
Abstract
A recent scoping review indicated military-connected children face stressors that may increase mental health issues. However, the majority of the included literature was American. To examine the experiences of Canadian military-connected children, we conducted in-depth interviews with a purposive sample of Canadian military-connected youth using a qualitative description approach. We conducted a content analysis on interview data, supported by qualitative data analysis software (MAXQDA), with coding done by two researchers who met regularly to discuss coding agreement. Thirteen children in military families participated and described the mental health impact of frequent mobility, parental absence, and risk of parental injury. The experiences of our participants were consistent with the results of an earlier scoping review on this topic. Our results suggest improving military cultural competence among health care providers and enhancing parental support may positively impact child well-being. More research is needed to understand resilience and vulnerability among Canadian military-connected children.
Keywords
Background
Persistent stress within the family system can increase the risk of mental health problems (De Girolamo et al., 2012). Families may experience persistent stress for many reasons; for military families, frequent relocation, parental absence, and risk of parental injury create a unique trio of persistent stressors (Daigle, 2013). These stressors, which are inherent in the military lifestyle, differentiate military families from their civilian counterparts and may put military-connected children at risk for mental health problems (Daigle, 2013).
The unique stressors of the military lifestyle and their associated risks warrant examination of the mental health issues and needs of military-connected children and were the focus of a recent scoping review conducted by Cramm, McColl, et al., 2019. Two primary themes emerged from their synthesis of the literature. First, children in military families seem to have more mental health issues than those in civilian families. Second, parental absence, frequent relocation, and risk of parental injury can impact the mental health of military-connected children across the developmental span. Parental absence emerged as the most negative element of the three across all developmental stages (Alfano et al., 2016; Gorman et al., 2010) while frequent relocation was most challenging for adolescents and children with special health needs (e.g., autism spectrum disorder) (Davis and Finke, 2015; Davis et al., 2016). There were few studies targeting the risk associated with parental injury in Cramm, McColl, et al.’s (2019) scoping review, but included studies indicate that the mental health challenges of parents can negatively impact child mental health. Primary research published after the 2016 cut-off date for Cramm, McColl, et al.’s (2019) scoping review shows these three trends continuing (Cramm, Smith et al., 2019; DeVoe et al., 2018; Nicosia et al., 2017; Ostler et al., 2018; Thandi et al., 2017). While research interest in military families has increased in recent years, the majority of the peer-reviewed literature has been conducted in the United States of America (USA) (Cramm, McColl, et al., 2019; Cramm et al., 2015; Cramm et al., 2016; Cramm et al., 2018). Indeed, 86% of the articles included in Cramm, McColl et al.’s (2019) review were conducted in the United States and only 3% in Canada.
Although military lifestyle factors and their associated risks may be shared across these two nations, the military contexts are different. The U.S. military is proportionately larger than Canada’s, 0.40% (1.3 million) versus 0.18% (66 000) of the total population of each country, respectively (Manser, 2018c; Military OneSource, 2018c). Furthermore, operational tempo is more intense in the United States, with a substantially greater proportion of the total U.S. population (0.73%) deployed to an operational tour since 2001 compared with the same timeframe in Canada (0.11%) (Verlezza, 2015). Both Canadian and American military families relocate 3 to 4 times more often than civilian families (Daigle, 2013; Drummet et al., 2003); however, American military members tend to deploy more frequently and for longer (Cramm, McColl, et al., 2019). Canada has a larger proportion of military members with spouses and/or dependents compared with the United States – 64% versus 52.3%, respectively (Manser, 2018c; Military OneSource, 2018c).
The infrastructure and systems in place to support military families also differ across the United States and Canada. Canadian military families, unlike their American counterparts, must access civilian health services administered by each province/territory rather than continuity in access that American military families experience through the federal health system designed for the U.S. military and their families (Cramm, McColl, et al., 2019). Canadian military families have voiced concerns regarding health care access in the context of mandatory relocation (Manser, 2018b) and Mahar et al. (2018) reported greater time to first contact with the health system among Canadian military families compared with civilian families. This is particularly problematic for Canadian military families whose children have special health needs (Cramm, Smith, et al., 2019). These differences in national contexts raise questions about the extent to which American-based research can be generalized to the experiences of military families elsewhere.
While military families have increasingly become a research priority in Canada (Cramm et al., 2016; Cramm et al., 2015), primary research on Canadian military-connected children is still limited in volume and consists largely of gray literature. The available gray literature appears to be consistent with the results of the scoping review, indicating difficulty with parental absence (Harrison & Albanese, 2012; Skomorovsky & Dursun, 2013; Skomorovsky et al., 2016; Sudom, 2010) and frequent relocation (Manser, 2018c; Perreault et al., 2020; Skomorovsky, 2013). No Canadian studies have explicitly investigated the broad mental health issues and needs associated with growing up in a military family from the perspective of the children themselves. The potential mental health implications of military life stressors and the historic lack of peer-reviewed research specifically on the Canadian population makes this an important area to explore.
The purpose of this article is twofold. First, we sought to answer the research question: What are the mental health issues and needs of children growing up in a Canadian military family from the perspective of the children themselves? Second, based on the answer to this research question, we sought to evaluate whether the experiences of Canadian military-connected children were consistent with the scoping review by Cramm, McColl, et al. (2019), specifically in relation to the second theme which dealt with the implications of specific military stressors. The results section of this article addresses the research question noted above while the discussion, in part, compares the results of this study with those of the scoping review.
