
Abstract
People who are incarcerated globally exhibit higher rates of mental health issues and adverse childhood experiences than the general population, yet prisons seldom address trauma’s role. This systematic review analyzed the mental health outcomes of implementing Trauma-Informed intervention programs with adults being incarcerated. Following PRISMA guidelines, systematic searches of electronic databases (e.g., PubMed) and a manual search identified relevant studies. Thirteen empirical studies were identified, featuring seven interventions, with Seeking Safety being the most common. All studies explored the effects of their respective intervention and/or treatment program on participants’ mental health, particularly traumatic symptoms and/or other mental health outcomes. Most samples included women who were incarcerated, with one study involving incarcerated men. Trauma-informed prison programs improved incarcerated individuals’ mental health and reduced recidivism. By highlighting gaps, such as limited studies on incarcerated males or research in European contexts, this study offers critical insights for improving and creating these programs.
Introduction
Several studies indicate that many people who are incarcerated (PI) experience significant mental health challenges, with correctional facilities reporting substantially higher rates of individuals suffering from mental health and substance use disorders compared with the general population (Fovet et al., 2020). The prison environment itself exacerbates these challenges, increasing the risk of developing certain mental disorders due to factors such as institutionalization, lack of autonomy, and exposure to violence (Edgemon & Clay-Warner, 2019; Raggio et al., 2017).
In addition, a significant proportion of males (Morrison et al., 2019) and females (Jewkes et al., 2019) who are incarcerated enter prison with high levels of preexisting trauma symptoms. Such trauma, defined as an emotional and psychological response to a deeply distressing or disturbing event/ experience (American Psychiatric Association [APA], 2013), often includes adverse childhood experiences (ACEs; Crouch et al., 2019). ACEs encompass a range of challenging situations that occur before the age of 18 and, while not all of them are necessarily traumatic, they have been associated with an increased likelihood of involvement in the criminal legal system (Wright et al., 2019). Previous research highlights higher rates of ACEs, mental health issues, and substance use among justice-involved individuals (Altintas & Bilici, 2018; Andrews & Bonta, 2016). Moreover, those who have experienced childhood trauma and/or trauma-related disorders are more likely to encounter and repeatedly interact with the criminal justice system (Altintas & Bilici, 2018).
Beyond preincarceration trauma, individuals in correctional settings are also at risk of experiencing further trauma during incarceration, which can not only contribute to new trauma but also exacerbate preexisting trauma symptoms (Yoon et al., 2017). Consequently, Posttraumatic Stress Disorder (PTSD), a condition that may develop following exposure to potentially traumatic events and cause ongoing symptoms that lead to significant suffering or functional impairment (APA, 2013), is more prevalent among people who are incarcerated than in the general population (Baranyi et al., 2018).
Despite the well-documented impact of trauma on mental health, the prison environment often emphasizes offense culpability and punishment over rehabilitation, failing to address the effects of trauma on PI’s mental health (Levenson & Willis, 2019). To mitigate these effects and specifically attend to trauma and PTSD-related symptoms, integrating Trauma-Informed (TI) Programs within prisons is crucial (DeCandia et al., 2014). TI Programs consist of specific, structured, clinical interventions delivered by trained professionals (DeCandia et al., 2014). These programs operate within a framework that recognizes the prevalence and impact of trauma, integrates this awareness into organizational practices, and actively seeks to prevent re-traumatization (Substance Abuse and Mental Health Services Administration [SAMHSA], 2014). In correctional settings, TI programs highlight how prison conditions can trigger or intensify past trauma, potentially exposing PI to additional traumatic events (Levenson & Willis, 2019). Their primary objective is to identify, comprehend, and mitigate the enduring traumatic exposure consequences, even in instances where the individual may not acknowledge that their behavior is intricately linked to the traumatic event (Kubiak et al., 2017). These interventions adopt a multimodal approach, incorporating various evidence-based therapeutic strategies, including psychoeducation, role-playing, cognitive-behavioral restructuring, and grounding skills tailored to address trauma-related challenges (Covington, 2013).
Although TI programs and Trauma-Informed Care (TIC) share similar principles, they differ in scope and focus. Unlike structured TI intervention programs, TIC represents a broader approach that integrates trauma awareness into general institutional practices, emphasizing supportive relationships, addressing current needs, and assisting individuals in achieving their evolving goals (Bloom, 2013).
While effectiveness research of TI programs remains relatively limited, some systematic reviews and meta-analyses have examined this type of intervention over the past 15 years (e.g., King, 2017; Malik et al., 2023; Yoon et al., 2017). For instance, King (2017) found that TI interventions generally led to positive outcomes, with decreases in PTSD and trauma-related symptoms being more pronounced in treatment groups than in treatment-as-usual (TAU) or waitlist groups. However, these improvements appeared to be additive to changes occurring in the comparison groups, suggesting that while TI interventions contribute to symptom reduction, other factors or baseline interventions may also influence outcomes. In addition, Malik et al. (2023) reported in their meta-analysis of 16 studies a small yet statistically significant overall effect size for TI interventions in reducing PTSD symptoms compared with prison control groups. Finally, Yoon et al. (2017) reviewed 37 randomized clinical trials, including seven implementing TI interventions in correctional settings. While these interventions contributed to reductions in PTSD and anxiety symptoms, their statistical significance was very low in the meta-analysis (Yoon et al., 2017).
