
Abstract
Individuals with personality disorder are often construed as difficult to treat, and sometimes even “untreatable.” In this study, 24 men who had completed treatment on the offender personality disorder treatment pathway participated in focus groups at a high-security prison in the United Kingdom. The results of the data analysis revealed three superordinate themes that captured the impact and experience of the therapeutic process. The three themes were “A self-reconstructed,” which focused on the reconstruing and reconstructions of participants’ identity and how intervention assisted with a coherent narrative of self. The second superordinate theme, “Relational resilience and dealing with abandonment,” relates to the attachment to therapists and the negotiation of relational boundaries and resilience. The third theme, “Reimagining and re-experiencing trauma,” focuses on participants’ exploration and reliving of trauma, and how group processes allowed for shared understanding and a reconstruing of their trauma. Implications for policy and practice are discussed.
Following a series of well-publicized cases of violent and sexual violent offending, the UK government commissioned the Dangerous & Severe Personality Disorder (DSPD) pilot service in 1999, to address the “long-standing frustration within government at the refusal of psychiatrists to admit high-risk individuals with personality disorder to forensic psychiatric facilities” (Maden, 2007, p. 8; see also Joseph & Benefield, 2010; O’Loughlin, 2019; Ramsay, 2017). The aim was “to deal with the most dangerous offenders of all, those with a severe personality disorder” (Labour Party, 2001, p. 5). However, despite some success, the government decommissioned the DSPD initiative in 2011, rebadging it as the Offender Personality Disorder (OPD) pathway (NOMS, 2015; O’Loughlin, 2019). The OPD pathway aimed to provide interventions for a greater number of individuals (NOMS, 2015; O’Loughlin, 2019), incorporating lessons learnt from the DSPD pilots and guidance from the National Institute for Clinical Excellence (Cooke et al., 2017; Skett et al., 2017).
The OPD pathway is a joint approach by the then National Offender Management Service (NOMS) (now Her Majesty’s Prison and Probation Service) and National Health Service (NHS) England enterprise, with the overall aim of “improving public protection and psychological health of individuals with convictions, through developing a comprehensive and effective pathway of services for this complex and often difficult to manage population” (NOMS, 2015). This overall aim is achieved through: (1) reducing serious violent and sexual reoffending, (2) improving psychological health, wellbeing, prosocial behavior and relational outcomes, (3) improving competence, confidence and attitudes of staff, and (4) increasing efficiency, cost-effectiveness, and quality of services (NOMS, 2015). A key objective of the pathway is to “provide a consistent and cohesive process of individuals transitioning through a range of different criminal justice and perhaps forensic health interventions from custody to the community” (Cooke et al., 2017, p. 6).
While it has long been recognized that the function of prison should include rehabilitation (e.g., Blagden et al., 2016; Ginn, 2012; Smith & Schweitzer, 2012), individuals with personality disorder are often construed as difficult to treat, and sometimes even “untreatable” (Chakhssi et al., 2010). Such individuals often have complex psychological needs and are at increased risk of reoffending (NOMS, 2015). It is well established that personality disorders are prevalent among the prison population, with an estimated 60%–77% of incarcerated males meeting the criteria for personality disorder compared with 4%–11% in the general population (Bennett & Hunter, 2016; Burki, 2017; Joseph & Benefield, 2010; O’Loughlin, 2019; Singleton et al., 1998; Slade & Forrester, 2013). These figures are similar to those seen in prisons across the Western world (Puri, 2017) and globally (Fazel & Danesh, 2002).
However, labels such as “high risk” or “personality disordered” also mask the highly heterogeneous nature of these groups, who rarely fit neatly into one diagnostic category or treatment pathway (Saradjian et al., 2010). Often the individuals participating in OPD services have multiple comorbid conditions, which may include developmental trauma (MacIntosh et al., 2015), substance dependency (Sher & Trull, 2002), and mental illness (Tyrer & Simmonds, 2003). The types of psychological conditions identified among people in high-secure OPD services involve long-standing patterns of thinking, feeling, behavior, and ways of relating, that often emerge from, or are exacerbated by, adverse childhood experiences (ACES) (Saradjian et al., 2013). The presence of ACEs in individuals with personality disorder is associated with increased prevalence of several health risk behaviors, including engagement in substance use, criminal, and risky sexual behavior (Flynn et al., 2022). These conditions are typically chronic, and intractable when addressed via treatment as usual in the prison service; many people admitted to high-secure residential OPD services often have multiple experiences of “treatment failures.” Individuals with PD also have an impaired quality of life, high amounts of stress, a reduced life expectancy, and high rates of suicide (Black et al., 2007; Fok et al., 2012).
