
Abstract
Military-to-civilian community reintegration in Northern Irish (NI) veterans has not been previously examined. The existing reintegration studies indicate that post-military service life can be challenging for many veterans. The current exploratory study aimed to identify service-related predictors of community reintegration difficulties in a sample of 749 NI veterans. Data were collected through a cross-sectional self-report survey of UK Armed Forces veterans residing in NI. Service-related variables were examined as predictors of overall and subdomain-specific reintegration difficulties. Combat exposure, time spent deployed in NI, length of service, being medically discharged, and being physically injured during service were significant predictors of reintegration difficulties. Receiving a mental health diagnosis since discharge and having been medically discharged were the two strongest predictors. Further results and implications are also discussed. Post-service adjustment to civilian life is affected by service variables, with implications for military/post-military interventions aimed at mitigating difficult transition experiences.
Keywords
Introduction
Community reintegration in a military context describes the process of a service member returning from a period of deployment or transitioning back into civilian life and re-joining their community as a private citizen (Forces in Mind Trust, 2013). This process spans multiple domains, from family to community to the workplace (Elnitsky et al., 2017). In an ideal reintegration, an ex-service member (hereafter, veteran) can step back into their roles in their community, putting aside their military lives regardless of how their service may have affected them. Although most veterans enjoy a smooth community reintegration (Iversen et al., 2005), there exists a “substantial minority” who experience difficulty in adapting to civilian life (Cooper et al., 2016). Those veterans experiencing reintegration difficulties have shown reduced social functioning, relationship problems, psychological distress, alcohol/substance misuse, and other issues (Resnik et al., 2012).
A variety of factors are known to adversely influence the community reintegration process; most significantly, physical injury and mental health issues (Iversen et al., 2005; Sayer et al., 2010). Some veterans may feel burdened by the expectation that their transition be one of immediate adjustment to complete self-sufficiency and perceive needing and/or asking for support as a “weakness” (Fulton et al., 2019), while others have experienced “the military as family” which provided for and supported them (Ahern et al., 2015), and many have described difficulty in adapting to the shift in identity after separation (Brunger et al., 2013; Tarbet et al., 2020). While being injured in service and experiencing psychological distress, particularly post-traumatic stress disorder (PTSD), can negatively affect community reintegration, service-based factors including military identity also affect the success of a veteran’s community reintegration (Gordon et al., 2020; Pedlar et al., 2019). Research into community reintegration has grown in tandem with an understanding of the underlying psychological mechanisms involved but until recently, there have been no studies examining this process in a solely Northern Irish (NI) context.
Northern Ireland was host to “Operation Banner” (1969–2007), a U.K. military engagement during a period of conflict known more commonly as “the Troubles” and defined by violence, unrest, and sectarian strife (Armour, Waterhouse-Bradley et al., 2018). Due to the historic nature of the conflict which pre-dated the Troubles and the recency of their cessation, the nation remains deeply divided along sectarian lines and as a result, the act of U.K. military service is seen as controversial in many parts of the country (Armour, Waterhouse-Bradley et al., 2018). These security concerns constitute a genuine threat-to-life that leaves many U.K. veterans residing in NI reluctant to disclose their veteran status and facing stigma, discrimination, and concerns of threat if they chose to do so (Bradley, 2018). Although the United Kingdom Armed Forces Covenant (Ministry of Defence [MOD], 2016) pledges that all members “should face no disadvantages” due to military service when compared with the civilian population, the Covenant is not implemented in NI. As defense is not a devolved matter, the NI Executive has no responsibility for the welfare of U.K. veterans resident in the nation, leaving a potentially vulnerable population with little formal support. Statutory support for NI veterans falls to 19 organizations, of which half are based in Great Britain and are U.K.-wide services, contrasted with 1,818 in England and Wales, and 461 in Scotland (Armour et al., 2017; Armour, Waterhouse-Bradley et al., 2018), including dedicated bespoke organizations such as Veterans NHS England, Veterans NHS Wales, and Veterans First Point Scotland. In addition, security issues compound the pre-existing barriers to help-seeking, resulting in decreased help-seeking behavior in NI reinforcing the belief that less support is needed (Armour et al., 2021).
Research into this population remains difficult due to the need for participant security and hesitancy to disclose/discuss veteran status. The Northern Ireland Veterans Health and Wellbeing Study (NIVHWS) was the first to attempt to explore the demographics and mental/physical health of the veteran community in NI, though was reliant on veteran participation as the MOD was unable to lift the high-security clearance on NI Armed Forces data to collaborate in data linkage (Armour et al., 2021). As a result, the U.K. veteran population in NI is described largely in estimation, with an assumed size of 150,000 individuals (Royal British Legion, 2014), and other general demographics largely unknown. Previous studies have investigated population subgroups, namely, help/treatment-seeking veterans, finding U.K. Armed Forces veterans residing in NI to be older and more disadvantaged than those in other parts of the United Kingdom, also reporting significantly more physical health problems (Ashwick & Murphy, 2017; Murphy & Busuttil, 2017).
The MOD (2020) has outlined the continued strengthening of community reintegration initiatives as part of its Strategy for our Veterans highlighting an increase in funding to existing support programs, new programs for veterans in extreme need, and several policies designed to ease the transition between military and civilian life. The general British population has been described as looking positively on the Armed Forces, as evidenced by the large amount of admiration and charity support for veterans (Duel et al., 2019) but such endemic social support is not present in NI (Armour et al., 2018) As veterans may withdrawal from social contact after service (Hatch et al., 2013), feeling a shift in identity outside the military “bubble” (Gordon et al., 2020), lack of perceived support may negatively affect on reintegration. Employment is a key cornerstone of the MOD’s ongoing strategy for successful reintegration, including career training initiatives and incentives for employers to hire veterans (MOD, 2020). In a cohort of treatment-seeking U.K. veterans, lower age, physical health problems, PTSD, and length of time since service were associated with not being able to work, which negatively affected reintegration (Hendrikx et al., 2020), while NI veterans faced the additional effects of cultural and socioeconomic barriers to employment after separation (Roy et al., 2020).
