
Abstract
Developmental theory indicates that success during a major life change requires attention to multiple life domains (e.g., physical health, mental health, employment, financial, and social). This study presents a revised conceptual framework and offers a new empirical model to assess the well-being of post-9/11 veterans as they transition to civilian life. Data from a large sample of post-9/11 veterans surveyed over 2.5 years revealed that post-9/11 veteran transitions were mixed: veterans improved over time in some domains (e.g., employment), stagnated in some (e.g., social), and struggled more over time in others (e.g., physical health). Even in domains with improvement, a large percent of veterans still struggled (e.g., 34% struggled with mental health at Wave 6). Moreover, certain groups tended to struggle more (e.g., enlisted, women, people of color). The conceptual framework and empirical model are intended to stimulate discussion on how best to understand, evaluate, and support veterans’ military-to-civilian transition.
As of 2021, there were an estimated 4.1 million post-9/11 veterans (United States Census Bureau, 2023). Every veteran goes through a military-to-civilian transition (MCT), which requires him or her to prepare to leave the military; re-orient to civilian life; adapt to civilian life; and, ideally, thrive over time (Blackburn, 2017; Robinson et al., 2017).
Several studies have examined MCT, and multiple frameworks have been posited (e.g., Blackburn, 2017; Castro et al., 2014; Thompson et al., 2016). However, no widely accepted framework or definition of MCT has been established, and an MCT timeline has not been consistently defined (Blackburn, 2017; Pedlar et al., 2019; Robinson et al., 2017). A guiding framework could promote MCT research, help community efforts that support veterans, help define outcomes (Robinson et al., 2017), make synthesizing literature and drawing conclusions easier, facilitate defining benchmarks for program development and evaluation, assist veterans in knowing when to seek additional help, and provide a common point of reference for policymakers. These efforts could, ultimately, improve veteran outcomes (Robinson et al., 2017). Furthermore, the lack of MCT theory hampers the ability to answer basic questions: What does a successful MCT look like? In everyday language, how do we know if a veteran is sinking, treading water, or swimming?
Military-to-Civilian Transition Framework
Although no widely accepted framework has been established, researchers have posited considerations for successful transition and components that should be included. Spiro et al. (2016) and Thompson et al. (2016) emphasize the life course nature of MCT. This perspective acknowledges that childhood and adolescent experiences influence later experiences, considers veterans’ experiences during their service, and includes postmilitary pathways to understand veteran outcomes in later life.
With wellness as the ultimate goal, Berglass and Harrell (2012) identified physical and psychological well-being as composite parts of overall veteran wellness. Here, well-being is comprised of positive personal relationships, health, fulfillment of material needs, and purpose. With the necessary supports in place, well-being does not require the absence of disease or injury and is possible regardless of service-connected challenges. For example, an individual with a service-connected disability can experience wellness when he or she has the supports and accommodations in place that enable him or her to accomplish daily tasks and life goals. Furthermore, veterans’ wellness must take into account several aspects of the military experience: (1) the long-term consequences of injury or illness, (2) the wide variety of social networks a veteran may have, (3) that veterans now need to attain material needs that were previously provided by the military, and (4) understanding that adapting to life after military service is a process and the veteran’s life may be different from the life he or she had before he or she joined the military (Berglass & Harrell, 2012).
Robinson et al. (2017) envision a holistic view of wellness and support. This conceptualization includes economic, physical, family, social, psychological, and cultural domains and proposes a “veteran support ecosystem” that consists of the individual; family; federal, state, and local government; community-based organizations; and private industry. Moreover, it is consistent with the U.S. Department of Veterans Affairs (VA) Whole Health Initiative (Department of Veterans Affairs, 2018), which emphasizes the many factors that impact wellness (e.g., personal development, surroundings, relationships, and activity).
Drawing from and building on previous conceptualizations (Berglass & Harrell, 2012; Pedlar et al., 2019; Robinson et al., 2017; Spiro et al., 2016; Thompson et al., 2016) and using a lifespan development perspective, we present the following modification to Robinson and colleagues’ indicators of progress toward successful transition (Table 1). This overarching framework suggests that pre-service experiences impact and interact with during-service influences to affect postservice outcomes. Postservice supports provided by federal, state, or local government; community organizations; faith-based organizations; and private industry, then, influence multiple short- and mid-term outcomes. For example, employment support may affect financial health and relationship satisfaction. In turn, numerous short-term outcomes will influence multiple mid-term outcomes. For instance, the short-term outcome of reduced mental health symptoms may impact mid-term outcomes of improved mental health, relationship satisfaction, and job attainment and satisfaction.
A Refined Framework for MCT.
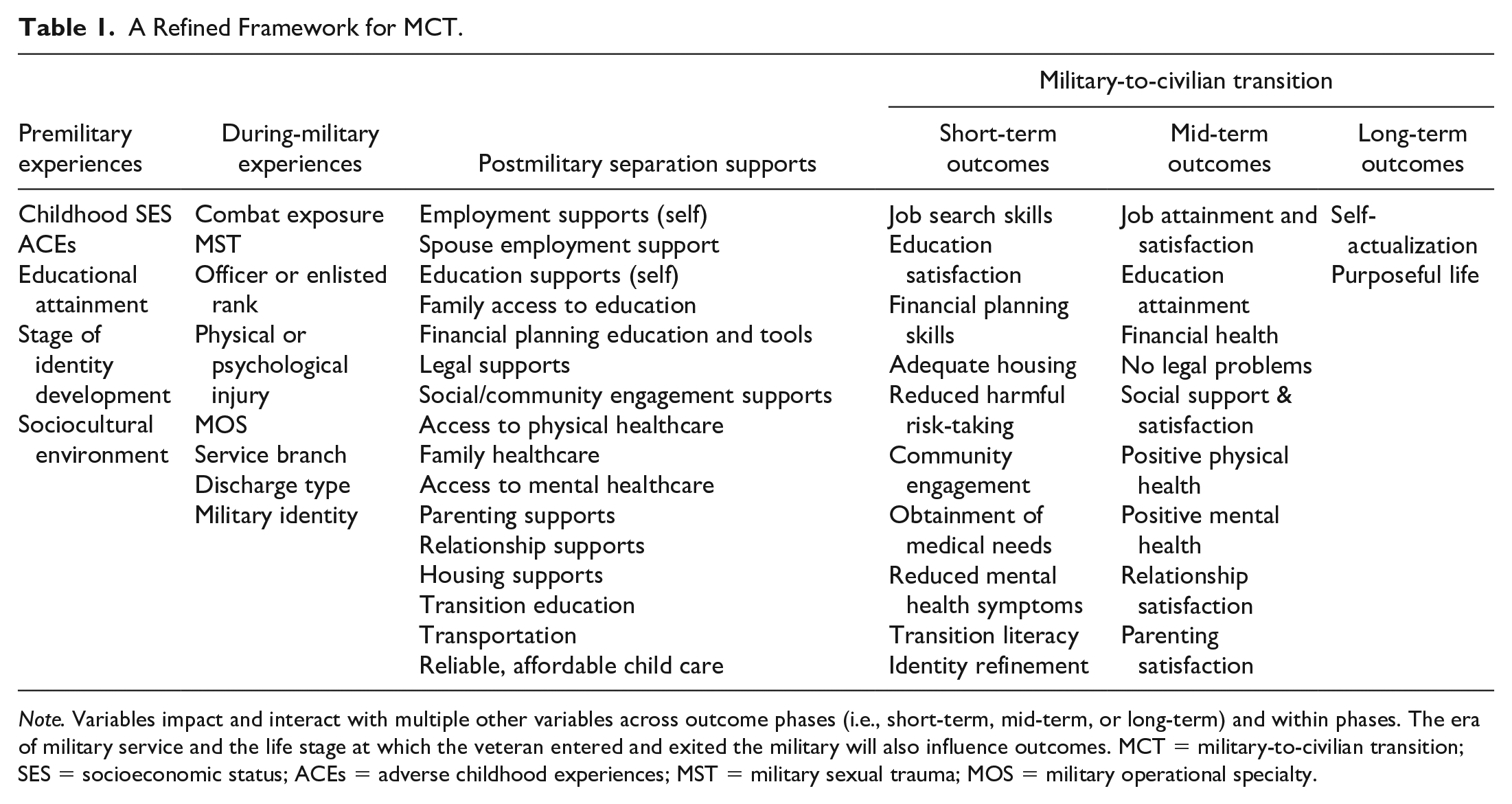
Note. Variables impact and interact with multiple other variables across outcome phases (i.e., short-term, mid-term, or long-term) and within phases. The era of military service and the life stage at which the veteran entered and exited the military will also influence outcomes. MCT = military-to-civilian transition; SES = socioeconomic status; ACEs = adverse childhood experiences; MST = military sexual trauma; MOS = military operational specialty.