These findings provide important insights into interventions addressing mental health in PI. However, not all studies specifically focused on TI programs (e.g., Yoon et al., 2017), while others concentrated on specific subpopulations or outcomes, such as women who are incarcerated (King, 2017) or PTSD symptomatology (Malik et al., 2023). This underscores the need for a more focused examination of TI programs and their mental health outcomes, which this systematic literature review (SLR) aims to address. By evaluating diverse mental health outcomes, this review seeks to provide more precise insights into the impact of TI interventions on both males and females who are incarcerated, thereby contributing to the knowledge base concerning this population. These considerations substantiate the scientific and societal relevance of this SLR, which endeavors to address the following research question: What are the mental health outcomes of implementing TI intervention programs in PI? Accordingly, this study sought to (a) identify the scope of TI programs available to PI and (b) examine their effects on mental health outcomes.
Method
Research Strategy
This SLR adhered to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines (Moher et al., 2009). The investigation was conducted on February 15, 2023, and updated on September 2, 2024, employing multiple scholarly databases, namely, EBSCOhost, PubMed, and Web of Science. The search strategy used the following terms: (inmates OR detainees OR prisoners OR offenders) AND trauma AND (intervention OR treatment). A manual search was executed to identify any articles that may not have been captured through the initial database searches. All identified references were then exported and meticulously managed using Rayyan online software (Ouzzani et al., 2016). This systematic and methodical approach ensured a thorough and systematic retrieval of relevant literature for inclusion in the review.
Eligibility Criteria
The following inclusion criteria were systematically applied: (a) only empirical studies-quantitative and/or qualitative; (b) focused exclusively on the implementation of TI intervention programs within the prison context; and (c) targeting PI, irrespective of gender, aged 18 years or older. Although (d) no temporal or geographical restrictions have been applied, the selected studies had to be written (e) in Portuguese, English, or Spanish. This requirement is based on the authors’ fluency in these languages, ensuring an accurate and comprehensive analysis of the research without the limitations of translation, and allowing for a deeper understanding of the studies’ context and nuances. Exclusion criteria were established: (a) studies exclusively addressing TI intervention programs, without specific reference to their implementation within prison settings; (b) studies specifically centered on TIC (i.e., focused on general principles for addressing trauma, without involving structured intervention programs); and (c) materials falling under the category of gray literature, legislation, news, book chapters, unpublished studies, conference proceedings, literature reviews and theoretical articles.
