
Abstract
Moral reconation therapy (MRT) is one form of cognitive-behavioral treatment that has been implemented in institutionalized settings to rehabilitate justice-involved individuals. However, the efficacy of this program in reducing recidivism has not been widely assessed for people on federal probation. This study collected data on 1080 people on probation from one federal district. Half of the participants (n = 540) had participated in MRT, while the other 540 participated in probation-as-usual. Contrary to much of the extant literature on MRT, results from this study indicate that participation in MRT does not significantly reduce the likelihood of recidivism. Individuals who participated in MRT and did not complete it had a higher likelihood of recidivism relative to those who were under probation-as-usual. In addition, individuals who successfully completed MRT did not have a lower likelihood of recidivism relative to those under probation-as-usual.
Over the past three decades, the population of incarcerated individuals in the United States has increased by 500% (Vogel, 2012). On a downturn after peaking at over 3.3 million incarcerated individuals (Minton et al., 2021), there were still more than 1.2 million individuals incarcerated in the United States in 2021 (Carson, 2022). However, of all justice-involved individuals under some form of correctional supervision, people on probation were the majority group in 2009 (58%; 4,199,800) and in 2019 (55%; 3,492,900; Minton et al., 2021).
Federal probation has served as an alternative to incarceration for justice-involved individuals since its inception in 1925 (Federal Probation Act, 1925). In addition, with growing legal, fiscal, and social challenges related to mass incarceration in the United States, the utilization of probation as a rehabilitation-focused alternative to traditional “tough on crime” sentences has widely expanded (Alexander & VanBenschoten, 2008; Glaze, 2011). In adherence with their “Principles of Good Supervision,” federal probation officers should aim to provide purposeful, individualized, proportional, multidimensional, proactive, and responsive supervision for their supervisees (Probation and Pretrial Services, 2023a). Therefore, people on probation who receive “Good Supervision” should more easily reintegrate into society, satisfying the goals of federal probation services to (a) reduce recidivism (i.e., reoffending) and (b) protect the public (Alexander & VanBenschoten, 2008; Probation and Pretrial Services, 2023a).
Effective recidivism reductions through federal probation services should reduce the strain prisons and jails face while maintaining public safety. For instance, Cochran et al. (2014) compared recidivism between justice-involved individuals on probation and those who were incarcerated, finding that 31% of individuals in the probation group recidivated while 35% of individuals in the jail group recidivated.
To increase the efficacy of federal probation at reducing recidivism, treatment programs that utilize cognitive-behavioral therapy have been widely employed in attempts to change patterns of dysfunctional thinking (and thus, major risk factors for recidivism such as impulsivity and self-control) in people on probation (Probation and Pretrial Services, 2023b). One form of cognitive-behavioral adjunct therapy that has been widely adopted across different contexts, but has not been assessed within the population of people on federal probation, is moral reconation therapy (MRT). Thus, this study aims to examine the efficacy of MRT in reducing recidivism in a sample of people on federal probation.
MRT: Basics
MRT was created by Gregory Little and Kenneth Robinson of Correctional Counseling, Inc., in 1985 as a response to the lack of effective treatment for “resistant” client populations including those who are identified as at least one of the following: (a) diagnosed with a substance use disorder, (b) of a minority population, (c) of low socioeconomic status, (d) has current or past history of mental health diagnoses, (e) has prior criminal offenses, or (f) has antisocial personality disorder (Little et al., 2010; Little & Robinson, 1988). The overarching goal of MRT is to improve conscious decision-making and moral reasoning through education and proper socialization in these resistant populations (Blonigen et al., 2018; Little & Robinson, 1988).
MRT is a step-by-step program that is completed in twelve weeks (Little & Robinson, 1988). Self-reflection on past actions and decisions is a significant part of therapy, and members are encouraged to change their ineffective decision-making strategies (Little & Robinson, 1988). Members are given take-home exercises to be completed before next week’s meeting, at which they present in front of the group (Little & Robinson, 1988). At this point, the other group members determine if the individual has passed the current step in treatment, and if the vote is affirmative, then the individual can move on to the next step (Little & Robinson, 1988). Another important aspect of MRT is volunteering, which encourages participants to give without expecting to receive something in return (Little & Robinson, 1988).
Thus, MRT is one form of rehabilitation that can potentially reduce society’s costs and the adverse effects of the prison system on justice-involved individuals. Notably, few other forms of treatment incorporate cognitive-behavioral therapy and directly target “resistant” client populations, and those that do exist are time-consuming and costly (Little & Robinson, 1988). On the other hand, MRT can be easily adapted to different treatment providers, settings, and client needs (Little & Robinson, 1988).
MRT: Prior Research on Recidivism
Several studies, mostly connected to Correctional Counseling, Inc. (e.g., Little et al., 1991, 1993, 1994, 1999) have examined the effectiveness of MRT in reducing recidivism in justice-involved populations. For example, Little and colleagues (1991) treated 70 males who committed drug offenses with MRT during and after incarceration. These individuals were reassessed for recidivism 38 months after their release and were compared to a control group of 82 justice-involved males. In the MRT-treated group, the recidivism rate was 24.3% while the control group had a much higher rate of 36.6%. Furthermore, the completed steps of MRT were significantly correlated with recidivism.
A 20-year follow-up on all participants previously recruited by Little et al. compiled rearrest and reincarceration data on 1,052 MRT-treated and 329 control participants (Little et al., 2010). More than half of the former MRT participants (60.8%) had been reincarcerated at least once after release; however, 81.8% of control participants had been reincarcerated at least once. Rearrest rates followed similar patterns, with 81.2% of MRT-treated participants having one or more rearrests after release, while 93.6% of the control group had at least one rearrest.
Applying MRT to a different population, Blonigen et al. (2022) examined the efficacy of MRT in reducing recidivism in a sample of 341 justice-involved patients admitted to a mental health residential treatment program. Patients were randomly assigned to either usual care or usual care with two MRT group sessions each week. Follow-ups conducted after 6 and 12-months revealed that, on most outcomes (e.g., substance use severity, criminal thinking, employment), patients in both conditions tended to improve across time; however, MRT did not significantly differ from usual care in reducing recidivism in this population.
Armstrong (2002, 2003) examined the effects of MRT on youth who were incarcerated in a county jail. Subjects randomly assigned to the treatment group were housed in a Youth Offender Unit, where they were enrolled in MRT. In contrast, control participants were housed in the general population. Although methodological concerns arise due to confounds within the study design (i.e., subjects housed in the Youth Offender Unit received additional benefits that general population subjects did not), placement in the Youth Offender Unit (and therefore, participation in MRT) appeared to increase minor disciplinary violations (Armstrong, 2002) and did not significantly reduce the risk of recidivism (Armstrong, 2003) relative to the general population group.