Although a substantial body of literature exists on military to civilian community reintegration, a critical review of 186 papers returned scant evidence of support initiatives, interventions, and/or models of care to address reintegration difficulties (Elnitsky et al., 2017), highlighting the importance of integration research on a local contextual scale. Unfortunately, most of the research into community reintegration in the United Kingdom has utilized veteran populations in England, not delineated between devolved nations in their methodologies (Roy et al., 2020), or have focused on theater-based cohorts (Iversen et al., 2005). To adequately design and trial successful interventions for U.K. Armed Forces veterans residing in NI, it is vital to understand both predictors of overall community reintegration difficulties as well as predictors of difficulties in specific subdomains of reintegration. This study utilized the Military to Civilian Questionnaire (M2C; Sayer et al., 2011), which provides a total reintegration difficulty score as well as scoring difficulties in Interpersonal Relationships, Productivity, Community Participation, Self-care, Leisure, and Meaning in Life. With support for U.K. Armed Forces veterans residing in NI falling largely to dedicated support organizations, the ability to tailor interventions to specific profiles of need in the population would greatly benefit veterans, their families, and the wider communities to which they belong.
The goal of this study was an exploratory examination designed to identify service-related predictors of community reintegration difficulties among NI veterans to (a) address gaps in the literature, (b) uncover predictors which may be distinct to NI, (c) identify predictors in specific subdomains of reintegration difficulties to improve intervention/support programs, and (d) generate a profile of service needs for use by policymakers in supporting veterans. Demographics, military service data, and scores from the Military to Civilian Questionnaire (Sayer et al., 2011) were collected as part of the NIVHWS and used in a multiple regression to identify variables predicting overall reintegration difficulties, with a further exploratory analysis to examine predictors of specific subdomains of reintegration difficulties.
Method
Data and Participants
The data for the current study were collected between December 2017 and June 2019 through a cross-sectional self-report survey of U.K. Armed Forces veterans living in NI. The survey was advertised through social media and local organizations working with veterans. Recruitment emails and text messages were also sent directly to veterans who had previously engaged with the research team as part of the NIVHWS and agreed to participate in further research. Questionnaires were available online and in pen-and-paper format. Initially, N = 3,521 respondents entered the study but n = 2,105 did not provide full informed consent and were removed, along with an additional n = 87 responses (n = 1 test response, n = 80 blank/demographics-only responses, n = 6 participants who did not meet study criteria), leaving an eligible sample of N = 1,329 participants. The effective sample for the current study was N = 749 participants who completed measures used in the analyses.
Measures
The questionnaire took approximately 1–2 hr to complete. Described below are items/measures relevant to the current study.
Demographic and Military Variables
Participants were asked about their age, gender (1 = female, 2 = male), length of time spent on deployment outside NI (years), length of time spent on deployment in NI (years), age of joining the Armed Forces, length of service in the Regular Forces (years), and in the Reserve Forces (years), whether they were medically discharged from service (1 = yes, 2 = no), whether they suffered any physical injuries during service (1 = yes, 2 = no), and whether they received a mental health diagnosis since leaving the service (1 = yes, 2 = no).
Combat exposure was assessed with six items adapted to the context of NI from the Combat Exposure Scale (Keane et al., 1989; see Appendix A for adaptation). Items were presented in Likert-type format (coded 1–5), but due to adaptation, the original weighted scoring was not used. Instead, a sum score was created and used as a continuous variable, with higher scores indicating higher levels of combat exposure. Cronbach’s alpha in the current study was .842.
Reintegration Difficulties
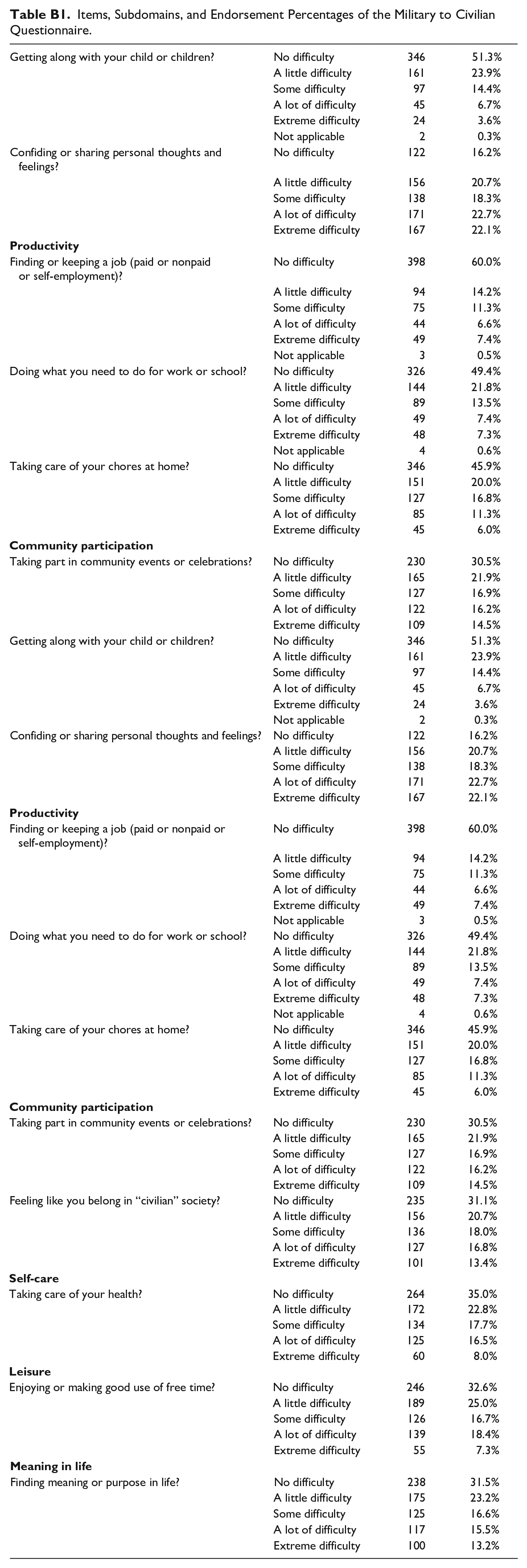
Reintegration difficulties were assessed with the Military to Civilian Questionnaire (Sayer et al., 2011; Appendix B: Table B1), consisting of 16 items assessing difficulties in community reintegration across six subdomains: interpersonal relationships, productivity at work/school/ home, community participation, self-care, leisure, and perceived meaning in life. The M2C utilizes a 5-point Likert-type scale (from 0 = “no difficulty” to 4 = “extreme difficulty”) and a “not applicable” option for 4 items. Participants were asked to answer in relation to the “time since [they] left the military.” Total reintegration and subdomain scores were calculated by summing the scores for all items and dividing by the number of completed items (i.e., responses other than “not applicable”), with higher scores indicating more reintegration difficulties. Cronbach’s alpha for the current study was .958.
