
Abstract
We meta-analytically examined program graduation rates among juvenile drug treatment court (JDTC) participants, the effects of JDTCs on recidivism and substance use outcomes, and the variability in these effects. We systematically searched for controlled evaluations examining the effects of U.S.-based JDTCs relative to traditional juvenile adjudication and used mixed-effects meta-regressions with robust variance estimates. We identified 55 eligible samples (providing data from 12,310 participants); the overall certainty of evidence was low or very low. The average graduation rate among JDTC participants was 54.74% (95% confidence interval [CI] [0.50, 0.59]). JDTCs had modest beneficial effects on general recidivism assessed during court supervision (odds ratio [OR] = 1.38, 95% CI [1.03, 1.84]) but these effects did not persist after program completion. Correlational analyses suggest JDTCs may be effective when program enrollment and service provision are better tailored to youth’s treatment needs. However, due partly to implementation failures, JDTCs may have minimal to no effects on postprogram recidivism.
The developmental transition from childhood to adulthood can be marked by an increase in the frequency of risky behavior, particularly the consumption of illicit substances (Degenhardt et al., 2016). Although developmentally normative, increased substance use during adolescence may be associated with increased aggression, delinquency, and the corresponding risk of contact with the juvenile justice system (Chassin, 2008; Doran et al., 2012; Young et al., 2012). Many justice-involved youth suffer from substance use disorders and addiction, which are correlated with the risk of recidivism (van der Put et al., 2014). Rehabilitative programs that treat justice-involved youth’s substance-related issues may therefore be effective in reducing their risk of recidivism. Juvenile drug treatment courts (JDTCs), defined here as problem-solving courts that aim to reduce recidivism by explicitly treating youth’s substance-related problems in a therapeutic and supportive manner, offer one such approach.
Typical elements of JDTCs include assessments of youth’s unique criminogenic risks and needs, frequent interactions between the youth and a judge or other court staff, intensive monitoring by court staff, behavior-shaping through incentives and sanctions, and referral to community-based substance use treatment services (Belenko & Dembo, 2003). In contrast to traditional juvenile courts, which are often guided by punitive deterrent policies, JDTCs are intended to be rehabilitative and responsive to the individual criminogenic needs of drug-involved and justice-involved juveniles (Office of Juvenile Justice and Delinquency Prevention [OJJDP], 2016). The goal of JDTCs is to reduce the risk of recidivism by providing tailored and supportive treatment; such benefits, however, may not be conferred to youth who fail to complete the full JDTC program.
The first drug treatment court program opened in 1989 in Miami-Dade County, Florida; in 2020, there were an estimated 3,848 drug courts in the United States, with 618 of those classified as JDTCs (National Drug Court Resource Center, 2021). Prior reviews suggest that adult drug courts are effective in reducing recidivism when compared to traditional judicial interventions (Mitchell et al., 2012; Rossman et al., 2011). Despite promising evidence supporting the effectiveness of adult drug courts, the evidence based on the effectiveness of JDTCs has been inconsistent and inconclusive (Tanner-Smith et al., 2016). This systematic review and meta-analysis therefore seeks to synthesize the current available evidence regarding the effects of JDTCs on recidivism and drug use, with specific emphasis on understanding whether and how JDTC completion (i.e., graduation) may play a role in this effectiveness.
JDTC Model
Whereas traditional criminal courts have historically used punitive approaches to deter criminal behavior (Loughran et al., 2015), problem-solving courts use a rehabilitative orientation wherein criminogenic needs are treated to reduce reoffending (Butts & Roman, 2004). Drug treatment courts are one type of problem-solving court, which aims to treat harmful substance use behaviors that may contribute to criminal offending (van der Put et al., 2014). JDTCs are specifically designed to use developmentally appropriate services to address the unique treatment needs of justice-involved youth (Belenko & Dembo, 2003). Services provided by JDTCs typically include status hearings with the court’s presiding judge, coordination between the court and the youth’s family, random drug screenings, community supervision, referrals to community-based substance use treatment services, and the use of incentives and sanctions to monitor compliance with program mandates. Most JDTCs are intended to take 12 to 18 months to complete, although the length of time required to complete these programs can vary widely. Youth who fail to graduate from JDTCs are typically expelled due to violations of program requirements such as failing urinalysis tests, failing to appear in court, or failing to attend mandated treatment services, although some youth may choose to discontinue participation in the program due to personal or family reasons (Polakowski et al., 2008; Sloan et al., 2004).
In 2003, the National Drug Court Institute and National Council of Juvenile and Family Court Judges convened a workgroup of experts that outlined 16 strategies and recommendations for JDTC implementation (U.S. Bureau of Justice Assistance, 2003). These 16 strategies were not designed to be research-based benchmarks. So, in 2016, the OJJDP (2016) collaborated with juvenile justice researchers, stakeholders, and other federal agencies to develop updated evidence-based guidelines for JDTCs based on existing research, including several systematic reviews and meta-analyses.
These OJJDP JDTC Guidelines include 28 evidence-based guidelines that JDTCs are recommended to follow, which fall under seven key objectives: (1) Focus the JDTC philosophy and practice on effectively addressing substance use and criminogenic needs to decrease future offending, decrease substance use, and increase positive outcomes; (2) Ensure equitable treatment for all youth by adhering to eligibility criteria and conducting an initial screening; (3) Provide a JDTC process that engages the full team and follows procedures fairly; (4) Conduct comprehensive needs assessments that inform individualized case management; (5) Implement contingency management, case management, and community supervision strategies effectively; (6) Refer participants to evidence-based substance use treatment, to other services, and for prosocial connections; and (7) Monitor and track program completion and termination, including facilitating equivalent outcomes for all program participants regardless of gender, race, ethnicity, or sexual orientation. Adherence to these guidelines is intended to help JDTCs improve the lives of participating youth by reducing their risk of recidivism and substance use, improving their mental and physical health, and promoting their healthy development.
Prior Reviews of JDTC Research
Several prior reviews have examined the effectiveness of JDTCs, but findings from these reviews have been inconsistent. Early narrative reviews of JDTC research concluded that there is limited evidence of their effectiveness in reducing recidivism, in part due to methodological limitations and weaknesses in the primary evaluation literature (Belenko, 2001; Roman & DeStefano, 2004). Later narrative reviews suggested JDTCs may be effective for reducing recidivism but noted their effectiveness might be contingent upon their ability to integrate theory-grounded and evidence-based practices into operations (Henggeler, 2007; Van Wormer & Lutze, 2011). More recent systematic reviews and meta-analyses have concluded that JDTCs are associated with reductions in recidivism, but these benefits are less than those conferred by adult drug courts (Mitchell et al., 2012; Shaffer, 2006) or are modest “at best” (Stein et al., 2015). In the most recent and comprehensive meta-analysis to date, JDTCs were found to be no more (or less) effective than traditional juvenile court processing for reducing recidivism or drug use (Tanner-Smith et al., 2016), replicating null findings from other reviews (Latimer et al., 2006).
All of these prior meta-analytic reviews, however, used techniques to handle dependent effect sizes that resulted in a significant loss of data. Namely, numerous effect sizes reported in the literature were either dropped entirely from the analysis or combined into synthetic averages of all effects reported within a given study. These techniques are no longer necessary given recent methodological innovations in integrative techniques for handling dependent effect sizes (e.g., robust variance estimation), which allow researchers to analyze all available evidence reported in the literature by permitting the inclusion of multiple effect sizes per study in the meta-analytic models (López-López et al., 2018).
Given the inconsistent conclusions from prior reviews, an updated and comprehensive systematic review of the empirical evidence is warranted to better understand the overall effects of JDTCs on justice-involved youth’s recidivism and substance use and to explore the potential reasons why JDTCs may have null effects on these outcomes. One consideration that has not been fully explored in prior meta-analytic reviews is whether JDTC completion (graduation) may play a role in JDTC effects. The successful implementation and delivery of the full range of therapeutic components intended to be provided in a JDTC, and participants’ subsequent graduation from the program, may play an important role in whether the program yields beneficial effects.