Some researchers have examined the effects of MRT on people on probation. In New Mexico, one group of adults on probation (n = 146) completed MRT as part of their sentencing in Drug Court. While 15.7% of drug court graduates had a rearrest within 18 months, only 11% of the MRT graduates were rearrested (Whitehead, 2003). Wakefield and Cameron (2011) assessed the entire population of one federal probation office in Omaha, Nebraska for over one year. MRT participants (n = 117) and unmatched controls (n = 113) were assessed on rearrests after six months and one year. Findings show that MRT participants who successfully completed the program (n = 19) showed no rearrests after six months or one year; however, MRT participants who had not yet completed the program (n = 98) and control participants displayed rearrest rates at an increase of 2.5 times relative to the six months. These findings suggest that participants must successfully complete MRT to show the benefits of this program in terms of recidivism.
Meta-Analyses and Methodological Assessments of MRT
Additional research has been conducted on extant MRT studies’ larger reliability and methodological strength. Allen et al. (2001) performed a “quality-based review” of the effectiveness of MRT and Reasoning and Rehabilitation, a similar program, at reducing recidivism. Although the authors conclude that both programs appear to be successful at reducing rates of recidivism, they note that methodological weaknesses of the included studies make any reliable conclusions difficult, mainly because many studies followed the same group of participants over time, lacked random assignment or matched control groups, and/or failed to control for potentially confounding variables.
Ferguson and Wormith (2012) conducted a meta-analysis of 33 separate studies of MRT with a trim-and-fill method (to account for publication bias, given the influence of Little et al. on studies assessing the efficacy of MRT). Nineteen of the studies (59%) included used nonequivalent, unmatched control groups, and the majority (59%) were published in a journal owned by Correctional Counseling, Inc. Regardless, there was a small but significant effect size (r = .16) over a total sample of 30,259, evidencing an influence of MRT on recidivism such that individuals who participated in MRT recidivated at two-thirds the rate of control participants (Ferguson and Wormith, 2012).
Most recently, Harrell et al. (2023) conducted a scoping review of MRT, including only peer-reviewed empirical studies published in English between 2011 and 2021. Of 145 articles screened, 30 studies quantitatively assessed feelings toward program implementation or sustainability and/or failed to assess the unique influence of MRT on client outcomes. Most articles screened merely mentioned MRT and did not empirically assess the program. Finally, six articles were reviews, commentaries, or editorial articles. Overall, no empirical articles met the search criteria after screening. This contradicts claims made by Correctional Counseling, Inc. about the “evidence-based” efficacy of the program on client outcomes and highlights a need for more in-depth assessment of commonly used interventions.
Similarly, a group of researchers from the Washington State Institute for Criminal Justice (WSICJ) sought to rank programs following a risk-needs-responsivity model for the Washington Department of Corrections (Campbell et al., 2018). The authors utilized operational definitions of “evidence-based,” “research-based,” and “promising practices” to rank programs, as agreed upon by WSICJ, the Washington State Institute for Public Policy, and the definitions utilized in extant Washington State legislature. Perhaps unsurprisingly, MRT was classified as a “promising practice,” failing to meet the more rigorous methodological thresholds for evidence-based and research-based programs (Campbell et al., 2018).
Considering the mixed findings and methodological weaknesses of previous studies assessing MRT, an unbiased effort to evaluate the efficacy of MRT using a sample of people on federal probation with (a) an equivalent control group and (b) longitudinal data are necessary to further this body of research and its applicability to different offending populations.
Risk Factors for Recidivism
Eight risk factors have been identified as strongly correlated with criminal behavior: (a) a history of engaging in antisocial conduct; (b) personality characteristics that predispose one to antisocial behavior; (c) cognitive patterns marked by antisocial thought processes; (d) associations with peers who exhibit antisocial traits; (e) difficulties or conflicts with family or marital relationships; (f) challenges at school or work; (g) problems experienced during leisure or recreation; and (h) patterns of substance use (Andrews & Bonta, 2006, 2010). These risk factors, commonly referred to as the “Central Eight,” are unique in that they include both dynamic (flexible) and static (fixed) aspects of risk. The Central Eight have been heavily associated with recidivism in offending populations within the United States; for instance, adults (Gendreau et al., 1996), juveniles (Baglivio et al., 2018; Guebert & Olver, 2014), and those with mental illness (Bonta et al., 1998, 2014; Morgan et al., 2010). Outside of the United States, the Central Eight have also been found to correlate with recidivism. In an international systematic review including studies from five different countries, focusing on justice-involved individuals given community sentences, Yukhnenko et al. (2020) found that static risk factors for this population include prior criminal history, younger age, non-White race, being male, and low levels of education. Dynamic risk factors identified include low socioeconomic status, mental health concerns, problems with employment, interactions with antisocial peers, and marital status (Yukhnenko et al., 2020).
In addition, many risk assessment tools utilized in the United States incorporate the static and dynamic risk Central Eight factors (e.g., COMPAS, STRONG-R; Brennan et al., 2004, 2007, 2009; Hamilton et al., 2016). The Post Conviction Risk Assessment (PCRA) is a measure developed by the Administrative Office of the U.S. Courts. It is used to determine the level of risk for individuals under community supervision (Administrative Office of the United States Courts, 2018). The PCRA incorporates a number of the Central Eight risk factors: substance use, criminal history, employment, social networks, marital status, and motivation to change, as well as more general static factors, including age, education level, and biological sex (Johnson et al., 2011). Numerous studies have evaluated the PCRA and have found it to be a valid predictor of re-arrest for individuals under supervision (e.g., DeLisi et al., 2018; Lowenkamp et al., 2013, 2015).
Static risk factors outside the Central Eight have also been associated with recidivism. For example, a special report from the Bureau of Justice Statistics on prisoner recidivism in 30 states over nine years confirmed that most individuals who were rearrested after initial release were male, younger in age, non-White, and had an initial nonviolent commitment offense (Alper et al., 2018). A 2016 report published by the United States Sentencing Commission also found higher rates of rearrest for individuals who had low levels of education, were younger in age, male, and non-White (Hunt & Dumville, 2016).
As previously discussed, most extant research assessing the efficacy of MRT does not account for variables that may further impact the risk of recidivism. Blonigen et al. (2022), in their assessment of MRT for justice-involved individuals admitted to a mental health residential treatment program, did include participant age, sex, and race as covariates in models, but excluded substance use and employment as covariates to use as secondary outcome measures instead.
Therefore, in addition to accounting for the methodological weaknesses identified by reviews and meta-analyses of MRT literature, this study accounts for the impact of well-established static and dynamic criminogenic risk factors on the relationship between participation in MRT and reductions in recidivism.
Research Questions and Hypotheses
The present research aims to answer the following questions related to the efficacy of MRT at reducing recidivism in a sample of people on federal probation. For all research questions, recidivism is measured with three outcomes: (a) any new charges after the start of treatment, (b) time to new charge after the start of treatment, and (c) charge rate after the start of treatment. Charges include federal felonies and misdemeanors. A 2-year (730-day) follow-up period is utilized for the first two outcomes, beginning at each individual’s last supervision start date. For charge rate, due to unreliable last charge dates for this sample, a 2-year standardized rate was employed instead of simply counting charge frequency (see Analytic Strategy).