Selection of the Studies and Analysis of the Results
Two independent researchers conducted the studies selection for eligibility. Discrepancies arising during this process were deliberated and resolved through consultation between the researchers, with oversight from a third reviewer. Initially, the selection process involved analyzing titles and abstracts according to predefined eligibility criteria. In case of doubt, the corresponding full text was retrieved for comprehensive assessment. Following a thorough examination of the full articles, selections were made based on alignment with the research question, determining their inclusion or exclusion from the study. The comprehensive search across the designated databases and the supplementary manual search procedure yielded a total of 5443 articles. Subsequent duplicate articles removal resulted in the elimination of 1556 entries, leaving 3887 articles for further consideration. The analysis of titles and abstracts led to the inclusion of 28 articles. Of these, 15 studies were excluded: five did not focus on the implementation of TI programs in PI; four were not empirical studies; and six implemented TI care principles instead of TI intervention programs. Consequently, this SLR ultimately comprised 13 articles (see Figure 1). Detailed information, encompassing general study information (references; sample’s country); participant details (sample size, sex, and age); study design specifics (methodology, aims, instruments, control group, TI intervention programs); and main results and conclusions were extracted and organized for reference (see Tables 2 and 3).
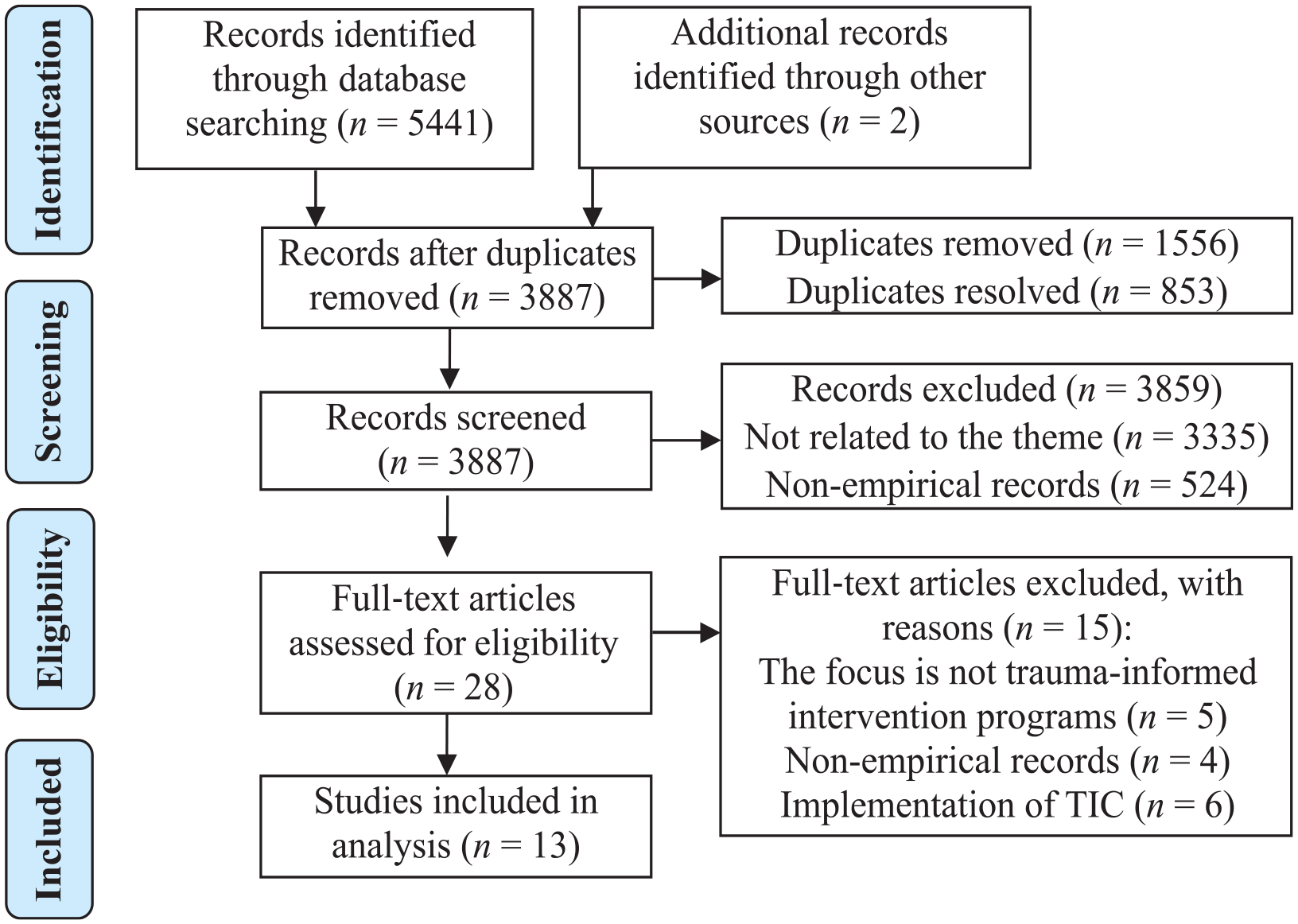
PRISMA Flow Diagram
Quality Assessment
To assess the quality of the studies included in this SLR, two independent reviewers employed Crowe’s tool (CCAT), a Critical Assessment Tool, comprising CCAT Form and CCAT User’s Guide (Crowe & Sheppard, 2011; Crowe et al., 2012). The CCAT Form encompasses eight distinct categories and 22 items, each of which can be classified as present, absent, or not applicable, providing guidance for scoring the category. Categories evaluate aspects such as research design, sampling, data collection, results, and discussion. Each category is scored on a scale from zero to five points and only whole number scores can be awarded. The cumulative score is capped at 40 points. All articles included in this SLR have moderate quality standards (see Table 1). To ensure reliability, Cohen’s Kappa coefficient was employed, revealing a strong agreement index between reviewers (K = .89, p < .001).
Quality of Studies Assessed Using the Crowe Critical Appraisal Tool (CCAT)
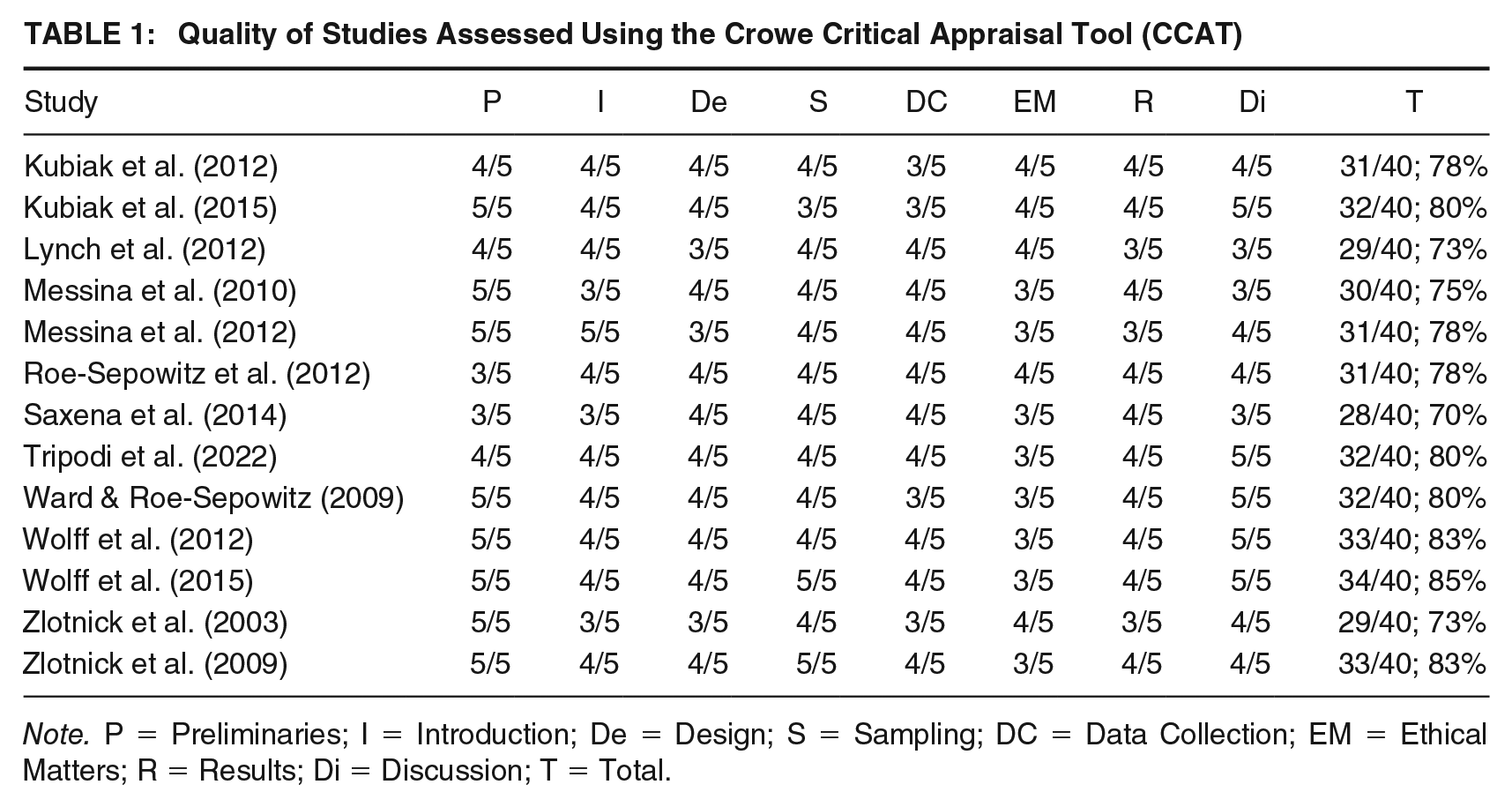
Note. P = Preliminaries; I = Introduction; De = Design; S = Sampling; DC = Data Collection; EM = Ethical Matters; R = Results; Di = Discussion; T = Total.