Data Analysis
From the study population of N = 1,329, n = 573 responses were removed due to no data on the M2C questionnaire, and n = 7 responses were removed for missing values on categorical variables, leaving an effective sample size of N = 749. For the purposes of the analyses, the remaining missing values (1.8%) on the continuous variables were estimated using the expectation maximization algorithm (EM) in SPSS. Preliminary analyses were conducted in SPSS 25 and the regression analyses were conducted in Mplus 7.3.
The association of reintegration difficulties with different military constructs was examined using Spearman’s rho correlations (time spent on deployment outside NI, time spent on deployment in NI, age at joining the Armed Forces, length of service in Regular Forces, length of service in Reserve Forces, combat exposure) and Mann Whitney U tests (medically discharged, physical injury during service), as the reintegration variable was not normally distributed. Age, gender, and mental health diagnosis since leaving the Armed Forces were also included in these preliminary analyses. Apart from being medically discharged, physical injury during service, gender, and mental health diagnosis since leaving the Armed Forces, which were coded as binary variables, all other variables were used as continuous variables.
A multiple regression was then performed to examine the relationship between the military-related variables and reintegration difficulties, with both unadjusted and adjusted models. The adjusted model controlled for the effects of age, gender, and having received a mental health diagnosis since discharge. An exploratory analysis was then conducted to examine the relationship between the predictor variables and the subdomains of reintegration difficulties. A multivariate multiple regression was used to determine the relationships between predictors and the subdomains. Wald’s tests of parameter constraints were used to compare the regression coefficients and Bonferroni correction was applied to account for the high number of pairwise comparisons.
Results
Sample Characteristics and Preliminary Analyses
Most participants were male (N = 669, 89.3%), the mean age was 55.7 years (SD = 10.8), and 99.5% self-reported their ethnicity as white. The majority (N = 649, 86.6%) had served in the Army, N = 81 (10.8%) served in the Navy, N = 57 (7.6%) in the Air Force, and N = 13 (1.7%) served in the Marines (some veterans served in more than one branch). Table 1 shows the descriptive statistics for the study variables.
Descriptive Statistics.
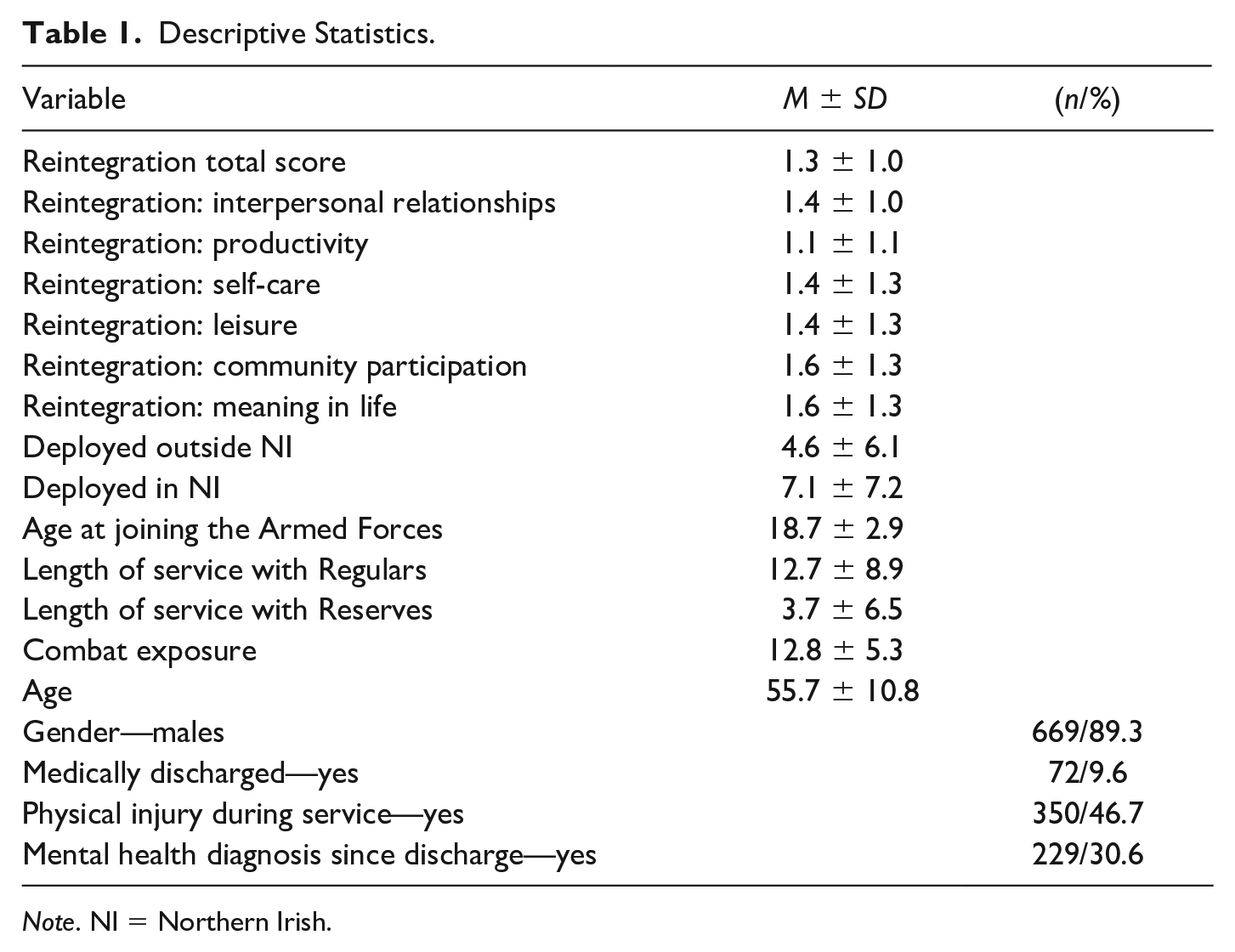
Note. NI = Northern Irish.
