
Abstract
The article explored overcrowding in Ghana prisons and sought to understand its impact on the health and well-being of persons in custody and prison officers. Qualitative data from 38 participants who were serving terms or working in three prison facilities in Ghana revealed three themes, including (a) fear over the spread of communicable diseases, (b) limited access to basic resources, and (c) psychological and emotional burden, attributing them to overcrowding in the prisons. We discussed the findings from human rights and prison and public security perspectives and concluded that addressing overcrowding in prisons would ensure a healthy prison environment, which may have implications for the well-being and human rights of persons in custody, as well as public safety and the health of prison officers and the community. To achieve a healthy prison, policies should target prison depopulation and commitment from stakeholders to implement local and international prison rules and conventions.
The world has witnessed a rapid surge in the prison population over the past three decades. Currently, there are over 11 million people incarcerated globally, which is an increase of 8% since 2010 (Penal Reform International & Thailand Institute of Justice, 2021). This era in penal history has been termed the era of “mass incarceration” (Mears & Cochran, 2015, p. 2), as most countries have resorted to incarceration as the primary mechanism for fighting crime (Horowitz & Uggen, 2019). In jurisdictions such as the United States of America and most parts of Europe, the focus on incarceration has resulted in the expansion of prison facilities and construction (Guetzkow & Schoon, 2015), as well as the introduction and reform of policies (Daems, 2008) aimed at addressing overcrowding in prisons.
In Ghana, the prison population has increased from 9,507 (2000) to 15,228 in 2023 (Ghana Prisons Service [GPS], 2023). The exponential increase has seen little to no improvement in prison depopulation policies. For example, to date, Ghana does not have a community service policy, as the penology system continues to rely on incarceration and fines. Baffour (2021) suggested that many persons charged by the court to pay a fine for their offenses end up serving a term of imprisonment due to their inability to pay. Further, a few prison facilities inherited from the colonial administration are not in use because they are not fit for purpose (Keta prison was destroyed by the waves in 1980) or converted to tourist sites (James Fort, Usher Fort, and Anomabo prisons; Baffour, 2020). With the Ankaful Maximum-Security prison still under construction and the recently constructed Ejura camp prison, the country still has a deficit in prison facilities, which has implications for overcrowding.
The United Nations Office on Drugs and Crime (2013) defines overcrowding as the “situation where the number of prisoners exceeds the official prison capacity” (p.8). The United States of America Bureau of Justice Statistics (2015) advised prisons to operate below capacity to prevent overcrowding and its consequences. In Ghana, the official capacity for the existing facilities is 10,265 (GPS, 2023). Currently, the Ghana prison system accommodates 15,228 individuals, including remand prisoners and pretrial detainees (GPS, 2023), indicating an excess of 4,963 individuals. The extant literature has reported poor conditions and limited access to basic needs such as health and food in Ghana prisons (Baffoe-Bonnie et al., 2019; Baffour et al., 2022a).
Recently, overcrowding in Ghana prisons has gained attention in public discourse, featuring on national media platforms, partly due to the COVID-19 pandemic. The Director General of Ghana Prisons lamented the deplorable state of the country’s prisons, which he attributed the cause to overcrowding, as reported by Agbenorsi (2021) on the “Graphic” website. A similar report was captured by the Ghana News Agency (2021), which called for pragmatic measures to address overcrowding. Despite the Government of Ghana granting amnesty to 1,555 individuals in 2020 as one of the measures to improve the health of persons in custody and prevent the outbreak of the COVID-19 pandemic in the country’s prisons, conditions continue to remain poor (Arusha Declaration on Good Prison Practice, 1999).
Overcrowding has become a chronic problem in Ghana prisons. In 2012, Amnesty International reported that prisons in Ghana did not meet international standards due to overcrowding, which has resulted in deplorable conditions among persons in custody. A recent report by U. S. Department of State (2022) suggested that overcrowding continues to pose problems to persons in custody’s fundamental human rights. In 2016, a group of lawyers sued the Ghana Attorney General for degrading and inhumane treatment of persons in custody. Center to the issues raised in court was the failure of the prison authorities to separate toilet facilities from the persons in custody’s bedrooms—they described this condition as “cruel” and “inconsistent” with the country’s constitution, as reported in “Attorney-General Sued Over Inhumane Conditions at Prisons” (2016) on “myjoyonline” website.
The study focuses on understanding the consequences of overcrowding on people who live and work in three prison facilities in the West African Country of Ghana. First, we review relevant literature on the effects of overcrowding on the well-being and fundamental human rights of prison occupants. Second, we present the concept of human rights as the lens that informs the study. We further outline the qualitative method that guided data gathering and presentation. The results and discussion contribute to the limited knowledge of prison research in Ghana and other parts of the continent and present a compelling perspective for policy and research implications. Significantly, while overcrowding is a global prison crisis, we believe the situation is worse in resource constraint countries, particularly areas where minimum resources are concentrated in education, health, and infrastructure in the mainstream community. A study like ours, designed to give a voice to people living with the consequences of overcrowding, has the potential to start and sustain a conversation on the ethical treatment of people in custody.
Prison Overcrowding, Persons in Custody’s Well-being and Fundamental Human Rights
Over the past three decades, a concerted effort has been made by leaders in Africa through regional declarations and conventions aimed at promoting persons in custody’s fundamental human rights and well-being. The agency to improve conditions in the continent’s prisons saw the African Union and other regional bodies adopting five declarations in the space of 6 years. The Kampala Declaration on Prison Conditions in Africa (KDPCA, 1996), Kadoma Declaration on Community Service Orders in Africa (KDCSOA, 1997), Arusha Declaration on Good Prison Practice (ADGPP, 1999), Kampala Declaration on Prison Health in Africa (KDPHA, 1999), and Ouagadougou Declaration and Plan of Action on Accelerating Prisons and Penal Reforms in Africa (ODPAAPPRA, 2002) are among the treaties signed by members of the African Union to protect the fundamental human rights and well-being of persons in custody. Today, two decades after these declarations, conditions in most African prisons continue to be inhumane and uninhabitable, partly due to overcrowding caused by overreliance on colonial structures and limited resources (Motlalekgosi & Cilliers, 2020; Van Hout & Mhlanga-Gunda, 2019).
A recent study by Boakye et al. (2022) highlighted the impact of limited resources and overreliance on colonial structures on prison overcrowding in Ghana and other parts of the continent. Similarly, Baffour (2021) suggested that the original ideology behind prison establishment in the region by the colonial administration was to control and punish, which sadly continues to remain the case due to colonial hangovers and limited resources. In many African countries, most prison facilities currently in use were inherited from colonial administrators with little to no addition or upgrade, creating inconsistency with modern prison standard conditions and management. The colonial prison structures, designed to meet the purpose at the time, their current adaptation, coupled with overcrowding, may have dire consequences on the well-being and fundamental human rights of occupants.
MacDonald (2018) argued that crowded prisons limit access to resources, which curtail opportunities for proper rehabilitation programs and deny prison occupants quality of life. In one South African study, the participants lamented how prison overcrowding affected their social, physical, and psychological well-being, leading to negative outcomes in rehabilitation programs (Nkosi & Maweni, 2020). Previous studies conducted in Ghana have reported the impact of overcrowding on poor rehabilitation regimes and subsequent recidivism (Baffour, 2016, 2020, 2021; Dako-Gyeke & Baffour, 2016). While reporting on the correlation between prison climate and recidivism in Germany, Woessner and Schwedler (2014) cautioned about the impact of an unsupportive prison environment on treatment programs and recidivism.
In addition, congestion has been tagged as a major cause of infectious diseases in the prison environment. For example, a study conducted in Taiwan highlighted scabies as a common disease among persons in custody (Chen et al., 2019). Similarly, a mixed-method study in the United States suggested the vulnerability of influenza outbreaks among persons in Custody (Khorasani et al., 2022). In their analysis of the linkage between incarceration and health, Massoglia and Remster (2019) highlighted diseases ranging from obesity to hypertension to health diseases and indicated a reduction in overcrowding could mitigate the rate of these diseases among persons in custody.
