
Abstract
The present investigation examined a group of 90 clients receiving treatment for issues related to sexual offending in The Central District (Ontario) Sex Offender Treatment Program operated by Correctional Service Canada (CSC). Treatment was provided in line with the Integrated Risk Assessment and Treatment System (IRATS) Model developed by the authors. A group of 55 individuals who had not received sexual offense–specific treatment but who received standard correctional programming offered by paraprofessionals were used as a basis of comparison. Risk assessment data were available for all clients included in the analyses. Results indicated that there were no differences between groups on the RRASOR (an actuarial instrument designed to assess risk of sexual offense recidivism) with reference to sexual offender recidivism risk. With reference to sexual offense recidivism, only one of the treated clients recidivated sexually over 8.17 years of follow-up versus four of the 55 comparison group who were followed for a significantly shorter period of time (i.e., 6.9 years).
Sexual offending is an issue that frequently generates concern, especially with reference to clients released to the community from institutional settings after serving time for sexual offenses. Recent reviews have suggested that contemporary treatment, using cognitive-behavioral approaches, results in significantly lower rates of recidivism in treated versus comparison samples (see Abracen & Looman, 2016; Schmucker & Lösel, 2015) and that change scores on measures of dynamic risk are associated with significant reductions in recidivism in the predicted direction (Olver et al., 2014). In spite of these findings, widespread skepticism still appears to exist regarding clients released to community settings and serving time for sexual offenses. As noted by Schmucker and Lösel, a number of methodological problems exist in the literature which have contributed to the skepticism. Coupled with this is the fact that there is a tendency for scientific findings to be ignored (see Janus, 2006, for a discussion), especially when addressing the needs of individuals convicted of sexual offenses who are released to community settings. As well, many moderate and higher risk individuals convicted of sexual offenses who live in community facilities exhibit signs and symptoms of mental illness (e.g., Abracen et al., 2014). Although in some cases such diagnoses may be directly related to sexual offending (e.g., exclusive pedophilia, Eher et al., 2015), in others the association may not be as direct. Regardless, many moderate- and high-risk individuals convicted of sexual offenses released to community settings suffer from the dual stigma of being convicted of having committed a sexual offense as well as suffering from mental illness.
Although legitimate debate exists regarding what role mental illness and other so-called noncriminogenic needs play in the genesis of violent offending (see Abracen & Looman, 2016, for a review of the literature), the fact remains that clinicians tasked with the treatment of moderate- and high-risk clients convicted of sexual offenses released in community settings must address a wide array of presenting concerns. For this reason, we have argued that there is likely a difference between psychoeducational programs directed at offender populations (typically which focus on circumscribed areas, for example, anger management) and more therapeutic programs typically run by clinicians with graduate-level training in a health care–related discipline (see Abracen & Looman, 2016). Recent evidence appears to confirm our earlier views regarding this matter. A large-scale institutional program operated by paraprofessional staff demonstrated marginally higher rates of sexual offense recidivism by treated clients than untreated controls (Mews et al., 2017). Furthermore, a recent meta-analysis regarding factors affecting treatment outcome with clients convicted of sexual offenses indicated that sexual offending treatment provided by paraprofessional staff does not appear to be as effective as treatment programs both administered and delivered by professional staff (Gannon et al., 2019). It is interesting to note that these authors observed that less than one in five programs consistently used qualified psychologists in hands-on facilitation of treatment, and the majority of those programs that did employ mental health professionals (83.3%, n = 10) were implemented in the 1970s, 1980s, or 1990s rather than more recently. As noted by the authors, this may explain why the meta-analysis did not find that more contemporary treatment programs were associated with improved outcomes. Another important difference between these two types of programs is the use of more didactic approaches with reference to psychoeducational groups. There is no doubt that such groups are of use and the research on Risk-Need-Responsivity (RNR)-based treatment approaches (see Andrews & Bonta, 2010) clearly attests to the utility of such options. Nonetheless, more comprehensive approaches to treatment that go beyond traditional RNR-based groups appear to be of value when working with complex presentations such as the case with moderate- and high-risk clients who have committed sexual offenses (e.g., see Abracen & Looman, 2016; Marshall et al., 2011; Olver et al., 2009).
Recently, we have introduced a new model, the Integrated Risk Assessment and Treatment System (IRATS) Model, that we have found to be useful when applied in institutional and community settings (Abracen et al., 2017; Abracen & Looman, 2016; see Figure 1). This model suggests that a wider range of treatment targets than suggested by Andrews and Bonta (2010) need to be included in contemporary approaches to forensic treatment. The IRATS includes a focus on the so-called “Central Eight” criminogenic needs emphasized by Andrews and Bonta and also on factors such as attachment difficulties and associated issues related to serious mental illness (SMI). It should be emphasized that the model only includes elements that have been empirically supported in the forensic literature. In this respect, the IRATS differs from approaches such as the Good Lives Model (GLM, Ward & Maruna, 2007) which includes factors such as “happiness” and “spirituality” which, although potentially important, may be impossible to operationalize for the purpose of research. The IRATS is specifically designed to be a therapeutic model and does not lend itself to psychoeducational approaches to treatment as is the case with RNR-based interventions. Issues associated with therapist training and the therapeutic alliance therefore receive substantially more attention than the case with RNR-based approaches (see Blasko et al., 2018; Marshall et al., 2011, for additional reviews regarding the importance of the therapeutic alliance with individuals who have been convicted of sexual offenses). The IRATS is compatible with other models directed toward individuals who have committed sexual offenses (e.g., The Motivation-Facilitation Model of Sexual Offending, MTM, Seto, 2019) that list both state (e.g., alcohol use) and trait (e.g., antisocial personality) factors as well as issues associated with inappropriate sexual arousal. The MTM has the advantage of providing a more general model that may prove to be useful in understanding which factors are associated with the etiology of sexual offending. Unlike general models such as the MTM, the IRATS offers additional specificity regarding which factors should become a focus of treatment.