Results
Initially, global characteristics of studies were analyzed (see Table 2). Subsequently, to address the research question, the outcomes related to mental health and recidivism were presented (see Table 3).
Studies’ Characteristics
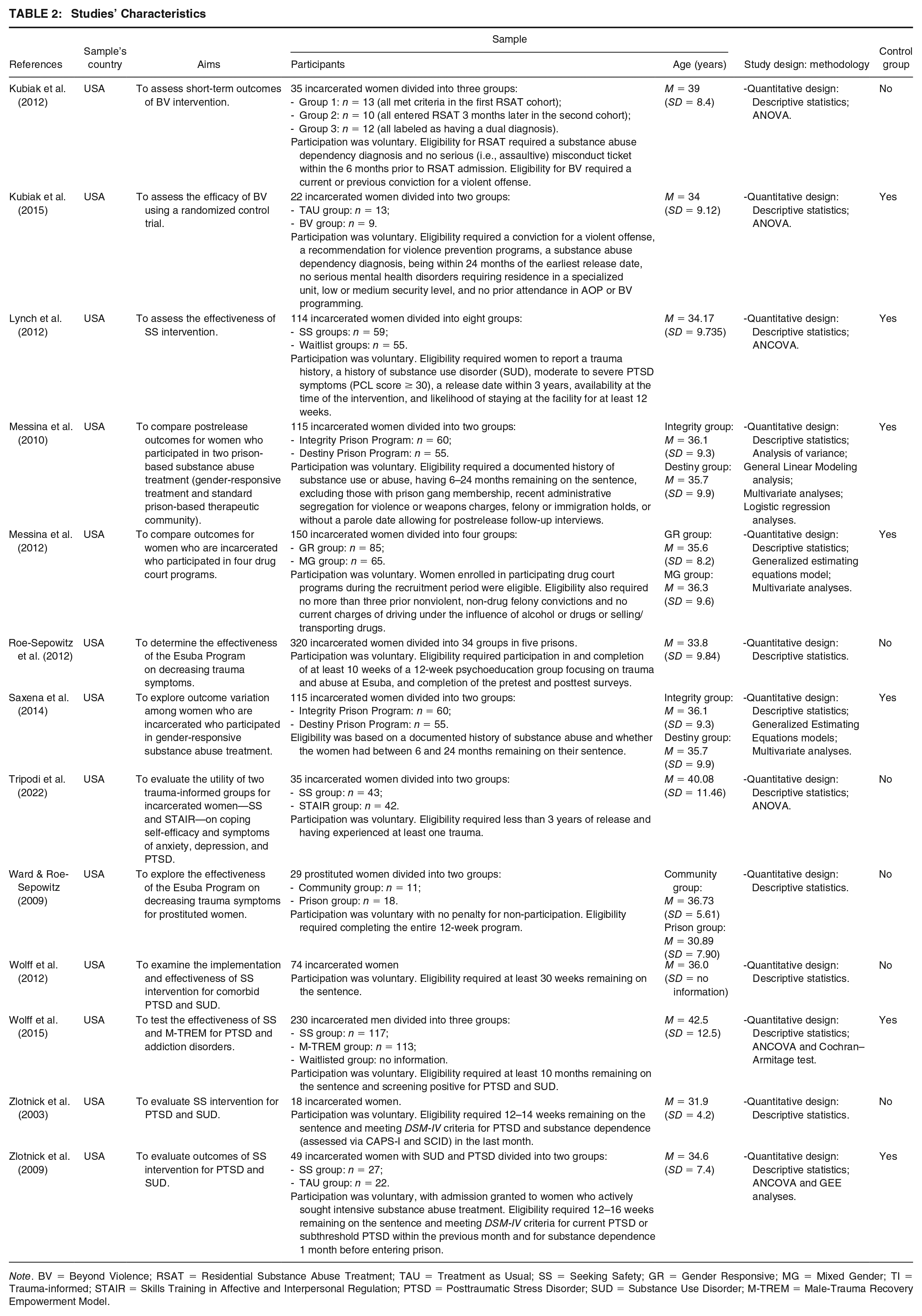
Note. BV = Beyond Violence; RSAT = Residential Substance Abuse Treatment; TAU = Treatment as Usual; SS = Seeking Safety; GR = Gender Responsive; MG = Mixed Gender; TI = Trauma-informed; STAIR = Skills Training in Affective and Interpersonal Regulation; PTSD = Posttraumatic Stress Disorder; SUD = Substance Use Disorder; M-TREM = Male-Trauma Recovery Empowerment Model.
