
Abstract
The purpose of this study is to examine the relationship between belief in divine healing and HbA1c (a biomarker of blood glucose control). Three major findings emerged from our analysis of data from a nationwide survey. First, a set of descriptive analyses suggest that faith healing beliefs are not the sole province of Conservative Christians. Instead, belief in divine healing is more widely spread in the general population. Second, our analyses indicate there is a nonlinear relationship between belief in divine healing and HbA1c values: HbA1c scores are relatively high (i.e., less desirable) among study participants with low levels of belief in faith healing. However, levels of HbA1c are lower among study participants with a stronger belief in the divine. Third, our analyses further indicate that a religious sense of meaning in life, but not a general sense of meaning, mediates the relationship between belief in faith healing and HbA1c values.
Introduction
The purpose of this study is to see whether belief in divine healing is associated with health. We define divine healing (i.e., faith healing) as the extent to which a person expects that physical and mental health problems can be cured or improved by the direct intervention of God or some other supernatural being. There are five reasons why it is important to empirically evaluate this relationship.
Historical considerations
Historians who study religion in the United States have gone to great lengths to document the nature and influence of the First and Second Great Awakenings (Ahkstrom, 1972). The First Awakening took place around 1734, while the Second Great Awakening took place around 1830 (Ahkstrom, 1972). The Great Awakenings were characterized by huge religious gatherings that were led by itinerant preachers who conducted services outside formal religious institutions. Many times (but not always) these meetings were held in large tents that were pitched in open fields. Faith healing was often an integral part of these meetings. This means that people with a wide range illnesses came forward during worship services to be cured of their maladies purely through faith in God’s healing powers. This healing was typically accomplished through the laying on of hands coupled with emotionally charged encouragement by people who were in the congregation. Lake (1949/2002) claims that, “By the most careful estimates the Church at Spokane reports 100,000 healings in the past five years” (p. 150).
The First Great Awakening did not escape the notice of none other than Benjamin Franklin. Isaacson (2003) reports in his biography of Franklin that he, “. . . became enthralled with George Whitefield, the most popular of the Great Awakenings roving preachers. . .” (Isaacson, 2003, p. 110). Franklin attended a Whitefield revival that drew nearly 6,000 people. In fact, Franklin was so taken by Whitefield that he had Whitefield stay in his home.
Although considerable attention has been paid to the historical analysis of the Great Awakenings, this phenomenon has largely been overlooked by social and behavioral scientists who study the relationship between religion and health. Although the Great Awakenings took place centuries ago, they left a deep imprint on the way many Christians view their faith. For example, a study by the Pew Research Center (2008) indicates that 34% of all American adults report they have experienced or witnessed divine healing of an illness or injury.
The first goal of our study is to infuse research on religion and health with insights that have their roots in the Great Awakenings. More specifically, we want to know whether belief in divine healing leads to measurable improvements in health.
Methodological problems with empirical research
Significant limitations exist in the few studies that focus specifically on divine health interventions. The bulk of this research has relied on small, nonrepresentative samples of adults, making it difficult to determine whether the insights they provide can be generalized to a wider population. For example, Village (2005) studied 400 people who attended 1 of 11 churches. Similarly, Johnson et al. (1986) conducted their research on 586 adults in Richmond, Virginia. In addition, Poloma and Hoelter (1998) drew a sample of study participants from a single movement: Toronto Airport Christian Fellowship. We address these sampling drawbacks by analyzing data that have been gathered from a large nationwide survey of American adults.
Mediators of the relationship between faith healing and health
Another limitation with current studies on faith healing arises from the fact that relatively little attention has been devoted to empirically demonstrating how the presumed effects of divine healing arise. Another goal of our research is to see whether belief in faith healing operates (in part) by bolstering a religious sense of meaning in life.