The results of the bivariate correlations are presented in Table 2. The length of deployment in NI, age at joining the Armed Forces, length of service in the Reserve Forces, combat exposure, and age were all significantly associated with the total reintegration score, whereas the length of deployment outside NI and the length of service in Regular Forces were not. There was no multicollinearity between the predictor variables, as indicated by the variance inflation factor (all values between 1.06 and 2.30). Tests of differences showed that the medically discharged (Med = 2.28) had significantly more reintegration difficulties than participants who were not medically discharged (Med = 1.06; U = 12,909.00, p < .001), those who had suffered physical injuries while deployed (Med = 1.50) had more reintegration difficulties than those without injuries (Med = 0.88; U = 50,568.00, p < .001), those who have been given a mental health diagnosis since discharge (Med = 2.25) had more reintegration difficulties than those without (Med = 0.81; U = 23,056.00, p < .001), but there were no differences between males (Med = 1.19) and females (Med = 1.13) on reintegration difficulties (U = 25,697.00, p = .561).
Bivariate Correlations.
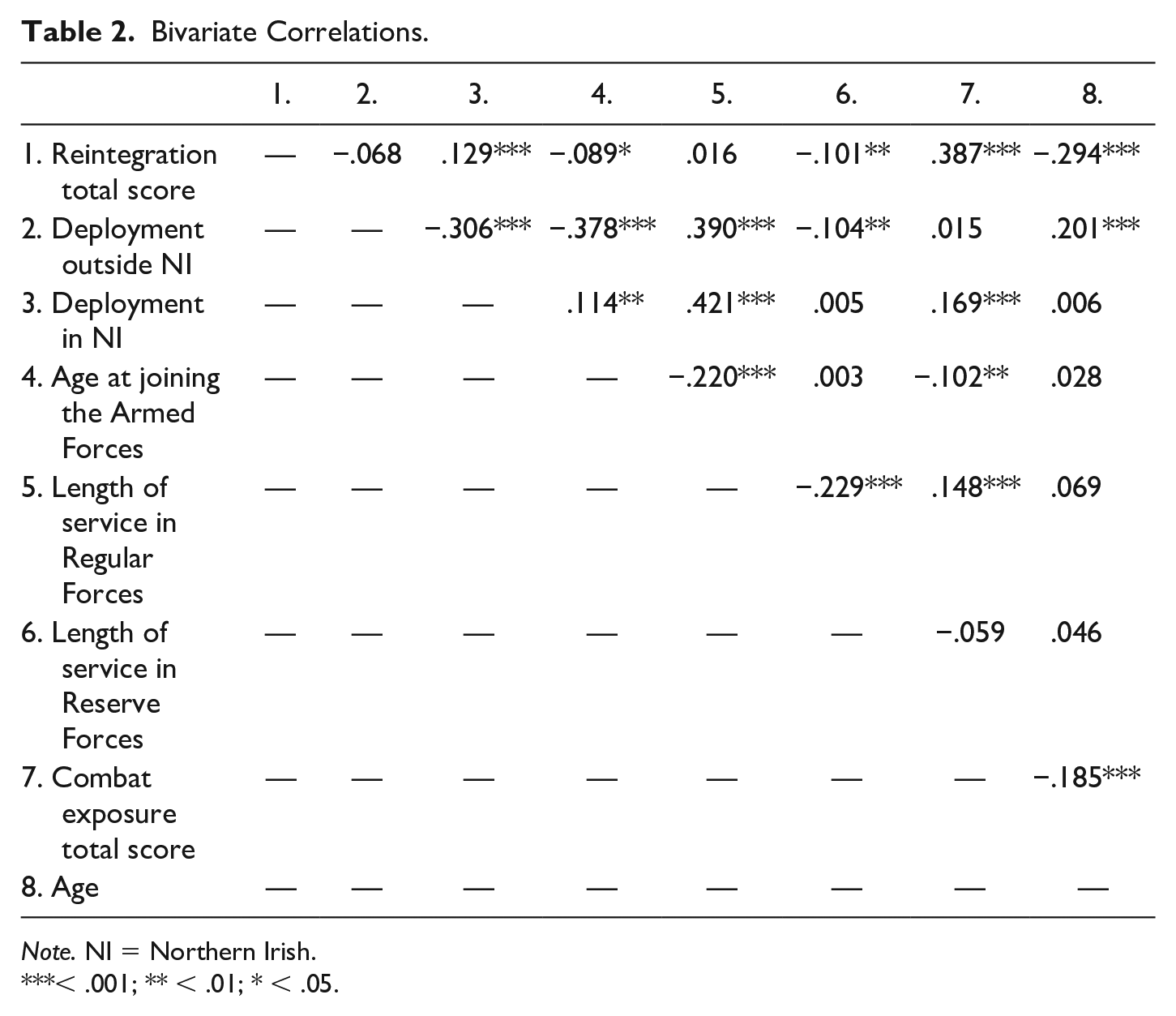
Note. NI = Northern Irish.
< .001; ** < .01; * < .05.
Multiple Regression
Results of the multiple regression analysis are presented in Table 3. In the unadjusted model, all variables excepting the length of deployment outside NI, significantly predicted the total reintegration score; more time spent on deployment in NI, younger age when first joining the Armed Forces, less time spent serving with the Regulars and the Reserves, and a higher combat exposure, predicted more reintegration difficulties. In addition, being medically discharged from service and having suffered a physical injury during service significantly predicted more reintegration difficulties. The model explained 20.4% of the variance in the total reintegration score (R2 = 0.204, SE = 0.026, p < .001).
Multiple Regression Results With Military Variables Predicting Community Reintegration Total Score.