Bender, Morey, and Skodol (2011) identified that impairments in self and interpersonal functioning make up the core dimensions of personality pathology, thus a coherent narrative of the self, structured by narratives of order, is essential to the functioning of personality (Cervone & Shoda, 1999; Kroch et al., 2021). Narrative identities can be understood as “an active information-processing structure,” a cognitive schema, or a construct system that is both shaped by, and later mediates, social interaction; in other words, “people construct stories to account for what they do and why they do it” (Maruna & Copes, 2005). Positive self-identities tend to be characterized by narrative coherence, order, and the positive resolution of negative past events (Pals, 2006). Ward and Marshall (2007) suggest that the ability to recognize previous adverse experiences presents an individual with the capabilities to establish a coherent future identity. This ability can be a catalyst for positive self-transformation (Pals, 2006). However, the experience of ACEs disrupts the development of a coherent sense of identity, and can make addressing such trauma difficult for individuals to address and impair their resilience in addressing past trauma (Wong et al., 2019). Given the importance of a coherent identity in functioning personality, the treatment implemented on the OPD pathway promotes the development of a cohesive self-structure, while recognizing the disruptive impact of ACEs.
The high prevalence of people with complex mental health presentations in OPD services, coupled with higher rates of recidivism, has long been a priority for researchers, clinicians, and policymakers to understand and implement effective forensic interventions. The Fens Unit, based in HMP Whitemoor, was the first high-secure treatment unit to become part of the DSPD pathway, and later transitioned to the OPD pathway (Bennett & Hunter, 2016; Joseph & Benefield, 2010). The Fens OPD Service treatment has drawn on cognitive interpersonal theoretical frameworks (e.g., Safran & Segal, 1996; Young, 1994) since its inception in 2003. More recently, treatment has incorporated sensorimotor psychotherapy treatment principles (Fisher, 2017; Ogden & Minton, 2000; Ogden et al., 2006; Porges, 2011). Treatment is delivered by a transdisciplinary team, which combines five years of individual therapy with a range of group interventions (focused on resolving childhood histories of trauma and attachment deficit, improving affect regulation, challenging cognitions and schema, and reducing antisocial behavior while increasing connection to others and prosocial behavior). The overall aims of the program are to improve the health and wellbeing of prisoners while also reducing their risk of violent and sexually violent recidivism. Within an adult male prison population, this is achieved by addressing the consequences of adverse childhood experiences and introducing prisoners to a psychological framework to make sense of themselves and their relationship with the world, before focusing on other long-term sequelae, including addictive behaviors and offending behaviors (see Murphy & McVey, 2010; Saradjian et al., 2010). Adopting a holistic, trauma-informed approach is particularly important within treatment services that form part of the OPD, given the complexity of presentations expected within this treatment population (Skett & Lewis, 2019).
Effective treatment for PD is a priority given both the health and criminal justice complications associated with the disorder, for example, the extensive use of health care resources, a reduced life expectancy, impaired quality of life, as well as an increased risk of recidivism among offending populations (Chiesa et al., 2021; Howard et al., 2013). While effective intervention and evaluation of service are a core part of the OPD pathway strategy (NOMS, 2015), there is still no agreed-upon, benchmark treatment for high-risk men with personality disorder (Nee & Farman, 2007). Previous research, both quantitative and qualitative, of the OPD pathway has focused on adjudications and treatment (Gould et al., 2018), reductions in the risk of reoffending (Saradjian et al., 2013), and process of change (McMurran & Delight, 2017). However, no study has had a sustained focus on treatment-completers’ process through the five-year “whole” intervention and the changes that the service-users go through during this intense therapy. The current study aims to explore the lived experience of a group of adult males who completed the Fens Unit intervention, and to understand the impact of treatment on their identity, their relationships with others, to explore the environment of therapy, and the process of therapeutic intervention.