Graduation from JDTCs has been shown to be associated with improved socioemotional functioning (Applegate & Santana, 2000; Thompson, 2006). Prior reviews and outcome evaluations have found that JDTCs provide program graduates with comparable benefits (Applegate & Santana, 2000; Sloan et al., 2004; Stein et al., 2015), some of which may persist into adulthood (Carter & Baker, 2011). In the most comprehensive review to date, Stein and colleagues (2013) synthesized evidence from 41 JDTC evaluations and found that slightly more than half of JDTC participants graduated from the program and recidivism was more likely among program dropouts. This review highlighted the importance of considering premature program termination as a possible reason for the minimal JDTC effects reported in the literature but only included evidence available through 2011. Research from the adult drug court literature also suggests that justice-involved adults who successfully complete a drug court program are less likely to recidivate and, those who do recidivate take longer to do so than those who are prematurely terminated (Gallagher, 2014; Taxman & Bouffard, 2005). Thus, the null JDTC effects reported in prior reviews could be due in part to low levels of JDTC program completion.
Objectives
Prior reviews of JDTCs have not exhaustively identified the features of these courts that may enhance (or inhibit) their effectiveness, nor have they systematically investigated the importance of JDTC graduation rates using the most recent available evidence. The current systematic review and meta-analysis aim to address these gaps in the literature. This meta-analysis therefore synthesizes findings from the current evidence base of JDTC research to examine (a) program graduation rates among JDTC participants, (b) the effects of JDTCs versus traditional court processing on youth’s recidivism and drug use outcomes, and (c) variability in these effect sizes across key characteristics of the participants and JDTCs.
Method
Protocol and Registration
The current study presents findings from an update to a prior meta-analysis examining the effects of JDTCs (Tanner-Smith et al., 2016). This updated meta-analysis used the same literature search and data collection procedures as the prior parent meta-analysis, and this update adds findings from 23 additional study samples. The protocol and analysis plan for this updated meta-analysis were pre-registered on OSF (https://osf.io/cjwnq/).
Inclusion and Exclusion Criteria
To be eligible for inclusion in the review, studies had to (a) evaluate the effects of a JDTC program, defined here as a specialized court designed to handle juvenile drug-involved cases, where the court refers youth to community treatment services, conducts regular drug screens, and involves a judge who actively monitors the youth’s progress and implements sanctions and rewards; (b) include a business-as-usual comparison condition (e.g., traditional court processing such as probation with or without referral to treatment services); (c) measure at least one criminal recidivism outcome after the start of the program; (d) report findings on a juvenile sample of youth age 18 or under; (e) be published during or after 1989; (f) be conducted in the United States 1 ; and (g) use an eligible controlled research design. 2 There were no other restrictions on eligibility. We restricted eligibility to studies conducted in the United States given that this review was designed to inform guidelines for best practices in U.S. JDTCs and given cross-cultural variability in JDTC structures and approaches.
Search Strategy
A comprehensive literature search strategy was used to identify studies that met all inclusion criteria. We included all studies that were originally reviewed in the prior meta-analysis on JDTC effectiveness (Tanner-Smith et al., 2016), which contained literature released between 1989 and December 2014. An updated literature search was used to identify any additional eligible studies reported between January 2015 and June 29, 2021 (see Supplemental Material, available in the online version of this article). We searched the following electronic databases using the ProQuest host: ERIC, International Bibliography of Social Sciences, ProQuest Criminal Justice, ProQuest Education, ProQuest Social Science, ProQuest Sociology, ProQuest Dissertations & Theses (United States, United Kingdom, and Ireland), and Sociological Abstracts. We searched the following databases using the American Psychological Association PsycNET host: PsycINFO, PsycARTICLES, and PsycTESTS.
We also conducted extensive supplementary searches of the following databases, research registers, and websites: Campbell Collaboration Library, Cochrane Collaboration Library, CrimeSolutions.gov repository, International Clinical Trials Registry, National Criminal Justice Reference Services, Center for Court Innovation website, Chestnut Health Systems website, National Drug Court Institute website, National Council of Juvenile and Family Court Judges website, NPC Research website, RAND Drug Policy Research Center website, Reclaiming Futures website, JJ Trials website, and the Urban Institute website. We also conducted hand-searches of 2015 to 2021 conference proceedings from the American Society of Criminology, as well as manuscripts published between 2015 and 2021 in Drug Court Review and Juvenile & Family Court Journal. Finally, we checked the bibliographies of all screened and eligible studies, as well as the bibliographies of narrative reviews and meta-analyses identified in the search. The literature search strategy was not restricted to studies conducted in the United States; however, studies identified during the search were evaluated for eligibility (including country location) during the screening stage.
Screening and Coding Procedures
Under the supervision of the first author, a team of bachelor’s and master’s level research assistants conducted screening and coding in three stages. First, all titles and abstracts were screened independently by two reviewers; we retrieved the full text for any report deemed potentially eligible by at least one reviewer. Second, all resulting full-text reports were independently screened for eligibility by two reviewers; the first author resolved any disagreements at this stage. Third, studies deemed eligible for inclusion were independently coded by two reviewers; again, the first author resolved any coding disagreements at this stage. All data extraction followed a standardized coding protocol, with data entered directly into a Claris FileMaker Pro relational database. A coding protocol provided detailed instructions for extracting data related to study characteristics, participants, drug treatment court conditions, comparison conditions, outcome measures, and statistical data necessary for effect size calculations.
Statistical Procedures
Effect Size Metrics
We used a proportion (p) effect size to quantify JDTC graduation rates. All analyses for graduation outcomes were conducted using the logit transformed proportion, with results transformed back into proportions for ease of interpretation. We used a log odds ratio (LOR) effect size to quantify JDTC versus comparison group effects for the binary outcomes of general recidivism (a new offense, arrest, conviction, referral, etc., not related to drugs), drug recidivism (a new drug-related offense, arrest, conviction, referral, etc.), and substance use (i.e., consumption of alcohol or other drugs). Some studies (k = 11) measured recidivism or substance use outcomes on a continuous scale (e.g., mean number of new arrests); for these studies, we first computed a small-sample corrected standardized mean difference effect size (Hedges’ g) and then used the Cox transformation to convert those to LORs (Sánchez-Meca et al., 2003). All analyses for these outcomes were conducted using the LOR effect size, with results transformed back into odds ratios (ORs) for ease of interpretation. These ORs were coded with values >1 indicating relative beneficial effects for the JDTC group (i.e., lower recidivism, lower substance use) and values <1 indicating relative beneficial effects for the comparison group. 3
Study Methods, Quality, and Risk of Bias Indicators
We collected data on several measures related to study methods, quality, and risk of bias. This included measures of study design (randomized experiment vs. quasi-experiment/regression discontinuity design), overall attrition from baseline to first follow-up, and differential attrition between the JDTC and comparison groups. We also measured whether there appeared to be possible problems in the implementation of the intended JDTC program elements (yes/no/unclear), which might have included problems such as staffing challenges, difficulties linking participants with community resources, or other sources of uncontrolled variation or degradation in the delivery of the intended JDTC model.
We also measured baseline equivalence effect sizes indexing the difference between JDTC and comparison group participants at baseline in terms of age (in years; measured with Hedges’ g), criminogenic risk (presence vs. absence of a risk factor such as a prior arrest history, measured with OR), race (White vs. person of color, measured with OR) and sex (female vs. male, measured with OR). All baseline equivalence effect sizes were coded such that positive values (g > 0, OR > 1) indicated the youth in the JDTCs were at lower risk of recidivism than those in the comparison group. These risk categories were informed by prior meta-analytic evidence on predictors of crime and recidivism (Tanner-Smith et al., 2013); for example, JDTCs with more participants of color, more participants with prior arrest histories, and more male participants than comparison conditions were coded as having higher baseline risk.