Other studies have documented the impact of overcrowding on persons in custody’s fundamental human rights. For example, A Romanian-based study by Chirita (2019) suggested that a congested prison environment threatens persons in custody’s human rights to health and dignity. Another study conducted in Zambia (Topp et al., 2017) argued that poor prison conditions “. . . represent a breach of the rights of prisoners themselves as well as an ongoing threat to the health and well-being of the communities into which prisoners are eventually released” (p. 858). One study conducted in Uganda suggested that prisons in the country have failed to comply with regional and international human rights standards (Martin, 2014). The danger posed by overcrowding in prisons has resulted in lawsuits against various states in most parts of Europe, North America, Africa, and Australia (see Guetzkow & Schoon, 2015; le Roux-Kemp, 2013). This suggests that the adverse consequences of overcrowding have been acknowledged, and democratic procedures are adopted to address it.
In addition, given the vulnerability of persons in custody to diseases, a prison condition like those in Ghana and other parts of the Global South, characterized by overcrowding and harsh treatment may increase the likelihood of health problems among occupants. One study conducted in the Southern African countries of Malawi, South Africa, and Zimbabwe highlighted the risk of communicable disease transmission (Van Hout, 2023). Motlalekgosi and Cilliers (2020) explained that the more crowded a correctional center, the more the maintenance of security curtails the quality of life. Movement is severely restricted, access to recreational and learning facilities decreases, invasions of privacy increase, and inmates spend a greater proportion of their time in the cells (p. 31).
Indeed, the challenges associated with overcrowding are grievous, physically and emotionally draining, particularly for persons in custody, and the associated human rights violation and physical and mental health are reported in the literature (Baffour et al., 2022a; Spencer, 2012; Topp et al., 2017).
Prison overcrowding puts pressure on limited resources, compromises the quality of services delivered in a prison facility (Baffour, 2021; Guetzkow & Schoon, 2015), and increases the risk of violence and unrest in prisons (Nkosi & Maweni, 2020; Spencer, 2012). These consequences can lead to disregard for fundamental human rights, health challenges, and reduced safety within institutions. In most prisons in Africa, persons in custody experience poor conditions. For example, Topp et al. (2016) described deplorable sleeping conditions and unbearable congestion threatening occupants’ health and human rights.
Even though overcrowding continues to be one of the main problems confronting prisons in Africa (Baffour, 2021; Martin, 2014; Topp et al., 2016), research on its impact on fundamental human rights and health is limited. For example, in Ghana, researchers have focused on the impact of prison conditions and administration on recidivism and rehabilitation (Baffour, 2021; Boakye et al., 2022; Dako-Gyeke & Baffour, 2016), life-sentence and mental health (Baffour et al., 2022b), persons in custody’s access to health care (Adomah-Afari et al., 2021), and prison officers’ understanding and knowledge about international guidelines that protect the rights of persons in custody (Golo, 2022). We acknowledge the contributions of previous researchers but also prioritize the need for an extended body of knowledge in the area of overcrowding, particularly for a continent where prison congestion poses unique questions while an empirical understanding of its consequences is limited. To date, the question of how overcrowding influences the health and human rights of prison occupants remains unanswered, hence the focus of the current study (using data from Ghana).
Overcrowding and Inhuman Treatment Through Human Rights Lens
For this study, we conceptualize fundamental human rights as the person in custody’s inalienable right to humane treatment that encompasses free from torture and access to humane living conditions that meet the environmental determinants of health requirements such as ventilation, hygiene, sanitation, protection from diseases and access to health care and adequate space and standard amenities. Over the past seven decades, local and international organizations recognizing the vulnerability of persons in custody to degrading treatments have codified rules to protect their human rights. For example, the universality of protection from degrading punishment, cruelty, and torture of all persons, including those in detention, runs through human rights laws, conventions, covenants, and treaties (see African Charter on Human and People’s Rights [Article 5, African Union, 1981], International Covenant on Civil and Political Rights (Article 10, United Nations General Assembly [UNGA), 1966)), The Nelson Mandela Rule [rule 1, UNGA, 2016], and the 1992 Constitution of Ghana [chapter 5, article 15, Government of Ghana, 1993].
Considering the report in the literature about the deplorable state of prisons in most parts of the continent (Martin, 2014; Van Hout, 2023), approaching the study through human rights lens helps us put prison overcrowding from the perspective of a forgotten human rights issue, attracting little to no attention from researchers and policymakers alike, particularly in the West African region, stemming from public disinterest in prison welfare (Baffour, 2021). As a result, unlike the mainstream community, a blatant breach of the fundamental human rights of persons in custody escapes public discourse and political scrutiny, making human rights violations in the carceral system perceived as “business as usual.” Sadly, in the African region, particularly Ghana, overcrowding presents unfavorable conditions requiring uncomfortable adjustment, particularly for persons in custody (Baffour, 2021; Topp et al., 2016). In addition to the legal deprivation of liberty (Clemmer, 1940; Sykes, 1958), administratively imposed deprivations (as a result of overcrowding) such as inadequate floor space, exercise facilities, water, nutritious food, health care, and hygiene facilities, submit persons in custody to systemic punishment that may constitute human rights violation.
Approaching the study from the human rights lens presents two benefits. First, it helps to put the results into perspective, for example, how prison overcrowding may influence prison administrators’ decisions on sleeping arrangements, food, and water rationing, and the negative impact on persons in custody’s right to health, sanitation, and humane treatment. And second, it helps us expand the conversation of human rights to a forgotten population, such as persons in custody, by suggesting cultural and resource-appropriate policy implications aimed at promoting ethical and moral prison management and administration in a region where the disregard for human rights attracted scrutiny.
Method
We employed a qualitative design to conduct in-depth interviews with 15 correctional officers and 23 persons in custody to understand the impact of prison overcrowding. The study participants were selected from three prison facilities in Ghana (Ankaful Maximum-security, Nsawam Medium security, and Kumasi Central prisons). The Nsawam Medium-Security prison is the most populous in Ghana, currently accommodating almost 4000 persons (over 5 times its original capacity of an estimated 700). The Kumasi Central Prison is the second most populous prison, accommodating almost 2000 individuals instead of estimated 400 people. The Ankaful Maximum-Security prison is still under construction, which has curtailed its capacity to accommodate the 2000 individuals it ought to and currently house almost 1400 persons. The prison facilities selected are the highest in terms of security and population in the country and use dormitory accommodation style, where people are clustered in a room. Recent studies in medium and minimum-security prisons reported overcrowding and suggested it had partly resulted in harsh conditions and the intermingling of people with diverse crime histories and security needs (Baffour, 2021). To this end, the choice to include these prison facilities in a study that sought to explore the impact of overcrowding on persons in custody’s health and human rights is considered appropriate.
The qualitative data were purposively collected from two participant groups (persons in custody and Correctional Officers) after the study was assigned the ethical approval number (H7124). The participants voluntarily nominated themselves by putting their names down on a piece of paper and depositing it in a box placed in front of the general offices or welfare offices in the participating facilities after explaining the purpose and inclusion criteria of the study to them. Only people serving their second or more terms of imprisonment and at least 1 month into their current prison term qualified for the study. Originally, we sought to understand the contributing factors to recidivism. However, during the analysis of the first data set (n = 30), we became aware of the participants’ concerns about overcrowding, prison conditions, and mental and physical health, prompting a second set of interviews with the same individuals and additional eight persons in custody to throw light on the impact of overcrowding. For correctional officers, at least 5 years of working experience was a requirement for participation—this guided the recruitment of staff members familiar with the prison environment and could share rich experiences about overcrowding. Further, the prison community is a space shared by persons in custody and prison staff, and therefore, experiences such as overcrowding, if present, affect all parties, hence the need to collect data from these participant groups.