Method
We chose a qualitative design because this methodology is well suited for shedding light on understudied phenomena. We used Sandelowski’s (2000) qualitative description approach because it is well suited to examining the “who, what, and where of events” (p. 339) and can facilitate an understanding of particular phenomenon while maintaining flexibility in interpretation that is not possible in other qualitative methods (Sandelowski, 2000, 2010). This method offers “a comprehensive summary of an event in the everyday terms of those events” (Sandelowski, 2000, p. 336) and allowed us to effectively address our research question and describe participants’ experiences relative to the scoping review findings and the resonance of those findings within the Canadian context.
Qualitative methodologies are meant to obtain an in-depth and nuanced understanding of a particular phenomenon by collecting rich data and thick description from people who have experienced that phenomenon (Holloway & Galvin, 2017). Qualitative research is not meant to determine causality among variables or generalize findings to broader population in the way some quantitative research is meant to do (Polit & Beck, 2017). Therefore, the results presented in this paper pertain specifically to the participants we interviewed and are not necessarily representative of all Canadian children growing up in military families.
Canadian children between 7 and 18 years old with at least one parent serving in the Canadian Armed Forces (CAF) were eligible to participate. We used purposive sampling to obtain a variety of perspectives based on age and parents’ military service. While there is no specific recommendation for sample size in qualitative description (Sandelowski, 2000), our sample size (13) in consistent with purposive sampling geared toward understanding a particular phenomenon (Creswell, 2014; Holloway & Galvin, 2017; Sandelowski, 1995). Data collection was halted once no new insights on the research purpose were gleaned with subsequent interviews (i.e., data saturation was reached). Recruitment involved poster distribution to community organizations (e.g., YMCA), advertising on social media, and in the Canadian Military Family Magazine, and word of mouth.
Informed consent and/or assent was obtained by all participants in this study. While the age of majority in Canada is 18–19 years (depending on the province), there is no specified age of consent for research participation (TCPS, 2018) or health treatment (Coughlin, 2018). Rather, researchers are required to determine the participants’ capacity to provide informed consent regardless of age. In accordance with these guidelines, we elected to collect signed informed consent from the parents as well as signed informed assent from children under age 16. For children between 16 and 18 years, we consulted with the parent(s) but only required signed informed consent from the child. We chose 16 years because this is consistent with the age most provinces or the federal government presume one has capacity to make decisions regarding health care (Coughlin, 2018). In addition, we evaluated the capacity to provide consent/assent among all participants. In addition to written informed consent/assent, we also ensured ongoing consent verbally at the beginning of each interview and advised all participants of their right to withdraw from the study at any point for any reason.
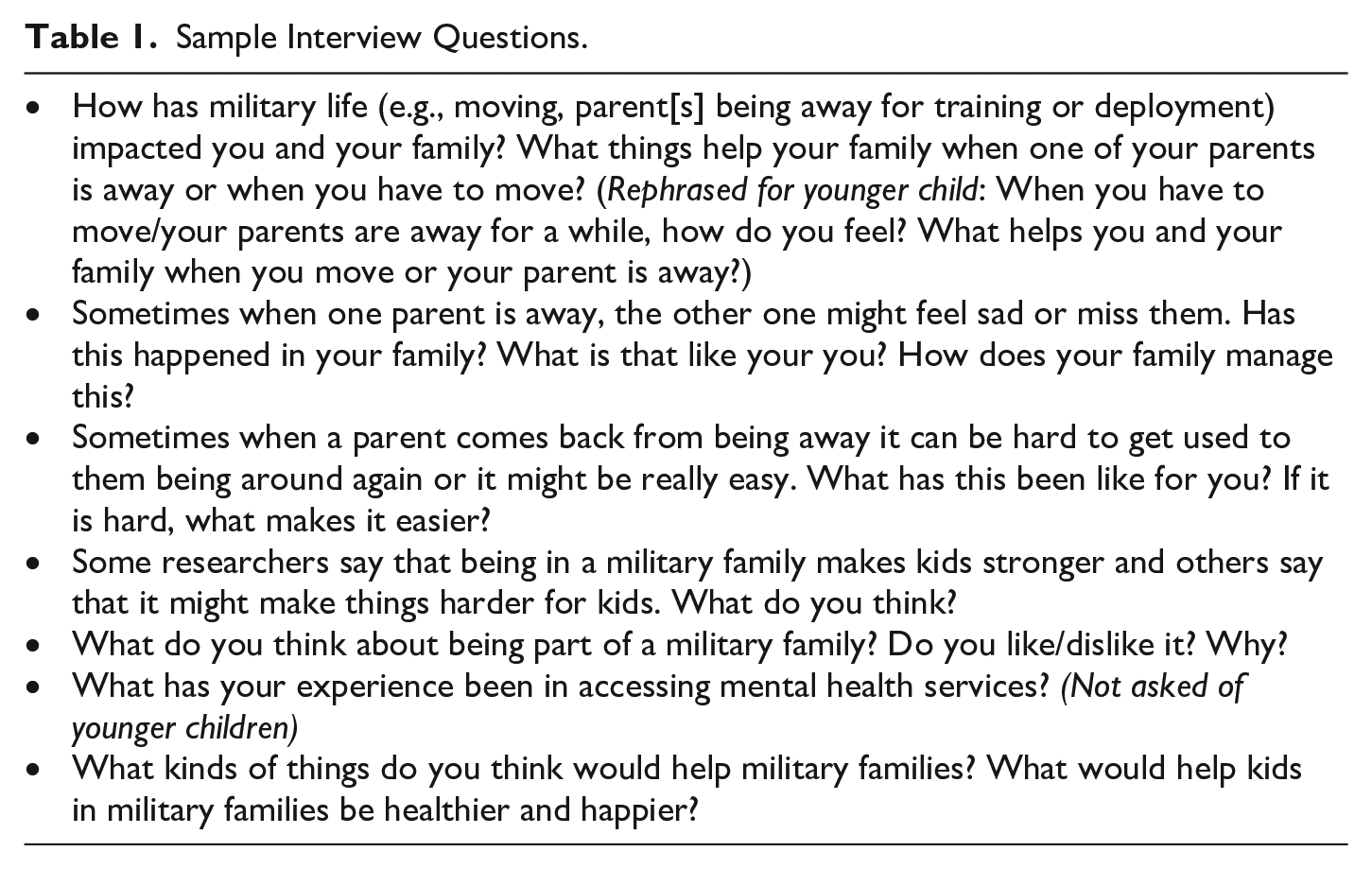