Moderator Variables
We collected data on a wide range of study characteristics to examine as potential moderators or predictors of effect size magnitude. In addition to the study methods characteristics noted above, other general study characteristics included publication type (journal article vs. other), publication year, and U.S. Census region (Midwest, Northeast, West vs. South). Characteristics of the participating youth included the sex composition of the sample (percent male), racial/ethnic composition of the sample (percent Black, Hispanic, and White), average age of participants, average number of arrests prior to program entry, average number of drug-related arrests prior to program entry, and average number of prior convictions prior to program entry.
Measured characteristics of the JDTCs included the year first opened, number of youth served per year, number of youth served in the most recent year, number of court phases, number of drug tests per week in the first phase, number of status hearings per month in the first phase, and length of the court (in months). We also measured JDTC practices to assess general adherence to the OJJDP JDTC Guidelines based on information reported in the studies. Proxy indicators for the Guidelines Objective 1 (Focus the JDTC philosophy and practice on effectively addressing substance use and criminogenic needs) were whether studies reported establishing collaborative relationships with community partners and whether studies reported establishing linkages with local educational system partners. Indicators for the Guidelines Objective 2 (Ensure equitable treatment for all youth) were whether studies reported using clearly defined eligibility criteria for program participation and whether they reported using a standardized risk assessment tool for determining program eligibility. Indicators for the Guidelines Objective 3 (Provide a JDTC process that engages the full team and follows procedures fairly) were whether the study reported actively engaging families in the process, whether they ensured the court team was collaborative and interdisciplinary, and whether the court had dedicated staffing to support the JDTC.
Indicators for the Guidelines Objective 4 (Conduct comprehensive needs assessments that inform individualized case management) were whether the studies reported using tailored and individualized treatment planning to meet the unique needs of participants, referred youth to community-based substance use treatment programs with multiple levels of care, and whether they referred youth to multiple modalities of substance use treatment programs. Indicators for the Guidelines Objective 5 (Implement contingency management, case management, and community supervision strategies effectively) were whether studies reported using consistent goal-oriented incentives and sanctions with participants, and the aforementioned measure of whether courts reported any possible implementation problems. Indicators for the Guidelines Objective 6 (Refer participants to evidence-based substance use treatment, to other services, and for prosocial connections) were whether studies reported referring participants to evidence-based substance use treatment services in the community.
Finally, indicators for the Guidelines Objective 7 (Monitor and track program completion and termination, including facilitating equivalent outcomes for all program participants regardless of gender, race, ethnicity, or sexual orientation) were whether the studies reported using developmentally appropriate program approaches, or gender-tailored/appropriate services. It is important to acknowledge that these drug court practice indicators were measured at the JDTC program level, such that JDTCs were only coded as offering developmentally appropriate approaches when the study explicitly reported the incorporation of services that were tailored to the unique developmental needs of adolescents (e.g., referring participants to adolescent-only substance use treatment programs, or referring to programs that provided skills training for negotiating peer environments where substances are present), or were only coded as offering gender-tailored services when the study explicitly reported incorporating gender-tailored services (e.g., referring participants to single-gender treatment programs or community services, or referring to programs that provided gender-specific programming such as training on the effects of prenatal substance use).
Missing Data
If primary studies failed to include sufficient statistical information needed to estimate effect sizes, we contacted the study authors for that information. Some studies also failed to provide information on the moderator variables of interest, but we did not query authors for this missing information (see Table 1 for the valid sample sizes available for each moderator). Because missing data on effect size moderators was limited, imputation was not used to recover missing values. Rather, we used pairwise deletion for all analyses and only presented descriptive or inferential information for those studies with available data.
Characteristics of the Methods, Participants, and Drug Treatment Courts in the Included Studies (k = 55)
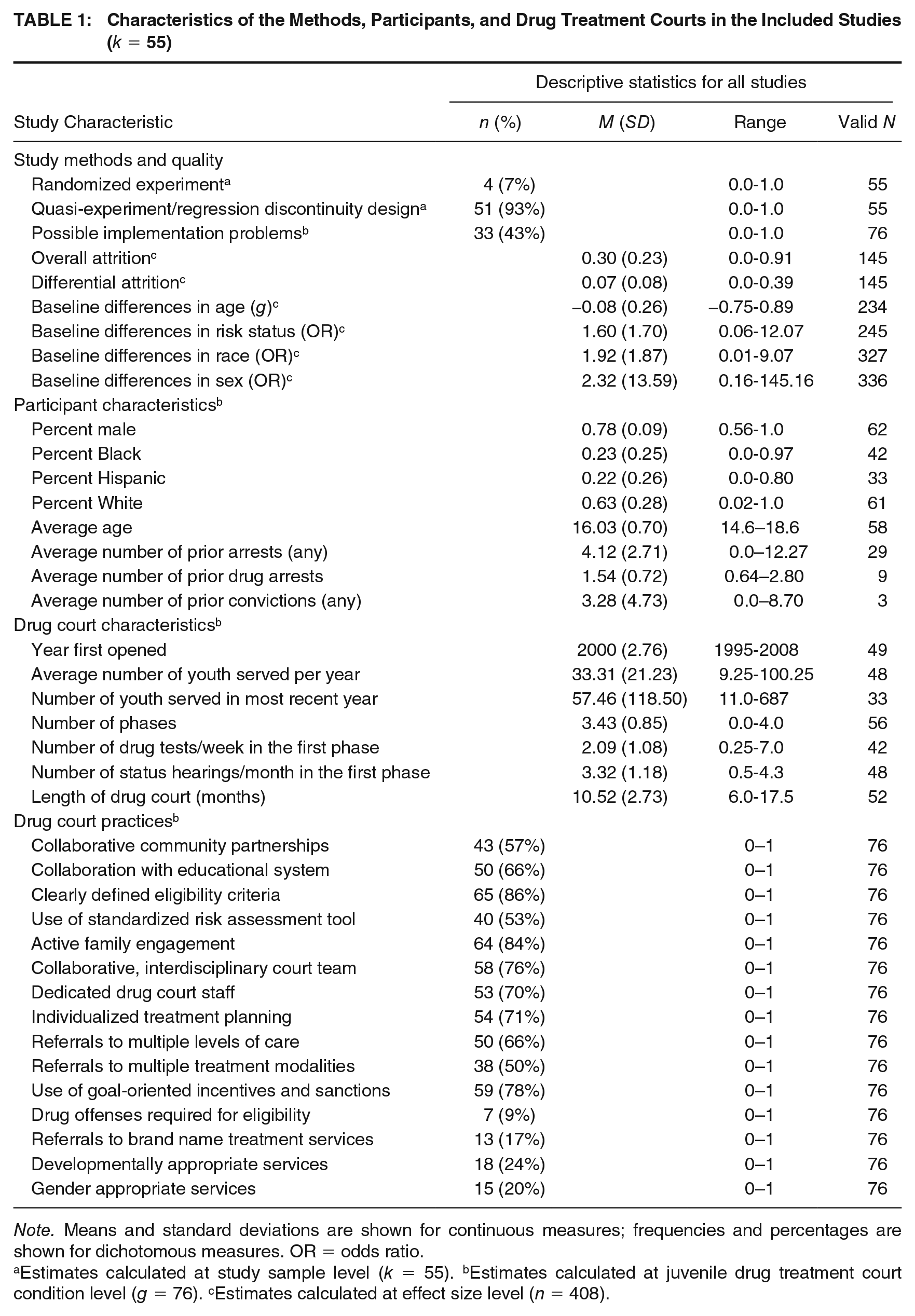
Note. Means and standard deviations are shown for continuous measures; frequencies and percentages are shown for dichotomous measures. OR = odds ratio.
Estimates calculated at study sample level (k = 55). bEstimates calculated at juvenile drug treatment court condition level (g = 76). cEstimates calculated at effect size level (n = 408).