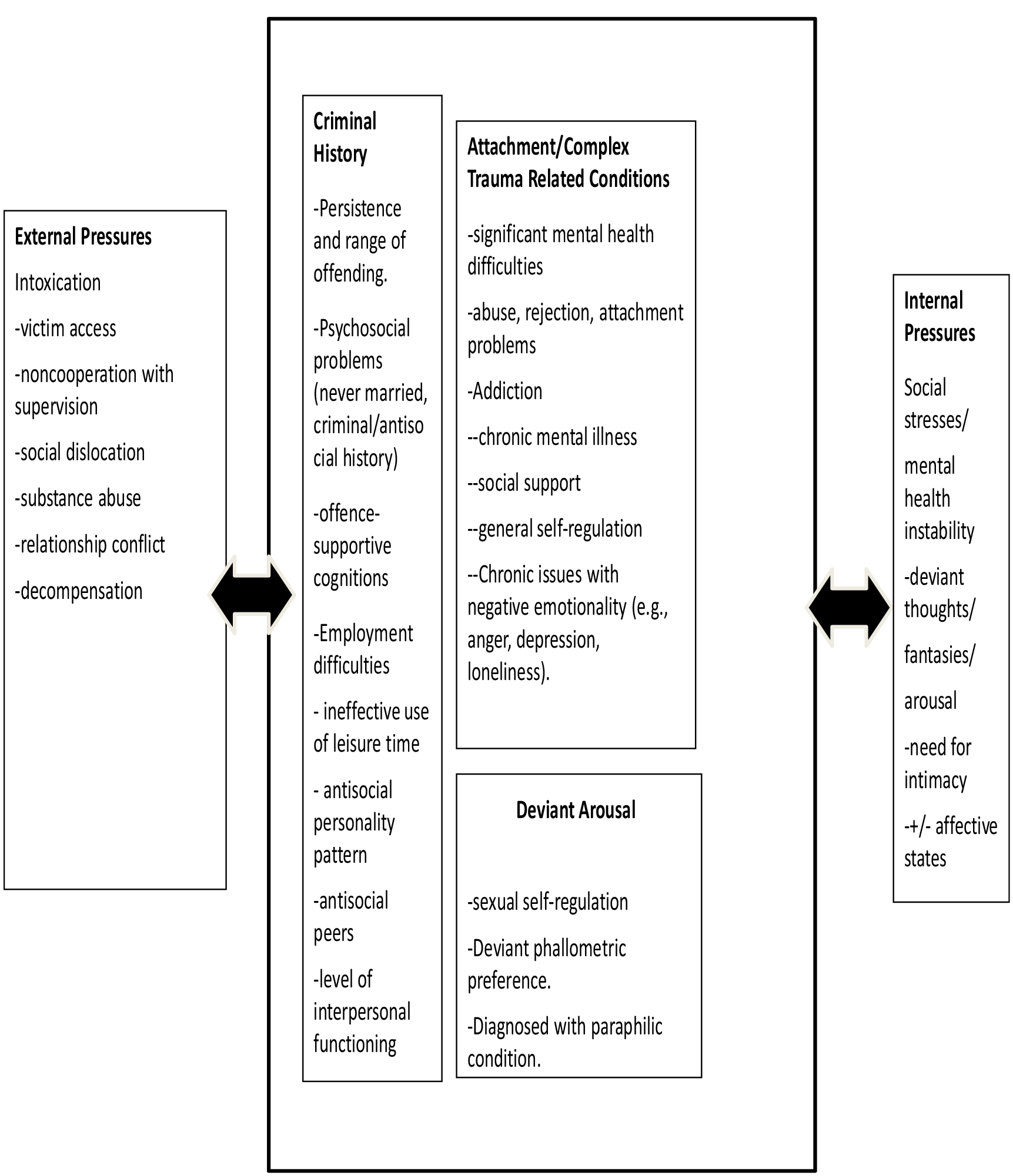
The Integrated Risk Assessment and Treatment System (IRATS) Model
With reference to outcome research supporting the IRATS Model, an early study by our team compared a group of 89 high-risk clients convicted of sexual offenses treated at the Regional Treatment Centre Sex Offender Treatment Program (RTCSOTP) to a matched group of 89 untreated individuals convicted of sexual offenses. The primary outcome measure used in this study was sexual offense recidivism. Over an average follow-up of approximately 10 years, treated clients recidivated sexually at a rate of 23.6% whereas the sexual recidivism rate was 51.7% for the untreated comparison sample (p < .0001; Looman et al., 2000). The Regional Psychiatric Centre (RPC) in the Prairie Region of Correctional Service of Canada (CSC) has operated an inpatient-based program for individuals convicted of sexual offenses, which, in many respects, is quite similar to the RTC Program. The RPC Sex Offender Treatment Program has also demonstrated significant reductions in recidivism for treated clients versus comparison samples (Nicholaichuk et al., 2000; Olver et al., 2009). In our view, these programs have several features in common, not the least of which is the focus on a wide range of clinical targets in a population that presents with numerous treatment needs. These programs were operated with substantial ongoing input from mental health professionals with extensive backgrounds in health care. In addition, the inpatient setting allowed for both formal and informal contact between clinicians and clients. That is, clinicians would have an opportunity to interact with clients and observe their behavior both while attending group or individual therapy and at times when clients were not attending treatment. We have argued that this latter component, which we have called milieu therapy (Abracen & Looman, 2016), is an important component of treatment and contributes to the establishment of the therapeutic alliance.