Are there differences in recidivism between MRT participants and controls?
As an exploratory analysis, the present research also aimed to answer a follow-up question:
How might MRT participants who are successful in the program the first time they enter it differ on the measures of recidivism relative to control participants?
Method
Participants
Our sample consists of 540 people on probation consecutively enrolled in MRT in one federal district and 540 people partaking in probation-as-usual, in the same federal district (N = 1,080; 17.8% female). Among MRT participants, 291 (53.9%) successfully completed the program, and 249 (46.1%) did not complete MRT. Successful MRT participants, or “completers,” pass through all twelve steps of the program. Unsuccessful MRT participants, or “noncompleters,” are those who either (a) missed more than three sessions and were involuntarily terminated, (b) committed another violation which led to involuntary termination, or (c) voluntarily withdrew from the group (Wakefield & Cameron, 2011). In this district, MRT group facilitators are federal probation officers. There are no formal criteria for eligibility, as individual probation officers determine the requirement to complete MRT (Wakefield & Cameron, 2011).
Individuals in this sample were, on average, under supervision for 1,863.51 days (SD = 1,400.47, Range: 31 – 7,184) and, at the first date of supervision, were charged with an average of 1.18 charges (SD = 1.79, Range: 0 – 13). Relatively few individuals (n = 67, 6.2%) were charged with at least one petty crime, while nearly one-third (32.9%) were charged with at least one misdemeanor (n = 355), and just under 30% were charged with at least one felony (n = 304). The average age of all individuals at the start of supervision was 33.19 (SD = 8.42, Range: 19 – 63), with a mean PCRA risk score of 9.49 (SD = 3.21, Range: 0 – 18). Most individuals were African American (n = 547, 50.6%) or White (n = 510, 47.2%), followed by Asian American (n = 12, 1.1%), Native American (n = 10, 0.9%), or some other race (n = 1, 0.1%). Many individuals were employed while on probation (n = 661, 61.2%), and just over half had no history of current or past mental health conditions (n = 572, 53.0%). See Table 1 for characteristics by the overall group.
Characteristics by Overall Group
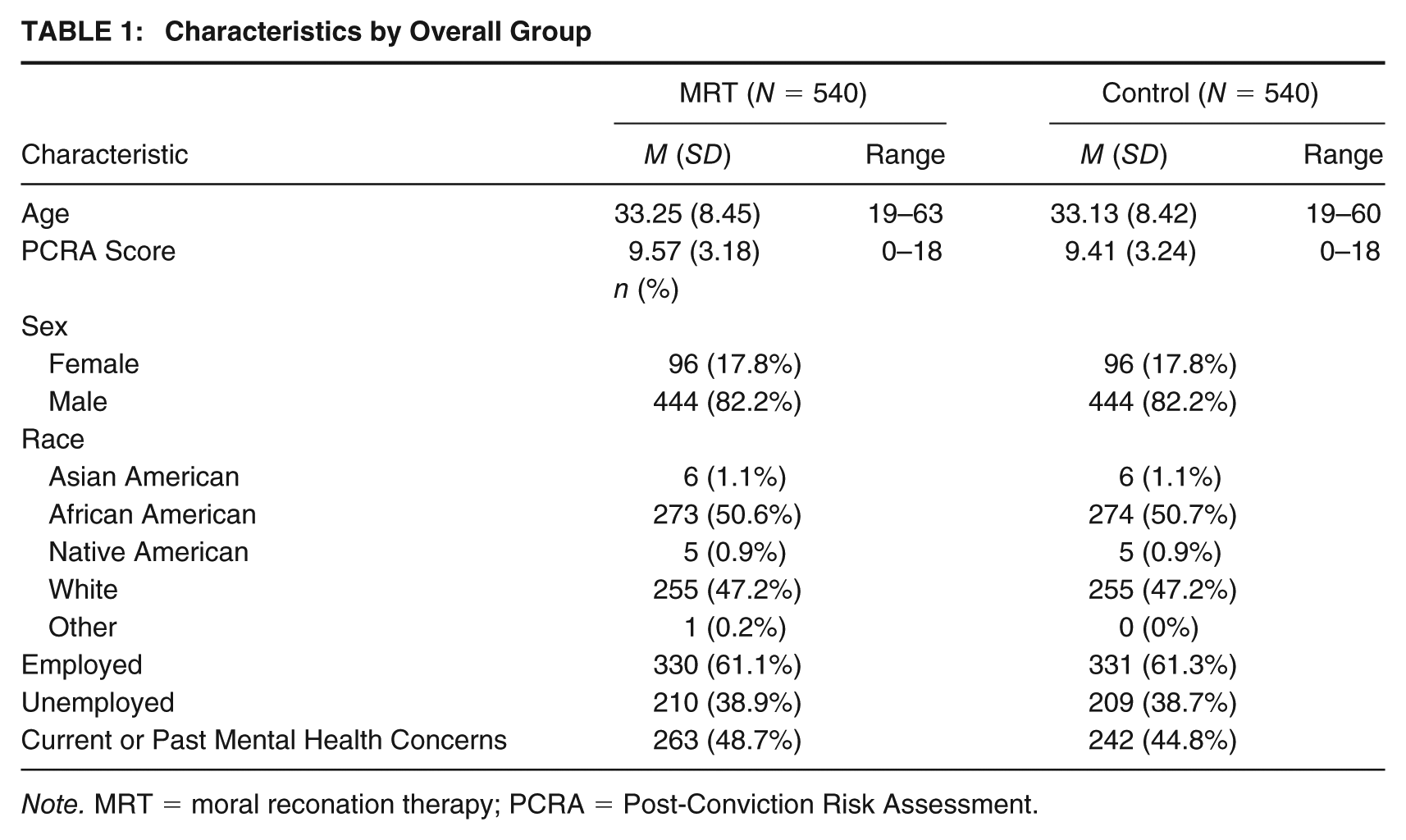
Note. MRT = moral reconation therapy; PCRA = Post-Conviction Risk Assessment.
Procedure
Prior literature has identified methodological weaknesses of studies assessing MRT; namely, failure to control confounding variables and lack of appropriate comparison groups emerge as major weaknesses across the extant MRT research (Allen et al., 2001; Ferguson & Wormith, 2012). To avoid these weaknesses, this study (a) utilized longitudinal data and (b) applied stabilized inverse-probability weights to create a pseudo-population in which the covariates of interest were balanced across probation-as-usual (Control), successful MRT (Completer), and unsuccessful MRT (Noncompleter) groups.
Archival data were collected using both the Probation and Pretrial Services Automated Case Tracking System (PACTS) and Decision Support System (DSS) for the relevant justice-involved individuals between 2007 and 2018. Variables of interest were first identified using the PACTS program, then compiled into reports for the researchers to export and subsequently analyze using the DSS report generator. Variables of interest addressed central factors such as demographics, offense type, recidivism, employment status, and PCRA scores. Data were imported into Microsoft Access, cleaned, and compiled into a database.