Analytic Strategies
All analyses were conducted using random effects meta-analysis models (Hedges & Olkin, 1985; Lipsey & Wilson, 2001). When studies reported multiple, dependent effect sizes from the same study sample, meta-analyses were conducted using meta-regression models with robust variance estimates that permitted the inclusion of all observed effect size estimates from the literature (Hedges et al., 2010; Tanner-Smith & Tipton, 2014). Random-effects meta-regression models were used to obtain overall mean effect size estimates and heterogeneity statistics; mixed-effects meta-regression models were used to investigate variability in effects associated with moderator variables. Given the relatively small sample size, it was not possible to estimate multivariable meta-regression models that simultaneously adjusted for potential confounders. Thus, each meta-regression examined the bivariate relationship between a given moderator and effect size for the respective outcome. 4 Standard errors, p-values, and confidence intervals are only presented for those coefficients with adequate degrees of freedom after accounting for small sample adjustments to the robust variance estimates (Tipton, 2015).
All main effects meta-analyses were conducted separately by outcome type (i.e., program graduation, general recidivism, drug recidivism, drug use) and follow-up period (i.e., outcomes assessed during program, postprogram). To maximize analytic sample sizes, the moderator analyses pooled effects across follow-up periods but included a dummy indicator control for the follow-up period. Given the large number of moderators examined, the Benjamini-Hochberg procedure (Benjamini & Hochberg, 1995) was used to control Type I error rates for all analyses within a moderator domain using a false discovery rate of 20%. Heterogeneity was assessed using the Q-statistic and the method of moments estimator of
Results
Literature Search
We identified 3,054 candidate reports in the updated literature search (3,013 through database/register searching; 41 through other sources); 756 were duplicates that were dropped from consideration and 2,090 were screened as ineligible at the abstract level (see Figure 1). Of the 212 articles retrieved in full text, 180 were deemed ineligible. There were 44 studies (with 55 study samples) eligible for inclusion that comprised the analytic sample in the meta-analysis. These 55 study samples represent data from 12,310 individual participants (see Supplemental Material for references to and descriptive characteristics of all included studies, available in the online version of this article).
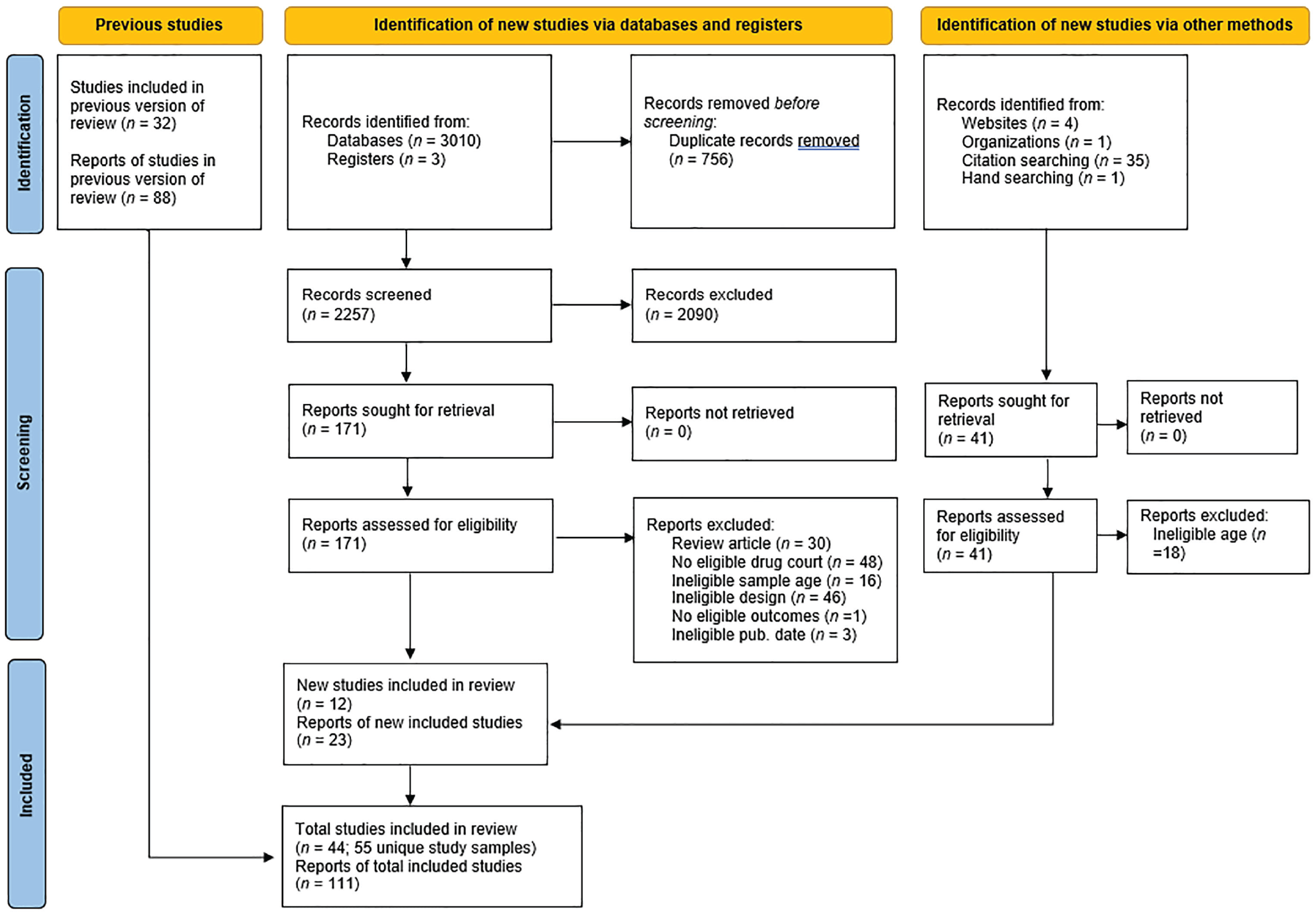
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Flow Diagram for Identification of Studies Included in the Updated Review
Description of Included Studies
Table 1 presents descriptive statistics for the key features of the study methods/quality, participants, and drug treatment courts in the 55 included samples. Only a few (16%) were published in journal articles, and they were conducted in multiple geographic regions in the United States (13% Midwest, 15% Northeast, 35% South, 33% West, and 4% multiple regions). The methodological quality of the studies was low—only four studies (7%) randomly assigned participants to conditions, one (2%) used a regression discontinuity design, almost half (43%) reported program implementation problems, the average overall attrition rate was 0.30 (SD = 0.23), and the average differential attrition between drug court and comparison groups was 0.07 (SD = 0.08). Although the JDTC and comparison groups in the studies were generally well matched in terms of age, groups were non-equivalent at baseline in terms of baseline risk, race, and sex: JDTC participants tended to be at significantly lower risk, more likely to be White, and more likely to be female than comparison group participants. Thus, this body of evidence may suffer from selection bias and there may be a risk of bias in effect estimates from these evaluations.
The study samples were predominantly male (M = 78%) and White (M = 63%), with an average age of 16.03 (SD = 0.70). Few studies reported arrest/conviction histories for participants; among those studies reporting this information, JDTC participants had an average of 4.12 prior arrests (SD = 2.71; k = 23, g = 29), 1.54 prior drug arrests (SD = 0.72; k = 6, g = 9), and 3.28 prior convictions (SD = 4.73; k =3, g = 3) upon entry into the court. On average, the JDTCs first opened in the year 2000, served 33.31 youth per year (SD = 21.23), involved 3.43 phases (SD = 0.85), conducted urinalysis screens around 2.09 times per week in the first phase (SD = 1.08), had 3.32 status hearings per month in the first phase (SD = 1.18), and lasted 10.52 months (SD = 2.73). Over half of the JDTCs explicitly excluded youth with histories of violent offenses (53%) and few (9%) required juveniles to have a drug offense to be eligible for participation in the JDTC. The last section of Table 1 shows the JDTCs’ adherence to proxy measures for the OJJDP JDTC Guidelines, which were collected based on information reported in the studies.
