnel [. . .], we would do this so much more straightforward and clear and faster. That’s how we were raised. So that makes sense. [R12-mil-deploy/staff]
Occasionally, some discrepancy emerged between the expectations on the partnership. These did not escalate into a conflict between both sides, but the results of this study do show how important intra-organizational dynamics are for the stability and effectiveness of the interorganizational, civil–military collaboration.
Discussion
This study focused on the internal organizational implications of civil–military cooperation in the exceptional circumstances of the COVID-19 pandemic. It shows that the COVID-19 crisis required long-term commitment from civilian and military partners, despite evolving competing priorities and the existence of distinct organizational interests without the proper conditions to adapt to the characteristics of a well planned long-term project while the crisis continued. Most recent studies on CMC focus on short-term domestic crises or long-term expeditionary civil–military cooperation, both of which present different dynamics. Domestic crisis situations often result in ad hoc collaborations with limited preparation time (Bollen, 2002), while expeditionary collaborations result in long-term partnerships but organizations maintain much autonomy (Bollen, 2002; Rietjens, 2008). Characteristics of both situations merged throughout the civil–military COVID-19 response. This combination was a new, unprecedented situation in which both organizations had to find their way. This is an important finding, which can be of relevance in other situations, which might require long-term civil–military collaboration. This might be the case with crises arising from climate change-related disruptions or as a result of changing geopolitical dynamics. In this section, we will elaborate on the main findings of our case.
Benefits and Interests in Civil–Military Partnerships
Beside the common goal of coping with the overwhelming patient flow, other benefits and interests can play a role in short- and long-term collaborations. The common benefit of expanding future training opportunities for both hospital and military personnel improves and expands clinical experience, which is critical for medical personnel (Haverkamp et al., 2022). In addition, partners benefit from the collaboration by learning from one another, such as UMCU having better access to expertise on military medicine and available knowledge on military trauma care after the COVID-19 collaboration (UMCU, 2024). For armed forces, the collaboration was also in the military’s interest by contributing to a positive image for the armed forces, which shows the organization’s efficiency and importance to society and potentially boosts recruitment campaigns (Kalkman, 2021). Positive media attention can also support counter-arguments for budget cuts (Erickson et al., 2023).
Nevertheless, the results also show that collaborative partners weigh the distribution of organizational benefits, maybe even more explicit during long-term collaborations. When crisis support is perceived to be possibly disproportional beneficial for the other partner, there may be ground for declining trust and motivation, which can undermine effective collaborations (Bollen, 2002). Therefore, it is important to be transparent about mutual goals, and existing benefits by collectively reconsidering the necessity of the partnership at intervals.
Organizational Impact
Competing Priorities
This study shows that long-term collaboration took its toll on both collaborative partners. The military medical unit compromised on military readiness. The disadvantage in the state of operational readiness was clearly felt when, shortly after the COVID-crisis, a full-scale Russian invasion of Ukraine led to a war on the European continent and required international military commitments. For UMCU, the dilemma emerged at the moment it was not able to restart regular care, because of the military presence at the hospital. This caused frustration because of the delays in diagnoses and treatment, next to financial concerns. Even more because of UMCU’s highly specialized hospital care, which could not be taken over fully by local general hospitals. Furthermore, the financial concerns derive from the funding model of the Dutch health care system, which is built on marketization and financial arrangements with insurance companies, meaning that hospitals have targets to meet to receive full funding. European countries like Norway, Sweden, or Denmark have a much more centralized governmental funding model for health care, funded for over 80% by the national governments (Van Polanen Petel, 2022). This finance model might overcome the competitive incentives and financial concerns in times of crisis. Both dilemmas show that long-term collaboration does not necessarily become easier over time, as it can also come with a price for the organization itself and dilemmas might arise due to the long timeframe of collaboration. It is therefore important to regularly organize a re-evaluation of the settled agreements. This action should be added to the standing working arrangements to reserve space for flexibility within the collaboration and with the mutual acknowledgment and respect toward the organizational interests at stake.