We implemented an inverse probability of treatment weighting (IPTW) approach using propensity scores to address selection differences and balance covariates across the three groups. First, a multinomial logistic regression model predicted group membership (Control, Completer, Noncompleter) based on pretreatment covariates: age at the start of supervision, sex, race, employment status, PCRA risk score, and current or known history of mental health issues. From this model, we calculated stabilized IPTW weights for each individual:

where
This yielded a pseudo-population in which the covariate distributions were balanced across groups (all postweight SMDs < 0.1; variance ratios < 1.4). Extreme weights were not present (M = 1.00, SD = 0.32, CV = 0.32, Range: 0.27 – 4.13). Effective sample sizes after weighting were 535.5 individuals engaging in probation-as-usual (Control), 259.5 successful MRT participants (Completer), and 193.5 unsuccessful MRT participants (Noncompleter). See Table 2, Panel A for the full preweight versus postweight covariate balance.
Preweight versus Postweight Covariate Balance
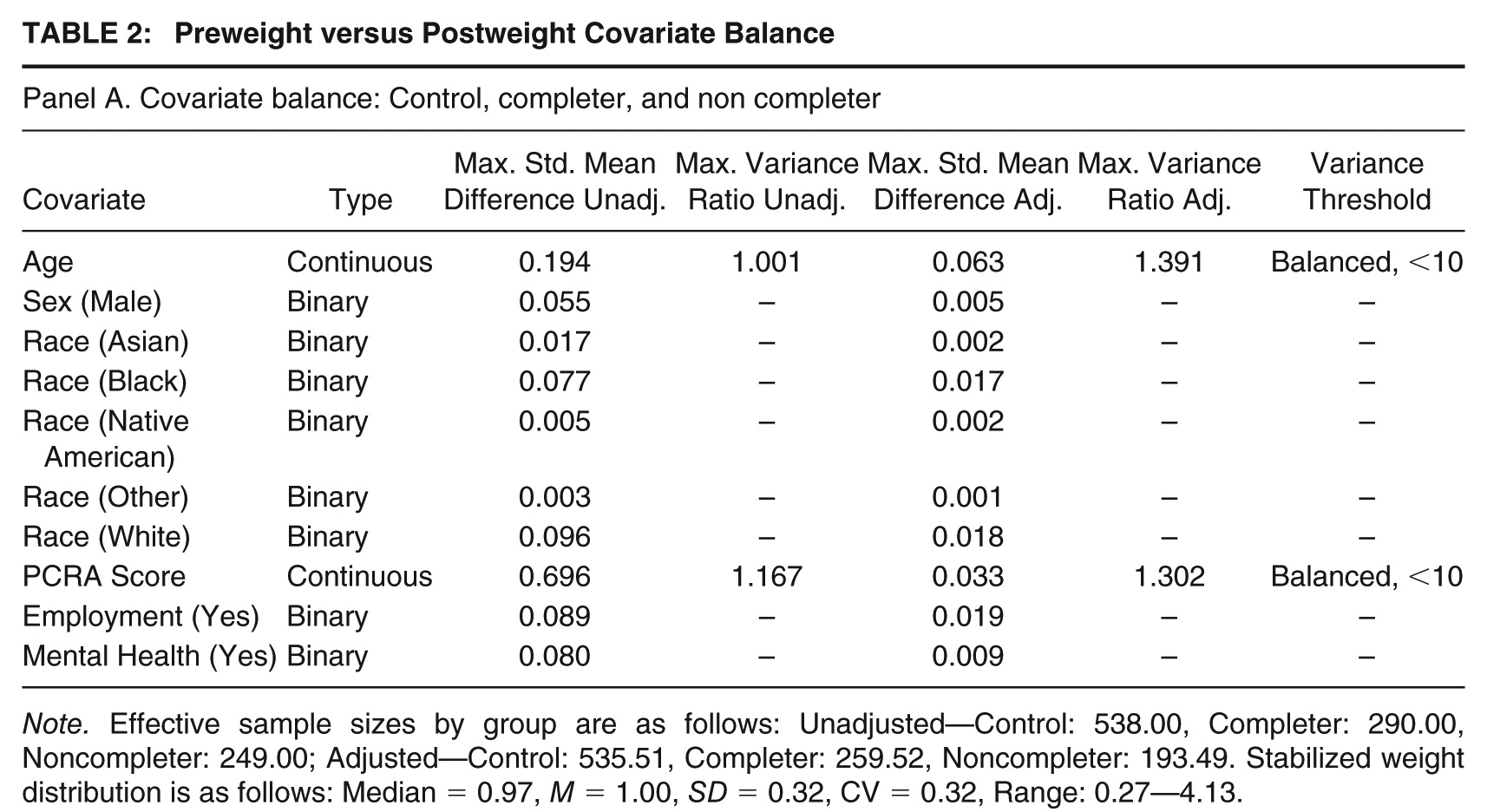
Note. Effective sample sizes by group are as follows: Unadjusted—Control: 538.00, Completer: 290.00, Noncompleter: 249.00; Adjusted—Control: 535.51, Completer: 259.52, Noncompleter: 193.49. Stabilized weight distribution is as follows: Median = 0.97, M = 1.00, SD = 0.32, CV = 0.32, Range: 0.27—4.13.