Method
Data Collection and Recruitment
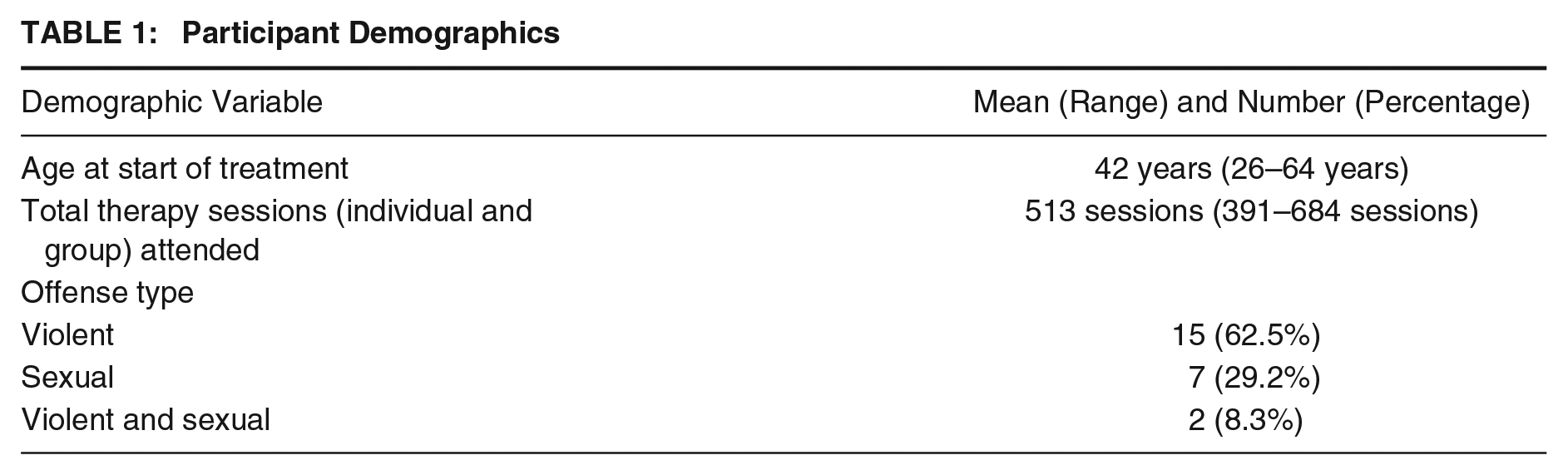
Twenty-four participants were recruited for ten focus groups, which focused on experience of treatment, the impact of treatment on the self, relationships with other patients and therapists, the environment of therapy, and whether they would change anything about the treatment. The men recruited to the study were all residing in a high-security prison in England and Wales, and had all participated in the Fens OPD pathway. A total of 24 out of 49 (approximately 50%) of eligible treatment completers agreed to take part in the research. Data for this study were collected between February 2010 and June 2020. Although this is a large time period the treatment modality, structure and intervention remained the same. As far as the authors are aware, this is one of the most comprehensive qualitative datasets for an intervention with personality disordered individuals. Table 1 provides a breakdown of the participants, including age, number of therapy sessions, and offense type. The majority of participants were convicted of either murder or rape, and both in some cases. The race and ethnicity breakdown for the sample was white British (n = 19), black British Caribbean (n = 4) and mixed Caribbean (n = 1).
Participant Demographics
Focus groups were the method of data collection and were used to explore the process, transitions, and journeys of participants who had completed treatment on the Fens OPD pathway. Focus groups are a type of group interview, which Kitzinger (1995, p. 299) claims “capitalizes on communication between research participants in order to generate data.” The interaction with group members distinguishes this method of data collection from that of one-on-one interviews (Wilkinson, 2011). Focus groups were selected as participants were used to discussing sensitive information in a group format, and because the interaction allows the participants to clarify individual opinions and to compare positions, and to explore both individual and group sense-making (Acocella, 2012). Indeed, Liamputtong (2006) suggests that focus groups can be an effective tool for exploring sensitive research topics. The group setting can encourage participants to explore issues on their own terms, to give each other support to discuss things that they may not feel comfortable discussing on a one-to-one basis. It also enabled more participants to be involved in the post-intervention interview process, as 24 interviews would have been difficult to operationalize.
Residents were approached to take part in the focus group interviews within two weeks of completing therapy. Focus groups took place in the therapy group rooms within the service. Prison operational staff were also present in line with prison and service protocols. Focus group interviews lasted on average for 66 minutes, with a range of 38–118 minutes. The only inclusion criterion for participation in the study was for the participant to have completed treatment. Treatment completion within the service during the study period was defined as finishing all group and individual therapy components throughout the five-year treatment program. In two proposed focus groups only one participant consented, and so they were conducted as semi-structured interviews instead of a group interview. However, each participant of those participants who were interview made valued contributions and so were retained for analysis. Due to the nature of the population and the fairly high attrition rate found in treatment programs with such service-users, as well as potential concerns around different individuals not associating with each other for security or personal reasons, in most cases, focus groups contained members of the same therapy group. This had the advantage of the group having established relational dynamics and group bond, which could allow for a greater depth of discussion.