Interventions’ Characteristics and Results
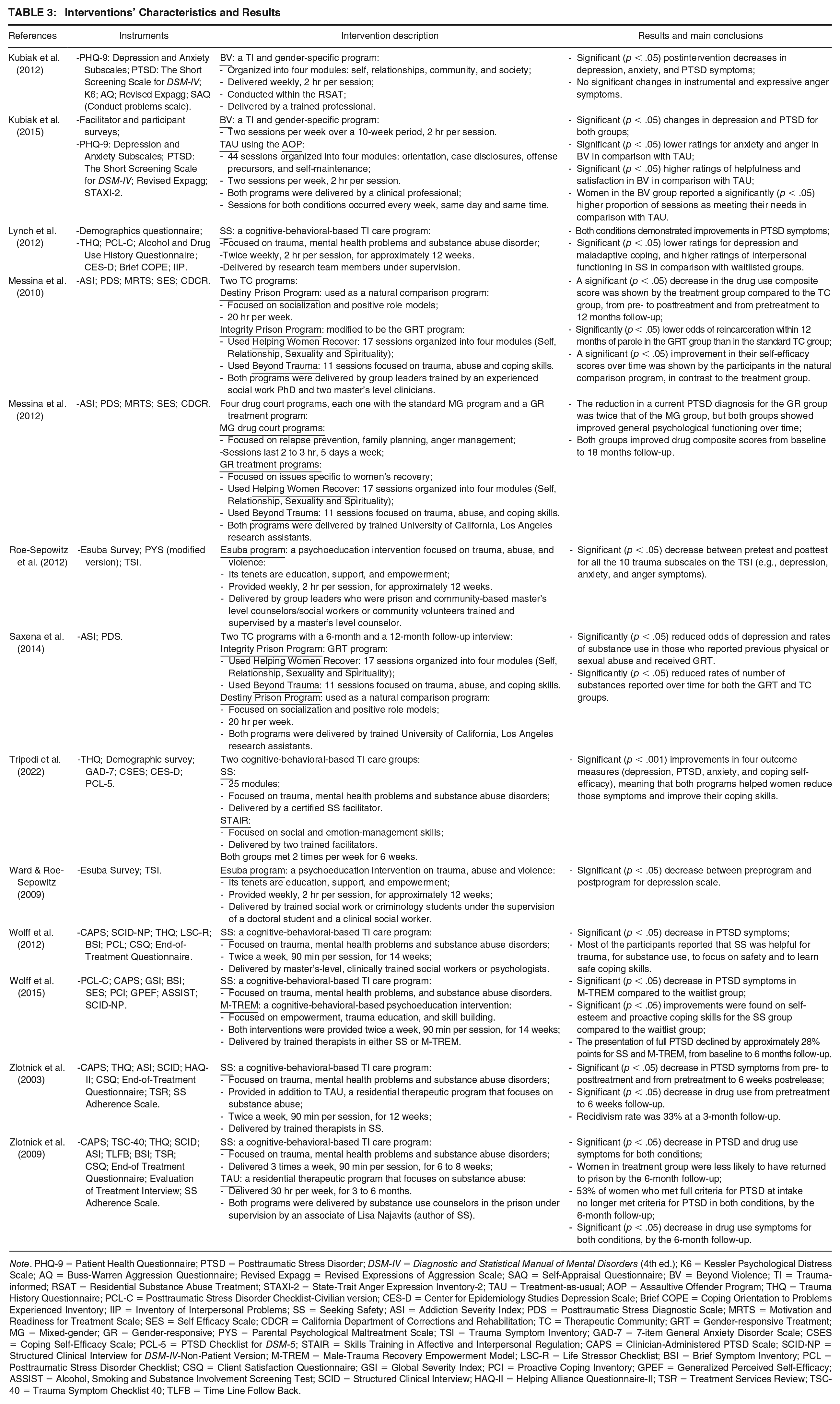
Note. PHQ-9 = Patient Health Questionnaire; PTSD = Posttraumatic Stress Disorder; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders (4th ed.); K6 = Kessler Psychological Distress Scale; AQ = Buss-Warren Aggression Questionnaire; Revised Expagg = Revised Expressions of Aggression Scale; SAQ = Self-Appraisal Questionnaire; BV = Beyond Violence; TI = Trauma-informed; RSAT = Residential Substance Abuse Treatment; STAXI-2 = State-Trait Anger Expression Inventory-2; TAU = Treatment-as-usual; AOP = Assaultive Offender Program; THQ = Trauma History Questionnaire; PCL-C = Posttraumatic Stress Disorder Checklist-Civilian version; CES-D = Center for Epidemiology Studies Depression Scale; Brief COPE = Coping Orientation to Problems Experienced Inventory; IIP = Inventory of Interpersonal Problems; SS = Seeking Safety; ASI = Addiction Severity Index; PDS = Posttraumatic Stress Diagnostic Scale; MRTS = Motivation and Readiness for Treatment Scale; SES = Self Efficacy Scale; CDCR = California Department of Corrections and Rehabilitation; TC = Therapeutic Community; GRT = Gender-responsive Treatment; MG = Mixed-gender; GR = Gender-responsive; PYS = Parental Psychological Maltreatment Scale; TSI = Trauma Symptom Inventory; GAD-7 = 7-item General Anxiety Disorder Scale; CSES = Coping Self-Efficacy Scale; PCL-5 = PTSD Checklist for DSM-5; STAIR = Skills Training in Affective and Interpersonal Regulation; CAPS = Clinician-Administered PTSD Scale; SCID-NP = Structured Clinical Interview for DSM-IV-Non-Patient Version; M-TREM = Male-Trauma Recovery Empowerment Model; LSC-R = Life Stressor Checklist; BSI = Brief Symptom Inventory; PCL = Posttraumatic Stress Disorder Checklist; CSQ = Client Satisfaction Questionnaire; GSI = Global Severity Index; PCI = Proactive Coping Inventory; GPEF = Generalized Perceived Self-Efficacy; ASSIST = Alcohol, Smoking and Substance Involvement Screening Test; SCID = Structured Clinical Interview; HAQ-II = Helping Alliance Questionnaire-II; TSR = Treatment Services Review; TSC-40 = Trauma Symptom Checklist 40; TLFB = Time Line Follow Back.