More recently, we have turned our attention to the assessment and treatment of high-risk individuals incarcerated for having committed violent (including sexual) offenses and who are living in community settings. In a study examining criminogenic need among all individuals under the jurisdiction of CSC and living in Community Residential Facilities (CRFs) or Community Correctional Centres (CCCs; Abracen et al., 2012), it was observed that there have been significant changes in the population living in such facilities between 1998 and 2008. CRFs and CCCs are residential facilities either operated directly by CSC (in the case of CCCs) or by community partners such as the Salvation Army (in the case of CRFs).
With reference to more traditional criminogenic needs, significant increases in the rate of factors such as substance abuse were observed in these facilities between 1998 and 2008. In addition, there were a significantly greater percentage of individuals with histories of violence living in such facilities in 2008 when compared with those living in the same facilities in 1998. In accordance with the IRATS Model, however, we also observed significant elevations with reference to a variety of indicators related to mental illness. For example, the rate of current mental health diagnoses had more than tripled from 4.7% to 18.5% between the 1998 and 2008 observation periods.
With reference to the presence of specific diagnoses, we have published a more in-depth analysis of all clients living at one of the CCCs described in Abracen et al. (2012; Abracen et al., 2014). Findings from this investigation revealed very high rates of SMI as evidenced by diagnoses made by licensed mental health professionals. For example, among the sample of 136 individuals mandated to reside at the Keele CCC in 2007–2008, approximately 20% had been diagnosed with some type of psychotic process within 5 years of living at the facility. In addition, those clients with borderline personality disorder and attention-deficit hyperactivity disorder were significantly more likely to recidivate or be suspended (i.e., returned to a more secure institutional environment). The sample consisted of individuals who had been convicted of both sexual and nonsexual offenses.
In a follow-up to this initial investigation, Abracen et al. (2015) examined these same 136 offenders to examine whether individual psychological therapy reduced their risk of recidivism. After accounting for actuarially assessed risk, moderate doses of treatment were associated with 7.7 times less likelihood of recidivism. High doses of treatment (defined as 20 or more individual therapy sessions) were associated with 11.6 times less likelihood of recidivism. Treated clients were compared with individuals who received no treatment or who were only assessed for treatment. Individuals who had been convicted of both sexual and violent (nonsexual) offenses were included among the treated subjects in this study.
Given that research supporting the RNR approach has typically yielded findings with low to moderate effect sizes (e.g., Schmucker & Lösel, 2015), research related to newer models such as the IRATS Model become critical to the further refinement of treatment. Although the data presented in relation to the IRATS Model are certainly encouraging, we wished to examine a group consisting entirely of individuals convicted of sexual offenses specifically attending sexual offense treatment in a community setting. There have been changes to policy in CSC regarding the treatment of such groups over the last number of years. Psychological staff were directly involved in treatment directed at individuals convicted of sexual offenses until approximately 2011–2012 when treatment delivery became the responsibility of the Programs Department. At present, treatment for sexual offending in CSC is delivered by paraprofessionals with only several weeks of training in the delivery of the treatment model. Although the model currently employed by CSC is in accordance with the principles of RNR, as noted above, recent evidence suggests that contemporary sex offender treatment provided by paraprofessionals has yielded few significant treatment effects (Gannon et al., 2019).
With reference to other community outcome research, Kim et al. (2016), in a review of recent meta-analyses, reported that overall results concluded that sex offense treatments can be considered as “proven” or at least “promising.” These authors also observed that community treatment produced larger effect sizes when compared with institutional treatment programs. These meta-analytic data regarding sex offense treatment outcome research are in accordance with nonquantitative literature reviews specifically related to the treatment of groups of high-risk individuals convicted of sexual offenses (e.g., Abracen & Looman, 2016), which have argued that even high-risk groups of individuals convicted of sexual offenses can be successfully treated.
Although these data are of interest, they do not necessarily speak to issues associated with community concerns regarding contemporary treatment for individuals convicted of sexual offenses. There are relatively few studies looking at contemporary treatment programs. As a result of the limited research in this area, it is difficult to make any assertions as to whether newer programs result in lower rates of sexual offense recidivism when compared with older programs. Rarer still are recent studies that include untreated groups of individuals convicted of sexual offenses.
Given the research cited above, it is hypothesized that lower than expected rates of sexual recidivism will be observed in the treated sample. Observed rates are predicted to be significantly lower than predicted rates based on the Static-99R, an actuarial instrument designed to assess for the risk of sexual offense recidivism. These clients were also compared with a group of people convicted of sexual offenses, the majority of whom received standard nonsexual correctional treatment programming offered by Correctional Service Canada (CSC). Comparison group subjects were assessed in the Ontario region of CSC and were included in a previous study reported by our team (see Abracen et al., 2011).