The participants had 5 days to express interest in the study. More than 23 persons in custody expressed interest in the individual prisons, but applying the inclusion criteria, only 16, 12, and 9 of them (37) qualified from the medium-security, Maximum-security, and minimum-security prisons, respectively. Nineteen correctional officers expressed interest in total who met the inclusion criteria. We purposively ranked the participants in order of their years of experience (correctional officers) and the number of incarceration (persons in custody), as we believed they had the rich experience to contribute to the study. The purpose of the study was explained to the potential participants before the expression of interest, and before they signed the consent form, we reiterated it. All the participants were rewarded for their participation with bath and laundry soap, toothpaste, and brush after the interviews in the individual prisons.
The prison administration assigned a room (inside the prison) for the interviews with the persons in custody. A prison officer was assigned to supervise the interviews, expressing concerns for safety and breach of security protocols. Prison officers were strict in the early days of data collection, but this eased when they became familiar with the research team and more aware of the purpose of the study. The initial 15 interviews with the persons in custody were handwritten, but the second phase was audio-recorded after they had consented. The interviews with the correctional officers were conducted outside the prisons and audio recorded with their consent.
We gathered rich data by following the principles of data saturation (Trotter, 2012), where we explored ideas and concepts until subsequent interviews with other participants who had lived with the problem under study produced no new ideas and concepts (Hennink et al., 2017; Sounders et al., 2018). To this end, we stopped collecting data after interviewing 23 persons in custody and 15 Correctional Officers after realizing that later interviews with individuals who had lived with the problem were a repetition of already collected information. The sample size (n = 38) is justifiable because previous qualitative prison studies in Ghana interviewed 21 (Baffour, 2021), 24 (Golo, 2022), 27 (Kankam & Baffour, 2023), and 20 (Baffour et al., 2021) participants. The participants’ characteristics, including pseudonyms, are shown in Table 1.
Participants Characteristics
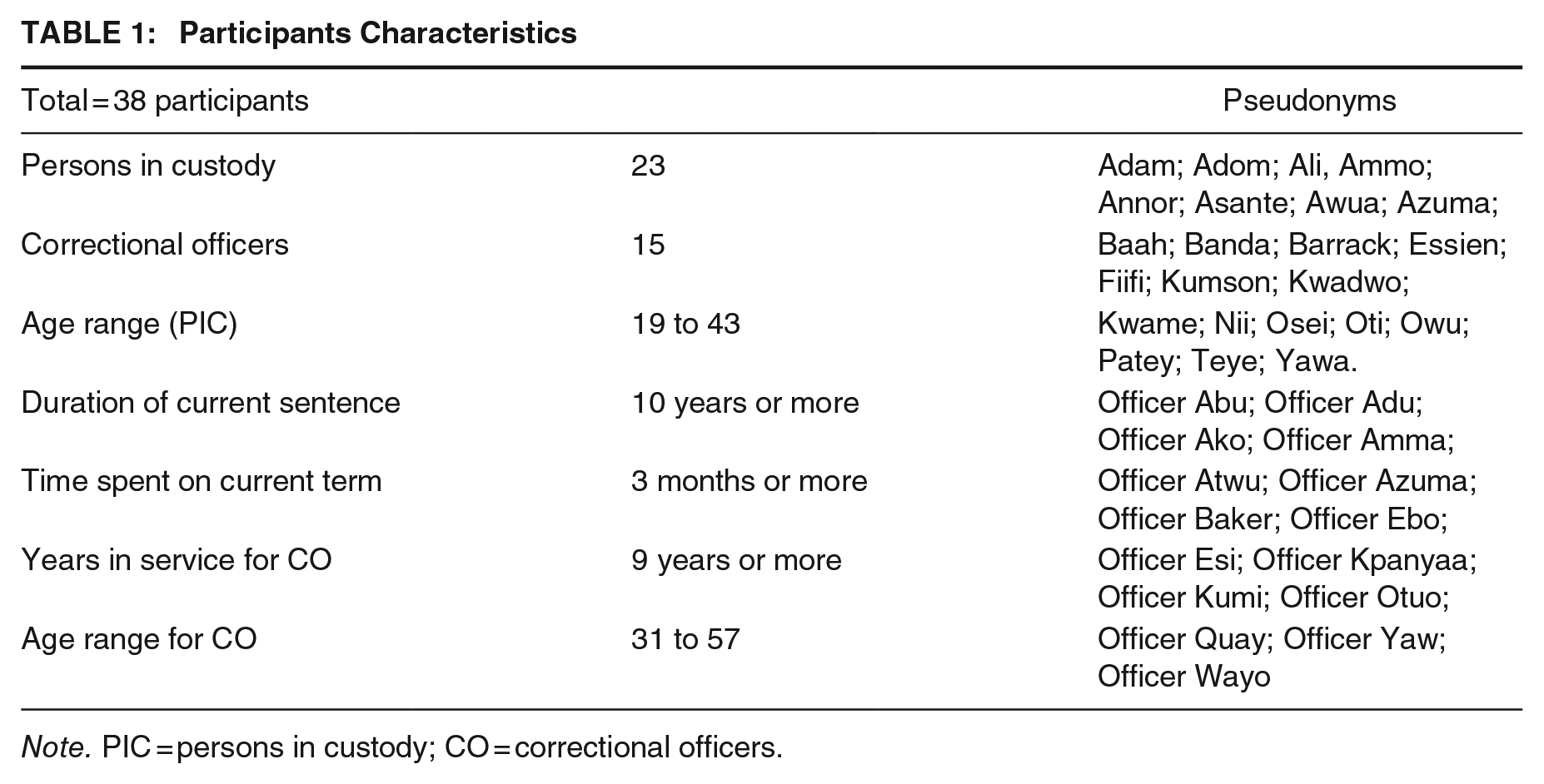
Note. PIC = persons in custody; CO = correctional officers.
Semi-structured interviews were conducted with the participants to explore overcrowding in the selected prisons, if any, and understand its impacts on their well-being and fundamental human rights. We asked the correctional officers to describe the extent of overcrowding in the prisons and the impact on prison conditions (e.g., in your view, how is overcrowding affecting the living conditions in this prison? Can you shed light on the fairness/unfairness of the living conditions in this prison?). We also explored whether there have been outbreaks and insurgences in the selected prisons and the impact of overcrowding in these events (e.g., can you remember any disease outbreak in this prison, and to what extent congestion might have contributed?). We asked the persons in custody about the issue of overcrowding and how it affected their health and fundamental human rights (e.g., what is the current estimated number of people in your dormitory, and can you describe the situation of sharing a space with this number of people? Can you shed light on any grievances about your experience in this prison?). Other questions probed the participants’ well-being, safety, food, and prison conditions (e.g., if you have ever fallen sick in this prison, can you explain how it happened?).
The interviews lasted between 1 hr to 2 hr 15 min per participant. The first interview phase lasted for 6 months, and we completed the second phase in 2 months. The need for the second phase of interviews arose when it became necessary to explore further and clarify some issues that emerged in the first interviews during the initial stages of data analysis. For example, the issue of persons in custody’s physical and mental health and human rights emerged, warranting the need to return to the field for in-depth information from the participants. The interviews with the correctional officers were conducted in the English language and with the persons in custody in Asante Twi.
The second visit to the selected prisons facilitated participant validation of the data collected in the first phase and an opportunity to collect additional data toward understanding the impact of overcrowding on health and human rights. In addition, we ensured trustworthiness through participant triangulation (Denzin & Lincoln, 2008) by collecting data from two sample groups (persons in custody and correctional officers), which helped the study to analyze divergent and convergent views, which enhanced understanding of the phenomenon understudy and suggested strategies for improvement. Further, we were reflexive throughout the research process through consciousness about our biases and presuppositions throughout the research process, preventing them from influencing the outcome of the study.
