
Abstract
Despite the increasing mental health needs of Asian Americans, service utilization remains notably low. This article contends that ethnoreligious identities may contribute to this issue. A community case study highlights primarily Korean and Chinese American Christian therapists and clergy who convened in response to rising mental health demands in their Chicago community. They acknowledged the necessity of addressing clients’ ethnic and religious identities to provide effective care. The article details the successful strategies employed by these professionals, demonstrating their alignment with the collaborative practice model (CPM). A fictional client case study then shows how this community could have coordinated care effectively. The discussion addresses additional factors beyond the CPM that enhanced collaboration, potential challenges, and broader implications for other regional areas, underscoring the importance of integrating cultural and religious considerations in mental health services.
Keywords
Ethnoreligious Identities Potentially Impacting Asian Americans’ Access to Mental Health Services
The Asian American community is growing at a fast pace, and their mental health needs are also on the rise. Between 2000 and 2019, this population expanded by 88%, and by 2060, this demographic is expected to quadruple (Pew Research Center, 2021). A highly unrecognized fact is that the prevalence of mental illness is just as high among Asian Americans as it is among White Americans (Lee et al., 2000). Despite this, Asian Americans continued to use mental health services at a lower rate (5.8%) than White Americans (19%; Yang et al., 2020) and at less than half the rate of other minorities (Cook et al., 2017). Efforts made to address cultural barriers specific to Asian Americans—such as stigma, suppression of emotions, and confidentiality (Leong & Lau, 2001)—continued, but disparities in utilization rates continue to persist (Yang et al., 2020).
Mental health services may be underutilized due to mental health professionals’ limited understanding of the intersectionality of cultural and religious identities among Asian American immigrants. When Asian families immigrated to the United States, many sought religious communities for cultural support, psychological gains, and access to resources (Hirschman, 2004; Yosso, 2005). As many as 67% of Asian Americans have been affiliated with an organized religion, with Christianity as the largest group (34%), Buddhism second (11%), and Hinduism third (11%; Pew Research Center, 2023). These microcosms provided refuge and the ability to navigate disparities between their native culture and the new overarching culture. Often, these spaces allowed for a collectivistic approach—through dialogue, collaboration, and consensus agreements—in determining how to assimilate into the broader culture.
As a result, many Asian Americans have developed identities that blend their religious beliefs with cultural values, forming what is known as an ethnoreligious identity (Karpov et al., 2012; Park et al., 2013). This blending may shed light on the hesitation some Asian American clients have felt when it comes to seeking mental health services. They may have perceived a gap between their ethnoreligious identities and what the psychological community offers, leading to the belief that these services have not adequately addressed their mental health challenges, especially in relation to their cultural and faith-based backgrounds. To provide effective and culturally sensitive treatment for Asian Americans, it may be crucial to cultivate a collaborative partnership between clergy members and professional clinicians, focusing on integrating the diverse aspects of Asian Americans’ ethnoreligious identities into their therapeutic practices.
Collaborative Practice Model: Framework to Enhance Effectiveness of Integrated Care
Evidence supporting relational and collaborative practices in clinical integration, in contrast to structural, functional, or manual-focused approaches, remains limited; however, existing studies have indicated promising results. Prior research has shown that treatment methodologies and clinical integration practices that have emphasized relationships among key stakeholders have been positively correlated with performance outcomes and provider experiences (Song et al., 2017).
Ness and colleagues (2014) have developed a framework that incorporates structural and process-oriented elements, the collaborative practice model (CPM; Figure 1). This model was designed for communities with multiple stakeholders, making it advantageous for professionals from various disciplines and clients with complex cultural identities. CPM consists of four key components, including (a) a framework for service orientation that is person-centered and recovery-oriented; (b) two collaborative structures, namely collaboration within service processes and system-oriented collaboration; (c) principles of collaboration, which include self-understanding, mutual understanding, and shared decision-making; and (d) processes of collaborative practice characterized by open dialogue and participatory engagement (Ness et al., 2014).