Furthermore, outcomes within each outcome phase (i.e., short-term, mid-term, or long-term outcomes) will influence each other. For example, mid-term outcomes of employment attainment and financial health will likely be interrelated. Because human lifespan development includes both equifinality (i.e., where different previous experiences lead to similar subsequent outcomes) and multifinality (i.e., where similar previous experiences lead to different subsequent outcomes; Almy & Cicchetti, 2018) and because of the interrelation of outcomes at each outcome phase and between phases, developing a framework for MCT is complicated. Thus, a one-to-one relationship between supports and outcomes is not likely nor expected. That is, employment support may not only impact employment attainment but also impact financial health and relationship satisfaction. Conversely, employment support may not be enough to help one attain employment; mental health support may also be required.
Following the example of Bronfenbrenner’s ecological systems theory (Bronfenbrenner, 1979), this framework is an initial endeavor to tie together the many variables and multiple phases of a veteran’s life (e.g., premilitary service, during military service, and postmilitary service) that have previously been examined and which may impact the veteran’s transition to civilian life. Furthermore, as discussed by Dewey (1938) when outlining the importance of theory, this framework is not intended to be examined as a whole, but to provide a “map” (p. 136) that may be useful as researchers consider variables that may be important to include in their investigations. Due to the complex nature of this framework, and the varied nature of veterans’ experiences, it is not intended to be final or all-inclusive; it is meant to be a building block, and further refinement must follow.
Data-Driven Conceptualization for Successful Military-to-Civilian Transitions
Focusing on the short- and mid-term outcomes listed in the overarching framework in Table 1, which were drawn from previous research (e.g., Berglass & Harrell, 2012; Robinson et al., 2017; Spiro et al., 2016; Thompson et al., 2016), we put forth an initial conceptualization of what a successful transition might look like by using the longitudinal data collected as part of The Veteran Metrics Initiative (TVMI). The original data collection for TVMI tracked veterans from their military separation to nearly 3 years after separation (Vogt et al., 2018). The TVMI survey was completed every 6 months. These data captured, over time, how military-to-civilian transitions unfolded for a representative sample of post-9/11 veterans at three time points: within the first 3 months after separation (Wave 1), 12 to 15 months after separation (Wave 3), and 30 to 33 months after separation (Wave 6).
Two principles guided this conceptualization of a successful MCT and the individual items that were selected for inclusion. The first principle specified that success must be theoretically achievable for everyone. For example, physical fitness requirements would need to be achievable for individuals who have a physical disability. In addition, structural, institutional, and individual barriers to achieving some transition goals likely exist. Thus, the expectation that all veterans will do equally well in each life domain is unrealistic. Therefore, we sought to create transition goals that should be achievable for everyone. Still, we acknowledge the existing barriers that may make achieving the goals more difficult for some people.
The second principle was that the MCT conceptualization had to be free of value judgments. As noted in the VA’s Whole Health approach (United States Department of Veterans Affairs, 2022), people have different goals and aspirations. For example, one person may want to pay their rent by driving for Uber at night and, therefore, have daytime hours free to pursue hobbies, volunteer, or start a business. Another person may want to be the CEO of a large company. Thus, individuals make life choices that make sense for them. Hence, a conceptualization of successful transitions must be free of value judgments around what a typical transition is “supposed to” look like. Relatedly, items were not included if the meaning of the item could be drastically different for different individuals. For example, the item, How often have you gotten along well with relatives other than your significant other or children?, was excluded because some individuals may choose to sever ties with abusive relatives to maintain their own and their family’s well-being.
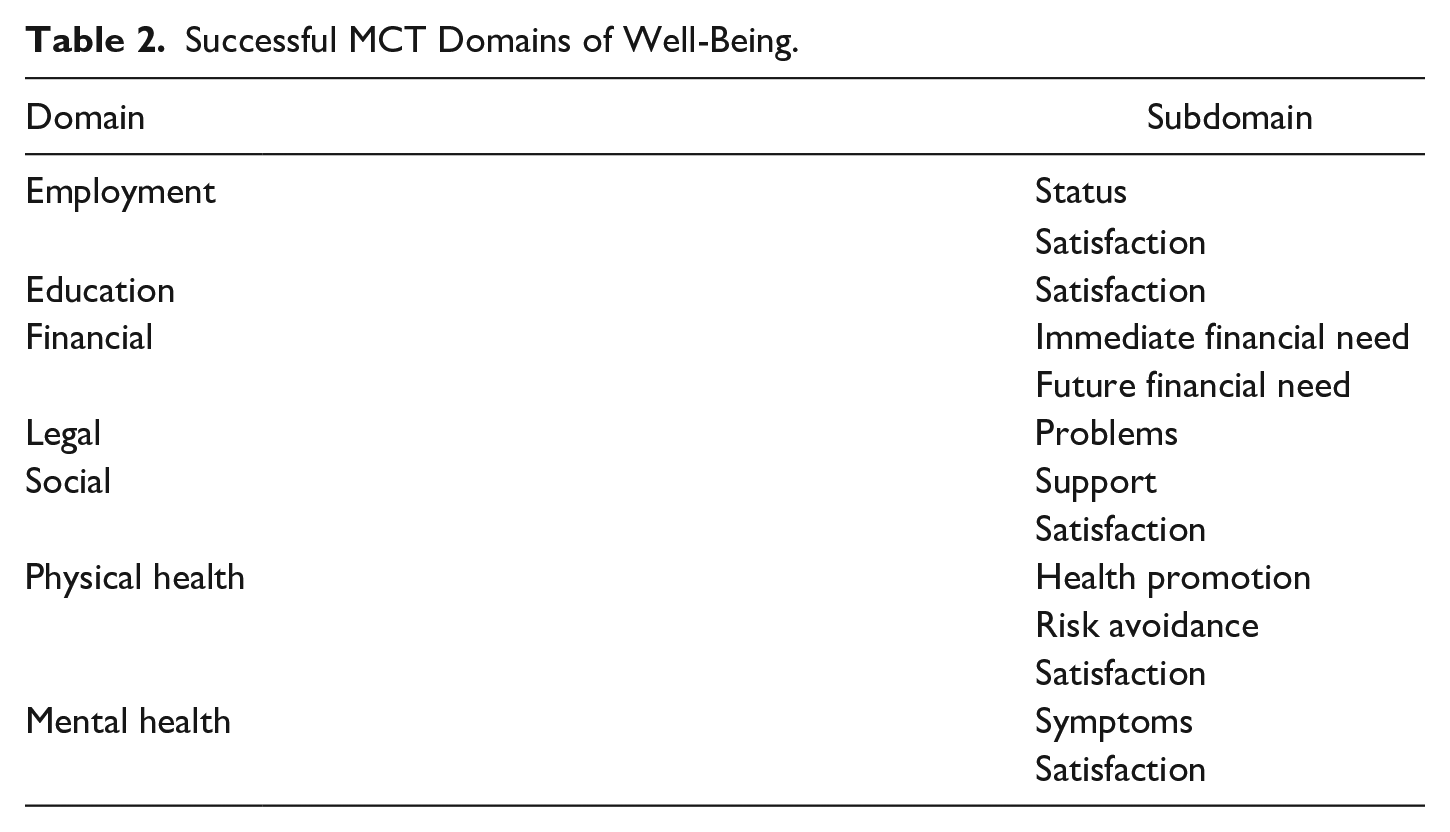
In this conceptualization of MCT, objective items were used when possible as they are largely free from bias (e.g., one either exercised for an hour or one did not exercise for an hour). However, examining veterans’ subjective values and sentiments is also important for measuring success as their voice needs to be an active part of their definition of success. Subjective assessments (e.g., satisfaction with one’s pay and benefits) allow for including important factors without inserting a value judgment by benchmarking the response (e.g., to be successful, one has to make $100,000 per year). Furthermore, researchers would not be able to capture every variable that may be important to a veteran’s MCT. Therefore, including broad satisfaction questions (e.g., How satisfied have you been with your physical health) allows participants to consider factors beyond those explicitly asked when assessing their well-being. Self-reporting subjective factors also provides insights into an individual’s internal experience, thoughts, feelings, and facets of life that often cannot be observed. Examining life domains using both objective and subjective data can provide rich data. For instance, research has shown that self-perceptions of underemployment are positively associated with turnover intentions and negatively associated with job satisfaction and psychological health (Liu & Wang, 2012; Luksyte & Spitzmuller, 2011; Wilkins & Wooden, 2011). Therefore, a veteran who is employed (i.e., generally perceived as successful), but is unhappy in the job, may require specific interventions and services to increase the likelihood of his or her successful transition. Seven well-being domains used to assess successful MCT within the TVMI data were identified (see Table 2).