Method
Subjects
Samples
A group of 90 consecutive admissions to the community-based sexual offense treatment program operated by the Department of Psychology in Central District (Ontario) Parole, Correctional Service of Canada were included in the present investigation. These clients received treatment between 2005 and 2009 and represent consecutive admissions to the program. The treatment program was open-ended and clients began attending treatment shortly after their release to the community. Groups met every 2 weeks and, after clients had been deemed to make sufficient progress, attended a group that met once a month. Clients typically attended treatment until the end of their period of parole. For clients serving life sentences, treatment would continue until such time as both treatment and parole staff agreed that no further interventions were required. Treatment was conducted in line with the principles of the IRATS Model. Every effort was made to ensure that issues associated with establishing and maintaining the therapeutic alliance were prioritized. For example, therapists begun by asking clients to “check in” regarding what had occurred over the last 2 weeks (or month) rather than beginning sessions with a list of topics to be covered in that session. All sessions were facilitated by staff with graduate training in psychology and virtually all treatment groups were facilitated by at least one registered psychologist. All clients attending the community-based sexual offense treatment program signed a detailed consent form indicating that information collected during treatment could be used for research purposes. The average age of subjects included in the present investigation was 40.67 years at the commencement of their sentence. With reference to risk, all treated subjects were scored on the Static-99R (Helmus et al., 2012), an actuarial measure designed to assess the risk of sexual offense recidivism. The Static-99R is an empirically derived actuarial risk assessment tool designed to predict sexual and violent recidivism in adult males who have been charged/convicted of at least one sexual offense (see also www.static99.org). It has 10 items with the total score ranging from −3 to +12. The Static-99R has been subjected to a number of evaluation studies that demonstrate that the instrument predicts sexual recidivism at well over chance levels (Lee & Hanson, 2021). The mean Static-99R score for treated subjects was 2.67, placing the average subject at the low end of the moderate risk range on this instrument. Follow-up data for the treated group ended on December 31, 2015.
A comparison group, consisting of 55 untreated clients who had been convicted of one or more sexual offenses from the Ontario Region of CSC, was included in the present sample. These subjects were described in detail in Abracen and Looman (2016). These individuals attended a variety of psychoeducational programs (e.g., cognitive skills) recommended by parole staff. Programs were group based and facilitated by program officers with a variety of educational backgrounds. This sample consisted of individuals included in the Millhaven assessment unit (MAU), a reception center for all individuals convicted of sexual offenses in the Ontario Region of CSC, between the years 1993 and 1998. From among the MAU sample, a group of individuals listed as having not attended institutional sex offense treatment were selected. Subsequent reviews of additional databases were conducted to ensure that none of these clients attended community-based treatment. The reason that clients did not attend treatment was, however, unavailable (e.g., treatment was not offered at a particular site, client refused treatment). Recidivism data regarding the comparison sample was retrieved from the Royal Canadian Mounted Police (RCMP) Finger Print Service (FPS) in May 2008. Given that the treated group received treatment from 2005 to 2009, there was a 3-year period of overlap between the two groups (i.e., 2005–2008). Although it may be argued that these two groups essentially involved different cohorts of offenders with limited overlap in terms of follow-up, all individuals included in the study were assessed in the Ontario Region of CSC. In addition, sentencing guidelines in the Ontario Region have remained largely unchanged with exception to legislation regarding child pornography. Given that virtually all of the individuals included in the present investigation had a history of hands-on sexual offenses, changes with reference to legislation regarding viewing child pornography were believed to have had little impact regarding the current group of clients who had all received sentences of 2 years or more.
An earlier risk assessment instrument, the RRASOR (Hanson, 1997), which includes four items later incorporated into the Static-99R, was scored for all participants. Unfortunately, data were not available to score the Static-99R for all comparison participants. Although the Static-99R is a more robust predictor of recidivism than the RRASOR, the RRASOR nonetheless has been shown to predict sexual offense recidivism. The mean RRASOR score for the treated sample (N = 90) was 1.33. The mean score on the RRASOR for the comparison group (N = 54) was 0.88. A t-test was computed to compare the means for the two groups with reference to RRASOR scores. Results indicated that there were no significant differences between treated and comparison subjects with reference to RRASOR score (p > .05). A t-test was also computed regarding length of follow-up for both groups. With reference to the treated group (N = 89), the mean follow-up time was 8.17 (SD = 1.76) years. Mean follow-up time for the comparison group subjects (N = 55) was 6.9 (SD = 1.51) years. Results indicated that the treated group was followed for a significantly longer period of time than comparison group subjects (t = −4.65, df = 142, p < .000).
Treatment Program
The community sex offense program operated in Central District Ontario (Parole) between 2005 and 2009 was designed in accordance with the IRATS Model described above. Clients attending this program were first assessed by clinical staff (all of whom had graduate-level training in psychology and were registered mental health professionals). Clients were primarily seen in group; however, individual therapy was provided on an as-needed basis. For example, for clients experiencing issues associated with SMI, individual therapy was provided until such time as clients were able to attend the group-based program. Treatment was in accordance with the tenets of the IRATS model in that issues associated with criminogenic needs (e.g., criminal thinking and personality) as well as issues associated with mental illness and attachment-related concerns (e.g., intimacy and relationship issues) were addressed on an ongoing basis. Sessions were open-ended and clients would join the group as they were released to the community. Topics covered in group were in accordance with a cognitive-behavioral model and information was presented as necessary given the needs of individual group members. Frequent topics of discussion included how to address issues associated with dating, management of intimate relationships, management of negative emotionality, and mental health–related concerns, as well as issues associated with community notification. Abracen and Looman (2016) describe the process of community management in more detail. The reader is referred to this text for a more detailed description of the program.