Data Analytical Procedure
Data were analyzed using thematic analysis, a method for identifying, analyzing, and reporting patterns and themes within a dataset. Thematic analysis aims to capture rich detail and represent the range and diversity of experience within the data (Braun & Clarke, 2006), and has been described as a “contextualist method,” sitting between the two poles of constructionism and realism. This position thus acknowledges the ways individuals make meaning of their experience, and, in turn, the ways in which the broader social context impinges on those meanings. As such, thematic analyzes reflect “reality” (Braun & Clarke, 2006). The analysis adhered to the phases of qualitative thematic analysis as outlined by Braun and Clarke (2021), consisting of familiarization and detailed readings of the data collected, progressing to initial and systematic coding of the data, and then generating initial themes from the coded data. The final phases included reviewing themes, ensuring that they were consistent with the coding and that they were grounded in the qualitative data (Braun & Clarke, 2021; Smith, 2015). The final themes were representative of the sample. A form of intercoder agreement was used as a verification procedure to check coding of qualitative data (see de Wet & Erasmus, 2005; Miles & Huberman, 1994). In qualitative research, this occurs when two or more researchers code the same data independently and check for consistency across coders (de Wet & Erasmus, 2005). The second and third authors of this article independently analyzed transcripts, as did an independent researcher. They then shared coding and themes in data analysis sessions with all authors present, and discussed emerging themes and codes from the data, as well as both similarities and differences in data analysis. No significant differences existed between the authors; however, the authors did discuss the different interpretations of the data to come to a consensus regarding the interpretation of the data. As de Wet and Erasmus (2005) argue, this dialogical process can help to produce safeguards against bias, and in this study it assisted the researchers toward intercoder agreement. The research team comprised of clinical and research staff who did not conduct any interventions with the participants. Analysis was completed by researchers independent of the therapy team.
Ethics
This study was approved by Her Majesty’s Prison and Probation Service and a university in the Midlands of England. Participation in the research was voluntary and participants were told, both written and orally, that there were no benefits to taking part, apart from having their voice heard in the evaluation of the service. A total of 24 out of 49 (approximately 50%) of eligible treatment completers agreed to take part in the research. There were a further 101 participants who did not complete all aspects of the five-year program and so were not eligible for this research.
Results
The results of the data analysis revealed three superordinate themes that captured the impact and experience of the therapeutic process for individuals with personality disorder. The three themes were “A self-reconstructed,” which focused on the reconstruing and reconstructions of participants identity as they went through treatment. The second superordinate theme, “Relational resilience and dealing with abandonment,” relates to the attachment to therapists and the negotiation of relational boundaries and resilience. The third theme, “Reimagining and re-experiencing trauma,” focuses on participants’ exploration and reliving of trauma, and how group processes allowed for shared understanding and a reconstruing of their trauma.
Superordinate Theme 1: A Self-Reconstructed
This theme explores service-users’ reflections and reconstructions of their sense of self through therapy, while on the OPD pathway described here. Central to this theme is the process of revision in treatment completers’ self-identity.
Extract 1: Well more than words can say actually. A lot more than words can say. I think if you put your, if you put everything into it, the amount you could actually get out is endless. The people who leave here are not the people who arrived.
This extract points to the potentially powerful and meaningful individual change that service-users make during their treatment. The process, although difficult, and requiring much from the individual, facilitates a shift in their identity. Extract 1 points to the construction of a new self, which the participant is able to recognize as qualitatively different from the past self. This transition is exemplified by the statement “people who leave here are not the people who arrived.” Furthermore, this process can lead to the facilitation and enacting of new future selves (McAdams, 2011; Vaughan, 2007). This process of reconstructing one’s self-identity is developed upon in Extract 2, which describes the difficulties and ambivalences of the treatment process.
Extract 2: Hell of a lot of talking; and a hell of a lot of soul searching. . . .You have to look right inside yourself, and you don’t like what you look, what looks back . . . I avoided it for about 2 years.
Extract 2 highlights how the therapeutic journey is difficult and how change is hard for those undergoing this treatment process. It takes deep introspection, “soul searching,” and self-excavation. The extract highlights the resistance and active avoidance that can come with this process of change. Personal change, identity transformation, and assigning oneself new core roles and beliefs is not easy and such transformations can be uncomfortable and liable to cause feelings of anxiety. Research has shown that those going through identity crises, change or revision experience higher levels of anxiety (Lillevoll et al., 2013). Transformations in one’s identity require people to make substantial and, at times, global shifts in one’s self-understanding, as well as requiring significant effort in renegotiating interpersonal interactions (Veysey et al., 2011).
Extract 3: A lot of help in developing insight as to where my behavior came from, one of my plans was to completely clear out my locker of all the abuse in my life and I’ve done it, so I feel proud of myself . . . that takes a weight off my mind.