Individual interviews were conducted using an interview guide developed by the research team based on the scoping review results (Cramm, McColl, et al., 2019), with a particular focus on teasing out the Canadian experience. We conceptualized mental health broadly, using the World Health Organization’s (2018) definition, 1 considering behavior, emotions, social interactions, academic performance, specific symptoms, and diagnoses. We collected demographic information related to the child, parental military career, and military-related stressors (e.g., relocation, parental absence, and conflict deployment). The interview guide also contained questions related to the child’s experience of military-related stressors, parental mental health, resilience and vulnerability, and recommendations for supporting children in military families. The interview guide was pilot tested by the first and senior authors and changes were made to enable better comprehension among younger children (see Table 1 for sample interview questions).
Sample Interview Questions.
Most interviews were conducted by the first author, with the exception of the first one, which was conducted by the second author. Neither interviewer had military services experience but both have personal and professional connections to military populations (e.g., clinical experience working with military-connected children, familial connection to the military). The children were the primary source of data; however, parents of younger participants were present during the interviews and occasionally provided information that the child could not (e.g., details of military parent’s career). Rapport was established by using probing questions to get to know the participants or allowing them to direct the conversation while staying on topic. For example, some participants told the interviewer about pets, friends, or other interest, which the interviewer showed interest in before redirecting the conversation back to the research topic. In addition, participant validation, was used throughout the interview to build trust and ensure reliability of the data. Interviews ranged from 30 to 90 min, were conducted in-person or by phone, and were audio recorded and transcribed verbatim with identifiers removed.
Interview data were inductively analyzed using qualitative content analysis, which is consistent with qualitative description (Morgan, 1993; Sandelowski, 2000). Transcripts were reviewed by two research team members in consultation with the senior author and initial impressions and memos were used to develop a list of categories and create the preliminary code book. The preliminary code book was pilot tested by having two coders and the senior author apply the code book to two transcripts. These three research team members then refined the code book until consensus was reached. Once the code book was finalized, two coders applied it to two transcripts and these were compared to ensure inter-coder reliability. Once both coders agreed on the criteria for each code, they each coded half of the transcripts. Once initial coding was completed, the coders and senior author collaboratively examined the coded data and clustered similar codes into groups, forming the overarching themes that represented patterns across the data. Qualitative data analysis software, MAXQDA (VERBI, 2016), supported this process. Once inductive data analysis was completed, we compared the results with those of the scoping review (Cramm, McColl, et al., 2019) to examine whether the experiences of our participants resonated with the results of the scoping review.
The Queen’s University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board granted ethical clearance (#6016357). Given the focus on mental health and the risk of emotional discomfort for participants, we provided participants with a list of mental health resources to use in the event they found themselves in need of support.