When going deeper into the competing priorities of the military, it is important to keep in mind that armed forces have multiple tasks. The COVID-support was an urgent deployment in support of civilian authorities in times of crisis. However, military training and preparedness for more conventional military activities, to meet international readiness standards, is often seen as the most important role of the armed forces, even if there is no actual deployment (yet) (Kalkman, 2021). It helps to get a clearer idea of military priorities to be able to assess whether or not to accept the consequences of long-term domestic military deployments. It is even more important to get military priorities straight in this current time-frame of a shifting military focus toward warfighting in response to geopolitical changes at the borders of NATO territory. Moreover, it seems that the limited military resources are planned for dual use in two major international challenges. On one hand, global organizations call for pandemic response plans in which the military is expected to play a role (World Health Organization [WHO], 2021, 2024) and on the other hand, NATO leadership is asking allied countries to prepare for war (NATO, 2025). If military assets are a multi-use instrument, with deployments based on situational circumstances, it can be debated if and how the military can be a strategic partner for domestic crisis relief. A reliable strategic partner must be able to comply with binding agreements (Janse et al., 2022). At the same time, the military must be able to respond to different national and international unknown threats, dealing with limited available resources (Erickson et al., 2023). Prioritizing activities will be inevitable, while at the same time priorities can be revised quickly by situational changes. For the armed forces, this may complicate the adherence to binding civil–military commitments and agreements. From the point of view of civilian partners, this uncertainty in military commitment may be perceived as unpredictability of a partner, and might have implications toward their trust in the collaboration. Prioritizing military activities is a political consideration of the national government though. For successful collaboration in any civil–military activity, it is essential to make clear decisions on military priorities and specify limitations so both sides to the partnership know what to expect and can prepare accordingly.
Fear of “Too Much Integration”
While considerable civil–military differences are typically a challenge to crisis response collaboration in short-term, domestic deployments (Banks, 2006; Kalkman, 2019), there is a “risk” of too much integration in long-term partnerships. Our study shows that military planners at tactical level actively countered military personnel’s integration during the Dutch response to the COVID-19 outbreak. It adopted measures and policies to prevent the full social incorporation of military personnel in the civilian medical institution that it was supporting during the various COVID-19 waves. This surprising finding seems contrary to established ideas of collaboration. There is general consensus among scholars that successful civil–military cooperation requires integration. Civilian and military partners need to integrate functionally and socially to boost performance. This explains why researchers emphasize long-term stakeholder commitments and low personnel turnover (Forestier et al., 2016; Morgan et al., 2003; Morton Hamer et al., 2019; Wignjadiputro et al., 2020; Zottig et al., 2020). Such measures might help to bridge organizational prejudices and build trust between civilian workers and military personnel (Johns & Blazes, 2010). Vice versa, mutual unfamiliarity and short-term interventions breed distrust and hamper integration (Gibson-Fall, 2021). Ultimately, integration facilitates the exchange of knowledge, data, and expertise between civilian and military partners, thereby leading to improved coordination of activities and better results (Ma et al., 2016; McGee & Michael, 2020; Sanchez et al., 2011). But this perspective on integration shows a focus on interorganizational level of analysis, while it neglects the interests at stake for the individual organization within the collaboration, such as the military’s desire to maintain control over their own personnel and the perceived risk that military personnel might care more about civilian than about military concerns over time. Here, the hospital needed the military, not necessarily the other way around.
This shows the nature of the interdependency and also affected the balance of power within the collaboration. Successful interorganizational collaboration needs interdependency between participating organizations, and these participating organizations must be aware of this interdependency. They are aware that they cannot obtain their own goals without each other (Bollen, 2002). During the COVID-support, the military could have walked away out of the collaboration with less practical organizational harm than it would have given to the hospital. This might explain the decision to keep a level of control over personnel by making a decision that did not necessarily benefit the collaboration. Even more, the military could afford to make this decision, which might not be the case if the dependence is the other way around.
For instance, the current geopolitical tensions in Eastern Europe might develop into a conflict situation in which the military health care system cannot cope on its own. In that case, the military will be dependent on the national civilian health care system. Moreover, reserve personnel with a regular civilian job will be incorporated into the military organization, probably for a long period of time. Based on this study, it is important that military planners consider the interests of their civilian partners (e.g., hospitals) to ensure that diverging interests or dissatisfaction does not adversely affect the civil–military cooperation. From an alternative point of view, the civilian and military workforce can be seen as one large strategic resource of health care workers, that can be allocated flexibly depending on the (crisis) situation at hand. In fact, this may become necessary in case of an international conflict with overwhelming numbers of (military) patients.