Throughout the analysis of this theme is the ability of participants to look into themselves and develop a new, more desirable self. Crucial to this identity development is the ability to look back upon past traumas, make sense of them, and begin to recognize and reconcile them. Ward and Marshall (2007) suggest that recognition of previous adverse experiences presents an individual with the capabilities to establish a coherent future identity. From this reconciliation, the individual in Extract 3 was able to gain a sense of achievement and relief. However, this process is challenging, exhausting, and likely to cause feelings of distress, ambivalence, and resistance. This process toward a new self, reconciling past traumas, can therefore be seen as part of the pains of desistance (Nugent & Schinkel, 2016). The intervention appeared to assist participants in making sense of their past experiences, coming to terms with those experiences, to allow forward movement. In this way, therapy helped move men from narratives of disorder to narratives characterized by order (Kroch et al., 2021). When traumatic experiences occur, the individual is faced with the challenge of reconstructing their identity and life story, to maintain a coherent sense of self (Crossley, 2000). In disordered narratives, individuals are experiencing “an incoherent story” or sense of self, where the self and future are seen as uncertain, and participants narrate their past experiences as disorganized and confusing (Kroch et al., 2021). The process of the ODP intervention appeared to assist participants in creating “order” narratives through helping to provide meaning to their life experiences. In Extract 4, the participant articulates how, by stripping back their traumatizing experiences, they were able to make sense of that trauma.
Extract 4: I kinda rebelled quite a bit because I felt like my life is an onion and they were stripping the layers back and each layer became more and more emotional and more and more traumatising, more and more sorta love hate relationships . . . Has it made me a better person after the five years? Absolutely. Has it given me more insight into my lifestyle and so on? Yes, absolutely, I’ve gained massive amounts from it.
The process toward self-understanding within the ODP pathway can expose the individual to trauma and psychological pain. The participant’s metaphor of the self as an onion reveals the challenges involved in the treatment process and in getting to know oneself, as “stripping the layers (of the self) back” becomes increasingly difficult and raw. The emphasis and repetition of “more” signifies the rawness and retraumatizing of therapy due to the reflection on past experiences. Resistance, avoidance, and defensiveness are thus unsurprising with this demanding therapeutic approach. Oreg (2003) has found that those who are dispositionally inclined to resist change will often be distraught by change, which will affect emotional reactions and functionality. There are links between participants’ narratives of change, the meanings they take from the process, the personal gains they make within therapy, and the narrative structure of rebirth plots. Participants appeared engaged in “rebirth” plots, whereby the individual begins in an aversive setting, and through various plot twists and turns, becomes a “new” person. This transformative episode (or rebirth) has been found to occur during and after traumatic events (including dealing with trauma through therapy) and is related to identity transitions (Robinson & Smith, 2009). This appeared as part of a process that allowed for individuals to create narratives of order and make sense of their experiences (Kroch et al., 2021).
Embracing, being ready for, or feeling worthy of change was a strong theme within the participants’ data. This was a hurdle that many of the men in this sample had to overcome to experience the benefits of treatment.
Extract 5: I had some hard times, erm, some truly difficult times and, and most of that difficulty I experienced was due to my resistance, you know, within therapy . . . once I started to, erm, focus on what needs to focus on myself . . . why I was here, why any of us are here . . . things became more easy. Extract 6: You have your ups and y’downs. And that’s all about change because we don’t, most of us, initially, don’t wanna change . . . that’s the hardest thing it’s like anything in life but once you start making them steps, you see the benefits. Extract 7: [didn’t feel worthy of therapy] You gotta have self worth though, and the self worth should override the self pity within what you do and how you look at the things you’ve seen.
Extract 5 epitomizes the difficulties participants faced throughout their treatment journey, including overcoming resistance and being ready for change. Indeed, initially, many of the men did not want to change, or struggled to accept change. There was a theme of low self-worth and not being worthy of treatment, which appeared related to resistance to change. Not feeling worthy or good enough for change can be a critical factor in resistance. This “worthiness” is linked to self-integrity, an individual’s sense of being “good enough”—competent enough to control important life outcomes (Steele, 1988). Threats to self-integrity, where an experience threatens one’s personal adequacy, are barriers to change for many behaviors (see e.g., Logel et al., 2019). It was clear that this was a ubiquitous experience for this sample and that going through this process was a necessary step in self-change.
Superordinate Theme 2: Relational Resilience and Dealing With Abandonment
This theme relates to the mirroring of abandonment that the participants experienced during early life experiences and through previous therapeutic relationships during interventions on the OPD pathway. It also details how participants negotiated feelings of abandonment, and how positive therapeutic relationships led to relational growth and resilience. It is important to note that secure childhood attachments are almost non-existent among prisoners with personality disorder (Frodi et al., 2001). Many of the participants expressed that their first significant bond was with a therapist, which may have intensified their negative emotional reactions if, for example, their therapist left during therapy.
Extract 8: No the nightmare was even worse because I, I would see my mother there and I was, I was rebelling against my mother in a way, with my therapist. Extract 9: I started off with XXX [therapist name], which was more like a dad and I warmed to him . . . I built up trust with XXX and we were getting somewhere and all of a sudden it was like out of the blue, well I’m going.