Results
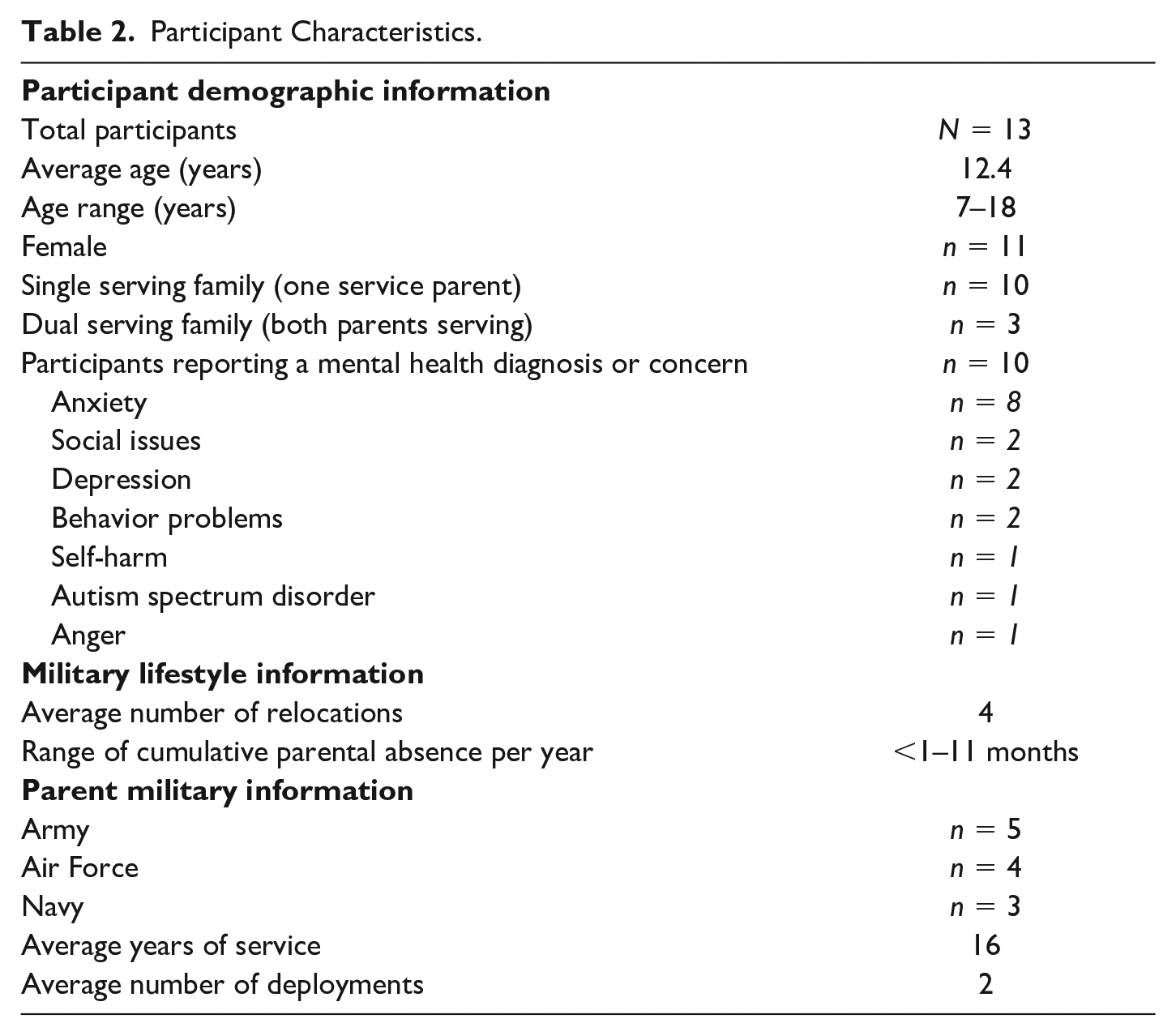
A total of 15 children or their parents inquired about participation; two did not respond to follow up. Thirteen children, including three sets of two siblings, representing 10 nuclear families, participated in the study (see Table 2 for additional demographic information). Ten participants had a current mental health concern or diagnosis (reported by the child and/or the parent). All CAF service elements (i.e., Air Force, Army, Navy) were represented.
Participant Characteristics.
The results of the qualitative analysis fit into two main themes: (1) Mobility, parental absence, and risk of parental injury/death had implications for participants’ mental health; (2) Military lifestyle stressors impacted participants in different Ways.
Mobility, Parental Absence, and Risk of Parental Injury/Death Had Implications for Participants’ Mental Health
Participants discussed three major stressors: frequent relocation, parental absence, and risk of parental injury. They also discussed the accumulation of all these factors.
Mobility
Participants’ spoke about mobility as a resoundingly negative experience and some indicated it was their least favorite part of growing up in a military family. Participants talked about academic difficulties, emotional problems—including sadness, worry, stress, and anxiety—as well as the social implications of frequent moves. With regard to academic performance, most felt their academic performance was on par with their civilian peers but recognized that differences in provincial curricula could present a challenge for children who experience more frequent moves. Once participant spoke to this: “I noticed that, like, I’ve lived in three different provinces so a lot of curriculum aren’t the same . . . so it’s just a different, different social experience and, uh, academic experience at school.” 2
Some participants reflected on the emotional pain associated with leaving friends and neighborhoods they had grown fond of. For example, one participant said,
I really loved [place]. I loved the neighborhood and everything. And I loved, I really enjoyed having my friends. And I was sad that I was going to leave my school and all the friends who were at my school. So, it was pretty heart-breaking for me.
Another participant felt it was difficult to get settled in a new location and sometimes the next move was coming up just as they were starting to feel established:
I don’t really like [moving] because, like, it takes about a year or two for me to at least become fully comfortable, and then we just have to move all over again . . . So, that’s kind of harsh for me.
Although these negative sentiments about mobility were pervasive among participants, some pointed out that frequent relocation may allow them to develop sharper interpersonal skills than their counterparts in civilian families who are less mobile. Others expressed difficulty making new friends after moving and felt isolated as a result. A concerning pattern emerged among some participants who discussed avoiding the formation of new relationships to prevent the emotional pain of ending those relationships when they have to move again. For example, one participant said,
[A] big issue with moving a lot is that I always have a hard time making friends . . . I almost see no point in making friends with new people. So, I’ve kind of isolated myself from people because I’m going to move away, anyways.