Meaning in life is a notoriously difficult construct to define. Our study is not the place to resolve this longstanding issue. Instead, we rely on the definition that was proposed by Reker (2000). He maintains that meaning in life entails a sense of, “ . . .order, coherence, and purpose in one=s existence, the pursuit and attainment of worthwhile goals, and an accompanying sense of fulfillment” (Reker, 2000, p. 41). Recently, some investigators have refined the general notion of meaning in life by arguing that greater insight can be obtained by working with a sense of meaning that explicitly arises within the context of religion (i.e., a religious sense of meaning in life). A religious sense of meaning may be a suitable mediator of the relationship between divine healing and health, because research reveals that it is an important determinant of health and wellbeing in its own right (Krause, 2003).
Issues in the measurement of health
All the studies we have been able to locate on divine healing and health focus solely on self-reports of health. Unfortunately, belief in faith healing and self-reports of health are both subjective phenomenon and as a result, it is difficult to determine whether belief in faith healing affects health or whether health influences perceptions of divine healing. We aim to overcome this limitation by seeing whether belief in divine health intervention is associated with a key biologically measured indicator of health—hemoglobin A1c (HbA1c). HbA1c, which is obtained through analysis of blood samples, is a measure of the extent to which a person maintains healthy blood sugar levels.
There are four reasons why we focus specifically on HbA1c and (by extension) diabetes. First, diabetes is a major social problem. Sherwani et al. (2016) report that 29.1 million Americans suffer from this condition. They go on to point out that this comes at a major cost to our society—US$245 billion in 2012. If we want our research to matter, then we must link it to specific real-world health conditions and the problems they create.
Second, as Sherwani and his colleagues point out, HbA1c is widely recognized as the “industry standard” for diagnosing diabetes and pre-diabetes (Sherwani et al., 2016). In fact, as these investigators go on to point out, HbA1c is now recognized by the World Health Organization (WHO) as a standard of care (SOC) for testing and monitoring diabetes. We ultimately aim to bridge the gap between basic research and clinical care. Studies that focus on specific biomarkers that are associated with particular health conditions are more likely to catch the eye of those who treat those conditions. This means, for example, that finding a link between faith healing beliefs and titers to the latent Epstein-Barr Virus (a measure of immune functioning) is less likely to be of interest to clinicians who treat diabetes.
Third, we focus on HbA1c because prior research indicates that this type of physiological measure is especially responsive to psychosocial influences such as stress, emotions, and psychological wellbeing (Coccaro et al., 2016). We have not been able to locate any prior research on faith healing and HbA1c (or any other biomarker for that matter). Documenting an empirical relationship between the two adds an aura of legitimacy to this phenomenon that some might otherwise consider improbable.
The need for descriptive analyses
The fifth reason more work is needed on faith healing beliefs is basic, but essential. We believe that before predictors of a phenomenon, like belief in divine healing, can be identified and evaluated empirically, it is important to first describe them. This means that work in this field should begin descriptively by identifying the people who are most likely to embrace faith healing beliefs in the first place. This kind of research is valuable because, as we will show below, it can dispel inaccurate perceptions about faith healing. Moreover, descriptive studies are useful because they can steer researchers toward other factors that influence faith healing beyond those that are considered in our study.
Theoretical Underpinnings
Before turning to the mechanics of our study, we flesh out the theoretical underpinnings of our work by elaborating on some of the issues we have just discussed.
How the potentially salubrious effects of faith healing arise
Findings from two closely related bodies of research help explain how the benefits of belief in divine health interventions might arise. The first has to do with expectancy theory while the second involves research on the placebo effect. In fact, the two are so tightly intertwined that Olson et al. (1996) maintain that, “Without question, the literature that has addressed the somatic and physiological consequences of expectancies is the placebo effects literature” (p. 224).