Data Analysis
The 2016 version of Microsoft Word was used to transcribe data for the study. Interviews conducted in the Asante Twi language were translated and transcribed into the English language. Further, we performed a thematic analysis of the field data using the Nvivo 12 qualitative software. The study followed the six steps of thematic data analysis (Braun & Clarke, 2006; Clarke & Braun, 2017), with the first author solely performing the second and third steps. Through transcription and reading the data, we familiarized ourselves with the data set. Initial codes were generated in the second stage (e.g., congestion, illness, tuberculosis, overcrowding as a major problem, living in deplorable conditions, N1N1 flu, skin rashes, fight, scarce resources, riot, limited supply, food, water, afraid, thinking, etc.). In the third stage, the researcher searched themes by identifying patterns and similarities in the initial codes. For example, initial codes such as skin rashes, tuberculosis, NINI flu, etc., were grouped under communicable diseases and physical illness because of their similarities. Initial themes, such as overcrowding, living in deplorable conditions, and mental health and psychological issues were also highlighted. In step four, we reviewed the themes and checked consistency with the data set and codes. During this stage, we deleted initial themes such as mental health because we felt the study did not set out to diagnose mental health conditions. However, we retained psychological issues because they were consistent with the data set and prevented us from labeling the participants’ experiences. Names were assigned to the themes in stage 5 (see Figure 1) before a detailed write-up, as presented in the section below.
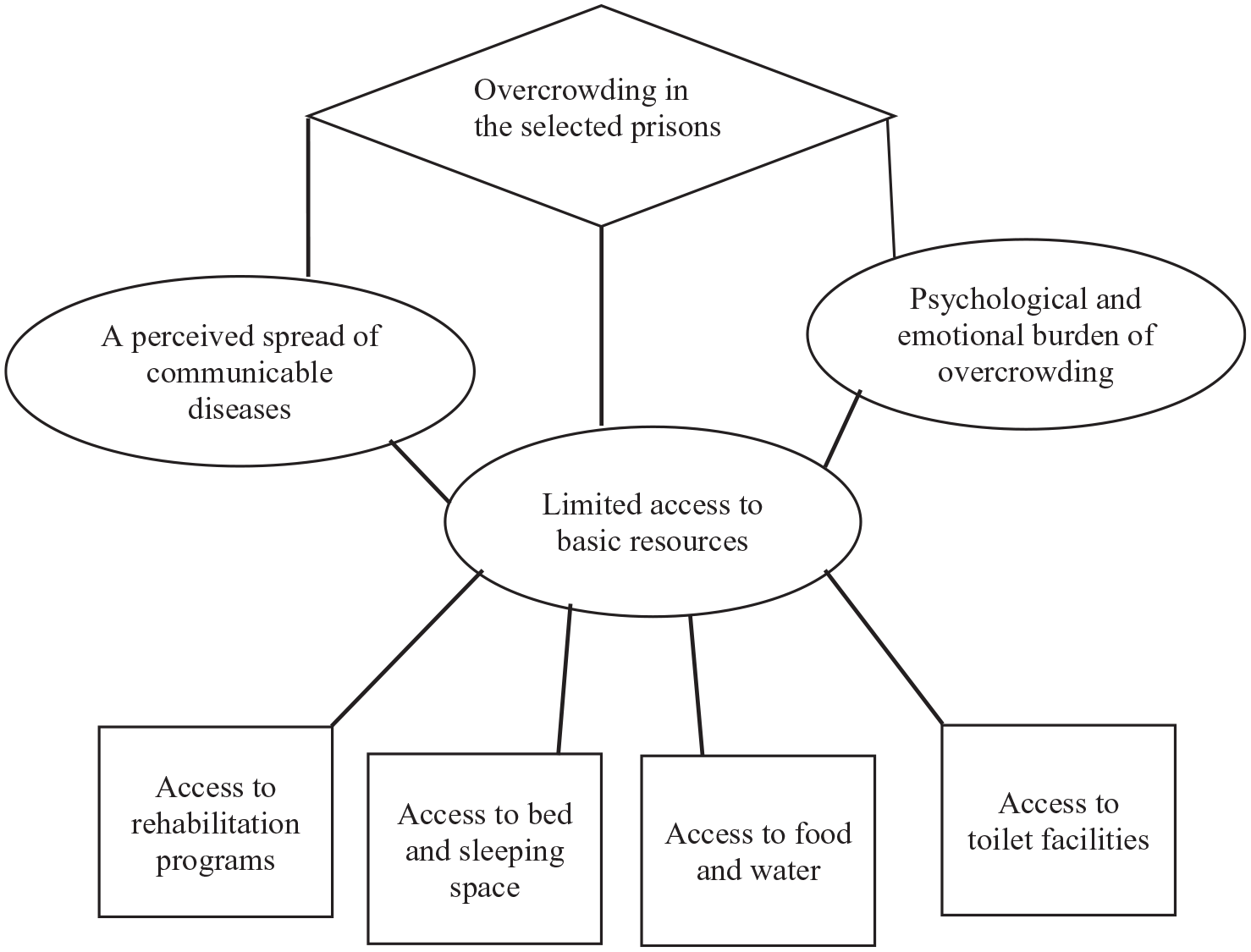
Thematic Map
Results
The phrase “overcrowding is a major problem” appeared in All 38 interviews. Despite the admission by all participants, the persons in custody perceived the situation as uncontrollable due to no efforts by the prison administration to address it. A statement running through all 23 persons in custody interview was “they admit new people every Friday, which shows they do not see the prison to be overcrowded.” However, the correctional officers suggested measures were in place to address the conditions, with some citing examples of new structures under construction to ease congestion. All participant groups expressed concerns about disease outbreaks, with the correctional officers sharing their fears about the possible consequences on their families and communities. The participant groups highlighted the deplorable effects of overcrowding on living and working conditions and made expressions suggesting perceived fundamental human rights violations. Our analysis produced one overarching theme: overcrowding in the selected prisons, and three subthemes (access to scarce resources, the perceived spread of communicable diseases, and the psychological and emotional burden of overcrowding).
In this study, the participants perceived overcrowding as the primary course of poor prison conditions. The persons in custody, particularly Yawa, described the living conditions in the prisons when he said: “In my room, we are more than 100 . . . every Friday they admit new people, once they are sentenced to the prison, they should get a place to sleep.” The population of persons in custody was increasing weekly, with new admissions compressed in the already congested facility. A statement by a correctional officer at the Minimum-security Prison described the magnitude of the problem: The Kumasi prison is too congested, and effort is not made to reduce the population . . . now, I will describe the situation as above the threshold of describing it. The prison has a current population of almost 2000 inmates, whilst it is a facility that should accommodate not more than 400 inmates (Officer Baker).
The participants’ responses suggest that the minimum-security prison was over 200% overpopulated. Similar to the minimum-security prison, persons in custody at the medium-security prison reported it was accommodating more than its original capacity: “I am glad you got the chance to visit where we sleep—it is clear that the cells are taking far more than it is supposed to—for me even if we were 600 in the prison it will still be too much” (Patey). An officer at the medium-security prison confirms Patey’s claim, he said: Our prisons are very crowded; the facilities we have here were constructed to accommodate at most 700 inmates, as I speak, the total lock up is over 3500. The cells are not supposed to accommodate more than 10 people but as it stands, because of overcrowding, we are forced to keep 40 to 50 inmates or more in a cell (Officer Wayo).
The responses above demonstrate an intense pressure on the limited prison facilities in the country, which has implications for prison occupants’ well-being and humane treatment. Twenty-one out of the 23 persons in custody expressed concerns about the deplorable prison conditions, describing it using words such as “inhuman, poor, bad, and heartless.” Osei, a person in custody revealed that “the conditions in this prison are not good for humans to live in.” Osei further perceived that some animal species known for surviving in a crowded and deplorable state “may struggle to survive in this condition.” Officer Kpanyaa shared this sentiment with Osei, he said: The situation here is not one we are proud of—it puts all of us and our families in danger. Because of their numbers, it is difficult to practice basic hygiene and observe security protocols. In my previous post, there was a riot, and it is not an experience I will wish for anyone . . . our health, security, and lives are constantly threatened.