Successful MCT Domains of Well-Being.
Methods
Participants
Participants were a representative sample of U.S. military veterans who separated or were deactivated from active-duty service within the prior 90 days between May and September of 2016. All 48,965 veterans who separated or were deactivated during this time period were identified using the VA/Department of Defense Identity Repository. Potential participants learned about the study via mailed postcards and letters. Monetary incentives for participation were provided via gift cards. Data were collected from participants at 6-month intervals over approximately 2.5 years, and six waves of data were collected. Additional details about the sampling approach have been previously published (Vogt et al., 2018). Data from Waves 1, 3, and 6 were used for this study.
At Wave 1, 18% of respondents were female; 82% were male. Sixty-five percent were white non-Hispanic; 11% were black non-Hispanic; 14% were Hispanic; 5% were Asian, Pacific Islander, or Hawaiian non-Hispanic; 4% were more than one race; 1% reported their race as “other.” With regard to paygrade, 28% were E1–E4; 30% were E5–E6; 18% were E7–E9; 2% were W1–W5; 8% were O1–O3; 14% were O4 and above. Thirty-three percent separated from the Army; 19% separated from the Navy; 19% separated from the Air Force; 16% separated from the Marine Corps; and 13% were deactivated from activated status in the National Guard or Reserves. Sample sizes across waves and by domain are presented in Table 3.
Sample Sizes and Demographics for Waves 1, 3, and 6.
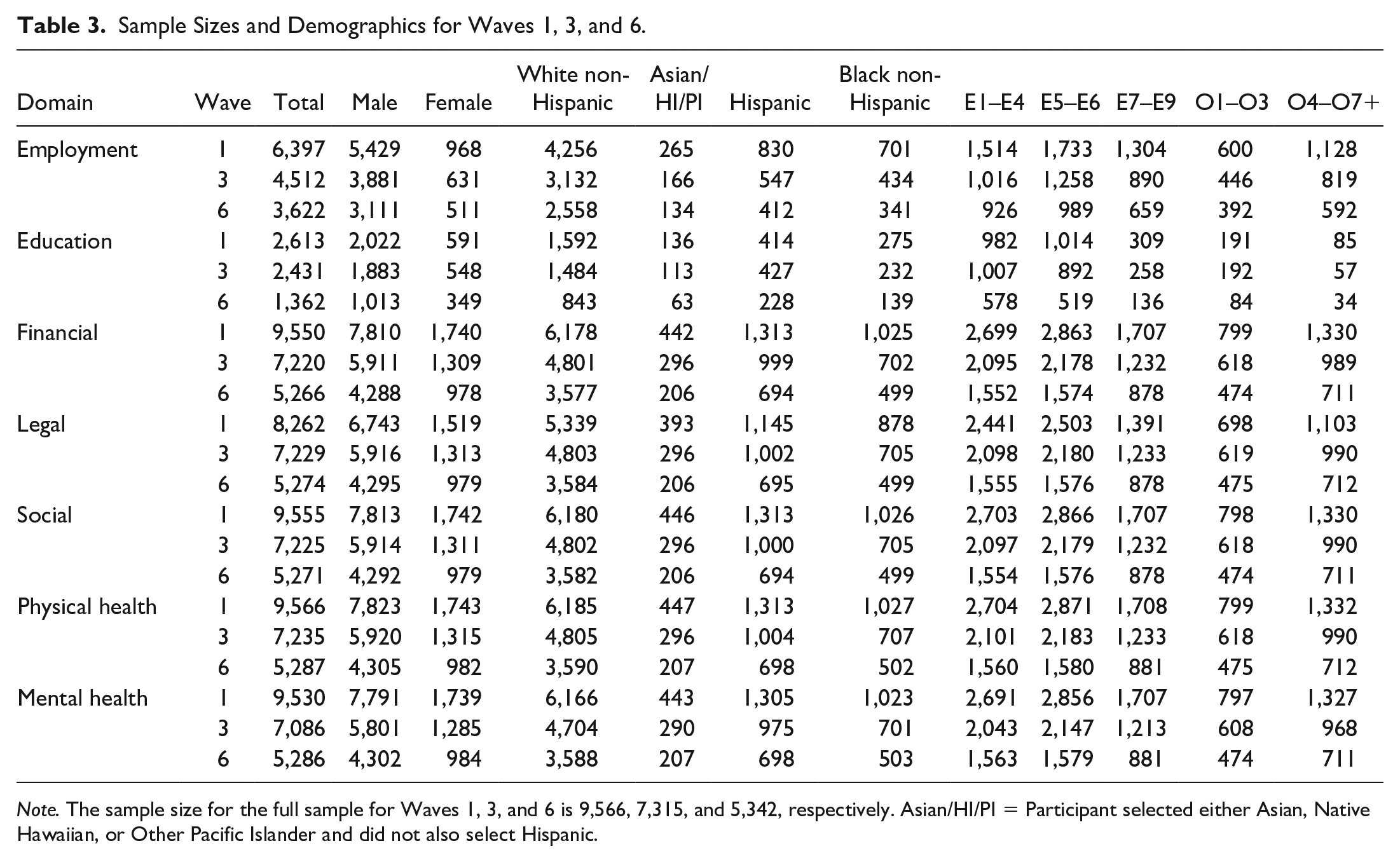
Note. The sample size for the full sample for Waves 1, 3, and 6 is 9,566, 7,315, and 5,342, respectively. Asian/HI/PI = Participant selected either Asian, Native Hawaiian, or Other Pacific Islander and did not also select Hispanic.