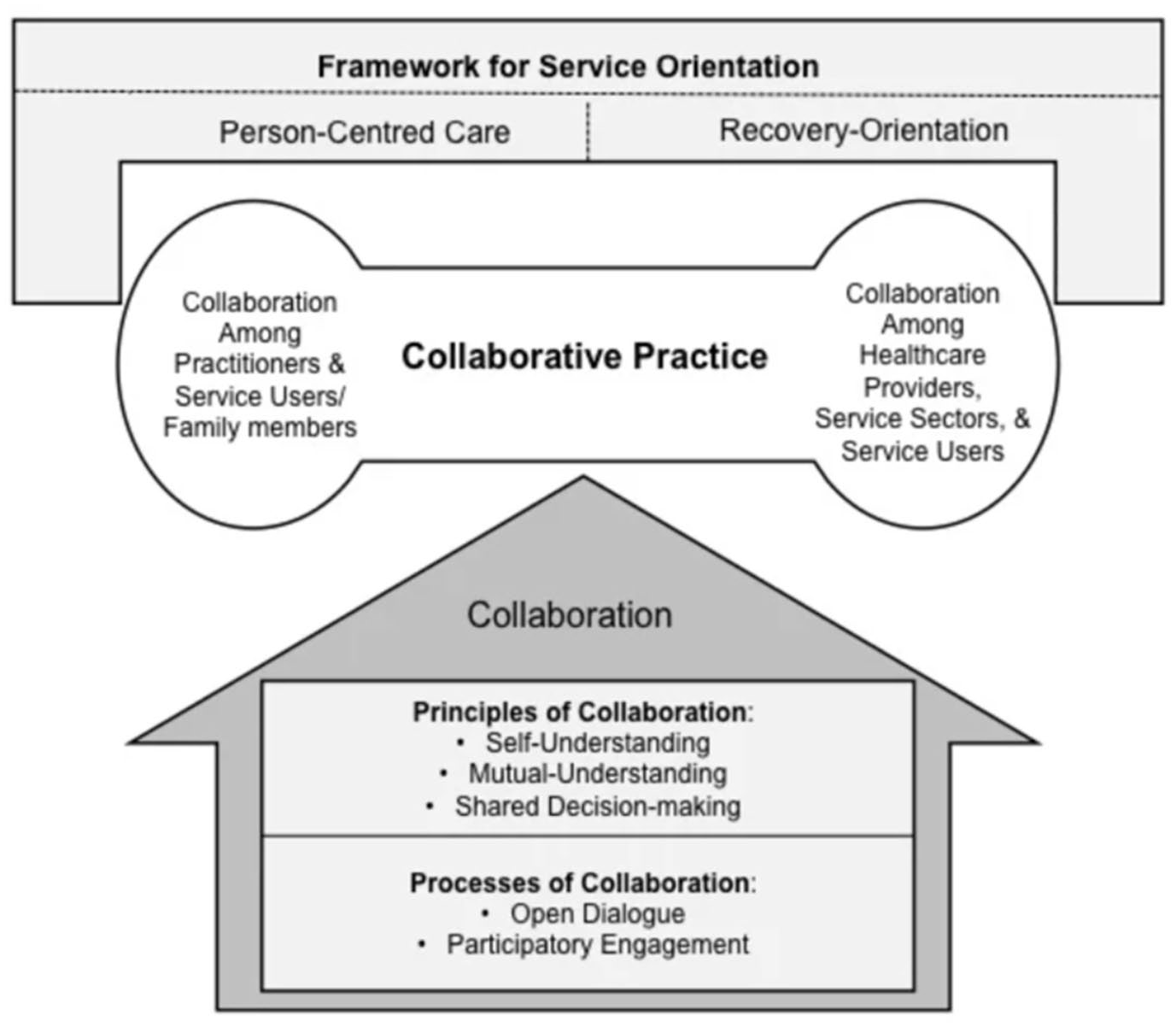
Collaborative practice model.
The first component of the CPM is grounded in theoretical principles emphasizing person-centered practices and a recovery-oriented approach. Person-centered practices view clients and their families as essential partners in identifying needs, especially in planning, development, and decision-making in mental health care. The recovery-oriented approach includes two key processes: an individual process focusing on identity and self-perception and a social process acknowledging the importance of contextual factors and relationships in recovery. This dual emphasis enables a strong focus on addressing clients’ needs while fostering collaboration with the client’s community (Ness et al., 2014).
The second component features a dual structure comprising two key areas: collaboration within service processes and collaboration within the health care system. Collaboration within service processes emphasizes building relationships between clients and clinicians to achieve optimal clinical outcomes. Conversely, collaboration within the health care system integrates various client-accessible services to enhance outcomes through effective service coordination. These areas are intrinsically linked, working together to yield the most favorable results for clients (Ness et al., 2014).
The third component of the model highlights three foundational principles of collaboration: (a) self-understanding, (b) mutual understanding, and (c) shared decision-making. Self-understanding encourages professionals to become aware of their perspectives, beliefs, motivations, and biases, laying essential groundwork for collaborating with diverse viewpoints. Next is mutual understanding, which fosters relationships among stakeholders, enabling them to address misunderstandings and dismantle existing dynamics of domination and oppression (Ness et al., 2014). This concept could also be referred to as “equal footing” (London et al., 2009, p. 1), implying that all participants’ viewpoints are significant and valuable. Such interactions have facilitated the examination of differing perspectives, beliefs associated with healing, and various interpretations of truth and correctness (Ness et al., 2014). The final principle, shared decision-making, is a process whereby participants exhibit mutually negotiated dialogues (Strong et al., 2011). This allows for shared responsibilities and coordinated care. This overall process has facilitated a unified approach toward common goals, ensuring that participants in the cooperative treatment process are aligned and committed to the shared objectives (Ness et al., 2014).