JDTC Graduation Rates
Table 2 presents the results of all main effects meta-analyses. The first section shows the results from the meta-analyses synthesizing the JDTC program graduation rates (see Supplemental Material for corresponding Galbraith plots, available in the online version of this article). A total of 50 study samples provided sufficient data to estimate JDTC graduation rates among program participants. In the meta-analysis synthesizing 68 effect sizes from those 50 studies, the average graduation rate was 54.74% and there was significant heterogeneity in the observed effects (95% CI [0.50, 0.59], p = .037; Q = 351.20, τ2 = 0.30). Thus, many youth who initially enrolled in JDTCs did not fully complete the requirements of the programs and thus never formally graduated from the JDTC; however, these graduation rates varied significantly across studies.
Mean Effect Sizes and Heterogeneity Estimates for All Meta-Analyses, by Outcome Type and Measurement Timing
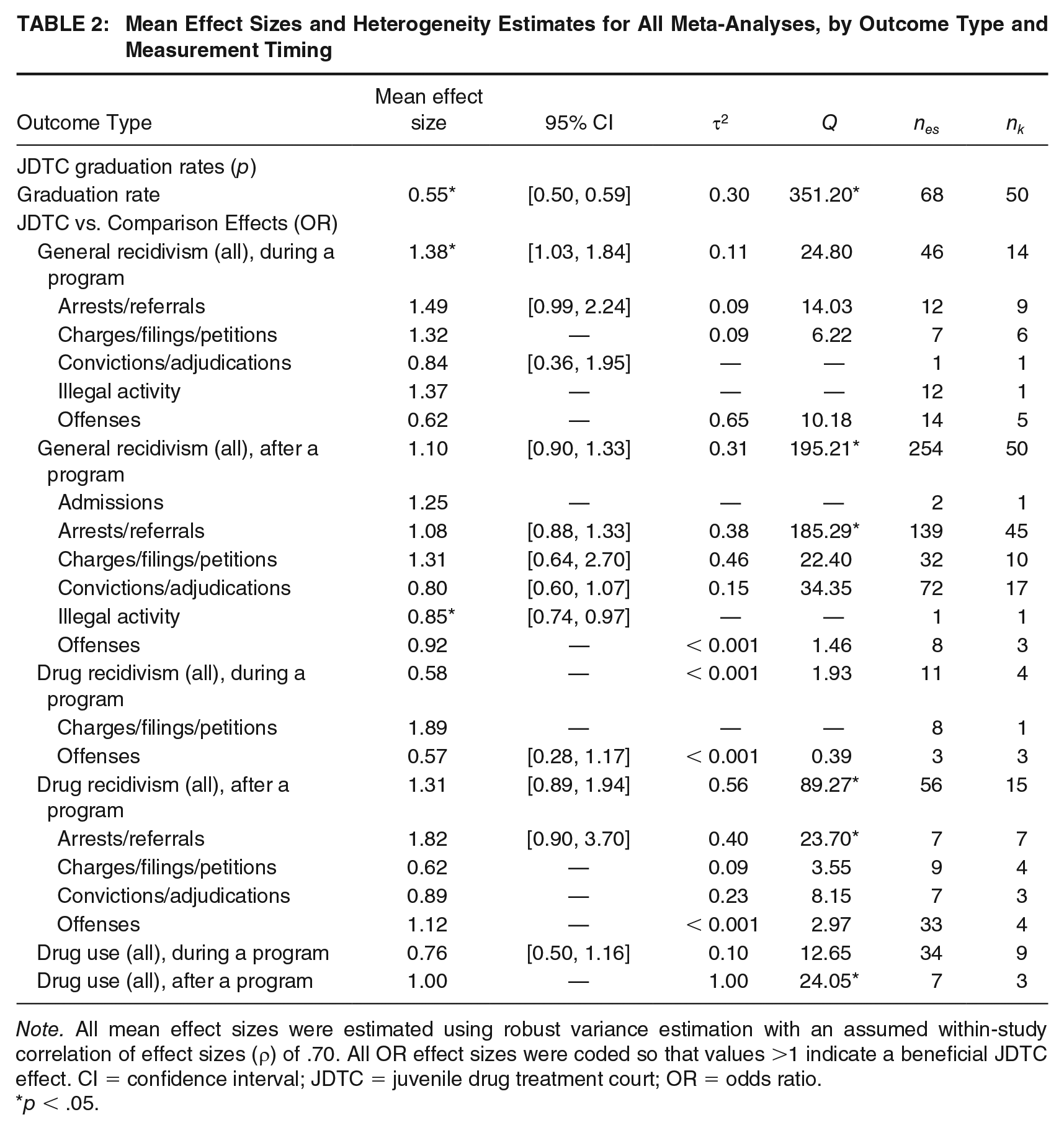
Note. All mean effect sizes were estimated using robust variance estimation with an assumed within-study correlation of effect sizes (ρ) of .70. All OR effect sizes were coded so that values >1 indicate a beneficial JDTC effect. CI = confidence interval; JDTC = juvenile drug treatment court; OR = odds ratio.
p < .05.
JDTC Versus Comparison Effects on Recidivism and Drug Use Outcomes
In the meta-analysis synthesizing 46 effect sizes from 14 study samples with general recidivism outcomes measured during the program period, JDTC participants had significantly lower odds of recidivism than comparison group participants (OR = 1.38, 95% CIOR [1.03, 1.84], p = .032; Q = 24.80, τ2 = 0.11). Namely, the odds of success among JDTC participants—defined as no recidivism during the program period—were 1.38 times higher than the odds of success in the comparison group. Or stated another way, the odds of recidivism among JDTC participants were 0.72 times lower than those of participants in traditional court processing comparison conditions. This mean effect, although statistically significant, is nonetheless relatively small in substantive magnitude: it translates to a risk ratio of 1.27, a risk difference of 6.5%, and a number needed to treat of 15 (calculated using the base rates of 24% and 31% for the JDTC and comparison groups, as shown in Table 4). When subdividing the data into more specific types of recidivism measures (arrests, charges, convictions, general illegal activity, offenses), the mean effect sizes were positive but no longer statistically significant, which is likely attributable to the lower statistical power in these models given the smaller number of included effect sizes/studies.
In the meta-analysis synthesizing 254 effect sizes from 50 study samples with general recidivism measured after the JDTC program period, the mean effect size was not statistically significant and there was significant heterogeneity in the observed effects (OR = 1.10, 95% CIOR [0.90, 1.33], p = .333; Q = 195.21, τ2 = 0.31). 5 When subdividing the data into more specific types of recidivism measures (i.e., arrests, charges, convictions, general illegal activity, offenses), there was again no evidence of a significant (positive or negative) effect of JDTCs. One study provided an effect size estimate of self-reported illegal activity recidivism after the program, indicating that JDTC participants had worse outcomes than comparison participants in terms of illegal activity (OR = 0.85, 95% CIOR [0.74, 0.97], p = .019); this result should be interpreted cautiously, however, given that it only reflects evidence from a single study.
There was no evidence of a significant (positive or negative) effect of JDTCs on drug recidivism assessed during the JDTC program period (OR = 0.58, Q = 1.93, τ2 < 0.001). However, these results should be interpreted cautiously because the meta-analyses did not have adequate degrees of freedom after applying the small sample adjustment in the robust variance estimation model. There was also no evidence of a significant (positive or negative) effect of JDTCs on drug recidivism after the program period, but there was significant heterogeneity in the observed effects (OR = 1.31, 95% CIOR [0.89, 1.94], p = .154; Q = 89.27, τ2 = 0.56). 6
Results provided no evidence of a significant (positive or negative) effect of JDTCs on drug use assessed during the program period (OR = 0.76, 95% CIOR [0.50, 1.16], p = .165; Q = 12.65, τ2 = 0.10). There was also no evidence of a significant effect of JDTCs on drug use after the JDTC program period (OR = 1.00; Q = 24.05; τ2 = 1.00). 7 But again, these results should be interpreted cautiously because the latter meta-analysis did not have adequate degrees of freedom after applying the small sample adjustment in the robust variance estimation models.