Measures
Guided by the above-mentioned framework and principles, we combined items from the TVMI questionnaire 1 (Vogt et al., 2019) and created subdomains. Subdomains were then combined into domains (i.e., employment, financial, social, physical health, mental health, education, and legal). Subdomain and domain scores were decided at the item level, as opposed to scale scores, and purposely conservative for this initial conceptualization. For example, for the subdomain satisfaction questions, to receive the highest score (i.e., 2), all responses had to be somewhat satisfied or very satisfied. When one or more response was neither satisfied nor dissatisfied and the remaining were satisfied, the subdomain score was at the midpoint (i.e., 1). If any subdomain item was somewhat dissatisfied or very dissatisfied, the subdomain score was the lowest (i.e., 0). The subdomains that inquired about frequency were similarly coded. The mental health symptoms subdomain scores were based on whether participants reported symptoms: no symptoms (i.e., 2), symptoms but did not meet criteria for probable anxiety, depression, or PTSD (i.e., 1), and met criteria (i.e., 0). The final domain score was created similarly: Successful required a 2 on all subdomains, At Risk required 1 and 2 on all subdomains, and Problematic was assigned if any subdomains scores were 0. Missing data was handled differently depending on the meaning, or potential meaning, of the missing data. For a participant to receive a subdomain score of 1 or 2 or a domain score of At Risk or Successful, all items and subscales required a response or score. This was purposely conservative to ensure that a 1 or 2 subdomain score or a Successful or At Risk domain score was not assigned to a participant who would have received a 0 subdomain score or Problematic domain score had they completed the items. Because only one item was needed to qualify for a 0 subdomain score or a Problematic domain score, missing items were allowed for those scores. The domains, subdomains, items, response options, and transition category coding are available in Table 4.
Successful Transition Conceptualization Variable Development.
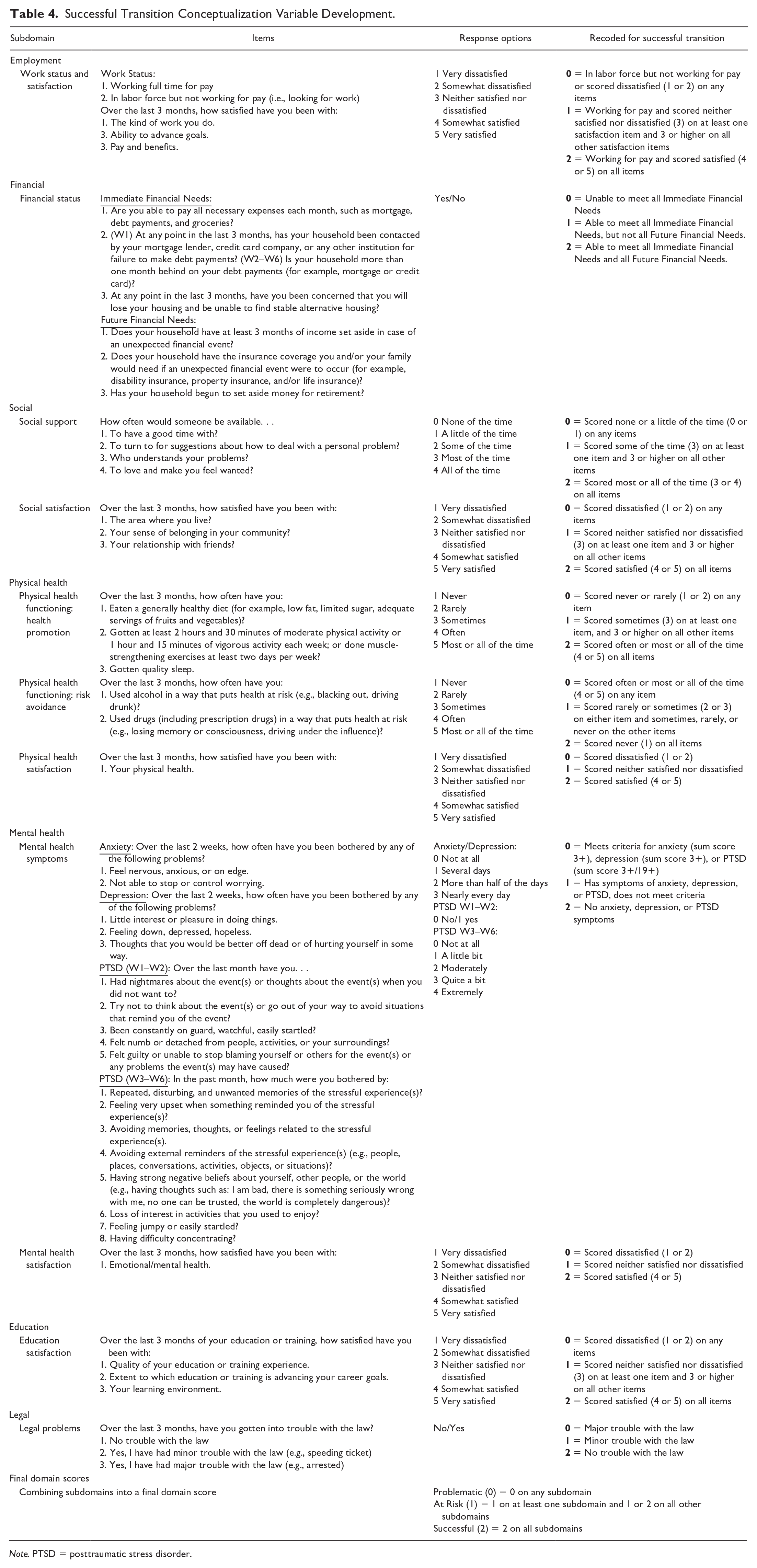
Note. PTSD = posttraumatic stress disorder.
In addition to the inclusion and coding decisions presented in Table 4, several other decisions were made regarding the variables. First, three groups of participants did not receive a score in the employment domain: individuals who were not in the labor force; full-time students as they may have different employment goals than individuals who are not full-time students (e.g., their job may be a source of income while in school but not related to their vocational goals); and individuals who were working part-time because whether respondents were working part-time by choice or because they could not find a full-time job could not be determined. Second, education completion was not used to measure success in the education domain because Wave 6 of the TVMI study was completed 2.5 years after separation. Many individuals may not have had enough time to complete their education goals. Third, a subjective measure of financial satisfaction was not included in the financial domain as in other domains. The relationship between income, one’s perception of whether he or she has an adequate income, and financial satisfaction is complicated and influenced by many disparate factors such as the symbolic meaning one puts on money and comparisons to one’s past self and others (Gasiorowska, 2015; Grable et al., 2013).
Based on available data and potential policy implications, composite scores were created (i.e., the number of domains for which a veteran was classified as successful, at risk, or problematic). These composite scores were intended to provide insight into the overall well-being of veterans as opposed to looking at each domain individually. The likelihood of an individual, veteran or not, being successful in all domains at the same time is likely small. Examining the number of Successful, At Risk, and Problematic domains individuals have may provide additional insight into veterans’ transition. The legal and education domains were excluded from the composite scores. There was minimal variability in the legal domain (i.e., very few veterans reported legal programs). The education domain was excluded because individuals often sacrifice “success” in one or more domains (e.g., financial) to pursue an education as they hope education will help them succeed in multiple domains later. Therefore, while pursuing an education, a perceived lack of success in various domains may simply be an individual engaging in delayed gratification. As such, the education domain will be better understood as an individual domain than part of a composite score.
Results
Employment Domain
For the employment domain, at Wave 1, 46% of the respondents fell into the problematic transition category, and 41% fell into the successful category (see Table 5). By Wave 6, 28% of the respondents were in the problematic category, and more than 50% were in the successful category. In terms of employment status at Wave 1, 29% were looking for work, 41% were working full-time and were satisfied, and 30% were working full-time but were dissatisfied or neither satisfied nor dissatisfied on at least one employment satisfaction item. By Wave 6, only 7% of those respondents who were in the labor market were looking for work. However, 40% were working but reported being dissatisfied or neither satisfied nor dissatisfied on at least one employment satisfaction item.