While the officers expressed concerns about their security due to the fear that unbearable conditions could trigger prison unrest, the persons in custody were particularly concerned about the impact of overcrowding on their physical and psychological well-being. Issues garnered interest in the interviews range from the participants’ concern about potential riots and infractions in the prisons triggered by persons in custody’s struggle over scarce resources to the spread of communicable diseases and the psychological and emotional burden of living in a congested environment. Three subthemes emerged from the overcrowding conditions in the selected prisons (limited access to basic resources, the perceived spread of communicable diseases, and psychological and emotional burden).
Perceived Limited Access to Basic Resources
Officer Otuo explained: The inmate population keeps increasing—we receive convicted and remand inmates every week, yet the resources in the prison stay the same. The place to sleep, bath, and do other basic things for themselves are fewer than their population and they struggle over these resources all the time.
The responses from the participants suggest the constraint and rationing of basic resources in the prisons. Ghana has a deficit in prison facilities, and the study reveals a few existing ones, even though in operation, were still under construction. A senior officer at the maximum-security prison, Officer Quay explained: The initial plan was that the maximum prison, when completed, will accommodate 2000 inmates and contribute to reducing the population in other prisons, but in its current state, it cannot accommodate this number because phase two is incomplete, and we cannot keep inmates in a facility which lacks basic amenities.
Generally, the experiences shared by the study participants suggest persons in custody’s demands for basic resources outweigh the supply. Among the resources perceived to be limited in supply were rehabilitation programs, sleeping space, food and water, and toilet facilities. Four additional subthemes emerged from the participants’ views on scarce resources (access to rehabilitation programs, access to sleeping space, access to food and water, and access to toilet facilities).
Access to rehabilitation programs
Officer Esi was concerned about the limited access to rehabilitation services, when she said, “we are admitting these young guys here and under normal circumstances should be equipping them with knowledge and skills, but their numbers do not allow—a few of them get the chance to be enrolled in the programs.” Osei shared his experience in support of Officer Esi’s, he said: “I have been coming to the prison since I was a teenager, but I have not gotten the opportunity to learn a trade.” Osei’s experience was the same for 20 persons in custody who participated in this study. According to the correctional officers, the rehabilitation equipment and space are limited to accommodate everyone. Officer Kumi shared this: When you go to the tailoring workshop, the good people of Ghana and some groups out of benevolence have donated tailoring machines for the inmates to train with, but we do not have space to keep them, and this has prevented us from enrolling more of the inmates.
Other prominent reasons for inadequate access to rehabilitation include limited access to rehabilitation equipment and uncompleted facilities. Officer Quay lamented the situation in the maximum-security prison. He explained: “In this prison, the second phase, which in the original plan, was supposed to house the workshops for inmates is incomplete—in its current state, it looks like it has been abandoned.” Further, the medium-security and minimum-security prisons had a few workshops, such as carpentry, kente weaving, etc., but limited training tools and staff. Officer Kpanyaa, an officer in charge of the carpentry workshop, lamented: “The carpentry shop, I can say is the biggest we have here, but where are the tools to train them—most of them are interested, but they come here one week or two and stop coming because they cannot learn without tools.” Another prison officer was concerned with the person-in-custody-staff ratio. Officer Atwu said this: Look, their numbers are way above ours—this makes it difficult to support them as we would have wanted to . . . when there is a riot in the prisons, we need reinforcement to manage the situation . . . sometimes you are the only one supervising over 700 inmates—how can you attend to everyone’s need?
Officer Atwu’s concern was partly answered by Fiifi, who indicated that “sometimes it is difficult to get the attention of the warders, but it is not their fault; our numbers are too much for them to respond to everyone.” Fiifi’s comment, to a certain extent, suggests contentment with the prison conditions and preparedness to adjust. However, inadequate rehabilitation and little to no correctional officer-person-in-custody contact have implications for successful community re-entry and recidivism.
Access to sleeping space
Apart from rehabilitation programs and equipment, sleeping space was also limited in supply. In the selected prisons, particularly minimum and medium-security prisons, overcrowding led to the situation where the persons in custody were sleeping in turns during the night. Owu says: “Sometimes you have to wait for a friend to wake up in the night before you can find a place to sleep.”
The description of the sleeping arrangements in the prisons by the participants depicts harsh and inhumane conditions. For example, Teye explained, Each cell has gotten five two-in-one beds—this means that we should be 10 in the room, as I speak, we are more than 100 in the room—no good air to breathe, and we pack ourselves before everyone can get a place to sleep in the night.
Extreme crowding in the cells, with limited beds for persons in custody to sleep on, results in life-threatening situations. Kwame tells: My first time in the prison, I thought I was going to die, I slept under the bed with other six inmates . . . I was struggling to sleep . . . my prayer that night was: God, please, do not let me die. Later, I was squatting throughout the night . . . we will sit like this (show) in a row of seven each night.
A few of the persons in custody had access to beds and mattresses, with most of them sleeping on the bare floor. “A lot of us sleep on the floor, and we have to use our mind, otherwise some may have to stay outside, which is impossible” (Asante). Awua adds: “If you see the way we sleep, it is very bad—we have 13 people sleeping under a student bed.”
Access to food and water
The participants attributed the quality of the food served in the prisons partly due to overcrowding. Officer Ako says: “I understand the feeding money is not enough, but I blame the quality of food on their number—preparing food for over 2000 people is not easy to get right all the time.” Officer Kpanyaa was in support of the comment above but added that “the inmates always complain about their food, and I sometimes share sympathy with the kitchen staff because it is not easy to share food to such a big group, us we have here.”
All 23 persons in custody indicated they could not rely on the food served in the prisons and had to devise other alternative survival means. Among the alternative means was depending on their social ties outside, for food through visitation. Yawa says: “The food served in the prisons is not enough, so you will have to depend on your family outside to visit and give you food.” It was revealed in the interviews that most of the persons in custody were not receiving visitors and had to rely on their ties within the prison. The participants had reservations about the social ties in the prisons, indicating it was a way some persons in custody used to lure others into bad companies, which had a detrimental effect on prosocial behaviors. Kumson revealed: In this prison, if you do not receive visits but have to depend on others for food, you should be ready to do what the person who gives you food wants. Is either you cook, wash and clean for them, or you learn or do what they do to get the food, which is mostly illegal.
Some of the participants commented on the water situation in the prisons. Asante said: “the pipe is not reliable—sometimes it will not flow for more than a week.” Officer Wayo’s statement supports the claim made by Asante. He said: Inmates were not sent here to be punished, but the fact the person is in prison is the punishment . . . here you are deprived of a lot of things, and you are poorly accommodated, you fight over resources; for the past weeks the pipe has not been flowing, their feeding is very bad; GHC1.80 a day.
Access to toilet facilities
Kwame, in particular, said: “Everything in the prison, including toilet facilities and food is in short supply.” The person in custody at the medium and minimum-security prisons indicated they were queuing for toilets and baths. “Almost anytime you visit the toilet you will have to be in queue, waiting for your turn to use it” (Ammo). All persons in custody indicated queuing to access the toilet always generates tensions that result from a misunderstanding over whose turn it is and some “powerful” persons in custody overlooking the queue. Nii described the place where the toilets are as “very hot,” he explained: At the backyard where the toilets are a day will not pass without a fight—that place is very hot—some of the guys, because they have been here for long, they have come to see themselves as powerful and will always wait to the last minute where they cannot control themselves and attempt to overtake everyone in the line to use the toilet . . . such acts generate misunderstandings among the inmates and could lead to an intensive fight.
Another participant, Barrack, shared his experience on a similar situation as described above, he said: During my first prison sentence, I wanted to use the toilet one morning, only to meet a long line—I patiently joined, and when it was about five people to my turn, a guy came from nowhere and walked straight to the front, I asked why he was refusing to join the line, and he responded with an insult and rushed towards me—before I realized this had turned into a fight between the guy and his friends and me and those who were in support with my question.
Congestion in the prisons described above had implications for the health and well-being of occupants. The participants perceived the prisons as a potential breeding ground for disease outbreaks, attributing to poor hygiene, sanitation, and ventilation. The following section presents data on the participants’ responses to the perceived spread of communicable diseases.