The final element is collaboration, which rests on open dialogue and participatory engagement. Open dialogue encourages unrestricted discussions on meanings and interpretations, leading to shared understandings related to conceptualization, assessments, and treatment recommendations. A recurring theme is the appreciation of uncertainty, allowing stakeholders to present differing perspectives without fear. This openness promotes participatory engagement, enabling participants to contribute their unique expertise with fewer constraints. Thus, the quality of the group’s collaboration and interactions significantly influences the outcomes generated (Ness et al., 2014).
Community Case of Korean and Chinese American Clergy and Therapists in Chicago: Highlighting Key Elements of CPM
In this article, we 1 provide details on the grassroots efforts of Korean and Chinese American (KCA) clergy and therapists in the Chicago area and the collaborative approach they undertook to provide culturally sensitive mental health care for their clients. This case commences with an overview of a Korean American (KA) therapist and clergy who noticed the escalating mental health challenges in their Asian American 2 Christian community and how ethnoreligious identities were intertwined with mental health symptoms. Both individuals sought the assistance of clergy and counselors within their professional networks, which were primarily comprised of Protestant and non-denominational Christians of Korean and Chinese descent. Following this initial collaboration, the article delineates how a broader cohort of KCA clergy and therapists convened to address the mental health needs of KCA Christian clients in the Chicago area, culminating in establishing the Pastors and Counselors Together (PACT) initiative. Furthermore, this article illustrates the alignment of collaborative processes among KCA clergy and therapists with the principles outlined in the CPM (Ness et al., 2014). A fictional case study will subsequently demonstrate the dynamics of shared decision-making and coordinated care established through this collaborative framework.
The KA therapist
Irene Cho is a second-generation KA Christian woman who has a private practice in Chicago and 30 years of clinical experience. Cho identifies as a Christian and was raised in a Korean Presbyterian church. She valued her upbringing within this community, as it provided her with a sense of belonging among like-minded peers; however, she felt that her religious experience emphasized legalistic rules and outward performance. She attended Wheaton College’s master’s-level clinical psychology program, which emphasized the integration of Christian faith and psychotherapy. Having worked with many Asian Americans, Cho has adopted the view that Asian Americans tend to intellectualize their situations and affective experiences. As such, Cho desires to counterbalance this tendency in her clinical work and has become partial to attachment-focused, psychodynamic approaches that aim to cultivate emotional experiences for the client within the context of a secure and safe relationship.
The KA clergy
David Lee is the founding and lead pastor of Harvest Community Church (HCC), an Asian American church in the Chicago area that is part of an independent evangelical network of churches. Lee has served as the head clergy member of HCC since it was established in 1995 by a first-generation Korean immigrant congregation. The first-generation Korean church had provided modest funding with the intention of allowing HCC to operate as an independent entity, which enabled Lee to establish a culture and set of values that were independent of the first-generation church. Lee has acknowledged that this independence has allowed him to openly address the mental health needs of the growing second-generation Asian American congregation.
Lee, a KA Christian, immigrated to the United States with his family at the age of five. During his early years, he attended a first-generation Korean church, but his parents became disillusioned with certain aspects of this community and began attending a predominantly White church when Lee started middle school. By immersing himself in a culturally different Christian community, Lee was able to parse the differences between his ethnic and religious identities. This helped Lee form a conceptualization of spiritual development that was not entirely infused with his racial-ethnic values, influencing his present approach to pastoral care.
Lee completed his Master of Divinity degree at Biblical Theological Seminary in 1995, focusing on missions and evangelism. During his coursework, Lee reported taking a substantial number of classes in biblical languages, including Hebrew and Greek, which helped him feel prepared to guide congregants through matters requiring spiritual and religious perspectives. However, Lee also acknowledges that he completed only one course in pastoral counseling, which at times, has left him feeling less prepared to counsel his congregants. Lee has shared that additional training would have been beneficial given that many members of his congregation turned to him for help with their inner struggles.
Rise of mental health issues among Asian American Christians in Chicago
In recent years, Lee observed that congregants began to share increasingly profound and more serious concerns with their religious leaders. The heightened awareness of mental health within the United States positively influenced the Asian American community’s interest in mental health resources. Lee observed a notable increase in congregants actively seeking counseling from their religious leaders for exacerbated struggles. He noted that an increasing number of members approached him with identifiable mental health symptoms.
This shift led Lee to feel inadequately equipped to address the growing complexity of these mental health issues. He began realizing that relying solely on theological explanations and teachings was becoming inadequate in addressing the mental health needs of his community. Given that Lee’s knowledge and training centered more on theological perspectives and interpretations of the Bible, he felt that he did not have the expertise to distinguish between clinical issues that required mental health interventions or personal matters that pastors could address from a spiritual perspective. The absence of clear boundaries frequently led to counseling engagements in which Lee perceived a necessity for more defined expectations regarding the use of his time and capabilities. He often experienced feelings of being overwhelmed, isolated, and burnt out. Consequently, Lee began to question whether he had received sufficient training to support his congregants effectively through their mental health challenges. This realization motivated him to seek more sustainable solutions.