Frequent relocation created additional vulnerabilities related to accessing mental health services and supports as needed. Three older participants discussed this issue. One participant was able to access mental health services as needed through the Military Family Resource Centre (MFRC), extended health benefits, or a primary care provider. Two participants, who were unable to secure a primary care physician through the provincially funded health care system, had to rely on walk-in clinics, limiting their ability to obtain referrals for specialized mental health services. Other barriers they identified included a lack of provider understanding of military culture and long wait times that sometimes surpass posting tenure. One participant said “it’s just been very hard to try and get the help that I need” when reflecting on this experience.
Parental Absence
All participants identified negative mental health implications resulting from parental absence including increased emotional difficulties, stress, academic problems, and negative impacts on parent–child relationships. Several identified protracted parental absences as the worst component of military life. Participants described negative emotions such as anger, sadness, and anxiety related to parental absence and pointed to the cyclical nature of mandatory military travel (e.g., for training, exercises, and deployments). One younger participant (under age 12 years) spoke to this: “when my dad’s gone, I’m like, I get angry and I get sad and I’m only a little happy when he’s gone. Just like about nine per cent.” Another participant commented on the implications of this increased stress on academics:
. . . you might be trying to study for a test, but you don’t really feel like studying, exactly. You just feel like being with your parents. And then it kind of, then winds you up because you feel like you haven’t studied as much.
Participants also discussed the impact parental absence had on their relationship with the serving parent, specifically related to the parent missing milestones such as birthdays, holidays, and special events and the impact this had on the child’s mental health. One participant stated,
For the most part it was, it was pretty hard having them away all the time, just because you don’t get to have the same memories that everyone else does . . . I feel like I don’t have a whole lot of memories of my parents when I was a kid.
These issues were particularly salient among participants whose families were living on imposed restriction, meaning they were living separately (i.e., serving parent living at the posting location and the family living in a different city/province). One participant spoke to this:
I feel that, like, I had a stronger bond with him when I did live with him . . . So I do feel like—I mean, when he comes home it’s great, but I just feel like I don’t have that father/[child] bond that I used to when we lived together.
Another participant with existing mental health issues, whose family was on imposed restriction, felt that their parent’s absence was an ongoing barrier to their recovery: “sometimes it feels like that does, kind of, affect my getting better . . . it just feels like he’s not really here while I’m trying to get better, which doesn’t help.”
Periods of protracted parental absence also introduce an additional dimension for the at-home parent, who is taxed with additional roles, stressors, and responsibilities. Most participants reported that, while their serving parent was away, their own emotions would mirror their at-home parent’s emotions. Participants appreciated the added stressors created for their at-home parent who functions as a sole parent and recognized how this can also impact the emotional tenor of the home. One participant expressed this eloquently: “if Mom’s sad, you’re generally going to be sad, too, even if you don’t understand why. But yeah, I think just the whole tone of your household.” Some participants also described worrying for their at-home parent’s well-being and attempting to comfort or support them during these times. This was particularly intense for families on imposed restriction, as one participant pointed out:
[S]o far it, um, I think it’s gone all, all right. There have been harder moments. Like, I know it, it can cause a lot of stress on, on my mom because that is a lot of, I mean, taking care of me and my sister. . . . which then, sort of, it fizzles out into the rest of the house.
Reuniting with a parent was generally seen as a very happy time and many participants described feelings of elation. Other participants described a relatively seamless reintegration back to family life after a parent returns home. One participant said “[T]hings go back to normal. Things are just a lot happier and everything seems, like, airier and more lively.” A minority of participants noted some awkwardness during reintegration and one participant identified that the parent will need to leave again just as the discomfort is receding: “he came home, comes home, I’m, like, just doesn’t feel right. But then, once I get used to him, he’s gone.”
Risk of Parental Injury or Death
The risk of harm to the serving parent was primarily discussed by older participants, most of whom expressed worry and fear about their parents when they are deployed to areas of conflict or disaster. Participants expressed anxiety related to not knowing whether parents will return home safely. One participant commented on how this worry affects their concentration at school:
I always worry about my dad, going somewhere, like going somewhere. So, sometimes on those days at school, I’ll feel a little, a little sad, or I won’t try to, like, I’m not very happy at, that day, if I really know that something big is going on.
Military Lifestyle Stressors Impacted Participants in Different Ways
Many participants felt that the stress related to military lifestyle factors—most notably frequent relocations and parental absence—caused them anxiety that their civilian peers may not experience; one participant stated:
I think I probably feel more emotions than most of my friends do. . . . Like, sad and angry, and nervous . . . Maybe because, like, I’ve moved a lot and there’s a lot of new things and a lot of changes.
Some participants point out that, like civilian children, the way military-connected children respond and cope with stressors is highly dependent on the individual differences and some children will cope better than others. Two participants felt that encountering the challenges of the military lifestyle can present opportunities to build adaptability and problem-solving skills that may not be present in civilian families, which participants felt promoted mental health. One summed this up by saying,
I think everybody has, sort of, challenges in their life. And military kids just happen to have different ones than everybody else, maybe . . . I think that military kids have . . . a bigger view on the world and life in general. Like, they’re more, I don’t know, maybe more open to change and they can adapt quicker, maybe.
Frequent relocation, in particular, seemed to present both challenges and opportunities for participants. One participant felt that the experience of moving and being away from their parents has increased personal adaptability and preparation for meeting life challenges like transitioning from high school to university. Several participants pointed out the complex impact of frequent relocation, indicating that moving gives them the opportunity to experience new things and meet new people while concomitantly increasing the frequency of having to say good-bye to friends and places. One participant captured this duality when they said:
I feel like it’s, in some ways, made me a lot stronger and realize to be grateful for what you have. But don’t like it, because, um, people are away and it just makes you, like, more sad, and I feel like, if I wasn’t in a military family, I’d have it easier life. But if there was to be a real problem, I wouldn’t be ready for it.