Domain and Subdomain Scores Over 2.5 Years.
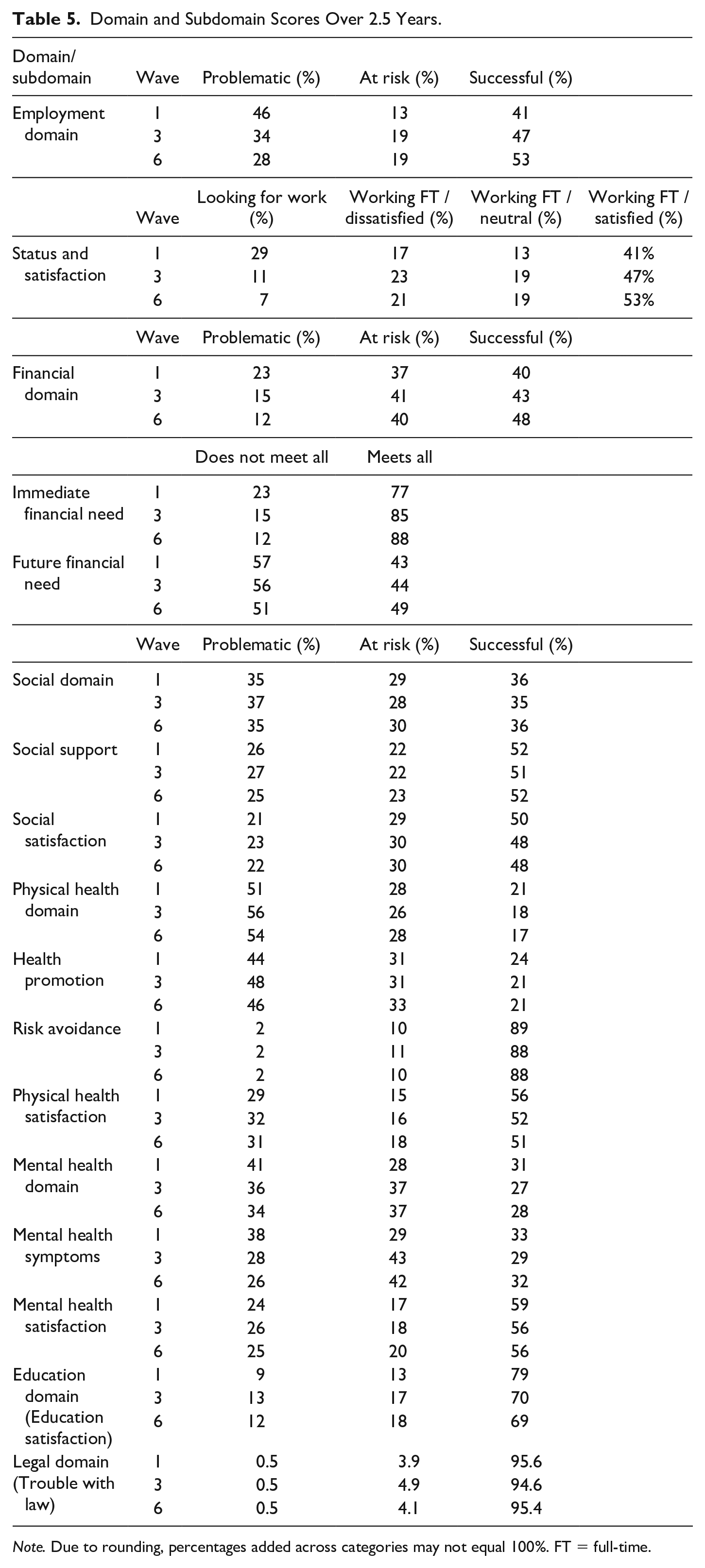
Note. Due to rounding, percentages added across categories may not equal 100%. FT = full-time.
Financial Domain
At Wave 1, 23% of veterans fell into the problematic transition category for the financial domain, while 40% were successfully transitioning (Table 5). By Wave 6, the percentage of veterans who were in the problematic category fell to 12%, and the percentage of veterans who were successfully transitioning rose to 48%. At each of the three time points examined, approximately 40% were in the at risk category. In terms of the subdomain of immediate financial need, at Wave 1, nearly one-quarter of veterans reported not being able to meet all of their immediate financial responsibilities. In contrast, just over three-quarters reported being able to meet all of their immediate financial needs. By Wave 6, 12% reported being unable to meet their immediate needs, while nearly 90% could meet all immediate financial needs. There was minimal movement in the transition success of veterans over time concerning items related to meeting future financial needs. A slight majority (51%–57%) consistently did not endorse all items associated with meeting future financial needs. Conversely, between 43% and 49% of veterans did endorse all items related to future financial needs.
Social Domain
Overall, success in the social domain did not change between Wave 1 and Wave 6 (see Table 5). Approximately one-third of veterans reported being in each transition category (i.e., problematic, at risk, and successful). There was also little change in the subdomain of social support. Over time, about one-quarter of veterans fell into the problematic category of transitioning, one-quarter fell into the at risk category, and 50% were successfully transitioning in terms of social support. Social satisfaction did not change over time, and approximately 20% of veterans fell into the problematic category, 30% fell into the at risk category, and 50% fell into the successful category at each of the three examined waves.
Physical Health Domain
There was very little movement between Wave 1 and Wave 6 regarding physical health during transition (see Table 5). At both time points, just over half of the veterans fell into the problematic category, almost 30% were at risk, and close to 20% were successful. In terms of health promotion, the proportions of veterans who fell into each category changed very little over time. Almost 50% fell into the problematic category, one-third were at risk, and 20% were successful. Risk avoidance also did not change over time, and 2% of the veterans fell into the problematic category, approximately 10% fell into the at risk category, and nearly 90% fell into the successful category. Physical health satisfaction became slightly worse over time. There were slight increases in veterans who fell into the problematic and at risk categories (i.e., an increase from 29% to 31% for problematic and 15% to 18% for at risk categories between Wave 1 and Wave 6), and there was a decrease in the percentage of veterans who fell into the successful category between Wave 1 and Wave 6 (i.e., from 56% to 51%).
Mental Health Domain
At Wave 1, 41% of respondents fell into the problematic category for the mental health domain (Table 5). However, by Wave 6, this proportion dropped to 34%. During the same period, the proportion of veterans in the at risk category increased from 28% at Wave 1 to 37% at Wave 6. There was also a slight decrease in the proportion of veterans in the successful category (i.e., from 31% at Wave 1 to 28% at Wave 6). Regarding mental health symptoms, there was a decrease in the proportion of veterans in the problematic category (i.e., from 38% at Wave 1 to 26% at Wave 6). However, there was a substantial increase in the proportion in the at risk category (i.e., from 29% at Wave 1 to 42% at Wave 6). Approximately 30% of veterans fell into the successful category for symptoms across the three examined waves. Mental health satisfaction remained largely unchanged. About 25% of veterans were in the problematic category, near or at 20% were in the at risk category, and almost 60% were in the successful category across the three time points.
Education Domain
Most veterans were in the successful category in the education domain (see Table 5). However, there were some changes over time. Just under 10% of veterans were in the problematic category at Wave 1, and just over 10% were in the problematic category at Wave 6. Thirteen percent of participants were in the at risk category at Wave 1 and 18% at Wave 6. Although 79% of veterans were in the successful category for the education domain at Wave 1, 69% were in the successful category at Wave 6.
Legal Domain
There was very little change across time in the legal domain (see Table 5). Very few veterans (0.5%) had major trouble with the law or minor trouble with the law (4%–5%). The vast majority (95%–96%) reported no trouble with the law over all three examined time points.