Simultaneously, in 2015, Cho also began treating an influx of KA Christian clients who were struggling with understanding their faith within the context of their mental health challenges. Many were educated, second-generation KA professionals or stay-at-home mothers who grew up in first-generation Korean Christian churches. Most were unfamiliar with their emotional world and presented with a variety of symptoms, including anhedonia, addictions, anxiety, inability to set personal boundaries, low sense of self-worth, or feelings of worthlessness/inadequacy.
Mental health struggles interwoven with ethnoreligious beliefs: Highlighting need for “individual process” of CPM
During her practice, Cho noticed recurring patterns among her KA clients. Their clinical issues often seemed closely tied to their ethnoreligious beliefs, affecting their responses to therapy. For instance, many of her clients struggled to manage their emotions and meet their religious community expectations. In many Eastern cultures, showing strong emotional reactions can be seen as a source of shame for both individuals and their families. When Christian teachings—such as the virtues of love, patience, self-control, gentleness, and kindness highlighted in Galatians 5:22–23—were woven into this cultural norm, the pressure to suppress emotions intensified, often worsening their mental health symptoms.
Cho also observed that her KA Christian clients struggled to balance ethnoreligious values with self-care practices. The Korean culture has emphasized prioritizing the group over individual desires, which has often merged with Christian teachings, such as Philippians 2:3–5, which states to “in humility value others above yourself” (The Holy Bible, New International Version, 1978/2011). Some KA clients have interpreted this as a guideline that labels self-care as selfish and setting personal boundaries as unloving. This ethnoreligious focus on sacrifice and service frequently overshadowed individual well-being, complicating the process of psychotherapeutic treatment.
Many KA Christian clients also exhibited mental health symptoms that were intertwined with their perception of God and their view of self within the context of this spiritual relationship. Within the framework of their faith community, many KA Christian clients have cultivated internalized beliefs regarding the characteristics of a “good Christian.” These beliefs often encompassed a distinct set of behaviors that aligned with religious and cultural expectations prevalent within their community. For instance, some of these behaviors could have included actively engaging in volunteer work at the church or being elected to hold leadership positions. In addition, these beliefs were intertwined with the perception of having received a particular array of “blessings” from God. Such blessings might manifest in experiences like achieving favorable outcomes at work that contribute to a financially successful career, narrowly escaping a tragic situation as a result of divine intervention, or securing a fortuitous marriage with a partner of good standing. Individuals who had lives that did not exhibit these characteristics began questioning why prayer did not “work” for them, viewing their faith as not being “strong enough.” Many would experience a crisis of faith as they began to perceive a diminished sense of God’s love and providence in their lives, resulting in these clients viewing themselves as “not worthy.”
These clinical cases have illustrated how the ethnoreligious beliefs of KA clients were intertwined with their internal self-perceptions. This association has underscored the need to address the client’s internal thoughts, beliefs, and emotional frameworks. Accordingly, a core principle of CPM’s recovery-orientation is that healing must entail an “individual process” (Ness et al., 2014). This underscores the importance of encouraging KA Christian clients to actively participate in their recovery journey as independent individuals, whereby they take the time to understand how their worldviews have shaped their thoughts and emotional experiences. This may include countering the perception that they were unlovable in the eyes of God or allowing themselves to experience and express previously repressed emotions.
Mental health struggles interwoven with commitment to ethnoreligious community: Highlighting need for “social process” of CPM
Cho also began noticing that many of her KA Christian clients had difficulty receiving treatment because of their commitment to their ethnoreligious communities, specifically around the expectations for obedience and behavioral conformity. As mentioned earlier, managing one’s emotions was considered an important norm for KA Christians. These societal and religious expectations led to the development of a performance-oriented identity, wherein individuals not only suppressed their emotions but also received praise when they demonstrated “deference” and “resilience” in the face of adversity. During treatment, many clients expressed the challenges of projecting an inauthentic facade of well-being. They described this as a strenuous effort that often resulted in symptoms remaining concealed as clients grappled with feelings of shame and humiliation, ultimately delaying access to mental health services.
In addition, many KA Christian clients grappled with an internal conflict in determining the “correct” course of behavioral action, as relying on their intuition and feelings were perceived as unfamiliar and risky. This struggle manifested in various forms, such as grappling with the guilt of spending money on personal needs, acknowledging both sexual and nonsexual desires, and asserting oneself in relationships. This became especially apparent for KA Christian women who were victims of intimate partner violence, which was a reported issue. At times, they felt pressured to conform to submissive roles due to the patriarchal framework inherent in both their family and church. Many expressed feelings of inadequacy for being unable to “save” their relationships, along with shame, self-doubt, and feelings of “selfishness” when they considered leaving their violent partners. Throughout treatment, clients heard internal voices urging them toward safety and healing but had trouble trusting these desires. The louder voices from authority figures and community expectations often overshadowed their inner guidance, leading to confusion.