Expectancy theory is a process theory of motivation which holds that an individual’s effort will be determined by the expected outcomes and the value placed on these outcomes by the person in question (Isaac et al., 2001). The placebo effect refers to a bogus substance or treatment that is deliberately designed to have no therapeutic value. In clinical settings, placebos typically include things like sugar pills. The underlying idea, and the factor that links placebo effects with faith healing beliefs, is that the recipient of the placebo does not view it as a sham and instead perceives the “treatment” to be real and capable of producing the desired effects. Based on these beliefs alone, the recipient of a placebo may experience measured improvement in their sense of health and wellbeing. As reviews of the literature reveal, the magnitude of the effects of placebos can be quite substantial (Brody & Brody, 2000).
There are four ways in which the findings from research on the placebo effect can contribute to our understanding of the ways faith healing may produce legitimate improvements in health. The first explanation is provided by Brody and Brody (2000). These researchers argue that if people genuinely believe that a treatment will eradicate unwanted health problems, they are likely to experience a reduction in the anxiety and stress that these physical challenges present and as a result, experience legitimate improvements in their health.
The second explanation comes from the work of Olson et al. (1996). These researchers maintain that belief in a placebo may encourage people to focus on small improvements in their health that they might not have noticed otherwise coupled with a negation of negative fallout that might would typically cause considerable health concerns. This shift in perceptual focus may lead to measurable health improvements.
Third, as Olson et al. (1996) also point out, belief in the legitimacy of a placebo may reduce unwanted health symptoms by activating the endogenous opiate system which may, in turn, reduce the pain and discomfort associated with a health problem.
The fourth way to explain the effects of placebos is unique to religious settings. When a person attends a revival that focuses on faith healing, the prospect of improvement in health is cloaked with an aura of legitimacy that arises from the authority of the pastor who is leading the healing session. Moreover, based on their training, status, and sense of responsibility, these pastors are likely to believe even more fervently in the efficacy of faith healing than rank-and-file congregational participants. Support for this mechanism is found in the theory of religion that was devised by Stark and Finke (2000). They maintain that, “Confidence in the explanations offered by a religion will be greater to the extent that ecclesiastics display levels of commitment greater than that expected of followers” (p. 112).
But there may be more to it than this. Faith healing takes place in front of a congregation which, as we noted earlier, can be quite large. These congregational members are, by virtue of their presence, also likely to believe in the legitimacy of faith healing. Moreover, these religious others are often encouraged to express their support for faith healing in a highly emotional manner. This group-level state of heightened emotional arousal can produce an emotional contagion effect (i.e., the spontaneous spread of emotions from one person to another; see van Kleef & Cote, 2022, for a review of research on the emotional contagion phenomenon). This issue was also discussed by Stark and Finke (2000). These investigators maintain that, “An individual’s confidence in religious explanations is strengthened to the extent that others express their confidence in them” (Stark and Finke, 2000, p. 107).
The discussion in this section may subtly convey the feeling that the effects of divine health interventions are contrived or artificial. We do not intend to create this impression. This is one reason why we focus on a biomarker (HbA1c) as an outcome in this study. If a significant relationship is found between belief in faith healing and levels of HbA1c, then we should feel more confident in concluding that faith healing has “real” measurable effects that are independent of bias that is associated with self-perceptions of health.
Elaborations and extensions
At first, it may seem that the relationship between belief in faith healing and health-related outcomes is linear. This means that the effects of belief in faith healing on HbA1c are constant across all levels of belief in divine healing. However, a deeper reading of the literature suggests otherwise. More specifically, we believe there may to be a nonlinear relationship between faith healing beliefs and HbA1c.