Composite Variable
After examining each individual domain, a composite variable was created that included five domains: employment, 2 financial, social, physical health, and mental health. The composite variable was the number of domains for which participants were categorized as successful, at risk, and problematic. Regression analyses were conducted to examine the association between gender; race/ethnicity; paygrade; and the number of successful, at risk, and problematic domains endorsed by veterans. As seen in Table 6 at Wave 1, 35% of the respondents had three or more problematic categories across the five domains. At Wave 6, 25% of veterans had three or more problematic categories. Conversely, 31% of veterans had three or more successful domains at Wave 1, and 34% had three or more successful domains at Wave 6.
Composite Variable Proportions by Category and Wave.
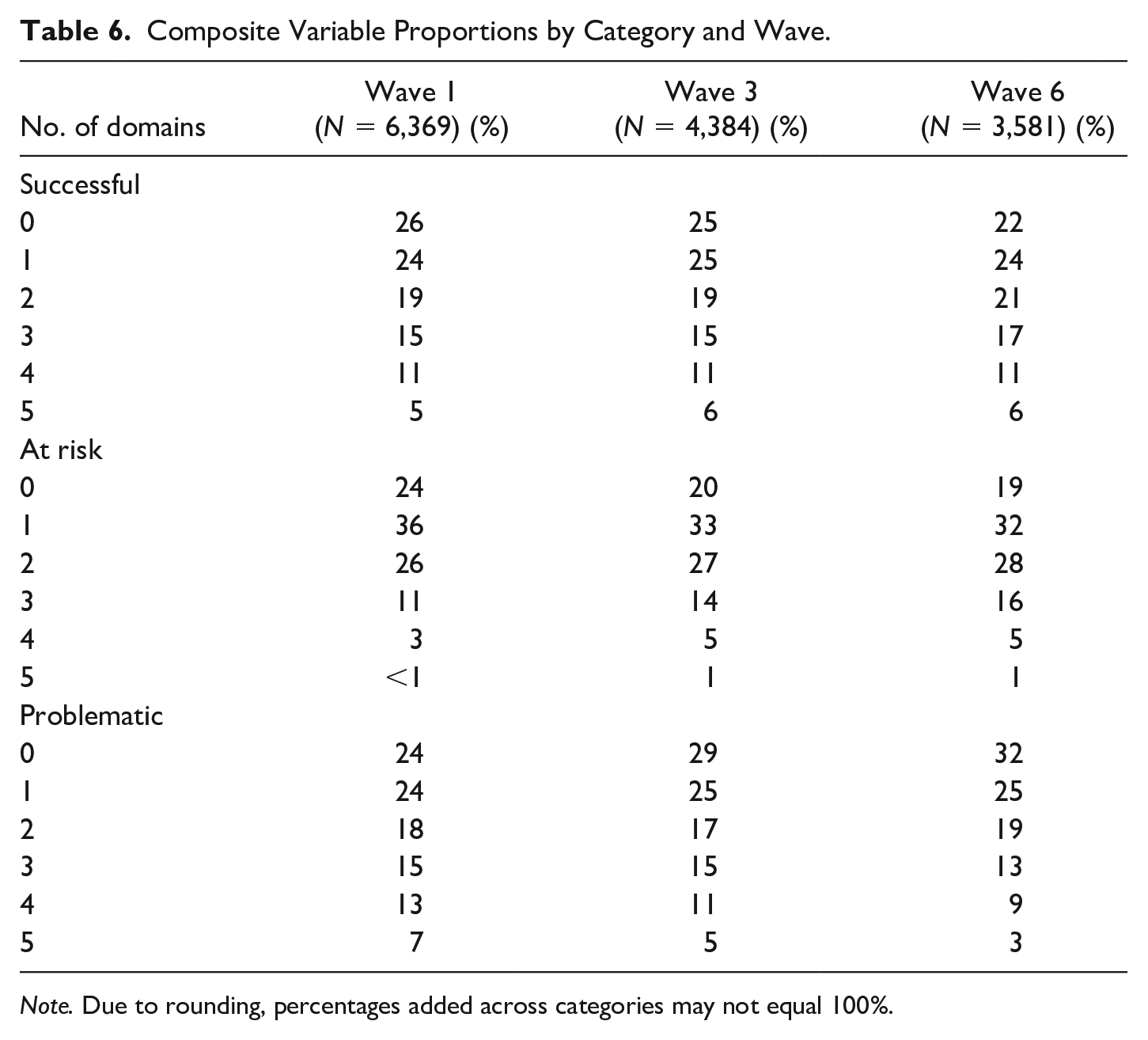
Note. Due to rounding, percentages added across categories may not equal 100%.
As shown in Table 7, higher paygrade, as opposed to lower, at separation was consistently associated with having fewer problematic domains (W1 ß = −.242, p < .001; W3 ß = −.202, p < .001; W6 ß = −.181, p < .001) and more successful domains (W1 ß = .292, p < .001; W3 ß = .257, p < .001; W6 ß = .236, p < .001). Among the variables included in the model (i.e., paygrade, race, and gender), paygrade also had the strongest association with the number of problematic and successful domains. Being Black non-Hispanic and Hispanic, as compared to White non-Hispanic, were consistently associated with having fewer successful domains (Black non-Hispanic W1 ß = −.107, p < .001; Black non-Hispanic W3 ß = −.075, p < .001; Black non-Hispanic W6 ß = −.071, p < .001; Hispanic W1 ß = −.079, p < .001; Hispanic W3 ß = −.076, p < .001; Hispanic W6 ß = −.043, p = .011) and more problematic domains (Black non-Hispanic W1 ß = .126, p < .001; Black non-Hispanic W3 ß = .089, p < .001; Black non-Hispanic W6 ß = .093, p < .001; Hispanic W1 ß = .085, p < .001; Hispanic W3 ß = .077, p < .001; Hispanic W6 ß = .053, p = .002). However, this association was not as strong as the association with paygrade. Finally, being female was associated with having more problematic domains (W1 ß = −.045, p < .001; W3 ß = −.068, p < .001; W6 ß = −.064, p < .001).
Association Between Race and Ethnicity, Gender, and Paygrade and the Number of Successful, At Risk, and Problematic Domains.