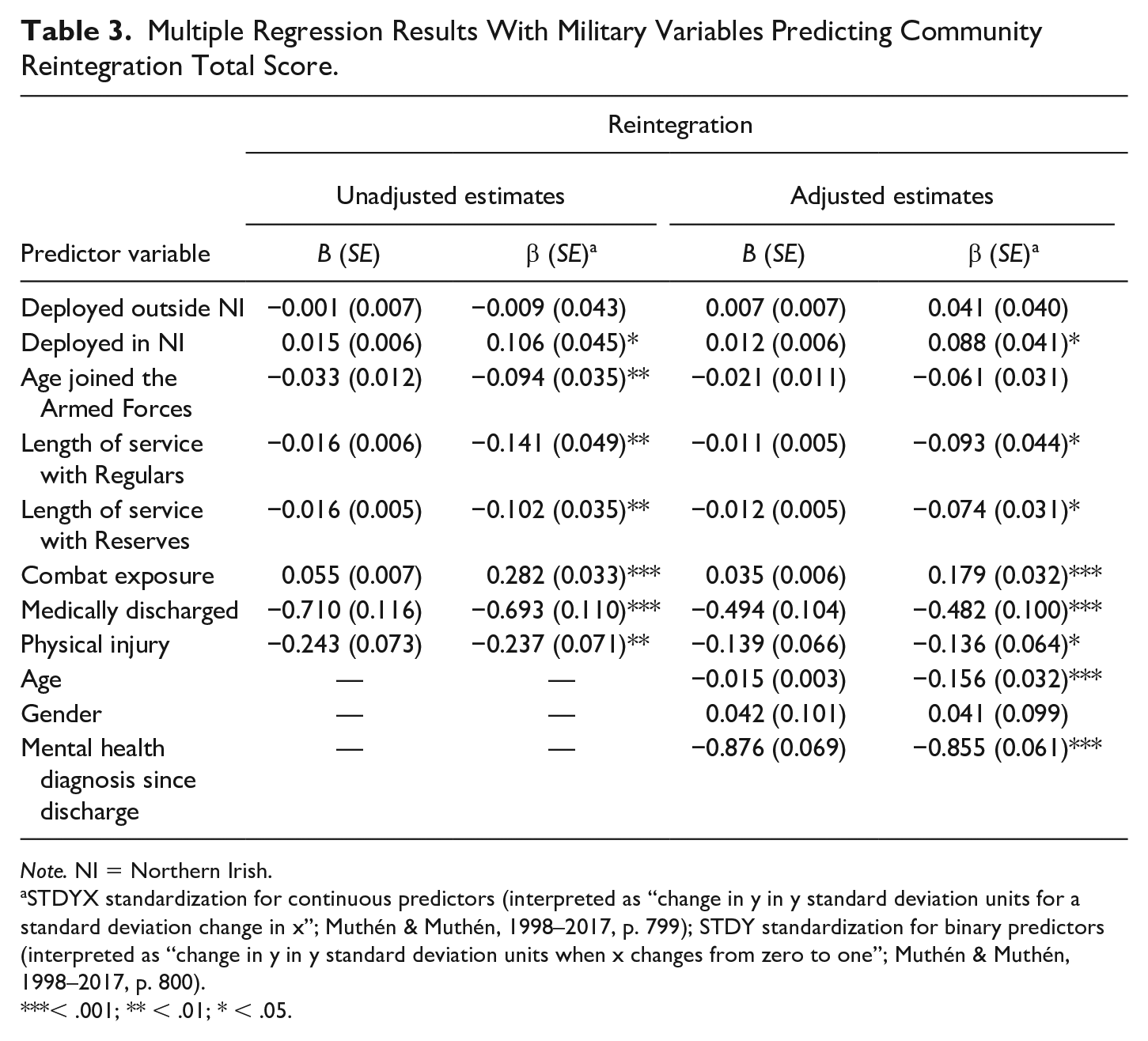
Note. NI = Northern Irish.
STDYX standardization for continuous predictors (interpreted as “change in y in y standard deviation units for a standard deviation change in x”; Muthén & Muthén, 1998–2017, p. 799); STDY standardization for binary predictors (interpreted as “change in y in y standard deviation units when x changes from zero to one”; Muthén & Muthén, 1998–2017, p. 800).
< .001; ** < .01; * < .05.
The results remained largely unchanged when adjusting for age, gender, and a mental health diagnosis since discharge from the service. The estimates were slightly reduced, and the length of time participants spent deployed outside NI became non-significant. Gender did not predict reintegration difficulties, but age and a mental health diagnosis since discharge from service were significant predictors of reintegration difficulties; younger age and a mental health diagnosis contributed to significantly more difficulties, with a mental health diagnosis being the strongest predictor of difficulties. The adjusted model explained 37.3% of the variance in the total reintegration score (R2 = 0.373, SE = 0.028, p < .001).
Exploratory Analyses
Because a mental health diagnosis had such profound effects on reintegration difficulties, unadjusted results are not presented for the exploratory analyses. Table 4 shows the effects of predictor variables on different subdomains of reintegration difficulties. High levels of combat exposure, having been medically discharged, younger age and a mental health diagnosis consistently predicted higher levels of reintegration difficulties across all subdomains. All significant predictors were compared using Wald’s tests of parameter constraints to identify the strongest predictor of each subdomain. Due to the high number of pairwise comparisons, Bonferroni correction was applied to the alpha level (e.g., with seven significant predictors of interpersonal relationship difficulties, the alpha level was p = .05 / 21 = .002). Across all subdomains, a mental health diagnosis and being medically discharged were the strongest predictors. The regression coefficients for these two variables did not differ significantly from each other on any subdomain, except for Leisure, where the mental health diagnosis was a stronger predictor.
Results of the Multivariate Multiple Regression With Military Variables Predicting Different Subdomains of Community Reintegration.
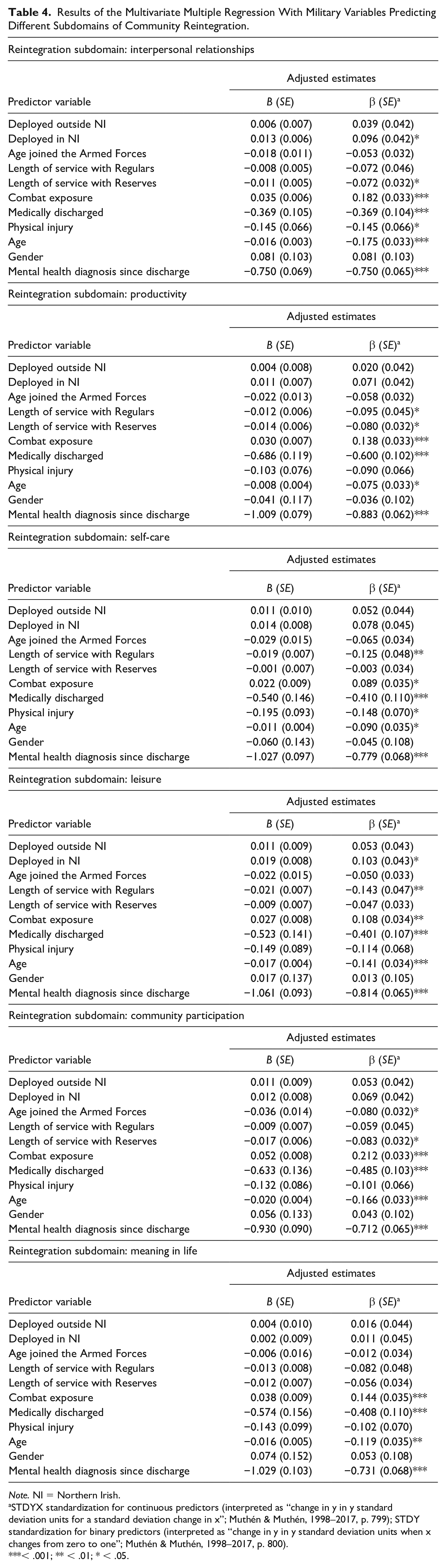
Note. NI = Northern Irish.