We suspect that relatively weak beliefs in the effects of faith healing will have a minimal impact on health because major health problems are not changed easily and only a deep sense of commitment to one’s faith can affect physiological changes in the body. Put another way, a half-hearted or guarded belief in divine health interventions is not sufficient to motivate God to permit significant change to take place in health. Evidence of this may be found in the literature on the Second Great Awakening. Charles Grandison Finney was a Presbyterian minister who was often called the “Father of Revivalism.” Writing in 1834, he identified the elements that are necessary for a successful revival. More specifically, Finney (1834/1968) wrote that
God has found it necessary to take advantage of the excitability there is in mankind, to produce powerful excitements among them, before he can lead them to obey. Men are so sluggish, there are so many things to lead their minds off from religion, and to oppose the influence of the gospel, that it is necessary to raise an excitement among them, till the tide rises so high as to sweep away the opposing obstacles. (Finney, 1834/1968, p. 87)
Cast within the context of our study, Finney’s (1834/1968) insights suggest that the benefits of believing in divine health interventions should only become manifest among those with the highest level of commitment to them. Similar views were expressed by George A. Coe, who was a pioneer in the psychology of religion. Referring specifically to religious healing, he argued that, “. . . it is clear, the subjective state of the patient, if a cure is to be wrought, must be one of intense faith” (Coe, 1900, p. 184; emphasis added).
It is important to reflect on the shape of the regression slope that captures the nonlinear relationship between faith healing beliefs and HbA1c values. By convention, HbA1c values are coded so that a low score indicates good glucose control. So, if Finney (1834/1968) and Coe (1900) are correct, weak faith healing beliefs will be associated with relatively high HbA1c values. However, the strength of this relationship will reach a tipping point. Beyond this threshold, HbA1c values will decline at an accelerating pace.
These insights lead to the following hypotheses:
H1: there will be a nonlinear relationship between faith healing beliefs and HbA1c values: initially, weak faith healing beliefs will be associated with high HbA1c values, but beyond a certain threshold point, the relationship between faith healing beliefs and HbA1c values will decline at an accelerating rate.
Exploring the mediating role of a religious sense of meaning in life
Findings from a considerable number of studies suggest that people who have found a general sense of meaning in life tend to enjoy better physical and mental health than people who have encountered more difficulty in finding a sense of meaning (Krause et al., 2013). Considerably less research has been conducted with a religious sense of meaning in life.
The benefits of working with a religious sense of meaning in life have been discussed by Krause (2012). He maintains that measures of a religious sense of meaning in life may be more responsive to the religious influences than global measures of meaning in life. Here is why it makes sense to focus on a religious sense of meaning in the current study. If people fervently believe that God will cure their physical health problems, and if these beliefs ultimately lead to an eradication of their health problems, then people are likely to redefine the nature of their relationship to God and the overall structure of their faith. More specifically, individuals who experience a healing will be more likely to view God in a more beneficent and responsive manner. To the extent this is true, they should experience a deeper and richer religious sense of meaning in life.
We have not been able to locate any studies that assess the potential mediating role that is played by meaning in life in the relationship between faith healing beliefs and HbA1c. Yet another goal of our study is to do so. In the process, we hope to stimulate interest in a religious sense of meaning in life by comparing and contrasting the mediating effects of a general sense of meaning in life and a religious sense of meaning in life.
The role of descriptive analyses
Many factors are likely to influence the extent to which individuals embrace faith healing beliefs. Fully enumerating all of the possibilities would require a separate paper. Consequently, our intent is merely to provide a preliminary assessment of this issue. Before we empirically evaluate the hypotheses that are specified above, we present a brief descriptive overview of the factors that are associated with adopting beliefs about faith healing. Because this overview is descriptive in nature, we will not test specific hypotheses. This is consistent with the stance that is taken by Koepsell and Weiss (2003), who argue that, “The hallmark of a descriptive study is that it is undertaken without a specific hypothesis” (p. 95). Instead, our intent is to get a glimpse of the wider social psychological context in which faith healing beliefs arise.
Our descriptive analyses will focus primarily on the social demographic correlates of beliefs in divine health interventions including age, sex, race/ethnicity, and participation in Conservative Christian congregations. By beginning in this general manner, we hope to identify constructs that serve as a gateway to more fine grained analysis of the social psychological underpinnings of belief in divine healing.