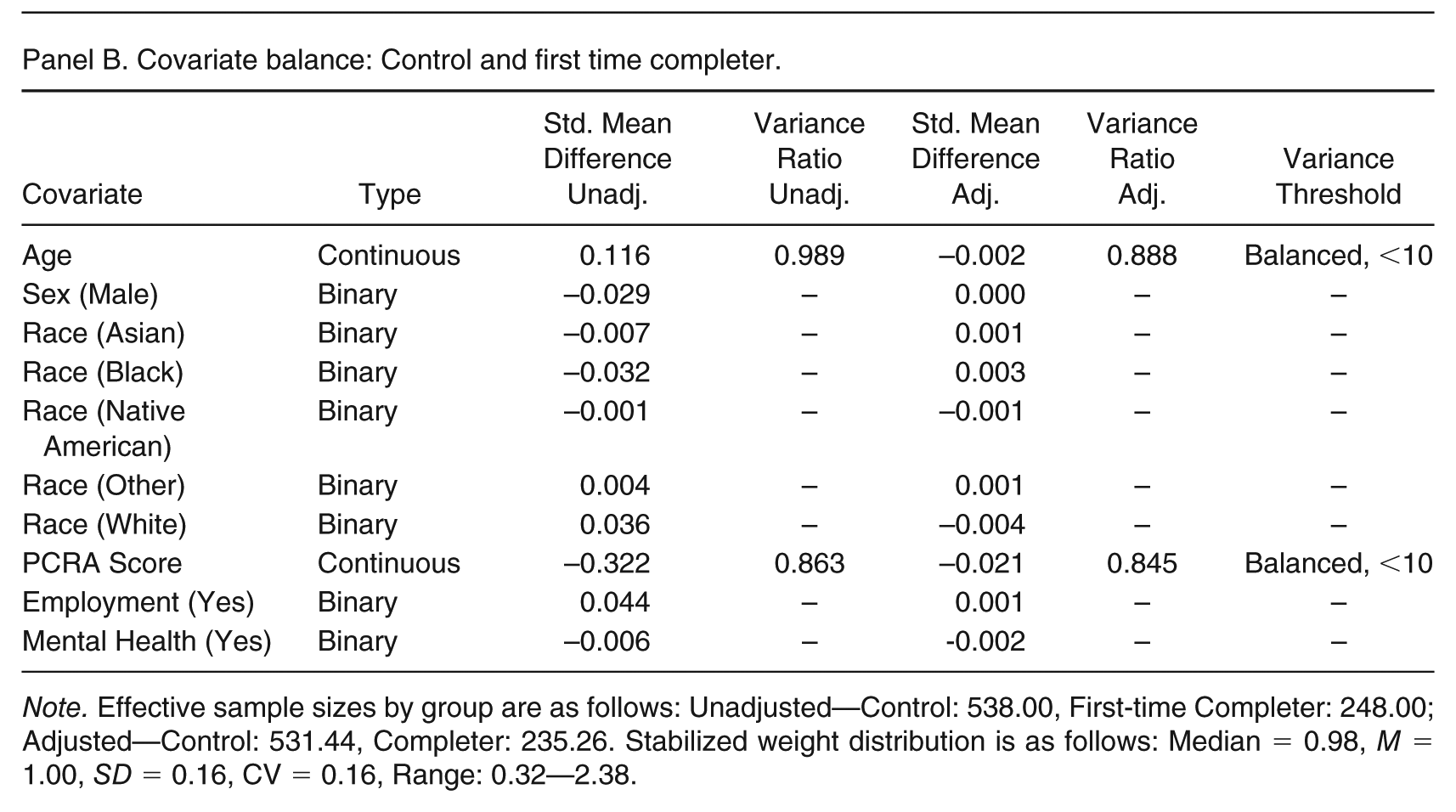
Note. Effective sample sizes by group are as follows: Unadjusted—Control: 538.00, First-time Completer: 248.00; Adjusted—Control: 531.44, Completer: 235.26. Stabilized weight distribution is as follows: Median = 0.98, M = 1.00, SD = 0.16, CV = 0.16, Range: 0.32—2.38.
Analytic Strategy
All analyses were conducted in R, and statistical significance was set at α = 0.05. All recidivism outcomes (binary recidivism, time-to-recidivism, charge rate) were measured from the start of participant treatment and were tracked for up to 2 years posttreatment (or until December 31, 2018, the cut-off date for the final data pull, whichever came first). This truncation censors cases with insufficient follow-up, mitigating possible bias due to varying supervision lengths.
Binary recidivism was operationalized as to whether an individual had any new charge within two years of their last treatment start date. Importantly, individuals who had not recidivated and did not have a full 730 days of observation (i.e., those who were only observed for a shorter period by the end of 2018) were treated as missing/censored to avoid unfairly counting them as “no recidivism” without adequate follow-up. Thus, the binary recidivism measure effectively indicates: 1 = recidivated within 730 days (with at least 730 days of observation), 0 = did not recidivate within 730 days or recidivated after the follow-up period (with at least 730 days of observation). Participants with fewer than 730 days of follow-up were marked as NA. Time-to-recidivism (days from start of last treatment to first new charge) is a continuous outcome (M = 562.63, SD = 243.55, Range: 0.5–730). Individuals with no recidivism by the end of the 2-year window (or by the censor date of 12/31/2018) were treated as right-censored at their last observed date. Finally, charge rate was used as an indicator of recidivism severity. Importantly, exact charge dates are not reliable for this sample, so rather than using frequency of charges after treatment start, a 2-year standardized rate was employed:

This standardized each participant’s total charges to a 2-year window, resulting in an overall incidence rate for the 2-year period (M = 0.62, SD = 1.75, Range: 0 – 26.39). All analyses were conducted on the IPTW-weighted sample using appropriate survey-weighted or nonparametric methods. To test for overall group differences in the likelihood of recidivism within 2 years, we fit a weighted binary logistic regression, including the three-level group variable (Control, Completer, Noncompleter) with Control as the reference category.
To address time-to-recidivism and censoring, we conducted a Cox survival analysis with IPTW weights. The weighted Cox model estimated hazard ratios (HR) for recidivism over time for Completers and Noncompleters relative to Controls. Time to recidivism evidenced acceptable levels of kurtosis (-0.45) and skew (-1.07).
Nonparametric tests were employed to assess the charge rate after the start of the last supervision, as this outcome is highly kurtotic (+81.21) and skewed (+7.59). Specifically, a weighted Kruskal–Wallis H test (nonparametric ANOVA) was utilized to determine if the distribution of charge rate differed among the three groups, followed by Dunn’s post hoc pairwise comparisons (with Holm adjustment) to identify which groups differed significantly.
In a supplemental exploratory analysis, we restricted the treatment group to First-Time Completers only (i.e., individuals who successfully completed MRT on their first attempt, with no prior failed MRT participation). Covariate distributions were balanced across groups (all postweight SMDs < 0.2; variance ratios < 0.9). Extreme weights were not present (M = 1.00, SD = 0.16, CV = 0.16, Range: 0.32–2.38). Effective sample sizes after weighting were 531.44 individuals engaging in probation-as-usual (Control) and 235.26 MRT participants (First-time Completer). See Table 2, Panel B for the preweight versus postweight covariate balance.
We then repeated the above steps in a binary propensity-weighted comparison between First-time Completer vs. Control groups. This analysis addressed whether those who received the full intended MRT intervention without any drop-out have improved outcomes relative to no MRT. A separate propensity score was estimated (using the same covariates) for this two-group scenario, stabilized IPTW weights were derived, and weighted logistic, Cox, and Kruskal–Wallis tests were conducted for binary recidivism, time-to-recidivism (M = 593.49, SD = 230.44, Range: 0.5 – 730, skew = -1.39, kurtosis = +0.36), and charge rate (M = 0.51, SD = 1.72, Range: 0 – 26.39, skew = +9.12, kurtosis = +108.79), respectively.
Results
Research Question 1
Our first research question aims to address the efficacy of MRT at reducing recidivism in people on federal probation. New charges within two years of the last treatment start date, time to new charge within two years of the last treatment start date, and the 2-year standardized charge rate were used as proxy measures of recidivism.
The IPTW-adjusted binary logistic regression, containing the independent variable of three-level group and binary recidivism as the dependent variable, revealed a significant overall effect of group on the likelihood of recidivating within 2 years, Wald χ²(2) = 8.85, p < .001. In contrast to predictions, Noncompleters were significantly more likely to recidivate than Controls. Specifically, Noncompleters had more than double the odds of recidivism relative to the control group (odds ratio [OR] = 2.26, 95% confidence interval [CI] [1.54, 3031], p < .001). Completers did not significantly differ from Controls: their odds of recidivating were slightly higher than Controls but not statistically significant (OR = 1.24, 95% CI [0.88, 1.76], p = .219). These results suggest that completing MRT did not reduce the short-term likelihood of recidivism compared to probation-as-usual; however, failing to complete MRT was associated with a markedly higher likelihood of recidivism. Table 3, Panel A presents the model statistics.