For many participants, their therapist(s) appeared to have become a surrogate attachment figure, as Extracts 8 and 9 highlight, as both compare their therapists with a parental figure. It is interesting to note the differences in how both extracts view this reflection; Extract 8 states he rebelled against his therapist, which reflected him rebelling against his mother, whereas in Extract 9, the relationship evoked feelings of warmth. Transference of this kind is common within therapy with those with personality disorders, and it is important that the therapist remains alliance-focused, as relational transactions, such as those described in Extracts 8 and 9, have the potential to rupture therapeutic relationships (Høglend, 2014). The ways patients interact with their therapists can provide important data about their personality, and interpersonal functioning (Bradley et al., 2005). However, forming and maintaining suitable bonds with their therapists can be relationally demanding, and the consequences of how such relationships are ended can have consequences for further therapeutic work. Extract 9, for example, highlights how the participant had built trust with his therapist, only for the therapeutic relationship to be suddenly ended. As suggested by Frodi et al. (2001), a therapist working with a prisoner who has a personality disorder should work with that individual for an extended period of time. This allows the therapist to act as a secure base for him to explore the different types of relationships he has experienced thus far and help to facilitate future relationships. While that was the expectation for therapists on the pathway, inevitably participants would experience the loss of a therapist.
Extract 10: It was just the same with [therapist 1], and even [therapist 2] . . . and it was like . . . who am I going to have next? Am I going to be able to trust them? Is he going to stay till the end? . . . I find it difficult to really put your trust in, most of my life has just been superficial.
Extract 10 portrays the magnified impact therapist change can have with this group, the impact it has on patients’ ability to form trusting relationships, and how therapist attrition can contribute to the cycle of abandonment that the patients may go through due to repeated staff changes. The low level of trust in others, specifically mental health professionals, is common among prisoners with personality disorders (Sheldon et al., 2010). This extract portrays the almost automatic distrust patients can have in others, due to their past aversive experiences. Therefore, patients are encouraged to establish trust in their therapists (Frank, 2004), which is made difficult if they feel that they are being repeatedly abandoned. This emphasizes the delicate relational balance within therapy with those with severe personality disorder, and how changes in therapists can cause lasting ruptures and delays in their treatment journey, if not properly managed.
Extract 11: If these staffing changes are going to continue happening then what’s the point? Because we’re building relationships with these people then if they move on just like that, then what’s the point? So, it was times like that with, with staff that we really, kinda, struggle within therapy. With, do I carry on? Do I just not commit as much? Do I not try and build relationships while I’m doing this therapy?
The transference from previously abandoned and damaged relationships impacts on patients’ therapeutic journeys, and there were repeated themes of the impact of therapist changes within the data. Extract 11 demonstrates how this has caused feelings of hopelessness, as this participant repeatedly asks “what’s the point?” He states that the constant building and breaking of relationships caused him to struggle in therapy, which made him question whether he should continue. This shows the lack of hope he had for completing treatment, as each time a therapist left, he perceived that he would have to start from the beginning again. A key element of hope, as described by Burnett and Maruna (2004), is the perceived ability to achieve a certain outcome. For some participants, the repeated breaking of relationships with therapists, may make patients feel that they are not able to complete treatment successfully, and therefore that it is hopeless to try. Hope is a crucial aspect of recovery, allowing prisoners to construct future-orientated, possible selves as a method of moving away from a life of crime (Perrin et al., 2018). However, staff changes on the unit were interpreted by one patient as a positive thing, as indicated in the following extract.
Extract 12: I think changes in staff takes you out of your comfort zone and that can make you a stronger person. Um, and its just made me a stronger person in the sense of because when I had, um, conflicts of interest it was knowing they were to do with myself rather than the other person.
In contrast to the other participants, Extract 12 shows an alternative view on staff changes in the unit; he construed it as a positive challenge, which takes him out of his comfort zone and leads to better outcomes. He also states that he benefited from having the input of more than one therapist, as he then had a better understanding of any disputes they might have had. This extract has an overall sense of positivity, and an ability to recognize that conflicts toward therapist change reflected their own self-conflict. However, this reflection was not shared by the majority of participants, suggesting that maintaining secure therapeutic relationships remains an important factor in treatment.
Extract 13: I think, those relationships initially were what helped me move forward, you see, and every one-to-one was a different kind of experience because they took me to a different place.
Crucial to Extract 13 is the individual’s recognition of the importance of a therapeutic alliance and one-to-one treatment sessions when progressing through the OPD pathway. This individual highlights the plasticity of the individual treatment sessions and how this developed self-reflection and contributed to self-change. The content of the treatment, alongside a positive therapeutic alliance, was the initial step in participants’ journey in self-change.
Extract 14: You can actually trust being in emotional relationships and actually that you are worthy of relationships and it feels like these are the longest relationships you’ve had that are consistent and safe.