Methods
Sample
The data for this study come from the Landmark Spirituality and Health Survey, a nationwide face-to-face survey of adults aged 18 years and older who reside in the coterminous United States (i.e., residents of Alaska and Hawaii were excluded). The data for this study, which was completed in 2014, were collected by the National Opinion Research Center (NORC) in Chicago. The NORC 2010 National Sampling Frame served as the basis for the sampling procedures. This sampling frame is based on two sources. First, the bulk of this database comes from postal address lists that are compiled by the United States Postal Service (USPS). Second, field employees were sent to enumerate all houses in areas where USPS address lists were unavailable. Sampling was done in three stages. First, National Sampling Areas (NFAs) were constructed. In essence, NFAs are formed from partitioning counties and metropolitan areas into geographical units of designated sizes. A total of 44 NFAs were selected with probabilities proportional to size. Then, in the second stage, NFAs were partitioned into segments consisting of Census tracts and block groups. Segments were selected with probabilities proportional to size. In the third stage housing units were sampled with equal probabilities of selection within each segment and the occupants of these dwellings were recruited for the interviews.
There are two reasons why we do not use the entire sample in the analyses that are provided below. First, a number of physical measures were obtained in our study including measured heigh, weight, and blood pressure. In addition, blood spots were obtained to assess other biomarkers, including HbA1c. As in any study, some people participated in the survey, but declined to provide physical measures (N = 711). The refusal rate for physical measures is comparable to the refusal rates for other major surveys, such as the widely cited Health and Retirement Survey (Health and Retirement Study, 2004). Second, questions on religion were not administered to study participants who self-identified as atheists (N = 78). Consequently, after using listwise deletion to deal with item nonresponse, complete data were available for between 1,733 and 1,770 (this number varies depending upon the variables in the analyses). Preliminary analysis reveals that the average study participant was 52.4 years old, he or she completed an average of 13.3 years of schooling, 42% were men, 48% were married, and 13.6% self-identified as African American.
Measures
Belief in Faith Healing: This construct was measured with three modified indicators that were taken from the Belief in Divine Intervention Scale that was developed by Degelman and Lynn (1995): (1) “Real miracles of healing from God occur today”; (2) “God sometimes directly intervenes to heal individuals with diseases like cancer”; (3) “God has healed me or someone I know personally.” A high score on these indicators denotes a stronger belief in divine healing (M = 11.27; SD = 2.84; range = 3–15). Since this is the focal variable in our study, we provide two additional statistics that more fully depict the distribution of this measure. The first is an estimate of skewness (−.754; standard error = .058), while the second is an estimate of kurtosis (.287; standard error = .116). The internal consistency reliability estimate (Cronbach’s alpha) for this brief composite is .853.
HbA1c: At the end of the interviews, a blood sample was collected via a capillary finger stick with a disposable lancet. Between three and five blood spots were applied to filter paper and shipped to the Department of Laboratory Medicine at the University of Washington for analysis. We did not work with raw HbA1c scores. Instead, the raw data were transformed using a Windsorizing procedure (Ratcliff, 1993). This means that HbA1c scores that fell beyond 3 SDs above the mean were replaced with scores that fell exactly at 3 SDs above the mean. This makes it possible to deal with the unwanted influence of outliers, while at the same time retaining highly skewed cases so that the sample remains representative. After using the Windsorizing procedure, the range of HbA1c scores was 3.96–8.13 (M = 5.48; SD = .76).
Religious Sense of Meaning in Life: Three items that were developed by the LSHS research team were used to measure a religious sense of meaning. The following indicator is representative of the measures in this scale: “God put me in this life for a purpose.” A high score on this short scale reflects a stronger sense of religious meaning in life (M = 12.47, SD = 2.90; range = 3–15). The reliability estimate for this composite is good (.916).
General Sense of Meaning in Life: A general sense of meaning in life was assessed with six indicators. These items are a shorter version of the meaning scale that Krause (2004) devised. Here is one indicator from this scale: “In my life I have clear goals and aims.” A high score indicates a stronger general sense of meaning in life (M = 24.43; SD = 3.74; range = 11–30). The estimate of Cronbach’s alpha for this scale is good (α = .845).