Moderator Analyses
The main effects meta-analyses presented in Table 2 provided mean effect size estimates for the two effect types of interest: JDTC graduation rates and JDTC versus comparison effects. As evidenced by the Q and τ2 estimates from these analyses, however, there was considerable heterogeneity in effects across studies (see also Supplemental Materials for Galbraith plots, available in the online version of this article). This suggests there was variability in effects across studies, so it is important to examine whether some of this heterogeneity may be explained by features of the study methods, participants, and drug courts represented in the review (as specified in our review protocol). Table 3 presents the results of the meta-regression models used to predict bivariate associations between study characteristics and the observed effects. Given the small number of effect sizes available for drug use outcomes, moderator analyses were only conducted for the JDTC versus comparison recidivism outcomes and for JDTC graduation outcomes. The Benjamini-Hochberg procedure was used to control for multiple comparisons within moderator domains and outcome types.
Bivariate Associations Between Study Characteristics and Effect Sizes
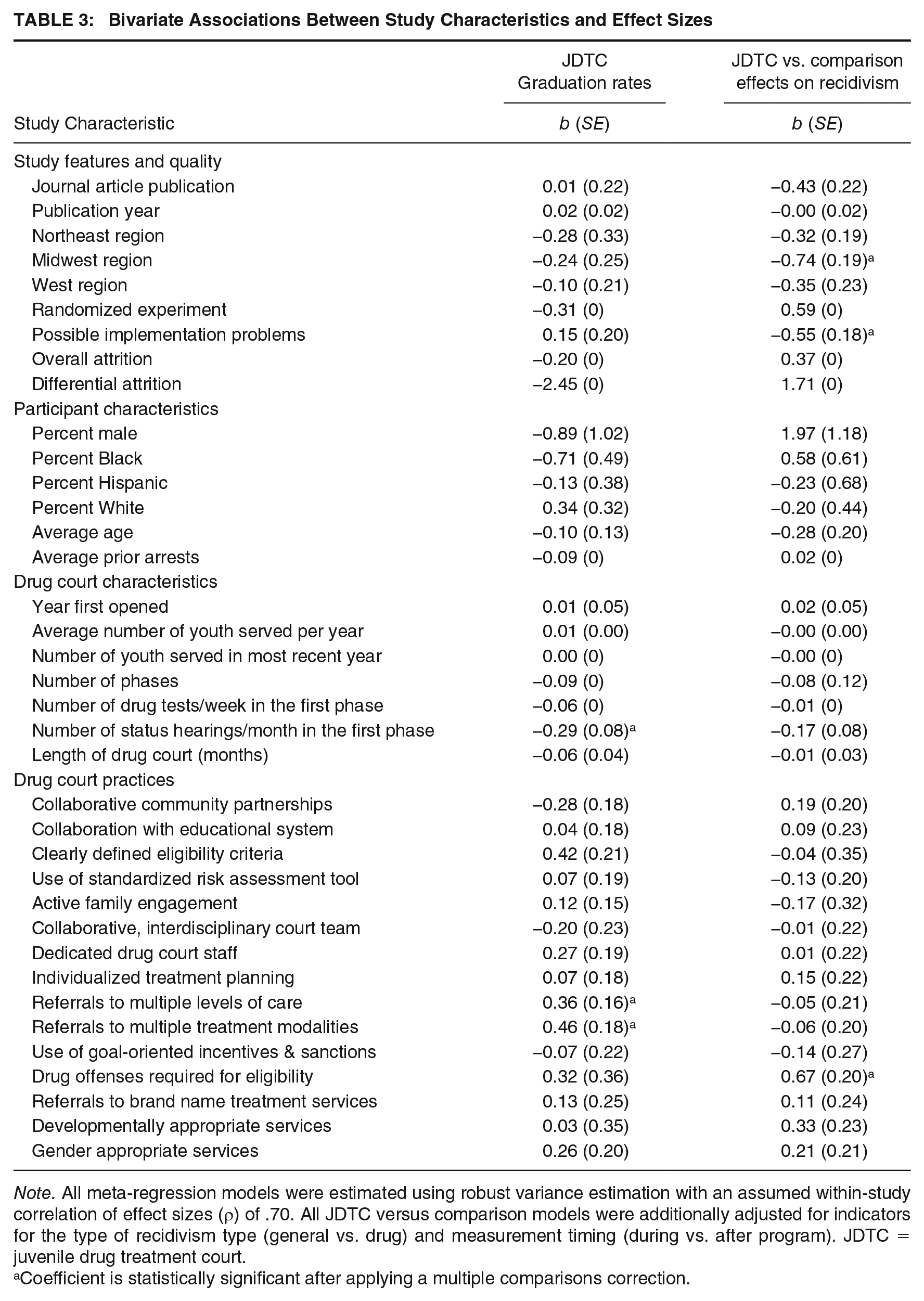
Note. All meta-regression models were estimated using robust variance estimation with an assumed within-study correlation of effect sizes (ρ) of .70. All JDTC versus comparison models were additionally adjusted for indicators for the type of recidivism type (general vs. drug) and measurement timing (during vs. after program). JDTC = juvenile drug treatment court.
Coefficient is statistically significant after applying a multiple comparisons correction.
Predicting JDTC Graduation Rates
The moderator analyses provided no evidence that any study features or participant characteristics were associated with graduation rates among JDTC programs. However, even after applying multiple comparison corrections, JDTC graduation rates were significantly lower in courts with more frequent status hearings in the first phase of the drug court (b = −0.29, 95% CI [−0.46, −0.12], p = .002, see Supplemental Material S8, available in the online version of this article). The predicted mean graduation rate for courts that had an average of one status hearing per month in the first phase was 70% versus 64% for courts with two hearings per month, and 50% for courts with four status hearings per month.
Results also indicated that JDTC graduation rates were significantly higher in those courts that referred youth to multiple levels of care for community-based substance use treatment (b = 0.36, 95% CI [0.04, 0.68], p = .029). Also, graduation rates were significantly higher in those courts that referred youth to multiple modalities of community-based substance use treatment (b = 0.46, 95% CI [0.10, 0.81], p = .013, see Supplemental Material S10, available in the online version of this article). The predicted mean graduation rate for courts referring youth to multiple treatment modalities was 61% versus 50% for courts referring youth to only a single treatment modality.
Predicting JDTC Versus Comparison Effects on Recidivism
The results provided no evidence that publication type or publication year were associated with JDTC effects on recidivism. After adjusting for multiple comparisons, effects did vary significantly by region: courts in the Midwest reported significantly smaller effects on recidivism than those in the South/multiple regions (reference category) (b = −0.74, 95% CI [−1.18, −0.30], p = .006) but all other region contrasts were non-significant. Nonetheless, despite this statistically significant association, overall, the JDTC versus comparison effects on recidivism were still consistently null across regions (see Supplemental Material S5, available in the online version of this article). There was also evidence that studies reporting JDTC implementation problems had significantly smaller effects on recidivism than those without such implementation problems (b = −0.55, 95% CI [−0.91, −0.19], p = .004). Again, despite this statistically significant association, the JDTC versus comparison effects on recidivism were on average null regardless of the presence of implementation problems (see Supplemental Material S6, available in the online version of this article). Given the small number of studies using randomized designs and the small number of studies for which attrition estimates could be calculated, it was not possible to reliably estimate the standard error of the coefficients for these predictors.