It should be noted that many of the clients were required to reside in a community residential facility either operated by CSC or contracted to CSC when first released to the community. As there was frequent communication between treatment staff and other members of the team who worked with our clients (e.g., parole officers, staff at the halfway houses), this allowed treatment staff to have some information regarding the client’s well-being while not being seen by treatment staff. From our perspective, such information was critical to help identify challenges faced by our clients when first released. Issues raised by other staff members (e.g., parole officers) would frequently be the subject of discussion with clients. The goal, however, was always to work collaboratively with clients, and all staff emphasized that the aim of treatment was to maintain clients in the community and not to adopt a punitive approach. Issues associated with developing and maintaining the therapeutic alliance with clients were stressed, both with clients and when providing feedback to other staff members working with the clients with whom we interacted.
Analytic Strategy
Clients attending sexual offense treatment were first compared with comparison group clients to determine whether there were absolute differences with reference to rates of general, sexual, and/or violent recidivism. Chi-square analyses were used to determine whether differences were observed between treated and comparison clients on these dependent measures. Treated clients’ actual rates of sexual offense recidivism were then compared with predicted rates of recidivism based on Static-99R scores. Differences between actual and predicted rates of recidivism were compared using recently published data regarding the Static-99R to determine whether the actual/predicted rates were significantly different. To control for differences between treated and comparison clients with reference to length of follow-up, Cox regression analyses were then performed.
Results
Chi-square analyses were computed with reference to any recidivism (i.e., general, violent, or sexual). With reference to treated clients, six of the 90 treated clients recidivated in any way (6.3%). Among comparison group subjects, 18 of the 55 subjects recidivated in any way (32.7%). Chi-square analyses indicated significant differences between groups, χ2 (1) = 16.77, p = .001; Cramer’s V = .340, p = .001. With reference to violent recidivism, significant differences were also found between treated (3.3%) and comparison clients (14.5%) in terms of rates of recidivism, χ2 (1) = 6.12, p = .013; Cramer’s V = .21, p = .013. Finally, with reference to sexual recidivism, significant differences were also found between treated and comparison group clients in spite of there being relatively low rates of recidivism across the entire sample. Among treated clients, only one of 89 participants recidivated sexually (1.1%), whereas four of the 55 comparison group clients recidivated sexually (7.3%), χ2 (1) = 3.84, p = .05, Cramer’s V = .163, p = .050. Thus, the effect was medium for any recidivism and small for sexual and violent recidivism.
With reference to the treated clients, recent norms have been made available for the Static-99R (Lee & Hanson, 2021). These norms include both 5- and 10-year predicted rates for sexual recidivism as well as 95% confidence intervals (CIs) regarding these listed rates. As the treated clients were followed for just over 8 years, the 10-year rates for the Static-99R appear to be most appropriate as a basis of comparison. Lee and Hanson (2021) list a 10-year rate of sexual recidivism for a score of 3 (the average Static-99R score for the current sample of treated clients was 2.67, as noted above) as 6.5% (95% CI = [5.8, 7.2]). Given that the observed rate does not overlap with the 95% CI associated with this score, it can be argued that the observed rate is significantly lower than the predicted rate of sexual offense recidivism based on the Static-99R. For the observed rate of sexual offense recidivism among treated subjects to overlap with the 95% CI associated with a particular score with reference to the Static-99R, treated subjects should have scored −2 on the Static-99R (95% CI = [0.8, 1.4]). According to the standards developed for the Static-99R, this represents an equivalency with a group rated as two risk levels lower than those observed for the current treated group.
To control for differences between groups in terms of risk and length of follow-up, group membership was entered into a Cox regression analysis, with the RRASOR score entered on the second step. The analyses were conducted for general and violent (including sexual) only. These analyses were not conducted for sexual recidivism due to the very low rate of this type of offending. For any recidivism, the omnibus test on the first step was significant, χ2 (1) = 38.40, p = .001. The RRASOR was entered on the second step, χ2 (2) = 42.64, p = .001, with the change from the first step being significant, χ2 (1) = 7.05, p = .001 (see Table 1 and Figure 2 for more detail). For violent (including sexual) recidivism, once again only group membership was a significant predictor of χ2 (2) = 17.32, p < .001. RRASOR score failed to reach conventional levels of statistical significance, χ2 (1) = 0.14, p < .701 (see Table 1 and Figure 3 for more detail).
Cox Regression for Group Membership and RRASOR
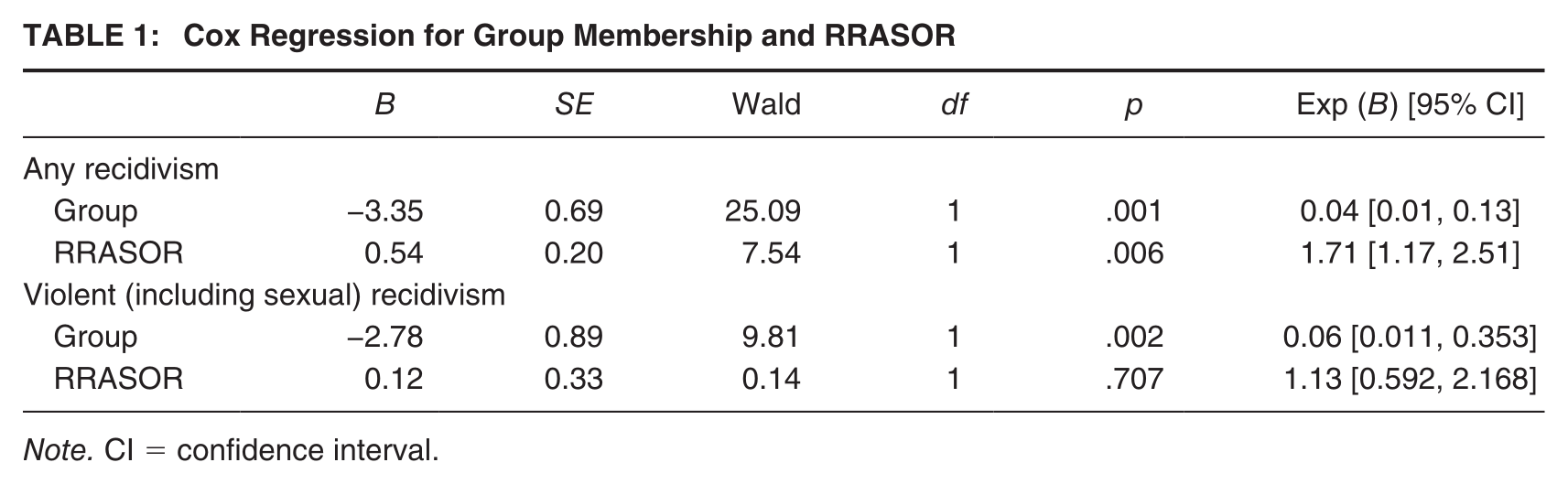
Note. CI = confidence interval.