To ensure adequate progress in treatment for these KA Christian clients, Cho recognized the importance of collaborating with members of her clients’ community. Cho’s insight also aligns with CPM’s principles of person-centered care and the “social process” of recovery-orientation (Ness et al., 2014), which emphasizes the necessity of a strong alliance among all parties involved (McCance et al., 2011; McCormack & McCance, 2006), and that stakeholders consider contextual factors essential for the recovery (Ness et al., 2014). This necessitates the establishment of mutual trust, respect, understanding, and agreement among the KA Christian clients, their families, KA clergy, and KA therapists. Furthermore, it is essential for each stakeholder to recognize the client’s sense of belonging within their ethnoreligious communities, as well as their successful reintegration into these communities upon the conclusion of treatment.
Enhancing collaboration between clergy and clinicians: CPM’s “focus on service-user recovery”
Recognizing how mental health symptoms and resistances to treatment were woven into the KA Christian client’s ethnoreligious beliefs and dedication to their communities, Cho began realizing the importance of collaborating with her clients’ ethnoreligious leaders. Early in treatment, it became evident to Cho that an in-depth conversation about the client’s beliefs, faith, and culture was necessary. However, clients frequently felt that they could not alter their thought patterns without receiving approval from a religious or ethnic authority figure. Exploring alternative perspectives without approval evoked uncertainty, fear, and anxiety. This yearning for validation surfaced in significant life decisions, such as divorce, as well as in minor intrapsychic struggles, such as permitting oneself to experience pleasure or acknowledge one’s feelings, such as depression.
Meanwhile, Lee noticed that divergent values underlying the field of psychology posed a challenge to Asian American clergies’ willingness to embrace psychotherapy. The field of psychology has been guided by values that contrast with those of Asian American Christian communities, causing skepticism among clergy. For example, the foundation of psychology began with Freud viewing religion as a falsification of reality, and he believed that adherence to religion was a mass delusion (Hood, 2012). As such, many pastors were concerned that psychotherapy would overlook the congregants’ spiritual needs and overly prioritize the medical model, particularly through the overuse of medication. Some also objected to psychology’s emphasis on individualism, arguing that decisions should consider the client’s family and/or community. Clergy also raised concerns regarding the potential for clients to deflect responsibility and disregard personal accountability. This was at odds with Christian doctrine that emphasizes the inherent sinful nature of humanity, suggesting that individuals possess some level of personal accountability.
In light of the increasing mental health concerns observed among her KA Christian clients, Cho initiated a conversation with Lee to explore the possibility of establishing a trusting, collaborative relationship. Both individuals maintained a respectful awareness of each other’s roles and responsibilities, yet they recognized the existence of significant misunderstandings between clergy and therapists, which contributed to a siloing effect that hampered the healing process for KA Christian clients. Cho and Lee saw the advantages a collaborative approach could provide when serving Asian American Christian congregants and clients. Consequently, they began discussing the prospect of convening a group of clinicians and clergy to foster and develop productive and collaborative partnerships.
Despite these differences and challenges, both Cho and Lee believed that clergy and therapists could unite around a shared desire to help Asian American Christian clients/congregants with their mental health struggles. They posited that the mutual commitment to caring for Asian American clients/congregants could foster collaboration between these professionals, enabling them to overcome their differences and deliver meaningful treatment and services. Their efforts aligned with CPM’s focus on person-centered and recovery-oriented principles, which underscore the necessity of maintaining a shared “focus on server-user recovery.” According to CPM, this shared commitment can encourage various professionals to collaborate through dialogue, negotiation, and integration of treatment recommendations, thereby enhancing outcomes for the end client (Ness et al., 2014).
Humanizing, dialoging, and collaborating: Highlighting principles and processes of CPM
A seemingly trivial but imperative step toward successful collaboration was allowing both groups to spend time to connect and humanize one another. Many early interactions between KCA clergy and therapists involved social gatherings that enabled each group the opportunity to lower their defenses and allow for more authentic connections. Eventually, these gatherings transformed into informal dialogues that focused on integrating mental health interventions and theological teachings, aligning with CPM’s process principle of open dialogue, or unrestricted discussions that culminate in creating shared understandings (Seikkula et al., 2003, 2006). Meetings initially consisted of providing clergy with psychoeducational information, but over time, the format transitioned into conversations that included perspectives from both clergy and clinicians. Both engaged in extensive case discussions and dialogues that allowed them to dissect their distinct perspectives, beliefs surrounding healing and spiritual transformation, and notions of truth and correctness. Clinicians provided valuable information on how they would treat mental health symptoms, and clergy provided insight into the spiritual arc of healing and wellness. Both groups shared that they learned the most from these small-group informal case discussions. The dynamic that emerged from these open dialogues became the cornerstone for connecting, learning, and influencing one another.