There was no evidence that the measured participant characteristics or drug court characteristics were associated with JDTC effects on recidivism. When examining drug court practices, the only statistically significant predictor was whether courts required drug offenses as an eligibility criterion for program participation, such that JDTC effects on recidivism were significantly larger in studies with this eligibility requirement (b = 0.67, 95% CI [0.21, 1.12], p = .010). Among the courts where drug offenses were required for eligibility, there was much less variability in effects and those effects were slightly higher on average (see Supplemental Material S7, available in the online version of this article). And indeed, the predicted mean effect size for courts requiring drug offenses for eligibility indicated significant beneficial JDTC effects (OR = 2.00, 95% CIOR [1.32, 3.04]) but was null among courts that did not require drug offenses for eligibility (OR = 1.03, 95% CIOR [0.82, 1.29]). Finally, we conducted a post hoc moderator analysis to examine whether the program graduation rate in a JDTC was correlated with the court’s effects on recidivism outcomes. Among the 50 study samples contributing program graduation data, there was no evidence that JDTCs varied in their effectiveness across graduation rates (b = 0.04, 95% CI [−0.33, 0.40], p = .832, see Supplemental Material S11, available in the online version of this article).
Publication Bias and Sensitivity Analyses
As shown in the Supplemental Material (available in the online version of this article), results from the planned publication bias and sensitivity analyses suggested that the findings of the meta-analysis were robust to analytic decisions. First, there was no evidence of publication or small study bias when examining the contour-enhanced funnel plots and regression tests for funnel plot asymmetry (Supplemental Materials S12 and S13, available in the online version of this article). Although there was a significant association between the general recidivism (during the program) effect sizes and their corresponding standard errors (b = −1.55, 95% CI [−2.61, −0.49], p = .010), this result did not provide evidence of small study bias. On the contrary, there were numerous small sample-size studies included in the meta-analysis reporting null or negative effects; rather, there was a noticeable absence of smaller sample-size studies that reported beneficial JDTC effects. So overall, there was no indication that the findings of the meta-analysis were upwardly biased due to publication or small study bias. Second and finally, the magnitude and statistical significance of all estimated mean effect sizes were robust across the range of model specification choices (Supplemental Materials S14, available in the online version of this article).
Discussion
This systematic review and meta-analysis synthesized findings from 55 controlled evaluation samples to examine the graduation rates achieved in JDTC programs and the effectiveness of JDTCs in reducing recidivism and drug use when compared to traditional juvenile court processing. Consistent with prior research (Latimer et al., 2006; Mitchell et al., 2012; Stein et al., 2013, 2015; Tanner-Smith et al., 2016), our findings indicated that just over one-half (55%) of youth who were enrolled in a JDTC actually completed the program. And, on average, although JDTCs yielded modest beneficial reductions in recidivism during the court supervision period, they produced minimal effects on postprogram recidivism and drug use outcomes.
This comprehensive review of the literature suggests that JDTCs, in their current and historical implementation, are unlikely to produce the beneficial effects intended under the program model (i.e., preventing future recidivism and substance use), but are also unlikely to produce significant adverse effects compared to traditional juvenile court processing. Extending prior research, we found correlational evidence that JDTC graduation rates may be higher in courts with less frequent client contact during the first month of the program as well as those that refer youth to multiple modalities of community substance use treatment. Although we found no evidence that JDTC graduation rates were predictive of program (in)effectiveness, we did find correlational evidence that JDTCs may be more effective in reducing recidivism (relative to traditional court processing) when courts require drug offenses as an eligibility criterion for participation. Beyond this, our investigation failed to find consistent evidence suggesting that JDTCs differ from traditional court processing in their ability to reduce a justice-involved youth’s odds of recidivating after receiving JDTC treatment.
Although this review represents the most up-to-date synthesis of the JDTC effectiveness literature, we identified substantial risks of bias in the included studies. As a result, the overall certainty of evidence for the meta-analysis findings was low or very low (Table 4). Namely, most included studies used quasi-experimental research designs without random assignment to conditions, and many studies suffered from high attrition and substantial non-equivalence between groups in terms of baseline risk, race, and sex. Although the research literature provided a high level of direct evidence (i.e., the studied participants, interventions, and outcome measures were aligned with those of interest in the population) and there was minimal evidence of publication bias, there was substantial heterogeneity in the meta-analyses that could not be fully explained by the measured study features. Given this, effect estimates from future evaluations of JDTCs could vary widely. These results nonetheless have several important implications for policy, practice, and research.
Summary of Findings Table for Effects on Risk of Recidivism and Drug Use
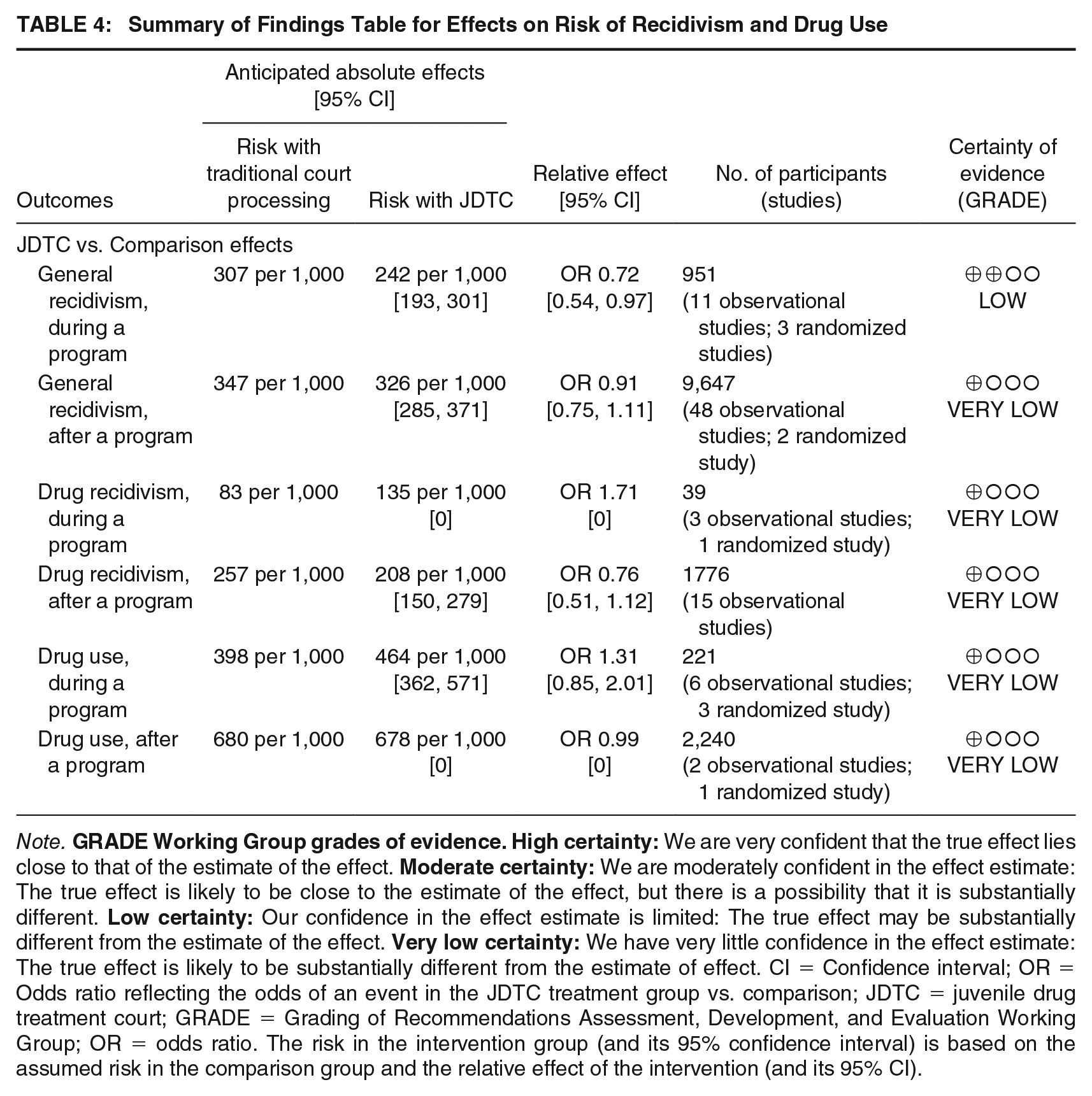
Note.