Characteristics of Studies
Thirteen empirical studies, all conducted in the United States, published between 2009 and 2022, were included in the analysis, employing seven different interventions. Among these, Seeking Safety was the most frequently used intervention, with six studies employing it. Each study sought to investigate the impact of its respective intervention and/or treatment program on participants’ mental health, specifically focusing on traumatic symptoms and/or other mental health outcomes. Sample sizes varied across studies, ranging from N = 12 to N = 320, comprising 1306 participants. Most participants were females who are incarcerated (n = 12), with one study including males who are incarcerated. Participants’ mean age ranged from 30.89 (SD = 7.90) to 42.5 years (SD = 12.5), although one study did not furnish complete information. Methodologically, all studies adopted a quantitative research approach, with seven incorporating a control group, and six relying solely on intervention groups. All interventions included TI programs. Concerning measurement instruments, all studies used surveys designed to assess various mental health dimensions.
Characteristics of TI Interventions
Seven different interventions were identified: Beyond Violence (BV; Covington, 2013), Seeking Safety (SS; Najavits, 2002), Esuba (Bedard et al., 2003), Skills Training in Affective and Interpersonal Regulation (STAIR; Cloitre & Schmidt, 2015), Male-Trauma Recovery Empowerment Model (M-TREM; Fallot et al., 2001), Helping Women Recover (HWR; Covington, 2000), and Beyond Trauma (BT; Covington, 2003). HWR and BT are incorporated into the Integrity model, a gender-responsive treatment (GRT). To determine whether these interventions were truly TI, they were analyzed based on the principles of TIC, which include Safety; Trustworthiness and Transparency; Peer Support; Collaboration and Mutuality; Empowerment, Voice and Choice; Cultural, Historical; and Gender Issues (SAMHSA, 2014).
All interventions emphasized the importance of creating environments where individuals feel physically and psychologically safe. For instance, BV, SS, and M-TREM particularly prioritize establishing a sense of safety while addressing trauma and substance abuse. Integrity, Esuba, and STAIR foster safety by focusing on trust-building and validation throughout treatment. All the included programs promote open, transparent relationships, which are vital for supporting trauma survivors throughout their recovery journey. In addition, peer support is integrated by encouraging shared experiences and mutual understanding among participants. The core TIC principles of Collaboration and Mutuality, Empowerment, Voice and Choice are also central to these interventions, as they encourage participants to take an active role in their recovery and foster autonomy. Finally, Cultural, Historical, and Gender Issues Sensitivity are also key aspects, as these interventions consider the impact of cultural and gender-based values into treatment, recognizing the diverse experiences of trauma survivors. Overall, these interventions embody the principles of TIC by fostering safety, empowerment, and inclusivity while addressing the complex needs of trauma survivors in a structured and sensitive manner. Moreover, they progress at the individual’s pace to prevent re-traumatization.
Mental Health
In the mental health context, the thematic framework has been compartmentalized into distinct categories: Depression; PTSD; Anxiety; Anger; Self-efficacy; and Substance Use.
Depression
Seven studies demonstrated the positive impact of TI programs on depressive symptomatology among PI. Namely BV (Kubiak et al., 2012, 2015); SS (Lynch et al., 2012; Tripodi et al., 2022); STAIR (Tripodi et al., 2022); Esuba (Roe-Sepowitz et al., 2012; Ward & Roe-Sepowitz, 2009); Integrity (Saxena et al., 2014). Saxena et al. (2014) found that while Integrity alone did not significantly impact depression, individuals reporting prior physical or sexual abuse who received Integrity had a significantly reduced (p < .05) likelihood of experiencing depression.
PTSD
Nine studies reported a consistent decrease in PTSD symptoms among participants who received TI programs, including BV (Kubiak et al., 2012, 2015), SS (Lynch et al., 2012; Tripodi et al., 2022; Wolff et al., 2012, 2015; Zlotnick et al., 2003, 2009), STAIR (Tripodi et al., 2022), Gender-responsive (GR; Messina et al., 2012), and M-TREM (Wolff et al., 2015).
Anxiety
Among all the identified programs, four exhibited a positive impact on anxiety symptoms in PI: BV (Kubiak et al., 2012, 2015), SS (Tripodi et al., 2022), STAIR (Tripodi et al., 2022), and Esuba (Roe-Sepowitz et al., 2012).
Anger
Only the BV (Kubiak et al., 2015) and Esuba (Roe-Sepowitz et al., 2012) programs demonstrated a reduction in anger symptoms among PI over time.
Self-Efficacy
SS (Tripodi et al., 2022; Wolff et al., 2015) and STAIR (Tripodi et al., 2022) group participants reported improvements in the self-efficacy measure.