During these dialogues, CPM’s principles of mutual understanding and trust also emerged between KCA clergy and therapists (Ness et al., 2014). KCA clergy’s misconceptions of the therapists were altered when they recognized that the healing process did not necessarily follow a straightforward trajectory. They also learned that clients may display temporary signs of regression, even though they are achieving meaningful progress. This fostered greater trust in the treatment provided by the KCA therapists. KCA therapists also developed a newfound appreciation for the knowledge and ability that clergy provided. Many therapists are trained to respect their clients’ multicultural identities and beliefs; however, many have not learned how to incorporate nuanced faith beliefs into the minutia of their therapeutic interactions with clients of faith. Clergy, on the other hand, have expertise in interpreting and applying religious teachings to the current cultural context of their congregants. As such, KCA clergy helped therapists interweave spiritual concepts into clinical interventions that not only resonated with their client’s belief systems but also propelled them forward in treatment. When clients intuited that the clinical interventions holistically fit their ethnoreligious beliefs, they exhibited less resistance and held an implicit felt assurance that there was approval from their faith community. The mutual understanding that developed between KA clergy and therapists ultimately allowed both to be in an equitable position, whereby they viewed each other’s perspectives as significant and valuable.
In learning and respecting what each had to offer, both KCA clergy and therapists gained insight into their respective roles, according to CPM’s principle of self-understanding (Ness et al., 2014). The developed mutual understanding fostered a sense of humility and openness for both professionals, whereby KCA clergy and therapists began recognizing their limitations. KCA clergy, for instance, become more adept at identifying when to refer congregants to therapists, particularly in cases of moderate mental health issues, and KCA therapists became more at ease in seeking assistance from clergy for matters pertaining to religious and spiritual interpretation. This approach enhanced the support offered to congregants but honored the distinct contributions each profession brought to mental health care.
Once mutual understanding and self-understanding were firmly established, CPM’s principle of shared decision-making and participatory engagement emerged as an essential component for successful collaborative treatment (Ness et al., 2014). With a foundation of trust, and empathy established, both groups established open lines of communication for consultation and support. They honed their ability to identify their area of expertise, collaboratively agree on assessments and treatment recommendations, make joint decisions, tailor their roles when treating the KCA client, share responsibilities, and provide coordinated care effectively. Ultimately, they exhibited a unified approach toward common goals, ensuring that all participants in the cooperative treatment process were aligned and committed to the shared objective of helping KCA clients with their mental health struggles.
The success of this process led to the formal establishment of a community known as PACT in 2017. PACT met regularly from 2017 to 2024 to discuss case studies among clergy and clinicians and hosted regional meetings with guest speakers to discuss mental health topics relevant to their ethnoreligious micro-communities. The objective of PACT was to provide a platform for Asian American practitioners and clergy to participate in constructive and open dialogues aimed at integrating their respective fields and cultivating robust professional relationships.
Case study: KCA clergy and therapists exhibiting shared decision-making and participatory engagement
The case study below provides a fictional example of how KCA clergy and clinicians from PACT could take part in participatory engagement following the implementation of collaborative processes and principles. The case commences with a detailed description of a fictional client that KCA clergy and therapists would likely encounter, along with the types of questions that they would engage in to foster an open dialogue. It then outlines treatment recommendations that KCA clergy and therapists would endorse. The purpose of this case is to demonstrate how these fundamental principles and processes would culminate in coordinated and culturally effective care for the Chinese American (CA) client.
The client
Sarah is a 19-year-old college sophomore. She was raised in a conservative Chinese Christian family and was actively involved in her local church during her high school years. Since beginning college, her church attendance has become infrequent and she has not been participating in her Christian communities. She retains her belief in God but acknowledges that she has been raised within a “Christian bubble” and is eager to explore outside those confines.
During her first year in college, Sarah joined a sorority and immersed herself in Greek life. She occasionally experimented with substances, such as consuming alcohol or using amphetamines during exam periods, to aid her concentration. During her freshman year, Sarah entered a romantic relationship and is now sexually active with her partner.
Clinical manifestations
Sarah presented with depressive symptoms following her initial year in college. She exhibited signs of loss of appetite, prolonged sleep (12–14 hours per day), and a lack of interest in activities apart from engaging in phone conversations with her boyfriend. She attributed the cause of her symptoms to the geographical distance from her boyfriend and the challenges imposed by her strict parents, particularly their discontent toward Sarah not attending church regularly. She presented with conflicted feelings where she desired to reconnect with her church friends but felt like a “hypocrite” and grappled with substantial feelings of guilt.
Upon returning to campus for her sophomore year and reuniting with her boyfriend, her symptoms alleviated. However, shortly thereafter, Sarah displayed atypical behaviors. She experienced periods of heightened activity, substantially reduced sleep, impulsive shopping, and expressed aspirations of becoming a social media influencer. In addition, she exhibited grandiose thoughts, believing that men were pursuing her and that her female acquaintances were envious of her. She confided in her boyfriend, disclosing her belief that she was being influenced by malevolent entities, compelling her to engage in risky behaviors.