Positioning of the Military in (Domestic) Crises
Last Resort or First Responder
The concept of last resort often refers to the use of foreign military assistance (FMA) (UNOCHA, 2012). Nevertheless, the principle of last resort aligns with many countries’ domestic military support regulations. But the principle of last resort may not necessarily apply in a long-term domestic deployment, such as a public health emergency. The principle also initially applied to the national military deployment during COVID-19 in the Netherlands, although this positioning of last resort was challenged by some. The latter group of respondents perceived that the choice to call in the military was based on successful preceding deployments in national crises. This trend has also been identified in previous studies (Kalkman, 2019; Ratchev & Tagarev, 2018), but problematically, it can blur the line and increasingly render military deployment a quick fix for a broad range of societal challenges (Kapucu, 2011). It can be debated if the military support during the COVID-19 pandemic fitted the principles of last resort, or instead made the armed forces a first responder. Indeed, during COVID-19 pandemic, many national military armed forces acted as first responders rather than last resort (Boland et al., 2023; Erickson et al., 2023). Distinction between the two different approaches is important and has organizational consequences. A first responder organization has to be prepared for this formal task of short-notice deployments with little time for preparations in an emerging crisis. This demands pre-crisis arrangements, such as those described at the WHO guidance document for a national civil–military health collaboration framework. It entails the establishment of multisector strategic partnerships, acknowledgment of differences between the public health and military health services, identification of technical areas for health emergency preparedness collaboration, institutionalization of national civil–military health collaboration for preparedness and jointly building of capacities and training for health emergency preparedness (WHO, 2021). A last resort organization can uphold an approach of less involvement in a preparedness phase of collaboration. It can bring in resources as they are available on that given moment when all else has failed. In such a situation, the military can hold on to the principle that it can decide on the spot for what it can do in that given situation. This strategy is much more ad hoc-oriented. However, even this latter strategy can be explicated and included in national preparedness plans to manage expectations. Meanwhile, global health organizations call for the development of preparedness plans for the next pandemic (WHO, March 2024). At the same time scholars predict that in future (health) crises, national military assets will be deployed as a first responder more often (Boland et al., 2023; Erickson et al., 2023). A choice between strategies related to last resort or first responder asks for a political decision on military positioning on which the military and civilian crisis organizations can design their plans.
Limitations and Future Research
This study follows the call for further research on CMC in the pandemic response to strengthen the lessons learned process on domestic CMC (e.g., Boland et al., 2023; Erickson et al., 2023; Gad et al., 2021). Some limitations must be considered. First, this study shows organizational-level conclusions based on data from a diverse sample population. The inclusion of more respondents on the strategic level, including those involved in policy-making, might have added more insights into the organizational interests at stake. Second, only one hospital was included in this study. While the UMCU was the primary site of CMC during COVID-19 in the Netherlands, collaboration dynamics and intra-organizational implications may have manifested differently in other hospitals. For these reasons, we recommend for further research to focus more explicitly on representatives from the policy-making level and include more CMC locations to compare different cases.
This empirical qualitative study contributes to academic knowledge on processes and dynamics within organizations involved in domestic CMC. While future crisis will be different and every country has its unique characteristics, this study identifies potential organizational barriers to civil–military collaboration that need to be considered within CMC preparedness plans. To advance the concept of CMC and facilitate the implementation of long-term CMC in crisis preparedness and response, a comprehensive research agenda is needed, for example on strategies to cope with emerging dilemmas in a prolonged domestic crisis and organizational interests that are at stake, but also on the development of a framework to prioritize involvement in times of limited military resources and an increasing (and competing) international demand.
Conclusion
In conclusion, this study shows organizational implications of long-term domestic CMC during the COVID-19 pandemic. In an attempt to cope with the unexpected patient flow, which overwhelmed health care facilities, civilian and military personnel did the utmost to reach the common goal of providing adequate care to the patients. Nevertheless, lessons can be learned for future long-term partnerships. During a prolonged collaborative crisis response, there must be room for re-evaluation of standing agreements with respect to shifting interests and emerging dilemmas from all organizations involved. Moreover, it is important to acknowledge that organizations involved may have their own interests to collaborate. This may cause some friction among partners, but when well-managed, can result in improved relationships and ongoing joint ventures. Defining the position of the military organization as a last resort or as a first responder within CMC is important to draw realistic preparedness plans for the future. Especially when military assets are considered as a multi-use instrument in times of new pandemic threats and geopolitical instability.
Footnotes
Acknowledgements
We sincerely thank all study participants for their availability and provision of valuable information. We also want to show our deepest gratitude to prof. dr. Myriame Bollen. Unfortunately, she passed away during the research process, but we will keep her inspiring energy close.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosures
JJ and JPK prepared this work within the scope of their employment with the Dutch Ministry of Defense. AT was employed by the LCI of the National Institute for Public Health and the Environment, which is part of the Ministry of Health, the initial part of the study—until February 2022—fell partly under the scope of the employment.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Jacobine Janse, MD, Lieutenant-Colonel is a PhD candidate and active-duty service member of the Dutch Ministry of Defense, which financially supported the PhD project.
Data Availability
Individual participant data will not be available to others. Due the impossibility of full anonymization of interview data, these are not publicly available. Interested researchers can submit a proposal for access to de-identified data by sending a request to the corresponding author at