Some older participants commented on the accumulation of multiple military family lifestyle factors (e.g., combination of parental absence and mobility) or frequent occurrences of one stressor (e.g., multiple and frequent parental absences) that, when compounded, created additional vulnerability. One participant spoke to this:
I think that them being away when I was younger is just like hitting now. I didn’t really, um, let it sink in when I was younger. I didn’t really let it affect me, and then, now I’m just scared that everyone’s going to leave me, like my parents did when I was younger, not knowing if they’re going to come back or not.
The sentiment from participants was that the impact of military life on child mental health is complicated and dependent on a multitude of factors and the military lifestyle has the potential to both promote and detract from mental health. Some participants reported that growing up in a military family “makes us stronger” and some aspects of the military lifestyle can lead to unique experiences that broaden one’s horizons:
I think . . . all the opportunities I’ve gotten from it—I’ve done so many things that none of my friends now could ever dream of doing . . . His job has opened so many doors.
Discussion
This study is among the first peer-reviewed studies to investigate Canadian military-connected children’s perspectives specifically on the mental health implications of growing up in a military family. This study also contributes to the small but growing body of research on Canadian military families examining military-connected children’s experiences (Cramm et al., 2015). The results of this study addressed the research question and indicated that, for our participants, military lifestyle factors including frequent relocation, parental absence, and risk of parental injury impacted mental health and these implications were variable and individual. In this discussion, we will compare our results to those found in Cramm, McColl, et al. (2019) scoping review on mental health among military-connected children. Then, we will discuss implications and future research directions as well as the study limitations.
Comparing Our Results to the Scoping Review
The first theme identified in Cramm, McColl, et al. (2019) scoping review is “children growing in military families seem to have more mental health issues than their civilian comparators” (p. 2). This study was not designed to compare mental health diagnoses or service utilization across military and civilian children, therefore, we cannot provide insight on this particular theme. In the United States, researchers have directly compared military and civilian populations by examining insurance claims data from military and civilian insurance providers and have found that mental health service use is greater among military-connected children (Pressley et al., 2012; Williams et al., 2004). In Canada, this sort of comparison has been difficult since children in military families access the same health systems as those in civilian families and there are inconsistencies across provinces/territories in how, or whether, they are identified. This work is beginning in Ontario but no comparisons have been made with respect to mental health service usage.
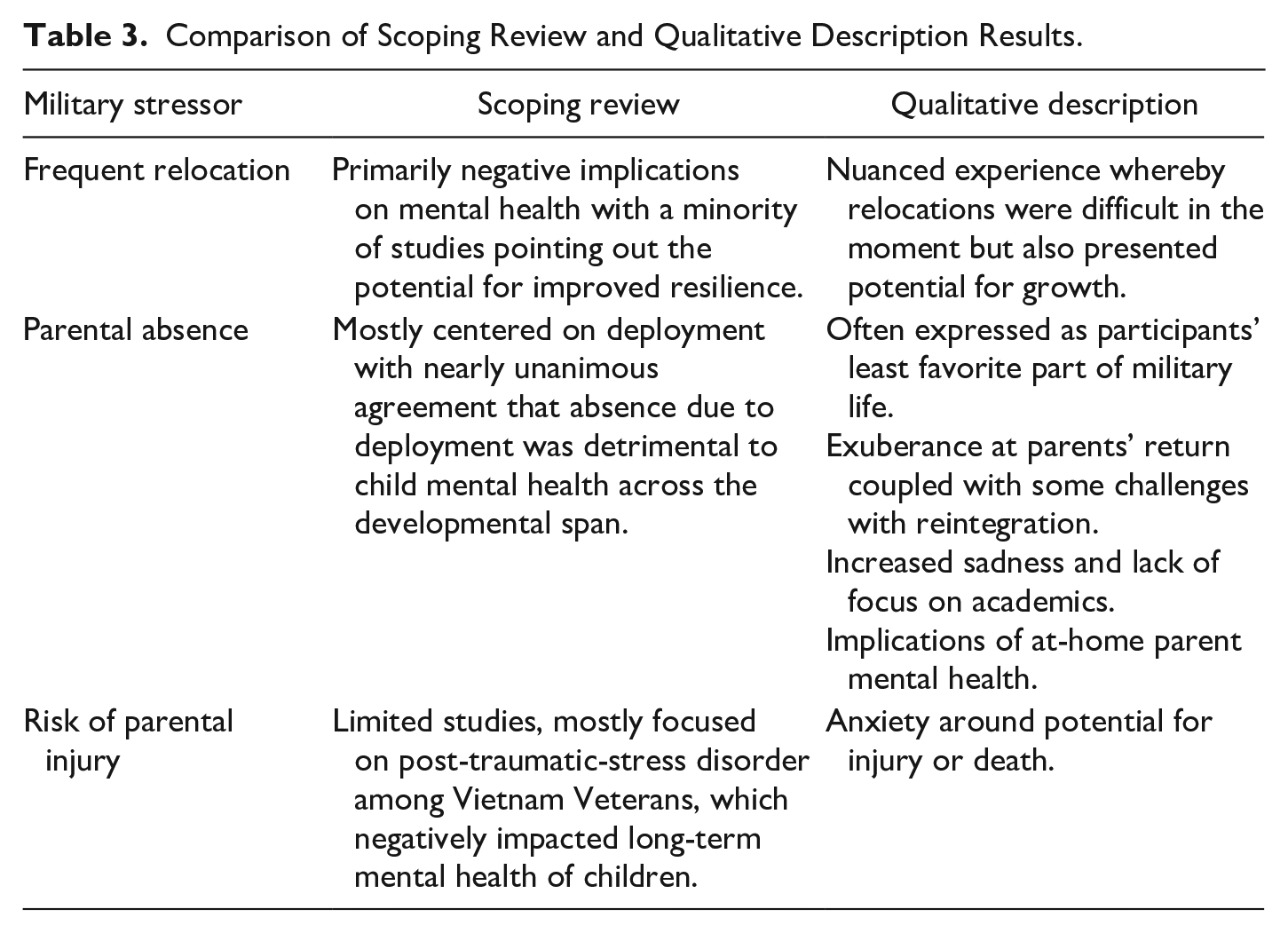
The second theme in the scoping review dealt with the impact of military-related stressors on child mental health, which our results do shed light on. For our participants, these components of the military family lifestyle created a unique set of stressors that recurred over time to create unique mental health challenges and needs, which was consistent with Cramm, McColl, et al.’s (2019) findings. Considering 86% of the scoping review articles were American, the consistency between our participants’ experience and the scoping review results provides preliminary evidence which may indicate that, although the national contexts are different, Canadian children may share some of the same experiences and mental health implications of military life as their American counterparts. Table 3 compares the scoping review findings to our participants’ experiences in relation to frequent relocation, parental absence, and risk of parental injury.
Comparison of Scoping Review and Qualitative Description Results.