At the urging of her boyfriend, Sarah sought medical attention at her university’s clinic, leading to a referral to a psychiatrist who diagnosed her with bipolar disorder. Upon notification of her condition, her parents intervened, compelling her to withdraw from college, return home, discontinue her medication, and seek counseling from their religious leader. Her parents attributed her condition to spiritual issues arising from perceived “sinful” conduct and substance use. They advocated repentance and spiritual deliverance as the remedy for her circumstances.
Questions to encourage open dialogue
In exploring the intersection of psychology and religious/spiritual faith, clergy and clinical professionals engaged in an open dialogue to compare and contrast their perspectives on behaviors, choices, and interventions that they perceived as either helpful or detrimental. The collaborative discussion encompassed several questions, including the following:
As a pastor/clinician, how would you intervene in this scenario?
How can we reconcile the clinical construct of mental pathology with the Christian concept of humanity inherently having a sinful nature?
Does our increasing dependency on a clinical framework for mental disorders erode our capacity to employ moral classifications in the assessment of thoughts and behaviors?
Is there an irreconcilable conflict between a psychological/medical framework and a spiritual/moral framework for comprehending the client’s predicament?
What would represent a “biblical” approach for clergy to assist Sarah?
What would be a religiously informed and culturally competent approach for counselors to aid Sarah?
In the initial phase of open dialogue, clinicians assisted clergy members in understanding the diagnostic criteria and risks associated with bipolar disorder, as well as detailing circumstances where clients could benefit from medical intervention. Clinicians emphasized that a psychological diagnosis should not serve as a broad stigma or a means of absolving individuals of personal responsibility. Instead, the degree of personal responsibility in treatment should gradually grow. Following this explanation, the clergy came to understand that Sarah’s bipolar condition necessitated medical treatment and was not solely a spiritual matter. As such, the clergy provided coordinated care with Sarah’s family to reduce the stigma surrounding her mental illness and urged them to pursue medical and psychotherapeutic interventions.
The clinician prioritized understanding Sarah’s mental health challenges in relation to her faith and worked with religious leaders to incorporate effective spiritual interventions. Sarah shared her feelings of shame and self-criticism and why she avoided her religious community and family. In addition, based on Sarah’s interpretations of specific biblical narratives and moral lessons, she expressed feeling like a “hypocrite” and believed she deserved her diagnosis. She also anticipated judgment from her church acquaintances and was reluctant to attend services. Upon obtaining Sarah’s consent, the clinician communicated some of these concerns with Sarah’s religious leader. The clergy and therapist collaborated to integrate faith-based beliefs and psychotherapeutic techniques in a balanced and dialectical manner. Their goal was to assist Sarah in maintaining autonomy in decision-making while developing a more self-compassionate understanding grounded in her ethnoreligious background. They helped Sarah recognize the importance of repentance, encouraging self-accountability in her healing process while also acknowledging the harmful impact of a legalistic approach to spirituality. By fostering a dialectical perspective, Sarah embraced self-compassion and self-agency. Following these interventions, Sarah demonstrated a gradual reduction in self-criticism, an improvement in mental health symptoms, and a continued willingness to maintain ties with her community.
The therapist acknowledged the importance of re-integrating Sarah into her ethnoreligious community for continued healing. With the goal of encouraging Sarah to expand her experience of self-acceptance to an overall acceptance from her ethnoreligious community, the clinician engaged with Sarah’s religious leaders to foster a more inclusive culture of mental health awareness at Sarah’s church. In their sermons, clergy began emphasizing the concept of God’s unconditional love and communicated that mental health challenges were not necessarily a divine punishment but rather an opportunity for self-care. This helped Sarah begin attending religious services, and she became less apprehensive about judgments from others. Other congregation members began showing support and empathy toward Sarah, which furthered her healing process.
Clinicians and clergy became adept at teaching Sarah how to balance psychotherapeutic and ethnoreligious messages. This approach helped Sarah receive personal acceptance, self-compassion, and unconditional positive regard while incorporating theological and cultural beliefs into her healing journey. The clergy played a pivotal role in expressing their approval for mental health services, creating a culture within Sarah’s faith community that was more inclusive of mental health awareness, and acting as a mediator between congregants and mental health providers. Through a collaborative relationship, clinicians and clergy offered personalized and coordinated solutions that resonated with Sarah’s ethnoreligious identity.
Discussion
The collaborative process undertaken by KCA clergy and therapists in the Chicago area proved highly effective in delivering culturally sensitive and impactful care for their Asian American Christian clients/congregants. Although the successful elements of this partnership closely align with numerous principles and components of the CPM, this section will emphasize additional factors that were essential for this community when implementing these practices. We will then explore potential limitations that future Asian American Christian professional communities ought to consider when serving the mental health needs of their clients and then conclude by highlighting the opportunity for collaboration and expansion throughout the United States.