STDYX standardization for continuous predictors (interpreted as “change in y in y standard deviation units for a standard deviation change in x”; Muthén & Muthén, 1998–2017, p. 799); STDY standardization for binary predictors (interpreted as “change in y in y standard deviation units when x changes from zero to one”; Muthén & Muthén, 1998–2017, p. 800).
< .001; ** < .01; * < .05.
Discussion
In a bivariate correlation, age, age of enlistment, length of deployment in NI, length of service (Reserve Forces), and combat exposure were significantly associated with the total reintegration score. Participants who had been medically discharged, suffered physical injuries during deployment, and who had received a mental health diagnosis since discharge showed more total reintegration difficulties than participants without those experiences. In the multiple regression model, all variables except length of deployment outside NI were significant predictors of the total reintegration score in a dose–response relationship, with the experiences of having been medically discharged from service and having been injured in service as significant predictors of increased difficulties. In the adjusted model, the mental health diagnosis was the strongest predictor, with age (younger) also significant, but gender did not affect difficulties, and time spent deployed outside of NI was no longer a significant predictor. The adjusted model also explained more of the variance in total reintegration scores (37.3% vs. 20.4% unadjusted). In the exploratory multivariate multiple regression, receiving a mental health diagnosis since discharge and being medically discharged were the strongest predictors in the model, of comparable strength in 5 of the subdomains, with a mental health diagnosis being a stronger predictor for Leisure. Age (younger) and increased levels of combat exposure also predicted reintegration difficulties in all subdomains of the construct.
Reintegration difficulties surrounding interpersonal relationships were predicted by variables associated with physical/mental disability (medical discharge, physical injury, mental health diagnosis). This subdomain covered a spectrum of relationships from family/friends tp acquaintances/strangers. It is well established that the physical and mental health issues of veterans affect their family members, particularly intimate partners and children (Cramm et al., 2019; Diehle et al., 2016), frequently incorporating aspects of caregiver burden (Thandi et al., 2018). These relationships may be further strained by role reversal, as partners and children take on the roles of caregiver, with the veteran’s identity shifted away from one of protecting/providing and toward being cared for. Outside of the family, veterans may experience difficulties relating to friends, co-workers, and community members without military experience (Sayer et al., 2011) in addition to any social avoidance/withdrawal due to poor physical/mental health. As social support is vital to both better mental health outcomes (Laffaye et al., 2008; Sandoz et al., 2014) and community reintegration (Demers, 2011), difficulties in this subdomain may have a compound effect on overall reintegration and veteran mental health outcomes.
Combat exposure, medical discharge, and a mental health diagnosis were significant predictors of difficulties in Productivity, which focused on economic and personal productivity. Securing and maintaining employment is crucial to the reintegration process but numerous barriers exist, especially for the NI veteran population. Combat exposure is independently associated with PTSD (Hoge et al., 2004, 2006), which can negatively affect on employment outcomes (Smith et al., 2005). Individuals with a physical disability and/or mental illness face employment discrimination and lower recruitment numbers (Krupa et al., 2009; Russell, 2002; Stuart, 2006), as do older jobseekers (Roscigno et al., 2007), with NI veterans are more likely suffer these disadvantages (Ashwick & Murphy, 2017; Roy et al., 2020). In addition, systematic differences in culture between military and civilian employment can make adapting to/maintaining new employment difficult (Cooper et al., 2016; Minnis, 2020), leading to increasing feelings of alienation (Ahern et al., 2015; Roy et al., 2020). Employment is vital to maintaining personal economic stability and can be beneficial for individuals with mental illness (Dunn et al., 2008), meaning difficulties in Productivity can have far-reaching adverse effects.
Difficulties in Self-care were described by issues with maintaining personal hygiene, medication schedules, and eating/drinking and were predicted by a medical discharge and mental health diagnosis. Physical and mental health disabilities are well known to affect on an individual’s self-care, including physical inability to engage in self-care behavior (Bayliss et al., 2003; Fried et al., 1994) and lack of self-care agency due to mental illness (Çiftçi et al., 2015), especially when both physical disability and psychopathology are present (Ehrlich et al., 2017). Self-care agency has been linked to identity and self-concept (Smits & Kee, 1992), with incorporating of disability into personal identity associated with increased well-being (Forber-Pratt et al., 2017). The loss of their previous (potentially able-bodied/minded) military identity before transitioning to a civilian identity could precipitate an identity crisis whereby participants’ self-esteem was insufficient to drive self-care agency.
The Leisure subdomain could be ideologically grouped with Community Participation as it also details active engagement, potentially social engagement (Sayer et al., 2011). Difficulties here were predicted by a medical discharge and a mental health diagnosis and could function in a self-perpetuating cycle with less social activities resulting in increased isolation, social withdrawal, and decreased well-being, further decreasing the desire to engage. Karstoft et al. (2014) also found increased Leisure difficulties in delayed-onset and worsening PTSD trajectories. Failing to “enjoy free time” can also be applied on a personal level, indicating that participants with higher levels of difficulty not only avoided social Leisure but were also unable to enjoy solitary time as well.
Community Participation covered both active participation in community events and the feeling of belonging in a civilian community. Barriers to participation were predicted by combat exposure, medical discharge, and a mental health diagnosis. The civilian “community” is best conceptualized here using an ecological systems perspective (Bronfenbrenner, 1979), with the veteran’s friends/family closest to the center, and individuals/institutions of increasing interpersonal distance with less direct impact on the veteran’s day-to-day life. This system of concentric influence develops naturally in normal circumstances; however, the newly separated veteran is in the position of having to create their system as they build their civilian identity. As above, combat exposure is predictive of PTSD and in a longitudinal analysis of Danish soldiers who served in Afghanistan, increased levels of Community Participation difficulties were found among those with delayed-onset, mild distress, and worsening trajectories of PTSD symptomology in concert with the other subdomains of reintegration difficulties (Karstoft et al., 2014). PTSD symptomology is negatively associated with socialization (Hofmann et al., 2003; Sayer et al., 2009), as are many common psychopathologies (Elisha et al., 2006; Harvey & Brophy, 2011), and living with a medical condition/physical disability has also been associated with social withdrawal (Emerson et al., 2020). Lacking a “place” in the civilian ecosystem and dealing with significant difficulties, it is not surprising that veterans may socially disengage.