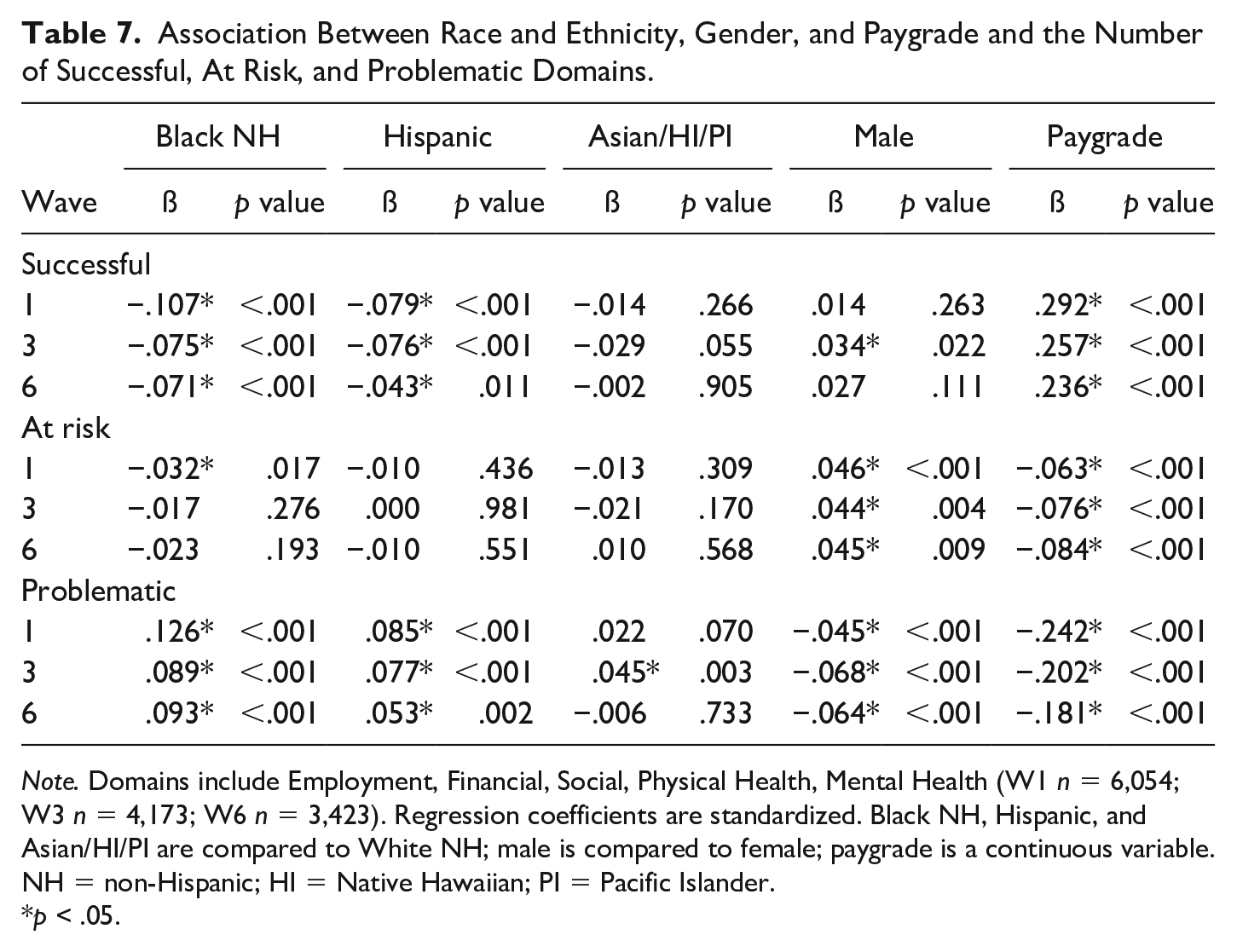
Note. Domains include Employment, Financial, Social, Physical Health, Mental Health (W1 n = 6,054; W3 n = 4,173; W6 n = 3,423). Regression coefficients are standardized. Black NH, Hispanic, and Asian/HI/PI are compared to White NH; male is compared to female; paygrade is a continuous variable. NH = non-Hispanic; HI = Native Hawaiian; PI = Pacific Islander.
p < .05.
Discussion
This study developed an overarching framework for MCT based on previous work (Berglass & Harrell, 2012; Pedlar et al., 2019; Robinson et al., 2017; Spiro et al., 2016; Thompson et al., 2016) and incorporated a lifespan development perspective. Further, based on the overarching framework, a conceptual model for evaluating the extent to which individuals make successful transitions from active-duty military to civilian life was proposed. Based on the framework, the conceptual model focuses on several critical well-being domains that have been identified in prior research on the health and well-being of veterans. The conceptual model includes domains and subdomains of functioning, and individual transitions will likely differ. MCT, like other transitions, presents opportunities for early prevention and intervention that put people on a pathway to success rather than waiting until individuals falter or spiral in a negative direction. By using this model, professionals can periodically assess veterans to help determine where they are thriving and where they might need assistance. Government services, community-based organizations, and private industry are available in many communities that can then provide early services related to challenges identified in these assessments before they become larger problems (e.g., homelessness).
Using the conceptual model proposed in this article, we examined the degree to which post-9/11 veterans were making successful MCTs across seven life well-being domains. In the employment domain, nearly half of the veterans fell into the problematic transition category, and less than half were successful when surveyed within the first 3 months of leaving the military. Approximately 2.5 years later, the proportion of veterans who fell into the problematic category declined substantially to 28%, and the proportion of those in the successful category increased to 50%. This finding suggests that many veterans may not leave the military with a job lined up, but employment challenges that are inherent early in transition do decline over time for many veterans. Indeed, early in transition, 30% of post-9/11 veterans were looking for a job, but, approximately 2.5 years later, only 7% were looking for employment. However, even though veterans successfully obtained employment, a substantial minority of veterans were either dissatisfied or at least not fully satisfied with their current job. Given recent research related to veteran underemployment suggesting that veterans are more likely to be underemployed than civilians and that there are differences in veteran underemployment based on paygrade (Barrera & Carter, 2017; Davenport et al., 2022), future research should investigate veterans’ employment trajectories after their separation from the military. These investigations should include examining the extent to which veterans change jobs in the years after their separation, the reasons for the job changes (e.g., poor fit, needing a temporary job to make ends meet while looking for a different job), and whether job changes lead to improved success in the employment domain including increased work satisfaction. In addition, programs or supports for veterans that specifically address underemployment may be beneficial in that they could encourage veterans to pursue jobs aligned with their skills and interests, help veterans translate their military skills adequately, and help fill any gaps in training needed for their civilian career.
By 2.5 years after separation, 88% of veterans reported that they were able to meet all immediate financial needs. This finding is consistent with the increase in the percentage of veterans who find employment in the first 2.5 years after separation. However, about 1 in 10 veterans were still unable to meet their immediate financial needs at 2.5 years. Thus, additional research is needed to explore why some veterans still struggle in the financial domain. Research could examine what co-occurring factors are present (e.g., employment difficulties, mental health challenges) and could determine what supports and programs could be impactful. At 2.5 years post separation from the military, just under half (49%) of the veterans are preparing for future financial needs (i.e., 3-month income saved, insurance obtained, and contributing to retirement). However, this finding is consistent with the general population. In 2019, the same year as Wave 6 data were collected, 37% of Americans reported that they could not pay for an emergency expense of $400 (Board of Governors of the Federal Reserve System, 2022).
In the social domain, the proportion of veterans in each transition category remained flat over time, and only half of the veterans were categorized as successful. Multiple factors in the social domain may help facilitate a healthy transition to civilian life. For example, social support is associated with better mental health and higher life satisfaction (Adams et al., 2017; Siedlecki et al., 2014). Veterans who are in the at risk or problematic transition category for the social domain may benefit from programs that make community connections through volunteering, joining veteran organizations, or attending peer-support groups (Drebing et al., 2018).
The physical health of veterans during the MCT is a concern. Compared to civilian peers, veterans generally have poorer physical health and are more likely to have cardiovascular disease (Hoerster et al., 2019). In addition, newly separated veterans are less satisfied with their health than they are in other domains (i.e., work, intimate relationships, and social; Vogt et al., 2020). Other studies have shown that many post-9/11 veterans do not engage in positive health promotion behaviors, such as not smoking (Hoerster et al., 2012) and getting sufficient sleep (Nguyen et al., 2023). The findings in this study are consistent with the previous research. Indeed, the low proportion of veterans in the successful category for physical health was largely driven by being in the problematic category in the health promotion subdomain (i.e., eating a healthy diet, exercising, and getting quality sleep). These factors are largely behavioral and modifiable. A comprehensive focus on modifiable health-promotion behaviors in veterans should be undertaken by using various interventions such as initiating social norms campaigns, providing health-promotion and health-education opportunities, and offering support groups. Nearly 40% of post-9/11 veterans do not use the VA (United States Department of Veterans Affairs, 2017), and many veterans do not seek programmatic assistance from any source (Aronson et al., 2019); thus, innovative government and community initiatives may be needed to reach veterans in need.