First, given the limited evidence that JDTCs yield sustained beneficial effects on youth recidivism and substance use, policymakers should be aware that the implementation of these specialized court dockets may not yield the positive outcomes desired. Although JDTCs appear effective in producing immediate, short-term reductions in youth recidivism (i.e., up to one year during which youth are enrolled in the program), there is no compelling evidence these effects will be sustained over time. This, combined with low graduation rates among JDTC participants, may suggest a general implementation failure of the JDTC program model as originally intended. Nonetheless, it is important to acknowledge that the current review did not examine the effects of JDTCs on other secondary outcomes that may be of interest, such as academic performance, school completion, quality of life, or other general well-being measures. An important direction for future research may thus be to examine whether JDTCs produce beneficial effects on other outcomes that represent the broader social functioning and well-being of justice-involved youth.
Our findings also suggest that JDTC programs may increase their program completion rates and effectiveness rates by ensuring youth are provided with appropriately tailored support and minimizing program burden on families. When youth receive services that are matched to their unique criminogenic needs, their likelihood of recidivism decreases compared to those who do not receive such services (Finseth et al., 2022). Yet, many JDTCs may be enrolling youth who do not meet diagnostic screening criteria for a substance use disorder and/or may be referring youth to inappropriate levels of care (Butts & Roman, 2004). Ideally, JDTCs would only be enrolling youth who meet some risk threshold for a substance use disorder (including, for example, whether youth were referred for a drug-related offense) and then offering individually tailored treatment plans to any youth enrolled in the program. Nevertheless, offering a greater array of services should not be equated with offering appropriate services. As treatment courts, JDTCs may more effectively reduce a youth’s likelihood of recidivating by offering need-appropriate services than they would by offering a greater number of services (Vieira et al., 2009).
This responsivity to the unique needs of each youth is believed to be a cornerstone of effective therapeutic jurisprudence (Bonta & Andrews, 2007), but may nonetheless be challenging for JDTCs operating in areas with few options for community-based substance use treatment or other mental health services (Choo et al., 2020). JDTCs operating within rural communities may shoulder a greater burden than their urban counterparts in this regard due to higher rates of substance use among rural youth (Havens et al., 2011). The likelihood that juvenile courts will refer youth to a substance use treatment provider is positively associated with the availability of such services within the community, and juvenile courts within rural communities may have less frequent contact with and access to local mental health service providers (Pullmann & Heflinger, 2009).
Furthermore, the potential benefits conferred by JDTC participation may be hampered by the intensive time commitment required of participants during the first phase of the program. In the context of adult drug treatment courts, the relationship between status hearing frequency and treatment outcomes is unclear, with some evidence suggesting that the usage of frequent status hearings may be beneficial for some individuals (Festinger et al., 2002) and other evidence suggesting that the benefits of increased status hearings fail to extend beyond drug court completion (Marlowe et al., 2005). Within JDTCs, strategic judicial supervision with frequent status hearings might instead be used in the first phase of the program to swiftly identify youth who would likely not benefit from JDTC treatment, so that they could be diverted to a more appropriate form of care. Nonstrategic judicial supervision during the first phase of the program, wherein status hearings are scheduled more frequently than what would be necessary to facilitate rehabilitation, could result in iatrogenic effects for youth and families who may be unable to meet these expectations due to other contextual factors (e.g., inflexible employment schedules, lack of transportation).
It is important to acknowledge limitations in the current systematic review and meta-analysis. First, given the number of included studies, we were unable to conduct multivariable moderator analyses to examine the potentially interacting effects of multiple moderators. Given the analytic sample size and observed heterogeneity, there was also imprecision in the estimates of the between-studies variance components in our frequentist meta-analyses. Although we attempted to address these limitations through intentional examination of theoretically informed moderators identified a priori, future evidence syntheses may consider exploring Bayesian meta-analytic approaches to attend to these issues. Another limitation is that we collected information about JDTC characteristics and practices at the study report level and did not have access to these data at the youth or community treatment program level. For instance, it is possible that a JDTC evaluation study did not explicitly report whether participating youth were referred to gender or developmentally appropriate treatment services, even if some youth were actually referred to community treatment programs that offered such services. As such, future evaluations may wish to explore these drug court practices as predictors of individual-level outcomes and provide more detailed reporting about exactly the types of community services youth are referred to as part of the JDTC program. Indeed, the (in)effectiveness of JDTCs may be driven largely by the (in)effectiveness of the community treatment agencies to which they are referring youth (Long & Sullivan, 2017), so making referrals to agencies that do not use evidence-based or appropriately tailored interventions could be a driver of null JDTC effects (Latessa et al., 2013).
Another limitation in the current review is that, given variability in program duration across courts and unclear reporting about the timing of follow-up assessments, we were unable to rigorously examine variability in JDTC effects over discrete follow-up periods. Rather, our analyses separated findings for outcomes assessed during the JDTC program period versus those assessed after the expected duration of the JDTC program. Although we attempted to address this issue in our statistical models through covariate control and sensitivity analyses, future reviews may wish to disentangle this further to better understand when and how these modest JDTC effects on recidivism may erode over time. Finally, given the inconsistent reporting of findings in the included studies, we were unable to reliably reconstruct intention-to-treat impact estimates for all analyses nor examine differences in effects for intention-to-treat versus per protocol analyses. This is another area where improved reporting quality in primary evaluations will permit more systematic meta-analytic evaluation of how JDTC program (in)completion may be driving null effects.
Despite these limitations, the current study advances the literature on JDTCs by highlighting their limited long-term effectiveness in reducing recidivism and the implementation failure of the intended model, as evidenced by poor completion rates. A promising direction for future research will be secondary data analyses from prior JDTC evaluations to further explicate the mechanisms underlying such null effects based on JDTC theories of change (for example, see Long & Sullivan, 2017). Such exploration may help identify malleable court practices and strategies that can be rigorously tested in future evaluations, including key features of the community treatment providers to which JDTCs are referring youth. Finally, if poor implementation of the intended JDTC model is hampering the program’s intended effects, the field should consider alternative therapeutic approaches for justice-involved youth affected by substance use. Given the developmental importance of social bonds and family support for justice-involved youth (Alarid et al., 2012; Gilmore et al., 2005), this might include family-engaged programs and other court-based behavioral health diversion programs designed to support youth’s well-being and healthy development.
Supplemental Material
sj-docx-1-cjb-10.1177_00938548231208208 – Supplemental material for Examining the Effects of Juvenile Drug Treatment Courts: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-cjb-10.1177_00938548231208208 for Examining the Effects of Juvenile Drug Treatment Courts: A Systematic Review and Meta-Analysis by Emily E. Tanner-Smith, Frank Mojekwu and Lauren Frankel in Criminal Justice and Behavior
Footnotes
AUTHORS’ NOTE:
This work was supported by Subcontract Number 0373700101 from the American Institutes for Research under the Prime Contract Number 2014-DC-BX-K001 from the U.S. Department of Justice. The content is solely the responsibility of the authors and does not necessarily represent the official views of the American Institutes for Research or the U.S. Department of Justice. Emily Tanner-Smith and Frank Mojekwu served as collaborators in the development and revision of the Office of Juvenile Justice and Delinquency Prevention’s Juvenile Drug Treatment Court guidelines. They have no financial interests associated with the development of these guidelines. This article does not contain any studies with human participants or animals performed by any of the authors. For this type of study informed consent is not required. Conceptualization: ETS; Data curation: ETS, LF; Formal analysis: ETS, FM; Funding acquisition: ETS; Investigation: ETS, FM, LF; Methodology: ETS; Project administration: ETS, LF; Resources: ETS, FM, LF; Supervision: ETS; Writing—original draft: ETS, FM; Writing—reviewing and editing: ETS, FM, LF.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.