Substance Use
Six studies found that TI interventions reduced posttreatment substance use symptoms and number of substances used, including Integrity (Messina et al., 2010; Saxena et al., 2014), GR (Messina et al., 2012), and SS (Wolff et al., 2012; Zlotnick et al., 2003, 2009). Saxena et al. (2014) reported that while Integrity alone did not produce a notable main effect on substance use, individuals with a history of physical or sexual abuse who received Integrity were significantly (p < .05) less likely to use substances. Furthermore, although SS (Wolff et al., 2012) did not have a significant positive impact on substance use, most participants reported the intervention as helpful.
Note that to ensure reliable assessments, substance-related measures (e.g., The Addiction Severity Index) were administered at intake, focusing on the 30 days prior to incarceration to capture substance use outside a controlled environment. During follow-up, substance use was evaluated for the prior 30 days (i.e., the 30 days before each follow-up), complemented by urine and blood alcohol tests and, in some cases, administrative data from systems like the Offender Substance Abuse Tracking System.
Recidivism
Three studies evaluated the impact of TI programs on recidivism, using data from administrative systems, participant self-reports, and prison census records. Messina et al. (2010) and Zlotnick et al. (2009) reported reductions in return-to-prison rates at 12- and 6-month postrelease follow-ups, respectively, whereas Zlotnick et al. (2003) found high recidivism rates at a 3-month postrelease follow-up.
Discussion
This SLR aimed to examine the mental health outcomes resulting from the implementation of TI intervention programs for PI. These interventions, strategically focused on reducing recidivism and improving community safety, prove to be more effective than conventional incarceration methods (McLachlan, 2022). This effectiveness is rooted in recognizing that a substantial proportion of PI have undergone, and continue to grapple with, severe adversity, trauma, and social exclusion, which are closely linked to their offending behavior (McLachlan, 2022). Instead of emphasizing offense culpability and punitive measures (Levenson & Willis, 2019), TI programs integrate TIC practices that recognize and respond to the widespread impact of trauma (SAMHSA, 2014). These practices have proven effective in prisons as behavior management strategies and as tools for ensuring correctional staff and client safety (Jones, 2017). Consequently, correctional organizations should adopt a TI approach to engender a transformative shift in institutional culture, thereby aligning with PI’s needs (Miller & Najavits, 2012).
Consistent with existing SLR on psychological therapies in prison settings (e.g., King, 2017; Malik et al., 2023), TI intervention programs appear to positively impact PI’s mental health. This finding is crucial and promising, as it reinforces the necessity of trauma-sensitive interventions within correctional environments. Another factor contributing to the observed positive impact of these interventions is the alignment of TI programs with the Risk-Need-Responsivity (R-N-R) model, which is the most used framework to guide correctional interventions (Andrews & Bonta, 2010).
Given that childhood trauma represents a critical static risk factor, addressing its enduring effects presents a key opportunity for intervention (Bates-Maves & O’Sullivan, 2017). As TI approaches are designed to account for the biological, psychological, social, and neurological impacts of child maltreatment (Bates-Maves & O’Sullivan, 2017), their implementation in correctional settings is particularly valuable.
In addition, it was observed that the most widely used program was Seeking Safety, which also demonstrated a positive impact on all parameters, followed by Beyond Violence. This might have occurred due to SS being a manualized, cognitive-behavioral intervention that addresses trauma consequences and its links to substance use (Lynch et al., 2012) while BV has a specific focus on dealing with domestic violence-related issues (Kubiak et al., 2015). Also, SS is relatively low cost and, as it is psychoeducational, does not necessarily require extensive training to implement (Miller & Najavits, 2012).
A noteworthy finding is that some control groups also exhibited mental health improvements, albeit to a lesser extent than treatment groups. One possible explanation is that in most studies, TAU was mandatory (ensuring that all participants received some form of intervention), whereas participation in TI programs was voluntary, potentially leading to differences in motivation or engagement. In addition, control groups may have benefited from general elements of the prison environment, such as routine, structure, or access to rehabilitative services. Some control groups may have also been indirectly exposed to TIC principles through staff training or facility-wide practices, contributing to unintended benefits. However, these improvements in control groups do not diminish the positive effects found in the treatment groups, as TI interventions may provide targeted benefits beyond those observed in standard correctional programs.
Regarding recidivism rates, experiencing trauma often is linked to higher mental health problems and substance use disorders, both of which contribute to increased recidivism rates (Tripodi et al., 2019). Among the limited studies that assessed recidivism, two (Messina et al., 2010; Zlotnick et al., 2009) demonstrated the efficacy of TI programs in reducing postrelease reoffending rates. These results can be explained as TI programs provide PI with the support and tools (e.g., coping mechanisms, communication skills and cognitive-behavioral restructuring) they need to address the underlying issues that may have contributed to their involvement in the criminal justice system and that are essential to reducing criminal behavior (Adams et al., 2017). It is noteworthy that, although Zlotnick et al. (2003) found a high recidivism rate at a 3-month follow-up, the authors did not provide an explanation for this outcome.
Interestingly, TI interventions have demonstrated positive effects across various populations and contexts, including residential juvenile facilities (Olafson et al., 2018), women with dual diagnoses of substance abuse and mental health disorders in residential treatment (Covington et al., 2008), educators (Kim et al., 2021), and male veterans (Boden et al., 2012). These findings align with the results of the present review, underscoring the broad applicability of TI programs in addressing trauma-related mental health challenges.
Finally, it should be noted that the most empirically supported interventions for PI largely align with the R-N-R principles with a cognitive-behavioral framework (Skeem et al., 2009). Yoon et al. (2017) found moderate-quality evidence supporting the efficacy of cognitive-behavioral therapy, particularly for anxiety and depression. However, their meta-analysis of seven studies on TI interventions in correctional settings did not achieve statistical significance. In contrast, Malik et al. (2023) reported a small but significant effect size for TI interventions in reducing PTSD symptoms across 16 trials compared with prison control groups. Both studies concluded that while some individual trials found significant effects of TI interventions in reducing symptoms compared with control groups (Yoon et al., 2017) and group interventions (Malik et al., 2023), these findings were not consistently supported by the broader body of research, indicating the need for further empirical validation.