Transitioning veterans’ mental health, that is, their symptoms and their satisfaction with mental health, also deserves further attention. Two-thirds of the veteran respondents reported mental health challenges early in their transition to civilian life; however, these struggles may not have risen to the level of clinical significance. The early identification of mental health difficulties could result in addressing challenges before they reach a clinical level. Another reason to pay close attention to mental health during MCTs is that there is a significant help-seeking stigma among veterans (Michalopoulou et al., 2017) both related to how veterans think others will perceive them for seeking help (e.g., others thinking less of them) and how they perceive themselves for seeking help (e.g., feeling inferior; Skopp et al., 2012). Furthermore, post-9/11 veterans report more barriers to receiving mental health care (e.g., appointment times conflict with work, negative attitudes toward mental health care, and attitudes of self-reliance) than veterans of other eras (Garcia et al., 2014). Significant efforts to engage transitioning veterans around mental health challenges at various time points could help prevent severe mental health problems from developing and reduce the associated negative repercussions that these problems may have in the employment, financial, legal, and education domains.
More than three-fourths of veterans who pursued education reported that they were satisfied with the quality of their education, their learning environment, and how their education advanced their career goals. However, satisfaction appeared to decrease somewhat over time; at Wave 6, 69% of veterans reported being satisfied with all three indicators. Therefore, campus programs intended to help veterans navigate the transition and provide community and support could benefit veteran students. Indeed, veterans who use veterans’ centers or participate in veteran-student organizations are more likely to attain a degree and are more likely to attain that degree within 4 years of separation from the military than those who did not use these services (Morgan et al., 2023). Some veterans may prefer veteran-related programming or groups, whereas others may prefer programs that help them integrate into the campus community (DiRamio et al., 2008). Therefore, offering a variety of programs may be beneficial.
Very few veterans in our sample reported trouble with the law. When they did, it was likely minor trouble with the law, such as speeding tickets. At each three examined waves of data collection, less than 1% of veterans reported experiencing major trouble with the law, such as being arrested.
The results of this study indicate that veterans from the enlisted ranks are more likely to experience difficulty during the MCT. There may be numerous and confounding factors that influence this. For example, on average, veterans from the enlisted ranks have less education when they separate from the military (Morgan et al., 2023) and earn less money than officers did while serving (United States Department of Defense, 2023). Therefore, enlisted veterans, on average, may not emerge from their military service with the financial or educational resources that officers do. In addition, without a college degree or civilian technical school training, which civilian employers easily understand, enlisted veterans may need additional assistance in translating their military experiences into the language of marketable skills in the civilian workforce. Furthermore, when veterans from enlisted ranks obtain employment after separation, they are more likely to report being underemployed (Davenport et al., 2022). Thus, multipronged and focused transition assistance programs that focus on veterans from the enlisted ranks should be initiated while they are still serving (Castro et al., 2019) and should continue throughout the transition process. Veterans of color and female veterans also appear more likely to struggle during MCTs; therefore, targeted transition support may also be helpful for these individuals. Future studies should investigate the degree to which targeted programs are having their intended effects by examining programs’ acceptability, cultural sensitivity, rate of adoption, and quality of program delivery.
This new conceptualization of veterans’ successful transitions to civilian life was primarily undertaken to initiate discussions among theorists, researchers, veterans, providers, and policymakers. Because the TVMI data were not collected specifically to examine this conceptualization of successful transitions, this study has several limitations. First, we were constrained by the existing survey questions. For example, it would have been helpful to ask veteran respondents how successful they felt in their transition using a mixed methods approach—qualitative and quantitative data collection. Second, the survey was subject to limitations that affect many large, longitudinal studies (e.g., limited items to promote participant completion and retention). Third, there may be different or better questions that could have been asked to better understand the domains of well-being. Fourth, additional domains not included in the current conceptualization or the original survey may be important to consider when thinking about a successful transition from military to civilian life. Fifth, the posttraumatic stress disorder (PTSD) measure was changed after Wave 2, which may impact the interpretation of the mental health domain. Sixth, these data were collected from a specific cohort of veterans who separated from military service within a specific time period in 2016. Thus, the findings may not be broadly generalizable to post-9/11 veterans.
Many variables likely impact an individual’s MCT. Three demographic variables were selected as a starting point and were examined in this study. Additional potential variables to incorporate into analyses related to MCT can be found in the framework in Table 1 and include, but are not limited to, adverse childhood experiences, educational attainment, military sexual trauma, discharge type, parent status, military identity, geographical location and community size, and community engagement. Furthermore, additional columns may need to be added to the framework in Table 1. Researchers should consider the role of postmilitary experiences (e.g., where veterans reside post separation [e.g., near their last duty station, near their family of origin, somewhere new]) and the role of the broader external environment (e.g., how service members and veterans are represented in social media and mass media) as veterans are transitioning out of the military.
Additional indicators of a successful MCT should also be examined. Parenting and romantic relationship constructs were originally considered for these analyses. However, as there were multiple variables for which not everyone would have responses (e.g., education, employment, romantic relationships, parenting), a decision was made to limit this type of variable to only employment and education. This helped simplify the analyses and preserve the sample size. However, these will be important variables to consider in future research. Researchers should also consider the utility of including these variables in terms of predicting a successful transition or as outcomes of a successful transition. Finally, variables related to relationships with family of origin (e.g., How satisfied have you been with your relationships with relatives other than your significant other or children?) were initially considered for the social domain. However, given that some individuals choose to sever ties with their families of origin to preserve their well-being, these questions may not have the same meaning to all participants. Further examination of these more complicated questions is needed.
Further, whether the categorization rationale utilized in this new conceptualization is accurate, reliable, or valid is not clear. The criteria used in several domains may be considered too conservative. For example, to be classified as having a successful employment transition, respondents could not endorse any dissatisfaction with their current employment. Similarly, to be classified as having a successful transition related to mental health, the participant needed to report zero anxiety, depression, or PTSD symptoms, as asked in the survey items. Thus, this conceptualization may be too stringent. 3 Future studies should examine a possible categorization that can provide a more nuanced account.
The current conceptualization assumes that there are commonalities across veterans when evaluating the success of the transition to civilian life. However, each veteran likely has his or her view of what a successful transition constitutes, and he or she may weigh domains differently when considering his or her own transition. Future qualitative, quantitative, and mixed methods studies could disentangle how veterans may value domains differently as they consider their transition challenges and successes.
These analyses examined how the participants were faring as a group at each time point. Future analyses should investigate individual trajectories to examine how individuals transition between categories over time. Some veterans may smoothly move from the problematic category, to the at risk category, to the successful category. Others may start in the successful category and move to the at risk category. Still others may vacillate between categories over time.
Finally, future studies should consider analyses that can improve the current conceptualization of successful transition. For example, analyses of convergent validity within domains and discriminant validity between domains, and an exploration of the hierarchical structure of the model should be conducted. Over time, this conceptualization will need to be refined, tested, and revised. Finally, comparable civilian data are lacking for several of these domains. For example, many veterans struggled with the physical health domain, specifically engaging in health promotion activities. However, these struggles may be no different than those that civilians encounter and, thus, may not provide the evidentiary support needed to conceptualize a successful transition. Thus, future studies should identify appropriate civilian data for comparative studies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Heinz Endowments (THE) under grant #E8181. The Veterans Metrics Initiative (TVMI) research was managed by the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc. (HJF), and it was collaboratively sponsored by the Bob Woodruff Foundation, Health Net Federal Services, HJF, Lockheed Martin Corporation, Marge and Philip Odeen, May and Stanley Smith Charitable Trust, National Endowment for the Humanities, Northrop Grumman, Prudential, Robert R. McCormick Foundation, Rumsfeld Foundation, Schultz Family Foundation, The Heinz Endowments, U.S. Department of Veterans Affairs Health Services Research and Development Service, Walmart Foundation, and Wounded Warrior Project, Inc. The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of any of the sponsor organizations listed.