Similarly to Extract 13, the significance of a therapeutic alliance is evident in Extract 14. However, this individual focuses on how this relationship is internalized and understood according to past experiences. Gunderson et al. (1997) explained that an adverse and inconsistent therapeutic relationship has the capacity to reignite elements of abandonment and loss previously experienced. However, for many participants, the contrast between the therapeutic relationship and previous relationships was apparent, as they recognized that their long-term interpersonal relationship with the therapist was important for their growth. For many, this was their first experience of a consistent and safe relationship. The experience of safe relationships can enable “headspace” for men to focus on the future (Blagden et al., 2016, 2017; Mann et al., 2019). As such, forging strong and meaningful therapeutic relationships is an integral part of the change process (Duncan et al., 2022; Ross et al., 2008), and Dahle (1997) reported that a key predictor of treatment readiness is client trust in the treatment provider. Trust can be developed by establishing a therapeutic relationship based on honesty (Drapeau, 2005) and mutual disclosure (Marshall et al., 2003). Constructive relationships with criminal justice professionals are also important in the desistance process in that establishing social relationships is seen as vital to the triggering, enabling, and sustaining of change (Weaver & McNeill, 2015).
Superordinate Theme 3: Reimagining and Re-experiencing Trauma
Participants’ experiences/re-experiences of trauma have been touched upon so far within this analysis, but the experience of re-trauma through the therapeutic process and gaining new understanding and meanings from shared experiences was a salient theme within the data. In addition, some men in this sample found that they were able to connect as a group and better support each other through shared trauma.
Extract 15: The abuse thing is what brought us all together and probably, if, uh, we didn’t have that bond we, I don’t know what we would have bonded over. Extract 16: That small group was the most I have ever been open and honest with anyone in my, my entire life, and the longest I’ve ever spent within a group of people.
Extract 15 highlights how participants bonded over shared disclosures and experiences of childhood trauma. The “abuse thing” is the fundamental relational shared aspect of patients’ experience within the treatment group. Extract 16 further exemplifies the solidarity from these shared experiences. Interestingly, Extract 16 also points to the openness and honesty that occurs within the treatment groups, which had important relational ramifications and allowed for growth and shared understanding. Disclosing trauma and the experience of vicarious exposure to trauma can lead to growth, particularly when the experiences are perceived as authentic. The honesty and authenticity can allow for relational connectedness, and contribute to therapeutic integrity (McCormack & Adams, 2016). Furthermore, it appeared that sharing these experiences together helped participants to cocreate narratives of order and gain new understandings of their past traumas. Hearing others’ authentic responses and bearing witness to the individual’s traumatic experiences, and in particular hearing how the telling of their story has resonated with and affected others, can have a powerful impact for survivors of trauma (see Carey & Russell, 2003). This is vitally important as childhood trauma is linked to social dysfunction in adulthood, which makes the formation of bonds with others difficult.
While honesty of shared trauma appeared to bond individuals relationally, this was not uniform. Participants in group treatments also discussed how being “honest” about some aspects of their offense histories appeared to worsen the symptoms of trauma, as highlighted in the following extracts.
Extract 17: I’ve got childhood issues to, to comprehend with. I don’t wanna be hearing about other people’s sex offenses, in detail, which is what’s been happening on [sic] group nine. Cause sometimes you think, it’s quite hard, and, difficult to hear and, to cope with afterwards. Extract 18: I found it, er, extremely difficult on groups, listening to people talking about their crimes, especially where children were concerned. I had, ere, had nightmares. I, er, used to ruminate, er, er, memory flashbacks of my sister being beaten up . . . It brought a lot of misery back to me, hearing other people’s misery.
Extracts 17 and 18 focus on the difficulties that participants’ faced during group therapy when dealing with both their own childhood trauma, and the details of others’ crimes against children. Both extracts imply that outside of the treatment room, they ruminated over disclosures made within therapy, which negatively impacted them. These extracts further highlight the level of intensity this model of treatment can have on participants. This experience of secondary trauma can cause severe psychological and physical effects (Catanese, 2010).