Weighted Regression Models Predicting Recidivism
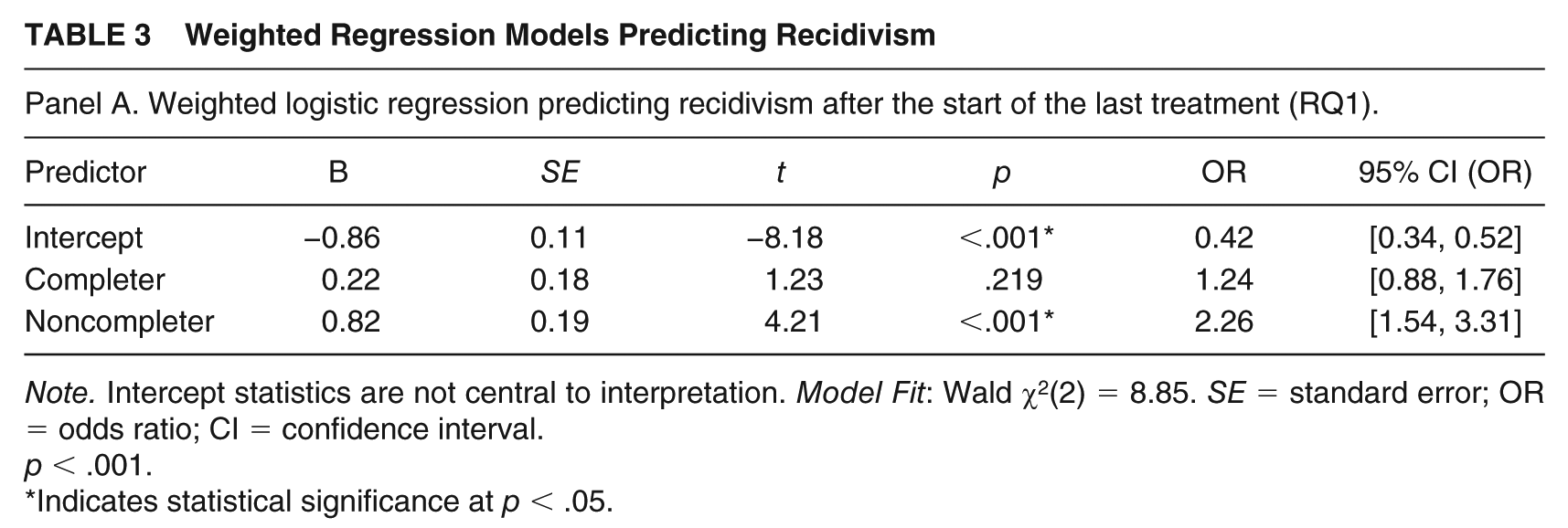
Note. Intercept statistics are not central to interpretation. Model Fit: Wald χ2(2) = 8.85. SE = standard error; OR = odds ratio; CI = confidence interval.
p < .001.
Indicates statistical significance at p < .05.
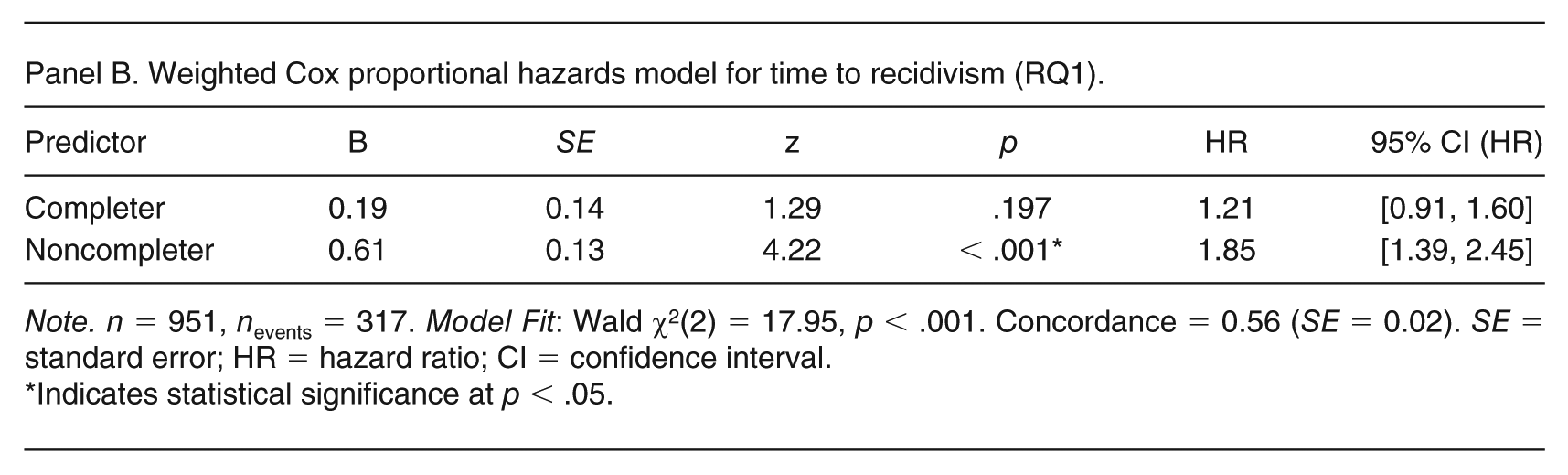
Note. n = 951, nevents = 317. Model Fit: Wald χ2(2) = 17.95, p < .001. Concordance = 0.56 (SE = 0.02). SE = standard error; HR = hazard ratio; CI = confidence interval.
Indicates statistical significance at p < .05.