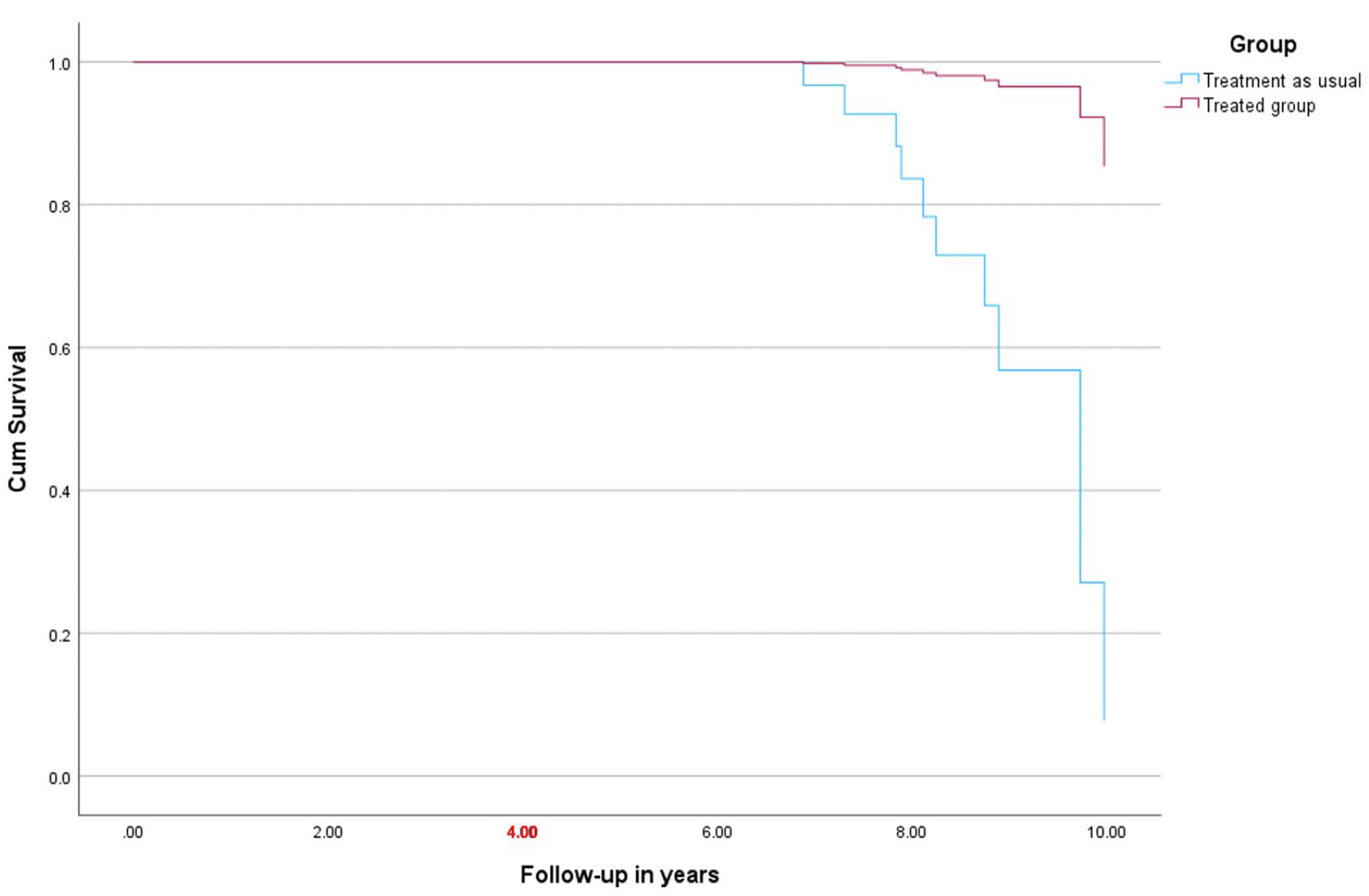
Survival Curve for Group Membership for Violent Recidivism
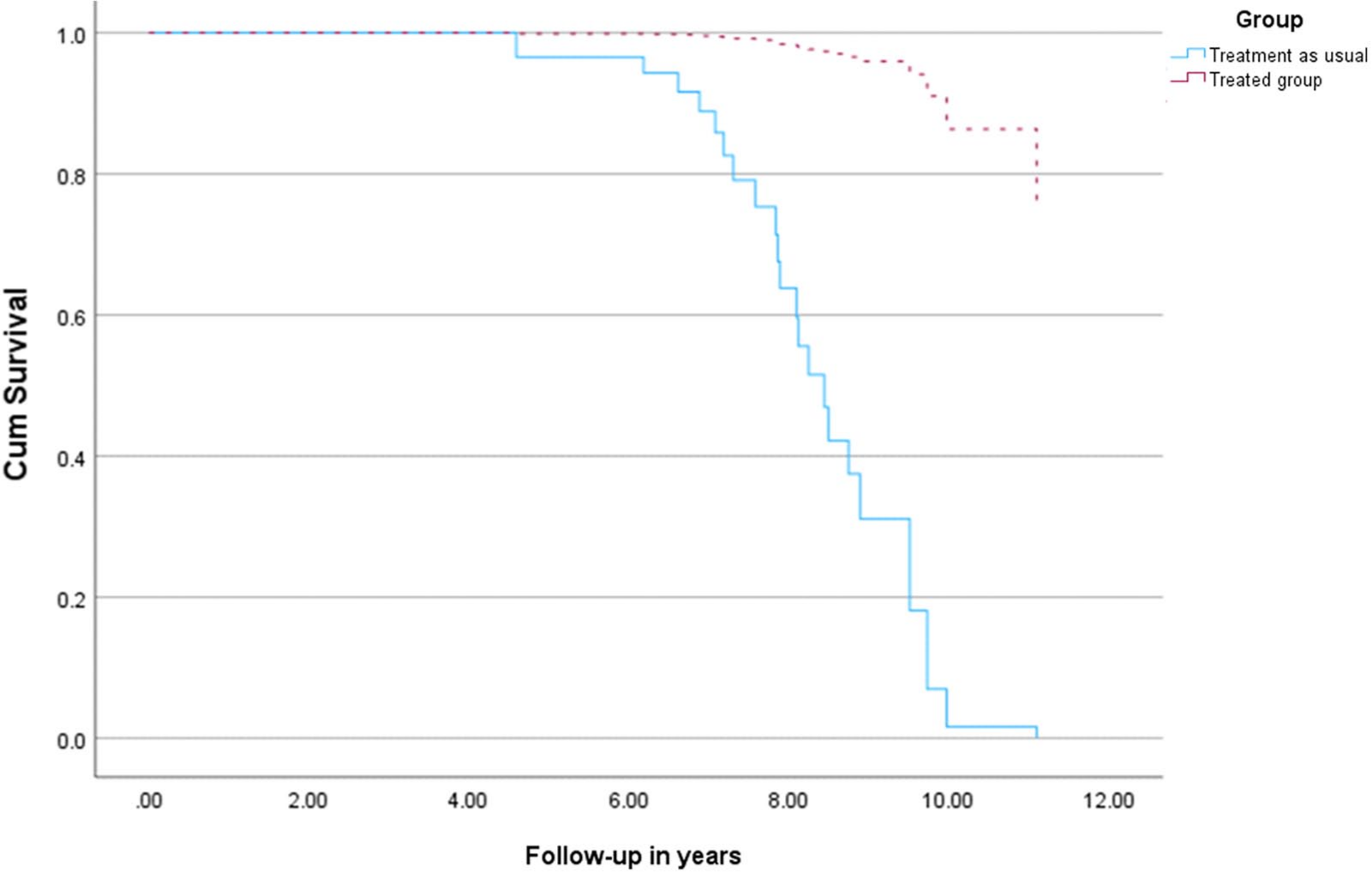
Survival Curve for Group Membership for General Recidivism
Discussion
The present study compared a group of clients attending sexual offense treatment with a comparison group who received standard correctional programming that was recommended by correctional staff. None of the comparison clients received sex offense–specific programming institutionally. All clients were followed up for an extended period of time. Results indicated that those clients attending sexual offense treatment programming evidenced virtually no sexual recidivism over an 8-year period of follow-up (i.e., only one subject recidivated sexually). When compared with comparison group clients, results indicated that significant differences were observed between the treated and comparison samples in the hypothesized direction. That is, despite being followed for a significantly longer period of time than the comparison group subjects, only one treated client (vs. four comparison group members) recidivated sexually.
It is our view that these data are significant for several reasons. First, there are few contemporary community outcome studies with individuals convicted of having committed sexual offenses that have compared treated clients with an untreated group from the same correctional jurisdiction using officially recorded sexual conviction data. Issues associated with the methodological limitations of contemporary sex offender treatment programs have been raised by others (e.g., Abracen & Looman, 2016; Schmucker & Lösel, 2015). Schmucker and Lösel (2015), for example, note that they were only able to identify 29 comparison studies that met the inclusion criteria for their meta-analysis on sexual offense treatment (only 20 of which reported on sexual recidivism per se). In addition, it has been observed that the sex offense outcome literature has demonstrated moderate effect sizes when sexual offense recidivism has been investigated (e.g., Hanson et al., 2002; Lösel & Schmucker, 2005). These data are in accordance with effect sizes observed for general offender treatment (e.g., Lösel, 2012). Although these data suggest that contemporary treatment programs are effective, they also suggest that there is much room for improvement in terms of outcome.