A Perceived Spread of Communicable Diseases
Officer Yaw, a prison officer, shared his concerns: This is a prison where the number we currently have is more than three times its capacity . . . you have seen for yourself, and I hope you will agree with me that if we are not fortunate and there is an airborne disease in here, it is not only the prison that will be affected—the whole community becomes at risk.
The concerns shared by Officer Yaw had been manifested in the selected prisons, with prison officers and persons in custody referring to cases of disease outbreaks. Officer Quay said: “There have been some scary moments here and other prisons I have worked in—often time, we are hit by an outbreak.” Officer Adu recalled a time when he believed to have contracted scabies from the prisons and infested his whole family, he said: “There was a scabies outbreak in my former post which I was not lucky to escape—what was worrying is that I ended up spreading it among members in my household.” Five other prison officer participants shared a similar experience, where they believed to have carried disease outbreaks from the prison to their respective homes and communities (Officer Azuma; Officer Otuo; Officer Amma; Officer Kpanyaa; Officer Esi). For example, Officer Amma explained: We spend most part of our days interacting with and supervising the inmates . . . sometimes you spend the whole shift with the inmates. When there is an outbreak, it will take a miracle for you not to be infested . . . there has been many times where I have contracted a disease from the prison and put my husband and children at risk.
To some extent, the responses from the prison officers suggest that their interactions and contact with the persons in custody placed them at risk of contracting diseases if there is an outbreak. The persons in custody were more concerned about how overcrowding and poor prison conditions put them at risk of contracting diseases. Essien lamented: “If you come to our rooms, in the nights you will not need anybody to tell you how easy diseases can spread among us.” Ali, in particular, explained: “The cells are congested, and we spend our days and nights in it with the poor ventilation we are exposed to each other’s breath, which I see as dangerous to our health.” The persons in custody shared their experiences and perceived that they contracted some diseases in the prison: I had heard of tuberculosis and how dangerous it is, but I got to the prison, and it was so common, it is treated as a normal cough, and most of us got it from the prison . . . some have had it for months with no proper treatment, and they keep circulating in the prison (Awua).
Another participant who was diagnosed with tuberculosis and was given initial treatment by the prison medical staff before being taken to the hospital for specialized care shared his experience: “I was diagnosed with tuberculosis in the prison but was taken to the hospital to get proper treatment” (Adam).
Baah, one of the persons in custody, was diagnosed with a disease he had never heard of until he got to the prison. He said: I was feeling unwell, and after two days, I started vomiting and had a severe runny nose—things went from bad to worse very fast . . . I was taken to the nurses, and after some tests, they said I had contracted N1N1 flu. I got scared because I had never heard of it, and I thought I was going to die, given how I became weak quickly.
In addition to Baah’s account, six other persons in custody participants indicated that they were diagnosed with N1N1 influenza. All the 23 persons in custody recalled a time in their prison sentence when they perceived more than half of their colleagues, including themselves experienced symptoms such as runny nose, loss of appetite, nausea, sore throat, cough, frequent sneezing, tiredness, sweating profusely during day and night. Asante shared his experience: There was a time when almost everyone in the prison was coughing and passing phlegm at a frequent rate . . . I had severe chest pains and headaches for more than one week, and it was not just me because most of the officers were having a similar experience.
Two of the correctional officer participants shared similar experiences to Asante’s. Officer Esi, in particular, said: “In this prison, there are times where almost everyone will be coughing and having a runny nose.” Officer Kpanyaa perceived that occasionally most of the incarcerated individuals suffer from a cold (the local name for flu) and that it is common in the prison. He said: The disease that is very common in this prison and other places I have worked is cold . . . when it gets to the prison it spreads so fast . . . what I have observed is that the new entrants bring along most of these diseases, and because we do not screen them before admission and given the congested nature of the cells, they infest others, and it spreads quickly.
While the correctional officers shared their experiences about outbreaks in the prisons, the persons in custody lamented the inadequate health care and delayed response by the prison authorities to outbreaks. All 23 persons in custody expressed their concerns and used words and phrases such as “careless; we are not their priority; they don’t care; and what happens to us is not their business.” They perceived the delayed responsive culture of the prison authorities made them go through some of these outbreaks all by themselves. Banda shared this: There have been many instances where our health has been affected by common conditions such as cough, headache, and runny nose . . . this should tell anyone that something is not right and there should be an immediate response to stop the symptoms we are having from escalating to something we cannot control—many times, this has not been the case . . . we go through it by ourselves with no treatment or medication.
The data suggest inadequate resources and experiences of outbreaks have put a psychological and emotional burden on the participants. The following section explores their experiences of psychological burden in the selected prisons.
Perceived Psychological and Emotional Burden of Overcrowding
The fear of communicable diseases and struggle over scarce resources placed psychological and emotional burdens on the participants, particularly the persons in custody. The participants used expressions such as, “It makes you feel bad,” “It makes you feel like you are not wanted,” and “You feel like you have been left here to die” to describe overcrowding and its resulting consequences, such as poor prison conditions, inadequate and malnourished food, and scarce resources. The persons in custody participants expressed concerns about their well-being and the fear of “dying before their time.” Annor, in particular, said: My brother! What goes on in the prisons makes you think . . . you think about your life, and you begin to harbor fear that you might die before your term . . . most of us are not feeling well, but there is no proper medication, and when you have witnessed a colleague passing away in the prison, it puts that fear in you.
The persons in custody who participated in the study had either witnessed an outbreak or the death of a colleague in the prison, explaining why 18 of them indicated they feared for their lives. Baah said: In this prison, if you wake up in the morning, you have God to thank and be grateful and hope for life the next day . . . others sleep to death—this makes you fear for what will happen to you the next morning.
Adam was admitted into prison at the time when there was an outbreak. He narrated his experience: I remember coming to the prison when there was an outbreak of Tuberculosis, and this had already brought tension and fear among everyone in the prison—at the time, I was afraid even to start a conversation with other inmates . . . I was afraid of getting infested by chatting with those who were here before I came—at the end, I got infested, and I nearly died.
Adam’s account reflects the experiences shared by all participant groups. The fear of contracting diseases in the prisons was pervasive and dominated the thinking of persons in custody and staff, particularly during an outbreak. Officer Azuma explained: When there is an outbreak, it takes the grace of God . . . there are times when all you are thinking about is how not to fall victim to an outbreak . . . this affects you because the least unusual feeling you have in your body gives you something to think about and if you have children, this can be worse.
Another correctional officer narrated how he “felt bad” about the hospitalization of his two children in the space of 3 weeks. He said: I nearly lost my children to a disease I believe I picked from the prison . . . I felt bad about the whole situation because I could have prevented it—most times, when I am feeling unwell, I chose to stay in the bungalow over the weekend and stay away from my family as a way of protecting them . . . I overlooked my feelings and went home. Two days after I returned, I was hospitalised and within three weeks, two of my children were also hospitalised (Officer Abu).
Some of the incarcerated individuals expressed concerns about how overcrowding and related conditions in the prisons affect them emotionally when they are about to be discharged into their respective communities.
One of the common diseases in the prison is skin rushes—you can get it at any time . . . when we are about to go home, we are very mindful not to contract it because if you go home with it no one will get closer to you (Nii).
Owu explained: Already the people outside see us as carriers of multiple diseases due to the time we spend here . . . sometimes, when it is getting closer for you to go home, you are too careful not to contract any skin diseases . . . you do not want it to be obvious to your friends and family that you came with those skin rushes, so you try keep reserved and disengage yourself, but it is not easy.
The participants indicated that the decision to protect themselves from contracting diseases before their release makes them feel self-isolated in a clouded environment. Patey said: “Sometimes you are here, but it is like you are not—your mind is on how to go home clean with no illness—you lose interest in doing what you will normally do, all to protect yourself.”
The participants’ responses depict a prison system highly congested to the point where a disease outbreak may be uncontrollable and regard for fundamental human rights pushed to the peripheral. The account by the participants suggests a prison condition that is a sharp contrast to the minimum standard for treating detained people. These have implications for policy, practice, and research.