Parental absence was particularly problematic among our participants who voiced unanimous and overwhelmingly negative mental health implications associated with this aspect of the military family lifestyle. This is consonant with the findings of Cramm, McColl, et al.’s (2019) scoping review, which reports that almost all the included studies revealed negative mental health implications of parental absence due to deployment, as did other Canadian government reports and academic research (Bullock & Skomorovsky, 2016; Harrison & Albanese, 2012; Skomorovsky & Dursun, 2013; Sudom, 2010).
Among our participants, the relationship between the military parent’s absence and the at-home parent’s mental health was more pronounced than in the scoping review. Participants discussed the impact of the at-home parent’s mental health during periods when the serving parent is absent from the family. They described the potential for the at-home parent’s emotional state to ripple into the rest of the family, who may feel a sense of responsibility for their at-home parent’s mental health, echoing other American and Canadian research included in Cramm, McColl, et al.’s (2019) scoping review and recent Canadian government reports (Manser, 2018a). These results also support calls from American researchers to increase assistance for at-home parents (Strong & Lee, 2017). Studies report the serving parent’s mental health can have negative implications for child mental health as well (Cramm et al., 2020; Cramm, McColl, et al., 2019; Fear et al., 2018; Norris et al., 2015) although this did not arise among our participants.
In this study, frequent relocation was associated with significant stress and sadness resulting from leaving important friendships as well as a negative impact on academic performance due to provincial and regional differences in curriculum. Participants also pointed out positive aspects of relocation including new experiences and increased adaptability. This closely echoes Cramm, McColl, et al.’s (2019) findings showing primarily negative implications of relocation with some positives, indicating similarities between these two nations.
One challenge of relocation that sets the Canadian experience apart is the way in which Canadian military families access health services. Cramm, McColl, et al. (2019) point out that American military-connected children all access the Military Health Service, while their Canadian counterparts must access provincial and territorial health systems along with the rest of the civilian population (Daigle, 2013). This study provided some insight into the lived experience of accessing public health services in the Canadian context. Indeed, concerns have been expressed regarding access and quality of health services for military families in Canada (Daigle, 2013; Davila et al., 2020; Vogel, 2014). Although a small number of participants discussed health service access in this study, other Canadian research indicates that securing health services was one of the primary concerns military families had when facing a move (Manser, 2018b). CAF spouses encounter barriers to health service access including difficulty finding a primary care provider, disruptions in continuity, and problems transferring health records (Darr & Doan, 2011; Vogel, 2014) and it stands to reason that these issues would apply to children in these families as well. Recent studies have reported delays in health service access among Canadian military family members (Mahar et al., 2018), especially those with special health needs (Cramm, Smith, et al., 2019). Our study contributes to this body of literature by adding the child perspective on access to mental health services specifically.
Our participants expressed that, although the military lifestyle presents challenges that make children vulnerable to mental health issues, there are opportunities for growth and resilience. Cramm, McColl, et al.’s (2019) drew similar conclusions based on their review of the literature, indicating that military lifestyle factors may “act as a catalyst to potentiate these resiliencies and vulnerabilities (p. 7).” Relocation may increase vulnerability among some children but may conversely bolster resilience in others. Other Canadian studies have pointed out the positive influences that the military lifestyle can have on children (Bullock & Skomorovsky, 2016; Kwan-lafond et al., 2011). This potential for both resilience and vulnerability was, in this study, most salient in the context of frequent relocation. The stress, anxiety, and social implications associated with frequent relocation were clear among participants, but so was the potential to build adaptability and have new experiences. This was echoed in Bullock and Skomorovsky’s (2016) study investigating children’s positive experiences regarding frequent relocation.