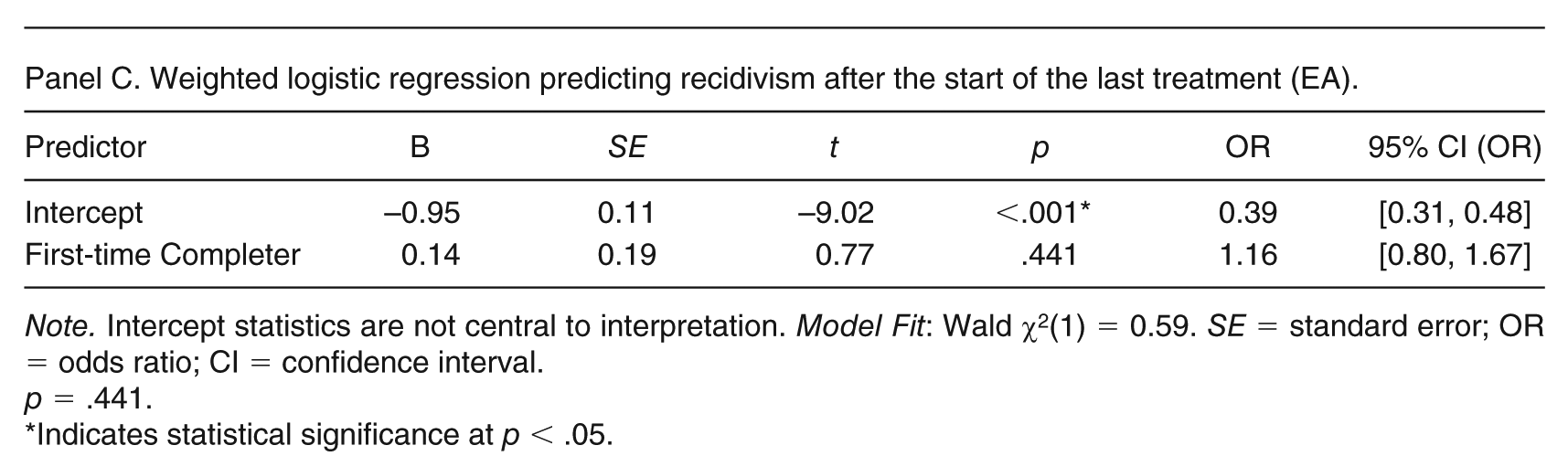
Note. Intercept statistics are not central to interpretation. Model Fit: Wald χ2(1) = 0.59. SE = standard error; OR = odds ratio; CI = confidence interval.
p = .441.
Indicates statistical significance at p < .05.
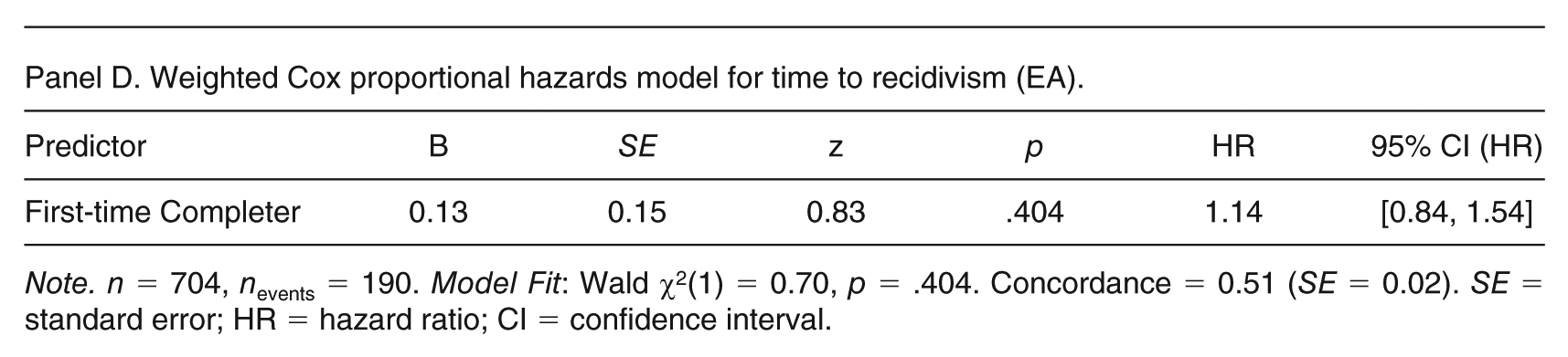
Note. n = 704, nevents = 190. Model Fit: Wald χ2(1) = 0.70, p = .404. Concordance = 0.51 (SE = 0.02). SE = standard error; HR = hazard ratio; CI = confidence interval.
Next, the weighted Cox proportional hazards model including three-level group as the independent variable and time-to-recidivism as the dependent variable showed a significant effect of group on recidivism timing, Wald χ²(2) = 17.95, p < .001. Mirroring the weighted logistic regression findings, Noncompleters experienced significantly faster recidivism than Controls, whereas Completers were not significantly different from Controls. Specifically, Noncompleters had an 84.6% higher hazard of recidivism compared to the Controls (HR = 1.85, 95% CI [1.39, 2.45], p < .001). This indicates that at any given time in the 2-year follow-up, the risk of recidivism was significantly greater for those who did not finish MRT. By contrast, Completers’ recidivism hazard was 1.21 times that of controls, which was not statistically significant (HR = 1.21, 95% CI [0.91, 1.60], p = .197). See Table 3, Panel B for model statistics.
Finally, the weighted Kruskal–Wallis H test containing three-level group as the independent variable and charge rate as the dependent variable displayed significantly different charge rates across groups, H(2) = 9.12, p = .011. Post hoc Dunn pairwise comparisons confirmed that the Noncompleters had a significantly higher rate of new charges than Controls, t(685) = 2.99, MRankDiff = 0.07, padj = .009. Meanwhile, Completers did not significantly differ from Controls, t(739) = 1.25, MRankDiff = 0.03, padj = .210, or Noncompleters, t(472) = -1.83, MRankDiff = -0.05, padj = .135, on charge rate.
Thus, predictions related to the first research question are unsupported by our findings. The primary outcomes paint a consistent picture: MRT Noncompleters had significantly worse recidivism outcomes on all metrics (higher likelihood of recidivism, faster time to recidivism, and higher charge rate) compared to both MRT Completers and Controls. By contrast, MRT Completers showed no statistically significant improvement over Controls on any recidivism measure within the 2-year follow-up. MRT did not yield a measurable benefit beyond what was achieved by standard probation alone, in this sample and timeframe.
Exploratory Analysis
Our exploratory IPTW analysis isolated First-time Completers (n = 290) versus Controls (n = 538) to test if successful completion of MRT on the first attempt leads to better outcomes than probation-as-usual. The propensity model for this subgroup analysis achieved excellent balance (all weighted SMD < 0.05), similar to the main analysis.
The weighted logistic regression showed a nonsignificant effect of first-time MRT success on 2-year recidivism (OR = 1.16, 95% CI [0.80, 1.67], p = .441), see Table 3, Panel C. In addition, the weighted Cox model found no significant difference (HR = 1.14, 95% CI [0.84, 1.54], p = .404) for time to recidivism between First-time Completers and Controls, see Table 3, Panel D. Finally, a design-based Kruskal–Wallis test on the 2-year charge rate found no significant difference between First-time Completers and Controls, t(702) = 0.82, p = .411; MRankDiff = 0.017. First-time Completers displayed a similar postsupervision charge rate to Controls.
This exploratory comparison reinforces the findings from our main analysis: among those who completed MRT, even on their first attempt, we did not observe a reduction in recidivism relative to Controls.
Discussion
MRT has been widely touted as a successful, evidence-based treatment for offending populations (e.g., Little et al., 1991, 1993, 1994, 1999, 2010). However, many studies assessing the efficacy of MRT for reducing recidivism have major methodological weaknesses (see Allen et al., 2001; Ferguson & Wormith, 2012; Harrell et al., 2023). Specifically, (a) a majority of the extant studies were conducted by the founders of MRT or their affiliates, (b) most studies do not control for potentially confounding variables, such as participant race or sex, on recidivism-related outcomes, and (c), few studies employ adequate control groups.