Discussions
The current study has contributed to the discussions on prison overcrowding and related consequences. Specifically, we focused on understanding the health and human rights implication of prison overcrowding. Being the first study in the Ghanaian context to understand prison overcrowding from a human rights lens, we have highlighted how prison conditions may violate persons in custody’s rights and threaten the environmental determinants of health. All the participant groups (correctional officers and persons in custody, n = 38) indicated that the prisons were overcrowded, resulting in deplorable conditions for people who live and work in the facilities. In particular, the impact of overcrowding on the participants’ well-being and fundamental human rights were issues of significant concern to persons in custody and correctional officers alike.
The two participant groups had a point of convergence and divergence in their perspective of prison overcrowding. They both acknowledged the prisons were overcrowded; the officers indicated efforts were in place to address it, while the person in custody thought otherwise and felt the correctional officers were apathetic about their situation. Issues relating to the impact of overcrowding on rehabilitation featured more in the correctional officers’ data set than in the data set of persons in custody counterparts. This could be the case that the persons in custody were more concerned about meeting basic needs such as food, water, and conducive sleeping space. Generally, the participant groups shared a similar sentiment about the effects of overcrowding, indicating the phenomenon had implications on effective prison management by putting pressure on limited resources and putting the health of all stakeholders at risk.
Rule three of the Nelson Mandela Rules (UNGA, 2016) requires prison administrators to cease practices and treatments that aggravate the suffering of individuals whose liberty is legally restricted. Our findings suggest that the persons in custody’s punishment (custodial sentence) was aggravated by administrative failures, which have supervised the accommodation of over 3000 individuals in a 700-capacity prison facility. Consequently, the persons in custody were compelled to sleep in turns due to limited sleeping space, survive on limited and insufficient food, and struggle over toilet facilities. In the current study, overcrowding in the selected prisons had reached a point of concern (human rights violation), requiring immediate actions from stakeholders, given the conditions under which the participants lived.
The basic principle of human rights is that human beings, irrespective of their circumstances, are treated humanely with respect and dignity and provided the opportunity to enjoy basic human rights such as security, shelter, health, potable water, and food. Per the findings, we argue that it became impracticable for the prisons to ensure the human rights of occupants in a facility overcrowded by 200%. One Romanian-based study argued that overcrowding creates circumstances that make it difficult for persons in custody to enjoy certain human rights (Chirita, 2019). Baffour (2021) reasoned that overcrowding limits the ability of prison officers to provide core services such as care, protection, rehabilitation, and ensuring persons in custody’s well-being. Like the case of the current study, the astronomical increase in the prison population failed to match the existing resources needed to promote prison occupants’ right to health, shelter, food, dignity, and security.
A study conducted in Central and Southern America highlighted the high prevalence of tuberculosis among persons in custody and partly attributed the cause to an increasing prison population (Walter et al., 2021). In addition to tuberculosis, the current study has reported other diseases persons in custody and prison staff were confronted with. While the cause of this malice could partly be attributed to overcrowding and structural failures, the current analysis agrees with Ghanaian-based studies that suggested persons in custody were largely responsible for their health care due to little to no medical services in the prison facilities (Baffour, 2020; Baffour et al., 2022b). We agree with the statement by Walter et al. (2021) that “the detention of people in an environment with an extraordinarily high risk of tuberculosis infection, without access to adequate preventive measures or health care, constitutes a systematic violation of national and international human rights laws . . .”
The World Health Organization’s [WHO] constitution and the Universal Declaration on Human Rights [UDHR] highlight people’s right to health. Article 25(1) of the UDHR stipulates the right to a living condition that promotes individuals’ well-being, emphasizing food, clothing, shelter, and medical care (UNGA, 1948). In the current study, the participants lamented little to no access to medical care in the selected prisons. The poor health care system is attributed to inadequate funding and skilled health care staff and overcrowding in studies conducted in Ghana and Zambian prisons (Baffoe-Bonnie et al., 2019; Topp et al., 2017). Another study conducted among individuals serving life sentences in Ghana reported that participants’ mental health symptoms were left undiagnosed and untreated due to the little to no mental health services and expertise in the country’s prisons (Baffour et al., 2022b). We argue that keeping people in a deplorable condition and ignoring their health and well-being needs is tantamount to torture, degrading and inhuman treatment, and human rights violations, which must be resolved urgently.
Limited access to basic needs such as food, shelter, and sleeping space reported in the current study is supported by a scoping review of prison literature conducted in 37 sub-Saharan African prisons. Van Hout and Mhlanga-Gunda (2019) observed that “basic needs are not met in relation to sanitation, ventilation, safe spaces, protection from physical and sexual violence, clothing, food, and access to HIV and medical care.” (p. 1). By way of analysis, it is important to understand if the issue of inadequate and malnourish food served in the prisons could only be attributed to overcrowding. We argue that the daily feeding fee of GHC1.80 a day (0.22 USD) is insufficient and could partly contribute to the standard of food served in the country’s prisons. We anticipate that the rising inflation rate in the past two years as a result of the COVID-19 pandemic and other international political issues calls for an urgent review of the current feeding fee in Ghana prisons. This has implications for policy, practice, and research.
Further, the current analysis has reported that overcrowding tends to cause tension in prison due to the struggle over scarce resources, which has implications for prison occupants’ right to security. Even though the extant literature in the Global North and West have reported inconsistencies in the effects of prison overcrowding and persons in custody’s infractions and violence (Dean, 2017; Farrington & Nuttal, 1980; Glazener & Nakamura, 2020; Wooldredge & Steiner, 2009), our findings pass credibility text for two reasons. First, the extant literature on overcrowding in the African context has reported the negative impact of overcrowding on prison violence and infractions (Baffour, 2020; Sibisi & Olofinbiyi, 2021). Second, Baffour et al. (2022a) suggested that the prison administration system and conditions in the Global North and West are different from those in the Global South, particularly Ghana. That said, even though we are not attempting to trivialize overcrowding in the Global North and West, we assume that the congestion and condition of living described by the participants in this study suggest an environment drowned in tension partly due to struggle over basic needs such as food, sleeping space, and toilet facilities.
Unsurprisingly, the poor living conditions and overcrowding, coupled with the blatant violation of fundamental human rights in the prisons, had impacted the persons in custody’s psychological and emotional well-being. Studies conducted in Ghana and jurisdictions outside have reported that overcrowding was associated with mental health conditions such as self-harm and suicide ideation (Baffour et al., 2022b; Wolff et al., 2016). Wolff et al. (2016), in particular, attributed the increase in self-harm in Switzerland prisons to the struggle over scarce resources. A sub-Saharan African study by Nwefoh et al. (2020) attributed the high rate of depression among persons in custody to the poor conditions in the Nigerian prison. The current study has reported similar events, even though it did not set out to measure the relationship between overcrowding and suicide ideation, as well as other mental health conditions, the emotional and psychological consequences of prison congestion if not identified and managed could negatively impact on the mental health of people who live and work in the prison.
The GPS (2020) annual report revealed that one person in custody committed suicide in the calendar year. While this rate is low compared to other jurisdictions (Stoliker et al., 2021; Zhong et al., 2021), it still raises concerns, given that past studies conducted in Ghana have reported suicide ideation and other mental health complications among persons in custody (Baffour, 2021; Baffour et al., 2022b). Stoliker (2018) suggested that persons in custody with psychological distress and other mental health complications are more likely to attempt suicide.