Finally, difficulty in finding Meaning in Life was predicted by combat exposure, medical discharge, and a mental health diagnosis. Searching for meaning in life is an endemic part of the human experience (Frankl, 1953; Miller, 2004) and can be conceptualized as an interplay between personal perception of identity, acknowledgment of the impermanent nature of existence, and the salience associated with ultimate acceptance of that identity (Steger et al., 2006; Thoits, 2012). Threat-to-life trauma has been shown to be predictive of PTSD (Holbrook et al., 2001) raising the possibility that confronting personal mortality in combat, in acceptance of long-term medical issues, and in the rumination of mental illness affects the process of finding meaning in life. As discussed previously, by separating from the military, veterans are forced into a shift in personal identity. Their military identity was codified by the chain of command and location within it, and they were defined by their use to the military, which provided meaning (Blais et al., 2009). After separation, civilian life may lack structure, and veterans with physical/mental health issues may experience the loss of the “usefulness” of their military identity, making finding meaning in their new civilian life more difficult.
Many of the significant predictors of community reintegration difficulties in NI veterans have established high rates of co-occurrence and inter-association. Veterans leaving service with physical health issues, especially injury, experience reintegration difficulties (Dillahunt-Aspillaga & Powell-Cope, 2018; Hawkins et al., 2015), particularly when several domains of functioning are affected (Resnik & Allen, 2007) as community reintegration is complicated by the process of the veteran adapting to their medical issues (McGarity et al., 2017). Service injuries are independently associated with PTSD (Grieger et al., 2006; Koren et al., 2005), as are length of deployment (Xue et al., 2015), and psychological distress/psychopathology (Stander et al., 2014). Receiving a mental health diagnosis since discharge affected all subdomains of reintegration, as many psychopathologies affect social interaction and/or increase social withdrawal (Shinn et al., 1984; Yanos et al., 2001). Younger age and shorter length of service were also significant predictors of reintegration difficulties, with early service leavers in the United Kingdom having been previously found to be younger age and at increased risk for PTSD and other adverse mental health outcomes (Buckman et al., 2013).
The results here are in line with the literature on community reintegration difficulties in a veteran population, but the unique circumstances of the NI veteran population compound these findings. This group is known to be disadvantaged compared with veterans in other parts of the United Kingdom (Ashwick & Murphy, 2017), in which several known variables predict reintegration difficulties, attempting to reintegrate into communities where their identities as veterans place them under threat (Roy et al., 2020). Although services are available to those who need help and who overcome stigma to engage with support, the veteran support sector in NI is smaller than in the rest of the United Kingdom (Armour et al., 2017). It is evident that NI veterans are increasingly disadvantaged in terms of community reintegration, a process where difficulties are associated with adverse, long-term outcomes (Sayer et al., 2011), deprived of the social support which proven to be beneficial to health and well-being (Langford et al., 1997; Vogt et al., 2021).
Limitations
The results here must be taken in line with the study’s limitations. Self-report data were used, carrying the risk of social desirability bias, especially when dealing with a socially sensitive topic (van de Mortel, 2008). Only 749 participants of the total 1,329 completed all of the measures required for these analyses, a difference of 43.6%, with possible explanations including the length of the survey and selective responses due to the nature of the study population. Due to the unique circumstances in NI, many in this population did not feel comfortable participating in data collection, yielding a study population far less than the estimated veteran population of NI, meaning this was not a representative sample of NI veterans. It is possible that the results here typify a specific subgroup associated with willingness to participate and disclose reintegration difficulties. Indeed, when conducting research of psychological well-being, multiple processes may be at work whereby those who have experienced any concerns around well-being are attracted to the survey but also those who are significantly distressed and thus have the poorest of wellbeing will be unable to engage. In addition, as these data have been collected specifically from the NI veteran population, differences in service-related experiences mean they may not be generalizable to the superordinate U.K. Armed Forces veteran population.
There are also several strengths associated with this work. While lacking data from the full study population, there were minimal missing data to accommodate (1.8%). Veterans provided information on physical injury and mental illness, including specific typology, thus while not assessed here, further nuanced analyses into type-dependant community reintegration difficulties remain a priority for future research. The scale used to assess community reintegration is a standardized measure with high reliability and validity, capturing the military to civilian transition with an easily replicable metric. Finally, data collected for the NIVHWS and utilized here represent the first instance of data collection in a U.K. Armed Forces veteran population resident in NI, who have been historically difficult to engage in research and who have often been ignored in higher level research due to the sensitivity and socio-political context of their service. This study and future research will allow the broader support community to understand NI veterans needs and tailor support programs accordingly.
Impact and Implications
It is clear that (a) community reintegration can be a difficult process for any veteran but especially for those with physical and mental health issues, (b) NI veterans face significant stigma, security concerns, and disadvantage when compared with other U.K. armed forces veterans, (c) service-related predictors for reintegration difficulties among NI veterans include higher levels of combat exposure, more time spent deployed in NI, shorter length of service, being medically discharged and having suffered a physical injury during service and importantly, (d) combat exposure, physical injury, a medical discharge, and a mental health diagnosis were significant predictors of subdomain-specific difficulties. Understanding the predictors of reintegration difficulties among NI veterans in both an aggregate and subdomain perspective can allow for tailored support programs based on veteran, family, and community needs. Support for a dedicated Veterans Centre was queried as part of the NIVHWS, with veterans and service providers largely in favor (Armour, Walker, et al., 2018). Recent initiatives have resulted in the creation of two localized veteran support locations (Cousins, 2021; Newsroom, 2021), the office of the Northern Ireland Veterans Commissioner, and elected Veterans Champions in local authorities (Kinahan, 2021).