Discussion
The aim of the current study is to explore the lived experience of a group of adult males who completed the Fens Unit OPD pathway, and to understand the impact of treatment on their identity, their relationships with others, to explore the environment of therapy and the process of the therapeutic intervention. The analysis revealed the complexity, relational challenges, and shifts in identity that participants make through therapy on the ODP pathway. The theme “A self-Reconstructed” revealed how participants’ identity and life biographies were reimagined and how the self changed through the treatment process. Participants were clear that this process was difficult and led to resistance in therapy. Indeed, transformations in one’s identity requires people to make substantial and, at times, global shifts in one’s self-understanding, as well as requiring significant effort in renegotiating interpersonal interactions (Veysey et al., 2011). In some senses, the ODP treatment process helped participants make sense of their life experiences by helping them move from fragmented, confused, and disordered narratives to ones characterized by narratives of order (Kroch et al., 2021). When traumatic life events occur, the individual is faced with the challenge of reconstructing their identity and life story, to maintain a coherent sense of self (Crossley, 2000). Participants discussed how therapy enabled individuals, and the group, to gain new insights into their traumatic experiences, to face them, and to move toward more positive selves. Narratives of coherence and a coherent narrative identity are thus crucially important in personality functioning (Cervone & Shoda, 1999; Pals, 2006). Participants articulated how the therapeutic process, although difficult and challenging, allowed for self-reconstruction and ultimately for more coherent narrative identities (Ward & Marshall, 2007). This is important for rehabilitative purposes and desistance from crime as individuals tend to act in accordance with the stories that they present about themselves (Maruna, 2001; McAdams, 1985). Moreover, an adaptive new narrative identity, which may provide coherence to their life story and sense of self, can help guide future behavior to align with such a narrative (Petrich, 2016).
The process of narrative and identity change for this group is especially challenging, and the theme “Relational Resilience and Dealing with Abandonment” demonstrated the important impact that therapeutic staff have on this process. Such relationships required considerable skill to balance safe and secure relationships without creating a sense of dependency. It was also apparent that previous attachments caused difficulties in forming a therapeutic alliance for some, as the therapist represented a previous figure in the participants’ personal life. While most negotiated this relational boundary, it did obstruct treatment gains. Most participants pointed to positive therapeutic relationships, characterized by trust and honesty, and these were often the first time the participants had experienced such relationships. Forging strong and meaningful therapeutic relationships is an integral part of the change process (Duncan et al., 2022; Ross et al., 2008), and Dahle (1997) reported that a key predictor of treatment readiness is client trust in the treatment provider.
The final theme considered Reimagining and Re-experiencing Trauma. There were two aspects to this theme; the first was about gaining new constructions and insights into their own abuse histories. This process was facilitated by the presence of other group members sharing their experiences, and this allowed for shared “narratives of order” of their experiences. This was an important aspect of the therapeutic process and allowed participants to gain new insights into the self (Whiting, 2008). As Yalom (1995) argues, individuals derive a sense of universality from their interpersonal therapeutic relationships, which, in turn, encourage motivation for self-discovery and identity change. The second aspect of this theme was how some participants re-experienced their trauma through the group process. This re-experiencing caused further psychological distress, at a time where participants were already trying to come to terms with their own traumas. However, both appear important for the process of change, as the suffering that came from such re-experiencing led to new understandings. Such processes have been linked to growth and human flourishing (Hall et al., 2010). The experience of trauma and reliving it through therapy was seemingly unavoidable and the trauma histories of the men and their experiences of ACES were high. It was thus crucially important that the ODP intervention spent nearly three years working on the individual’s trauma. Indeed, the acknowledgment in therapy that hurt people hurt people was an important aspect of their reconstruing of their trauma histories (Taylor et al., 2020). As Creeden (2004) argues, not addressing the impact of trauma will impede the learning and effective use of skills that are taught in treatment programs, as well as others who argue that it is a necessary condition of treatment for such client groups (Taylor et al., 2020)
Limitations
There are several limitations to this study, despite the robustness of the data collected. It must be noted that the data here represent one unit (the Fens) delivering the five-year “offender personality disorder pathway” and as such experiences may differ from those in other establishments. Furthermore, this research explores the experiences of individuals who completed therapy, thus those who had either dropped out before treatment completion or who were not interested in participating in the study, were not captured, potentially excluding conflicting accounts. The use of focus groups can also be problematic as some participants may dominate, withdraw, or struggle to disagree with ideas shared and endorsed in the group, although all groups were facilitated by experienced researchers/psychologists in an attempt to mitigate this and allow for equal participation. Finally, participant responses may have been influenced by external factors such as presence of operational staff in the room, feeling unable to discuss aspects of treatment, or concerns about disclosing information in the group. However, one of the primary reasons for focus groups was to ease the pressure sometimes experienced in one-to-one interviews and allow for group discussion, allowing the group to give each other support to discuss things that they may not feel comfortable discussing on a one-to-one basis (Liamputtong, 2006).
Conclusion
The current research provides a unique insight into the challenges, progression, and self-change in men with PD on the Fens OPD pathway. This is the first qualitative study to explicitly focus on the experience of this intense five-year therapeutic intervention. This research highlighted that crucial to an individual’s progression through treatment intervention was the ability to reflect upon their sense of self and past experiences, to shift narratives from disorder to order and gain new understanding of self and their trauma from therapeutic and other group member relationships. This article contributes to the evidence for the OPD pathway and provides a platform for further research into specific elements of the pathway that facilitate treatment progression of personality disordered people with convictions.
Footnotes
Authors’ Note:
We have no conflicts of interest to disclose.