Another debate in the extant literature is the impact of overcrowding on rehabilitation and recidivism (Baffour, 2021; Nkosi & Maweni, 2020). A classical study by Farrington and Nuttall (1980) suggested that overcrowding destructs prison management and administration effectiveness. Our analysis supports Farrington and Nuttall’s report, explaining the perceived negative impact of overcrowding on prison-based rehabilitation due to its ability to reduce meaningful contact between persons in custody and correctional officers, limiting their access to treatment and trade programs. Nkosi and Maweni (2020), in a South African-based study, support our findings that overcrowding compromises rehabilitation. In Ghana, the prison service’s mandate is to ensure safe custody and persons in custody’s welfare and undertake rehabilitation when prison conditions and available resources permit (Baffour, 2019), making it likely for prison administrators to overlook rehabilitation in the current situation described in this study. We believe a custodial sentence without a proper rehabilitation program regime is costly to all stakeholders, particularly persons in custody, which may increase their criminogenic needs post-prisons. Baffour (2021) highlighted the “. . . aim of rehabilitation and reformation of incarcerated inmates is to instill in them prosocial behavior, healing, interpersonal, and life skills and empower them to be economically independent—all in the effort to reduce their reincarceration risks” (p.1175). Further, Nelson Mandela Rule 4 emphasizes the importance of rehabilitation in any efforts aimed at reducing recidivism.
Ghana has ratified international prison rules and conventions such as the Nelson Mandela Rules, KDPCA, KDHPA, and the ODPAAPPRA, to name a few. The rules and conventions listed above recognize the negative impact of prison conditions and obligate state parties to promote the well-being and human rights of persons in custody in African prisons, Ghana included. For example, in 1999, the KDPHA suggested an urgent need for prison reforms that improve conditions in African prisons. The ODPAAPPRA (2002) made a similar call and suggested the need for countries to pay attention to overcrowding in African prisons. Two decades into these declarations, prisons in Africa, particularly Ghana, continue to be overcrowded, causing prison administration challenges.
Despite the significant contribution of the current study, we identified methodological and security limitations that need consideration when interpreting the findings. Overcrowding affects all individuals living in the prison space. However, the nature of the study limited the participation of first-time persons in custody who could have provided dynamic and diverse information to further strengthen the study. Future research that extends investigation to all persons in custody could build on the current study to provide much more diverse information on prison overcrowding. Further, one study in Ghana reported the intense security protocols researchers go through to conduct prison research (Baffour et al., 2022a). This always creates a tense ambiance for researchers and participants alike, and we noticed this during a few interviews during data collection. Our ability to anticipate these challenges and the impact they could have on data collection helped in mitigating this potential threat by clearly explaining the purpose of the study and agreeing with prison officers to stay a few meters from the interviews. Yet, we cannot dismiss the impact it could have on the individuals in custody. Despite the limitation of the study (which has also been identified in previous studies in Ghana and other jurisdictions; Abbott et al., 2018; Baffour, 2021), our findings have implications for policy, research, and practice.
Implications
Based on the analysis from the current study, we have suggested the following four approaches (Depopulation, Implementation of international conventions and local laws, Alternative means of punishment, and Coproduction in offender management and prison administration [DIAC]) for consideration:
First, an effort toward prison depopulation is required: this can start with the GPS and other stakeholders prioritizing the completion of the maximum-security prison. As we indicated in the current study, the maximum-security prison, even though it started operation in 2011, is still under construction and accommodates less than its intended capacity. We believe completing the second phase would be a step toward depopulation. The analysis suggests that overcrowding was a pathway to many challenges faced by the prisons. To this end, a prison depopulation agender would help the GPS work toward mitigating many of the challenges confronting the prisons, such as the struggle over scarce resources and reducing social distancing between incarcerated individuals and prison staff.
Second, implementation of international conventions and declarations, as well as local laws and policies on the treatment of persons in custody and prison administration: Ghana has ratified many international treaties and conventions on the rights and treatment of persons in custody, which the findings presented in the current study suggest they are barely implemented or applied. We suggest that the prison administration and the Ghana Government’s efforts to abide by its laws (such as the 1992 constitution and 1972 Prisons Service Act), as well as the provisions in international prison conventions and treaties such as the Nelson Mandela Rules, KDPCA, ODPAAPPRA, KDHPA, among others, would contribute to improve the conditions in the country’s prisons and promote the fundamental human rights of persons in custody.
Third, alternative means of punishment: in Ghana, the punishment options available to the courts are custodial sentences and fines. In a developing country like Ghana, where many people live below the poverty line, there is a possibility many people asked to pay fines by the court may default, leading to imprisonment and could account partly for overcrowding. Based on the current analysis, we suggest an urgent need for noncustodial sentences to serve as an alternative to fines for those who cannot pay fines imposed by the courts. Further, a system where a person in custody can serve part of their sentence in the community after demonstrating good behavior can be introduced in the country’s penology system. In Australia and the Global North and West, parole is predominantly used to honor good behaviors. The GPS can adopt this system in a cultural and context-appropriate manner to manage overcrowding and resulting consequences.
Fourth, a coproduction between prison officers, criminal justice social workers, and other human service professionals is needed: the suggestions presented above will best be implemented by prison officers, administrators, criminal justice social workers, and other human service professionals. As recommended in Baffour (2020), we believe that social workers, because of their skills of empathy and compassion and core values in social justice and the promotion of equality through individual dignity and respect, are well-placed to promote prison well-being and human rights.
The effective implementation of the suggestions above will be complemented by future research focusing on understanding persons in custody’s knowledge of human rights issues and standard treatment in prisons. Other future studies should employ clinical methods to understand the mental health implication of overcrowding, risk assessment for recidivism in crowded Ghanaian prisons, and investigate the impact of workforce development targeting training prison staff on ethical prison practices.
Conclusion
In recent times, health and well-being are not just the individual’s ability to create and maintain healthy behavioral cultures but a collective effort from the individual, their community, and the state. The findings presented in this study suggest that in the event where the individual’s liberty and other fundamental human rights, such as the decision to choose the food to eat, clothing to wear, and place to sleep, are externally managed and decided, the onus lies on the managers (prison administrators) to maintain and promote the health, dignity, and worth of those (incarcerated individuals) who bear the direct consequences of their decisions. We suggest that the deprivations coupled with systemic overcrowding and resulting harsh conditions infringe on the fundamental human rights of those whose liberty has been curtailed in exchange for public security and protection in the carceral system.
What we already know is that the effective way to address the health and well-being of a population is the adoption of a population health approach where the health and well-being of vulnerable groups are prioritized and the recognition that multiple factors interplay to affect population health. Therefore, the findings of the current study and the fact that the GPS (2020) reported 47 deaths in a calendar year across the country’s prisons call for a pragmatic approach directed at multiple factors (overcrowding causing disregard for the person in custody’s health and well-being, infractions and violation of fundamental human rights) that could impact prison population well-being and human right.
Further, the prison is an institution within a community. Like the case of the current study, all the selected prisons were either sited in the middle of a city/town or closer. In addition, the prison officers work in the prisons and live in the communities. To this end, it is assumed that an unhealthy prison environment could affect the health of the entire community and the nation at large, making the factors that impact incarcerated individuals’ well-being public health concerns, requiring a national strategy to address them.
While we ask for carefulness in the generalization of our findings, we also believe that the current analysis has implications for prisons across the globe by suggesting that overcrowding, irrespective of the magnitude, requires adjustment on the part of persons in custody and prison staff, and compromise on the part of prison administrators. While such adjustment would favor prison administrators and continue to serve the public interest through incapacitation, it has implications for incarcerated individuals’ well-being, human rights, and the tendency of undermining prison and public security, as well as the health of a country’s population. To this end, we suggest that prison overcrowding is not just a problem in Ghana but a global public health and human rights violation challenge that requires national and international approaches to address it.
The current study, in addition to giving a voice to one of the marginalized populations in the world, has also touched on a phenomenon that not only perpetuates injustice but is a threat to national and global public health. Given that overcrowding could impact national security and population health, there is an urgent need to prioritize efforts to address prison overcrowding, improve prison conditions, and promote persons in custody’s well-being and human rights to mitigate potential public health and security crises that could begin from the prison.
Footnotes
Authors’ Note:
The authorship and publication of this research received no external funding support. We extend our heartfelt gratitude to the Ghana Ministry of the Interior and Ghana Prisons Service for generously allowing this study to be conducted within their facilities.