The use of subdomain analysis here and in future research with this population can direct resources to areas of greatest need, including family support networks, employment reintegration training, self-care interventions, community and leisure events to allow veterans social opportunities without disclosing their veteran status, and even difficulty-specific counseling programs. Additional research is still urgently needed to determine the best methods of support and to design viable programs for use in NI, while future research is planned to address the specific relationships between predictors and difficulties and the impact of reintegration on veteran family members. Community reintegration is an important process in the lives of all veterans and difficulties can be moderated with intervention and support.
To conclude, multiple service-related variables predicted both general community reintegration and subdomain-specific reintegration difficulties in a NI veteran population, creating a roadmap of support need in the region. Discharge from military service is an ending for the soldier and a beginning for the veteran; the onus is on the military and support communities to ensure proper care and support for those who have served.
Footnotes
Appendix A: Adapted Combat Exposure Scale (Adapted From Keane et al.,1989 )
Please select the answer that best describes your experience in relation to your military service:
No 1–2 times 3–9 times 10–24 times 25+ times
No 1–2 times 3–9 times 10–24 times 25+ times
No 1–2 times 3–9 times 10–24 times 25+ times
Never 1–2 times 3–9 times 10–24 times 25+ times
Never 1–2 times 3–9 times 10–24 times 25+ times
Never 1–2 times 3–9 times 10–24 times 25+ times
Appendix B: Items,Subdomains,and Endorsement Percentages of the Military to Civilian Questionnaire
Items, Subdomains, and Endorsement Percentages of the Military to Civilian Questionnaire.
| Getting along with your child or children? | No difficulty | 346 | 51.3% |
| A little difficulty | 161 | 23.9% | |
| Some difficulty | 97 | 14.4% | |
| A lot of difficulty | 45 | 6.7% | |
| Extreme difficulty | 24 | 3.6% | |
| Not applicable | 2 | 0.3% | |
| Confiding or sharing personal thoughts and feelings? | No difficulty | 122 | 16.2% |
| A little difficulty | 156 | 20.7% | |
| Some difficulty | 138 | 18.3% | |
| A lot of difficulty | 171 | 22.7% | |
| Extreme difficulty | 167 | 22.1% | |
|
|
|||
| Finding or keeping a job (paid or nonpaid or self-employment)? | No difficulty | 398 | 60.0% |
| A little difficulty | 94 | 14.2% | |
| Some difficulty | 75 | 11.3% | |
| A lot of difficulty | 44 | 6.6% | |
| Extreme difficulty | 49 | 7.4% | |
| Not applicable | 3 | 0.5% | |
| Doing what you need to do for work or school? | No difficulty | 326 | 49.4% |
| A little difficulty | 144 | 21.8% | |
| Some difficulty | 89 | 13.5% | |
| A lot of difficulty | 49 | 7.4% | |
| Extreme difficulty | 48 | 7.3% | |
| Not applicable | 4 | 0.6% | |
| Taking care of your chores at home? | No difficulty | 346 | 45.9% |
| A little difficulty | 151 | 20.0% | |
| Some difficulty | 127 | 16.8% | |
| A lot of difficulty | 85 | 11.3% | |
| Extreme difficulty | 45 | 6.0% | |
|
|
|||
| Taking part in community events or celebrations? | No difficulty | 230 | 30.5% |
| A little difficulty | 165 | 21.9% | |
| Some difficulty | 127 | 16.9% | |
| A lot of difficulty | 122 | 16.2% | |
| Extreme difficulty | 109 | 14.5% | |
| Getting along with your child or children? | No difficulty | 346 | 51.3% |
| A little difficulty | 161 | 23.9% | |
| Some difficulty | 97 | 14.4% | |
| A lot of difficulty | 45 | 6.7% | |
| Extreme difficulty | 24 | 3.6% | |
| Not applicable | 2 | 0.3% | |
| Confiding or sharing personal thoughts and feelings? | No difficulty | 122 | 16.2% |
| A little difficulty | 156 | 20.7% | |
| Some difficulty | 138 | 18.3% | |
| A lot of difficulty | 171 | 22.7% | |
| Extreme difficulty | 167 | 22.1% | |
|
|
|||
| Finding or keeping a job (paid or nonpaid or self-employment)? | No difficulty | 398 | 60.0% |
| A little difficulty | 94 | 14.2% | |
| Some difficulty | 75 | 11.3% | |
| A lot of difficulty | 44 | 6.6% | |
| Extreme difficulty | 49 | 7.4% | |
| Not applicable | 3 | 0.5% | |
| Doing what you need to do for work or school? | No difficulty | 326 | 49.4% |
| A little difficulty | 144 | 21.8% | |
| Some difficulty | 89 | 13.5% | |
| A lot of difficulty | 49 | 7.4% | |
| Extreme difficulty | 48 | 7.3% | |
| Not applicable | 4 | 0.6% | |
| Taking care of your chores at home? | No difficulty | 346 | 45.9% |
| A little difficulty | 151 | 20.0% | |
| Some difficulty | 127 | 16.8% | |
| A lot of difficulty | 85 | 11.3% | |
| Extreme difficulty | 45 | 6.0% | |
|
|
|||
| Taking part in community events or celebrations? | No difficulty | 230 | 30.5% |
| A little difficulty | 165 | 21.9% | |
| Some difficulty | 127 | 16.9% | |
| A lot of difficulty | 122 | 16.2% | |
| Extreme difficulty | 109 | 14.5% | |
| Feeling like you belong in “civilian” society? | No difficulty | 235 | 31.1% |
| A little difficulty | 156 | 20.7% | |
| Some difficulty | 136 | 18.0% | |
| A lot of difficulty | 127 | 16.8% | |
| Extreme difficulty | 101 | 13.4% | |
|
|
|||
| Taking care of your health? | No difficulty | 264 | 35.0% |
| A little difficulty | 172 | 22.8% | |
| Some difficulty | 134 | 17.7% | |
| A lot of difficulty | 125 | 16.5% | |
| Extreme difficulty | 60 | 8.0% | |
|
|
|||
| Enjoying or making good use of free time? | No difficulty | 246 | 32.6% |
| A little difficulty | 189 | 25.0% | |
| Some difficulty | 126 | 16.7% | |
| A lot of difficulty | 139 | 18.4% | |
| Extreme difficulty | 55 | 7.3% | |
|
|
|||
| Finding meaning or purpose in life? | No difficulty | 238 | 31.5% |
| A little difficulty | 175 | 23.2% | |
| Some difficulty | 125 | 16.6% | |
| A lot of difficulty | 117 | 15.5% | |
| Extreme difficulty | 100 | 13.2% |
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.