To address these weaknesses and extend the base of literature on MRT, this study examined the efficacy of MRT for reducing recidivism in a sample of people on federal probation. Overall, the findings contradict our predictions, and in turn, contradict previous research on the efficacy of MRT. MRT completion did not significantly reduce recidivism compared to probation-as-usual in this sample: Completers and Controls showed statistically equivalent recidivism rates, timing, and charge rates. This echoes findings from some prior studies that failed to find added value of MRT over treatment-as-usual in certain populations (e.g., Blonigen et al., 2022, who reported no differences in recidivism between MRT vs. usual care in a veteran sample). However, we found clear evidence that failing to complete MRT is associated with significantly worse outcomes: Noncompleters were more likely to recidivate, and to do so sooner and with a higher charge rate, than even the Control group.
One interpretation is that noncompleters (“dropouts”) represent a high-risk subgroup for whom any exposure to MRT is insufficient to counteract their risk, leading to outcomes worse than if they had not attempted MRT at all. It is also possible that partial exposure to MRT or a failed treatment attempt has negative effects or demoralizes participants, though establishing causality is difficult. Regardless, this finding underscores the importance of treatment retention: if MRT is to be effective, participants likely need to complete the program, as suggested by Wakefield and Cameron (2011).
Our data show that Completers fared better than Noncompleters on all measures, aligning with the notion that MRT completion is at least associated with avoiding the worst outcomes seen in dropouts. Crucially, though, MRT completion did not confer a measurable benefit beyond probation-as-usual. This raises questions about the overall efficacy of MRT in this context. It could be that MRT has no actual effect on recidivism for this population (i.e., Completers resemble Controls because MRT provides no added value), or that any positive effect of MRT is too small to detect without a larger sample or longer follow-up period. Another possibility is that unobserved differences remain between groups (e.g., motivation levels or external support) that our weighting could not capture. However, our exploratory “First-time Completer” analysis, which focused on those participants who were likely most engaged in MRT, still showed no improvement relative to Controls.
Our results emphasize a need for further investigation into factors that might enhance MRT’s effectiveness. Given the focus of this study on people on federal probation, it is possible that MRT may be more effective for individuals in residential settings than for participants under community supervision, although the effectiveness of MRT for residential settings has also come into question (e.g., Blonigen et al., 2022). It is also possible that program administrators did not completely adhere to treatment fidelity for this sample, as the authors did not observe sessions. However, Harrell et al. (2022) suggest that it is fidelity to the MRT program that negatively impacts participants, outlining how MRT is incompatible with the National Association of Social Workers’ Code of Ethics for social workers (who often act as facilitators of MRT sessions).
It may be the case that, at baseline, the individuals in our sample were simply more likely to recidivate. Yet, given the purported ability of MRT to treat “resistant” client populations including those who are identified as at least one of the following: (a) diagnosed with a substance use disorder, (b) of a minority population, (c) of low socioeconomic status, (d) has a current or past history of mental health diagnoses, (e) has prior criminal offenses, or (f) has antisocial personality disorder (Little et al., 2010; Little & Robinson, 1988), it is unlikely that community-supervised individuals would be too “resistant” for this form of treatment.
In addition, by using data from over 10 years of observations, balancing covariates across groups, and including covariates known to be important static and dynamic risk factors, our analyses should have detected an effect of treatment if one were present. Therefore, we conclude that MRT is not associated with measurable improvements in recidivism outcomes for people on federal probation.
While every attempt was made to prevent the methodological weaknesses observed in previous studies assessing the efficacy of MRT, there are some limitations to the present research. It is important to acknowledge that this study is quasi-experimental. The IPTW approach balances observed covariates, but unmeasured confounders could still influence who completes MRT and their propensity to reoffend. We also focused on a 2-year follow-up; it is possible that MRT’s effects (for Completers) might emerge over a longer term or in specific subdomains that are not captured by probation data. In addition, while our sample is drawn from a full district and weighted to represent the target populations, generalizability may be limited to similar federal probation settings.
Data were collected for justice-involved individuals under community supervision between 2007 and 2018. While this does provide a sizable amount of information on individuals who participated in MRT, this time frame does not account for the COVID-19 pandemic and any resulting impact on MRT. Participants in MRT may be quite different post-2020, given the impact of the pandemic on probation departments’ practices (Martin & Zettler, 2022) and people under community supervision more generally (LeMasters et al., 2023).
We did not control for treatment year, so there may be supervision practices and MRT deployment unaccounted for that might have impacted participants differently in 2007 relative to 2017 or 2018. Further, the great recession from 2007 to 2009 may have influenced probation (e.g., Finlay & Mueller-Smith, 2021) in ways that were unaccounted for in this study. We also did not control for location (three sites in our district provided MRT). Future research should consider the year and location of treatment in determining the effectiveness of MRT.
The structure of our data also poses some limitations (the data were pulled from the management system utilized by our federal district, and therefore, we were limited to the variables and metrics utilized by that system). First, our measure of recidivism revolves around new charges after the start of treatment. However, we do not have information on nonfederal charges accrued by participants. Furthermore, we do not have information about the overall failure of supervision: we only know if a violation occurred, not what sanctions may have followed. In addition, we do know that MRT participants in our federal district did not participate in any other rehabilitation program directed by the federal probation office (outside of MRT); however, it is possible that MRT participants could have also participated in mental health or substance use programs which are not accounted for by the present analysis. Finally, we could only obtain the overall PCRA score, not the individual items. Given the predictive power of the PCRA for this population, future research should collect the individual items for a deeper understanding of this association.
Conclusion
Although many studies have touted the positive impact of MRT on offending populations (e.g., Little et al., 1991, 1993, 1994, 1999, 2010) this study adds to an increasing base of mixed literature on MRT which has shown null (e.g., Blonigen et al., 2022) or even negative impacts (e.g., Armstrong, 2002, 2003) of MRT on criminal behavior. Our results indicate that MRT is not an effective form of treatment for reducing recidivism in people on federal probation. In our sample, those who successfully completed the program, even on their first time, were not significantly less likely to recidivate than those in the control group. Furthermore, participants who entered MRT and were unsuccessful were significantly more likely to recidivate than controls.
Given the popularity of MRT as a form of treatment for offending populations, more research should continue to examine the efficacy of MRT for reducing recidivism, especially considering the growing number of studies that report null or negative findings. In addition, it may be important for future research to consider how MRT may differentially impact justice-involved individuals under community supervision relative to those who are incarcerated and/or in residential facilities. While MRT may be useful for some populations, for people on federal probation, it may be prudent to consider alternative forms of treatment; or at least, to consider how to strengthen the MRT program so that it more positively impacts those individuals who are predisposed to recidivism.
Footnotes
Authors’ Note:
The authors have no conflicts of interest to disclose.