Cramm et al. (2018) conducted a synthesis of the literature describing models and theories of resilience in military families and presented a visual model representing their results. This model depicts how intrafamilial factors (e.g., stress management style differences), family processes (i.e., belief systems, organizational patterns, and open communication), and ecological factors (e.g., military culture, formal and informal support systems) interact with military lifestyle stressors (e.g., chronic and acute stressors) to influence resilience. This framework highlights the complex and dynamic nature of resilience and vulnerability and provides some insight into the ambiguity seen in this study regarding military-related stressors like relocation.
Resilience and vulnerability may depend on a number of factors including developmental stage, individual child and family traits, and contextual factors (e.g., frequency of relocations). Skomorovsky (2013) pointed out that individual traits play a role, reporting that children who maintained relationships with friends from previous postings and were more extraverted seemed to cope better with moves. This is consistent with the reports of our participants who indicated that children who are shy may have more difficulty making friends after a move. Another factor influencing resilience and vulnerability can include the circumstances in which military-related stressors are experienced (e.g., more frequent absence and/or moves). For example, American research reports that the more frequent and protracted parental absence, the more detrimental they were to child mental health (Millegan et al., 2013; Mustillo et al., 2015).
Implications and Future Research
Our results provide health, education, and other service providers with a preliminary understanding of the mental health implications of military life on children, from the perspective of the children themselves, with a specific focus on the Canadian context. This study may help improve providers’ military cultural competence—the “degree to which providers are sensitive to the unique needs and relevant issues of concern (Tanielian et al., 2014, p. 2)” related to military members, Veterans, and their families—and promote more effective service provision. Military cultural competence among health providers is gaining attention from Canadian researchers. For example, Tam-Seto et al. (2018) developed and validated a military family cultural competence framework that is being used by Calian Health’s Military Family Doctor Network to build military cultural competency among family doctors. There seems to be some recognition of the importance of health provider awareness of military family issues as evidenced by an educational resource that was recently developed for family physicians by The College of Family Physicians of Canada & Canadian Military and Veteran Families Leadership Circle (2016) and a recent article focused on caring for military-connected families in primary care (Cramm, Mahar, et al., 2019). Our findings build on this work and can help inform future efforts aimed at preparing clinicians and other civilian community supports for working with military families.
Our findings also reveal that there is still much to learn about the mental health implications of military life on Canadian children and additional research is needed to inform practice. Access to health services in the context of frequent relocation is an area needing more attention. While there has been political recognition of this challenge—like Ontario’s Fairness for Military Families Act (2007)—little research has examined health care access and quality for military families, let alone access to mental health services specifically. More research is needed to inform current efforts to improve access and quality within provincial and territorial health systems and cultural competency among public and private practitioners. Increased attention to mental health need and service access is essential to build the capacity of health systems to support military-connected children.
Our results support the prioritization of programs and services that assist at-home parents during serving parent absences may have a significant impact on improving the mental health of children. Focusing research funding priorities on nonserving/at-home parent mental health during the serving parent’s absence will build an evidence base for the development and evaluation of programs and services that address these needs.
The dual potential for resilience and vulnerability related to specific military lifestyle factors and individual child traits calls for a better understanding of which factors contribute to mental health vulnerability and which facilitate resilience. There may be particular combinations of factors at particular developmental periods that position children for resilience or vulnerability; understanding these is a key to developing evidence-based programs and policies that can effectively address vulnerabilities and enhance resilience.
Limitations
This was a qualitative study and, as such, was not intended to generalize results across the broader population of Canadian military-connected children. We endeavored to capture a range of experiences and represent a diversity of narratives through purposive sampling to allow transferability (Holloway & Galvin, 2017). However, despite using inclusive eligibility criteria for participant recruitment, all the participants came from heterosexual, married families with no representation from more diverse family structures (e.g., single parents, blended families, same-sex couples). This may limit the transferability of our results to military families that do not retain this family structure. Furthermore, the majority of the participants were female, limiting our ability to represent the experience of male children. In addition, some interviews were conducted in the presence of the participant’s parent (particularly younger participants), which may have influenced the data obtained from those participants. There was also a wide range in age and geographic location among participants, which resulted in a sample with varied self-awareness and nuanced reflection.
Conclusion
We interviewed 13 Canadian military-connected children to better understand the mental health issues and needs of children growing up in military families. We also sought to determine whether these children’s experience was consistent with Cramm, McColl, et al.’s (2019) scoping review examining the mental health of military-connected children, which yielded mostly American research. Our participants experienced mental health implications related to frequent relocation, parental absence, and risk of parental injury which were quite individualized and presented the potential for vulnerability and resilience. Our results are consistent with Cramm, McColl, et al.’s (2019) findings on the mental health impact of military lifestyle factors on children. Our findings provide a more nuanced picture of the Canadian experience from the perspective of the children themselves. Although attention to the well-being of military families in Canada is increasing, additional research is needed. Particular focus on the impact of parental mental health as well as access to mental health services in provincial/territorial health systems could be valuable in building knowledge and capacity aimed at improving the mental health and well-being of children in Canadian military families.
Footnotes
Acknowledgements
This research was supported by Queen’s University Master of Science in Occupational Therapy students, Emily Adams and Danielle Rettie.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Health Research Foundation.