Limitations
The quality assessment of the included studies revealed a predominance of moderate-quality research, a trend potentially influenced by the inherent challenges of conducting research in prison settings, including ethical and logistical considerations (Wolff et al., 2015). Consequently, the findings of this SLR should be interpreted with caution. Furthermore, as all the studies included were conducted in the United States, the potential for limited generalizability arises due to specific population characteristics, cultural context, and health policies.
Another limitation concerns gender representation and balance, as most studies exclusively focused on females who are incarcerated. This gender disparity may influence the overall findings of the review, as the experiences and mental health needs of males who are incarcerated remain underexplored in TI research. Although the high prevalence of trauma exposure among females who are incarcerated has led to a research focus on this group (Altintas & Bilici, 2018; Baranyi et al., 2018), it is crucial to recognize that males who are incarcerated also experience significant trauma before incarceration (Morrison et al., 2019), yet their specific needs within TI frameworks remain largely unexamined.
Finally, another key limitation is the lack of long-term follow-up assessments in many studies. Although some studies included follow-up measures, findings varied considerably, making it difficult to determine the sustained impact of TI programs on PI’s mental health and recidivism rates.
Implications for Practice and Policy
The results of this review highlight the importance of integrating TI programs into prisons as a policy and practice imperative. Policies should mandate TI training for prison staff and implement systematic trauma assessments during admissions to identify early trauma histories and facilitate timely, targeted interventions. Furthermore, fostering stronger partnerships between health care providers and prison systems is essential to ensure the successful implementation and sustainability of TI programs.
In practice, correctional facilities should adopt structured, evidence-based interventions like Seeking Safety, which are cost-effective and easily implementable. Training staff to recognize and address trauma is also vital for creating a supportive and rehabilitative environment. Gender-sensitive programming is equally critical to address unique challenges faced by PI, such as complex trauma and systemic inequities. Furthermore, expanding TIC principles to community-based reentry programs ensures continuity of support postrelease, sustaining the positive mental health outcomes achieved during incarceration and reducing recidivism.
Overall, these findings underscore the transformative potential of TIC in fostering a rehabilitative prison culture, promoting public safety, and improving outcomes for individuals and communities. This signals a promising avenue for developing effective, inclusive, and sustainable interventions.
Implications for Future Research
The findings from this SLR highlight opportunities to address the root causes of criminal behavior, improve mental health outcomes, and reduce recidivism in correctional systems. Unlike prior reviews that have solely focused on females who are incarcerated, our SLR included both males and females, emphasizing the need to consider gender differences in trauma-sensitive care. While existing literature has appropriately prioritized females who are incarcerated due to their high rates of trauma exposure, it is important to acknowledge that males in correctional settings also experience significant trauma. However, they remain an understudied population in this context, limiting the ability to develop tailored interventions. This gap underscores the need for further research to explore the specific traumatic experiences of males who are incarcerated and assess potential differences in their responses to TI programs. Expanding this area of research will help refine trauma-sensitive interventions in correctional settings, ensuring they are more comprehensive and better tailored to the experiences and needs of both genders.
Furthermore, all the studies included in this review were conducted in the United States, raising concerns about the findings’ generalizability to other cultural contexts. Future research should examine and adapt TI programs in diverse cultural settings, such as European correctional systems, to evaluate their applicability across different populations. Tailoring interventions to local cultural norms and values is crucial for enhancing their relevance and effectiveness. In addition, with only three studies in this review examining the relationship between TI interventions and recidivism-yielding mixed results, further research is needed to determine the long-term effectiveness of these programs in reducing reoffending.
To measure the sustainability of TI programs on PI’s mental health, rigorous studies with extended follow-up periods are needed. Moreover, although this SLR included only quantitative studies (as the qualitative studies identified did not align with the predefined objectives), qualitative research is vital for understanding participants’ lived experiences and perspectives. Future research should integrate qualitative and quantitative data to provide a more comprehensive understanding of the effectiveness, acceptability, and contextual factors influencing TI programs.
While this SLR analyzed the interventions through the lens of TIC principles, the limited details in the included studies on how these principles were operationalized or maintained highlight the need for more thorough reporting. Research should focus on the practical implementation and sustainability of TIC principles within correctional environments, where safety, trust, and empowerment are often challenging to maintain.
Finally, prisons are inherently stressful and potentially re-traumatizing environments, which can undermine the effectiveness of TI interventions. Although all interventions included in this SLR were conducted in prison settings, the studies provided limited insights into how these programs addressed the unique structural constraints of incarceration, such as exposure to violence, lack of autonomy, and restricted access to mental health care. Future research should explore strategies to enhance the adaptability of TI interventions within correctional settings, ensuring they adequately mitigate the risks of ongoing trauma exposure. Moreover, long-term research is needed to assess the enduring impacts of TIC, including follow-up evaluations beyond the immediate postrelease period to account for ongoing exposure to environmental stressors.
In conclusion, while TI interventions show significant potential, refining their design and implementation to align with the realities of prison environments will be crucial for enhancing their therapeutic effectiveness for PI.
Footnotes
Authors’ Note:
The authors declare no conflicts of interest. The study was conducted according to APA ethical standards. This work was supported by national funding from the Portuguese Foundation for Science and Technology (UIDB/00050/2020).