Olver et al. (2020), in accordance with the results of the meta-analysis reported by Gannon et al. (2019), noted that the specialized prison-based sex offender program operated by William Marshall and his colleagues was associated with substantial reductions in sexual recidivism relative to standard correctional sex offense treatment programming (5.6% adjusted rate for sexual recidivism vs. the 10.7% unadjusted rate for standard sex offense treatment programming operated by CSC over an 8-year follow-up). It should be noted that the Rockwood program operated by William Marshall and his colleagues had many features in common with the program evaluated in the current investigation. For example, both programs were operated by psychology staff and used cognitive-behavioral (CBT)-based interventions that expanded upon the range of treatment targets dictated by RNR-based principles and had an attachment-based perspective. Nonetheless, clients attending the Rockwood Program evidenced similar rates of sexual offense recidivism to the group of comparison clients reported in the current study (7.27% vs. 5.6% for the Rockwood Program).
Aside from there being relatively few contemporary outcome studies employing appropriate comparison groups (Olver et al., 2020, being an exception), the lack of treatment models specifically developed for use with individuals convicted of sexual offenses also represents a challenge to program developers. Although models such as the MTM (Seto, 2019) are theoretically elegant, such perspectives only provide limited guidance to clinicians regarding “what works” in correctional programming. The present research adds to the existing literature by presenting a perspective developed based on a review of the empirical literature, which is further supported by a number of long-term outcome studies including the data reported above. We have noted that perspectives such as the GLM have not been supported by long-term outcome studies regarding its efficacy. This is especially true when one considers controlled studies using sexual offense recidivism as an outcome measure (Mallion et al., 2020). Although there are aspects of the GLM that overlap with the IRATS Model (e.g., the importance of the therapeutic alliance, the need to focus on the complex treatment needs of individual clients, the need to focus on approach goals rather than the elimination of criminogenic needs alone), other aspects of the models diverge. For example, the IRATS includes only treatment targets that have been explicitly supported by the empirical literature. For illustrative purposes, we have included a copy of the IRATS in Figure 1. When one looks at the available literature regarding community-based treatment of sexual offenses, studies indicate that community-based interventions are certainly effective though, to the best of our knowledge, no research has observed the near-zero sexual recidivism reported in the present investigation. For example, Lambie and Stewart (2012) investigated a community-based program for sexual offenses in New Zealand. Treatment was associated with lower rates of sexual recidivism (8.1% for all participants treated in the community-based programs) when compared to a probation comparison group. Elliott and Beech (2013) produced a review of data regarding Circles of Support and Accountability (CoSA)-based treatment for sexual offenses. Although the study provided a cost–benefit analysis associated with CoSA programming, the authors report that CoSA-based treatment was associated with an approximate 50% reduction in both sexual and nonsexual recidivism. The authors identified four relevant studies in the literature and nine comparisons listed in these four studies which included comparisons between CoSA attendees and either a matched sample or normative risk data for sexual offending. Actual rates of sexual reoffending are not listed however. A more recent review of the research related to CoSA treatment (Clarke et al., 2017), however, was more critical of the outcome data reported. These authors identified three relevant outcome studies as well as 12 papers or reports. The authors noted that studies with controls generally report lower recidivism among Circles members although there were few statistically significant differences.
Craissati and Blundell (2016) examined a community service directed toward high-risk mentally disordered sex offenses and reported a 11% sexual offense recidivism rate over 40 months. Interestingly, in accordance with the IRATS Model, failures were more likely to have either a history of trauma or higher Static-99R scores. Similar rates of reoffending were noted by Elliott et al. (2019) in a U.K. community sample of individuals with convictions for indecent images of children. These authors observed a 12.6% reconviction rate for their full sample of 87 offenders over a 13-year average follow-up.
Limitations of the Current Investigation
First, although the current study employed a comparison group of treatment as usual clients, the treatment and comparison group data were not contemporaneous in that the comparison group data consisted of clients reported in an earlier investigation by our team. Although the follow-up periods for the groups overlapped, this is not to say that they were identical. Whether any influence of factors such as changes to sentencing guidelines or other issues impacted recidivism rates for the two groups is not known. As well, little background information was available regarding comparison group clients. For example, it would have been useful to be able to compare the treatment and comparison groups with reference to psychiatric history or number of previous sexual offenses.
Second, the present investigation included relatively small number of treated and comparison group clients. Ideally, it would have been better to include a larger number of individuals. Nonetheless, at least some background information related to risk (e.g., age) was available as well as actuarial data related to risk level.
Conclusions
It has long been argued that individuals convicted of sexual offenses should receive extended periods of incarceration to maintain public safety, notwithstanding the fact that most sexual offenses occur among individuals who are known to one another (see Wilson et al., 2020, for a discussion regarding public perception of sexual offenses). Among other cogent arguments made by Wilson et al. (2020), the fact that many government-driven sexual violence prevention policies are influenced by high-profile cases and the public reaction to them suggest that existing policy is based at least in part upon public apprehension toward individuals convicted of sexual offenses rather than empirically derived decision-making. This is particularly the case in the United States with legislation such as the Adam Walsh Child Protection and Safety Act (2006) and Megan’s Law (1996). In addition, registration and community notification practices have been mandated in 50 states in spite of the fact that most research has failed to reveal any significant impact of such policies on recidivism (see Wilson et al., 2020, for a review of this research).
Although contemporary treatment programs have clearly resulted in reduced rates of sexual offense recidivism in comparison to no treatment or treatment as usual comparison groups, the reality remains that very little such research has been conducted to date. RNR-based programs have resulted in only low to moderate effect sizes based on the available literature.
To the best of our knowledge, no study examining the long-term recidivism rates of individuals convicted of sexual offenses with hands-on sexual offenses has managed to find the near-zero rates of sexual offense recidivism observed in the current investigation. These data suggest that community-based programs, using comprehensive treatment models such as the IRATS, and operated by psychology staff, can produce results in line with community expectations regarding community safety.