Culturally relevant elements necessary for successful collaboration among KCA clergy and therapists in Chicago
The CPM emphasizes open dialogue as a fundamental aspect of effective collaboration (Ness et al., 2014). This element was particularly important for the practitioners and clergy of PACT; however, other culturally relevant preliminary steps were also necessary for the KCA Christian community in Chicago before effective engagement could occur. Specifically, the clergy and therapists from the Chicago KCA community required several gatherings focused solely on social interaction, devoid of work-related topics. These interactions allowed them to connect personally as individuals before embarking on collaborative discussions concerning clinical integration. This example underscores the importance of honoring the unique characteristics of each cultural microcosm. It emphasizes the importance for each community to permit itself to modify a codified model to align with the model’s higher goals and principles effectively.
Numerous KCA clergy and therapists also note that adopting a hermeneutical stance when engaging in discussions is instrumental in their adherence to many of CPM’s principles, such as equitable roles, mutual understanding, and shared decision-making. Hermeneutics involves a reflective approach to the interpretation and understanding of the meaning-creation process (Gadamer, 1985). This methodology encourages individuals to set aside preconceived notions and consider perspectives that differ from their own (Ricoeur, 1970). As a result, a “third space” is created, which minimizes the power struggles that often arises within a dichotomous framework of disciplinary integration (Benjamin, 2004) and leads to a reconceptualization of one’s understanding (Sandage & Brown, 2015). The adoption of a hermeneutical stance allows the KCA clergy and therapists to gain new insights and enables the development of effective interventions specifically designed to address the diverse needs of Asian American clients.
For clinical integration to be effective, recognizing that individuals, communities, and microcosms are dynamic beings is also essential. Drawing from dynamic systems theory (Thelen & Smith, 1994), successful integration must understand that therapy and integration are deeply interconnected and dynamic experiences. There is a constant exchange within a symbiotic relationship between individuals and their cultural backgrounds, thinking and relating patterns, developmental histories, and many other factors. Whether in a clinical setting or within an ethnoreligious community, no two relationships are the same, nor do they remain the same. As a result, successful clinical integration cannot be a fixed model but rather an emerging and evolving phenomenon developed through the continual experience of humbly relating, openly communicating, authentically emoting, and acting together (Sandage & Brown, 2015).
This community case also supports the notion that case conceptualizations are a highly effective way to develop culturally appropriate clinical integration methods and cultural competency (Mackrill & Iwakabe, 2013). With case studies, professionals can learn to adapt their approaches so that they are tailored to the client’s needs, all while developing a “language” and “new knowledge” that can be understood and shared with professionals across disciplines and domains (Mackrill & Iwakabe, 2013). This way of learning—narrative telling and discussion, as opposed to lectures and model-building—also allows for culturally thoughtful ways of understanding and intervening and is more effective at motivating individuals into action as they imagine simulations of treatments and what they might do in similar situations (Strawn et al., 2018). Case study discussions can accommodate various complexities by focusing on the process of treatment, culturally relevant interventions to the client, and the synthesis of critical factors unique to that client, given their specific context and cultural identities.
Key considerations prior to implementing the CPM
When implementing CPM’s principles, practices, and techniques, maintaining a deep understanding of each ethnoreligious microcosm’s uniqueness is crucial. This community case underscores the importance of considering various factors linked to a client’s mental illness, which are closely tied to their individual and community context. For instance, a deep understanding of the client’s interpretation of theological teachings, how it manifested into their mental health symptoms, and the prevailing theological views within their micro-community were all significant. Therefore, each implementation must be customized to key variables. The CPM should be approached as a means of genuine engagement with clients, requiring an understanding of their lived experiences before proposing solutions. Neglecting these components to expedite implementation may jeopardize effective collaboration.
National and regional implications
The model set forth by PACT and the effectiveness of CPM for clinical integration could also benefit other Asian American Christian communities. Increasing openness, humility, and relational dialogues among Christian therapists and religious leaders appear to be advantageous in addressing the rising mental health needs of Asian American Christian clients. There are likely many untapped opportunities in other metropolitan areas with sizable Asian American populations, such as New York City, Los Angeles, San Jose, and San Francisco (U.S. Census Bureau, 2012). However, in the context of replicating the CPM in various communities, local leaders must underscore the significance of adopting a collaborative and relational approach to integration. It is important for various professionals and stakeholders to highlight elements that are pertinent and suitable for their specific ethnoreligious community.
The power of the internet and digital communication could also allow for regional professional networks to be replicated at a national level. Catalyst Wellness Alliance is an organization that has been actively involved in creating a national digital ecosystem to connect pastors, counselors, researchers, and nonprofit organizations. They have developed strategies to replicate PACT’s processes in the Chicago area and, as of January 2024, began hosting monthly virtual gatherings for pastors to engage with mental health professionals by fostering discussions using many of the principles and processes highlighted by CPM. This approach has the potential to provide culturally effective care to a population that has been chronically under-utilizing professional mental health services. Allowing for successful integration and collaboration among key professionals within an ethnoreligious community has the potential to cultivate a culture that could prevent mental health illnesses, mitigate psychological symptoms, or provide more effective spiritual–clinical interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.