Religion Control Measures: The relationships among belief in divine healing, meaning in life, and HbA1c were estimated after the effects of three measures of religion were included as control variables in the study models. The first is the frequency of attendance at religious services, which was assessed with an item that was taken from the work of the Fetzer Institute/National Institute on Aging Working Group (1999). A high score stands for more frequent church attendance (M = 4.96; SD = 2.80; range = 1–9).
The frequency of private prayer served as the second religion control measure. This item was also taken from research by the Fetzer Institute/National Institute on Aging Working Group (1999). A high score on this indicator represents more frequent private prayer (M = 6.18; SD = 2.31; range = 1–8).
A measure of affiliation with a Conservative Christian congregation was developed in the following manner. First, a battery of items was administered to determine a respondent’s religious preference. Then, this information was classified with a modified version of the scheme proposed by Steensland and his colleagues (Steensland et al., 2000). These investigators made a distinction between Evangelical Protestants and Black Protestants on the grounds that even though these groups are doctrinally similar, their political views differ significantly. However, because our study is not concerned with political views, Black Protestants and Evangelicals were combined in the analyses provided below. A binary variable was created that contrasts Conservative Christians; i.e., Evangelicals scored 1, and all others scored 0. Approximately 44.4% of the participants in our analyses self-identify as Conservative Christians.
Demographic Control Variables: Our substantive study estimates were derived after the effects of age, sex, education, marital status, and self-identification as African American were controlled statistically. Age and education were coded continuously in years. In contrast, sex (1 = men; 0 = women), marital status (1 = presently married; 0 = otherwise), and self-identification as African American (1 = African American; 0 = all other racial/ethnic groups) were coded as binary variables.
We contrasted Blacks with members of other racial/ethnic groups for the following reason. Research consistently reveals that Blacks have higher (i.e., worse) HbA1c values than members of other racial/ethnic groups (e.g., Ginde et al., 2008). In addition, a considerable number of studies indicate that Blacks are more deeply involved in religion than members of other racial/ethnic groups (Taylor et al., 2004). Therefore, a binary measure contrasting Blacks with all others was included in our analyses to help ensure that the relationship between faith healing beliefs and HbA1c is not spurious.
Data analysis strategy
All the analyses in our study were conducted with ordinary least squares (OLS) multiple regression procedures. The purpose of this section is to review how the most complicated of these models was estimated. This model has to do with assessing the nonlinear relationship between belief in faith healing and HbA1c values. The procedures recommended by Aiken and West (1991) were adopted for this purpose. This analysis was conducted in three steps. First, all the independent variables were centered on their means. Second, a quadratic term was created by squaring the centered faith healing belief scores. Third, a regression model was estimated in two steps. The first step (Model 1) had to do with estimating the linear effects of all independent variables. This was followed in the second step (Model 2) that involved entering the quadratic term into the equation.
If the significance test associated with the quadratic term is statistically significant, then additional steps must be taken to insure that the nonlinear relationship is in the predicted direction. If the nonlinear relationship we propose is present in the data, there should be a positive relationship between low levels of divine healing beliefs and HbA1c values. But as belief in faith healing intensifies, the sign of this relationship should change signifying that stronger beliefs in divine healing are associated with a decline in HbA1c scores. Although any score on the divine health beliefs measure could be used to illustrate these effects, we follow conventional practices and derive estimates at −1 SD below the mean faith healing belief scores, the mean score on belief in divine healing, and 1 SD above the mean divine healing belief score. A formula that is provided by Aiken and West (1991) was used for this purpose (see page 64). An additional formula was subsequently estimated see whether the three coefficients were statistically significant (see page 64).
Results
Descriptive analysis of faith healing beliefs
An OLS regression equation was estimated to provide a preliminary sense of the social demographic correlates of faith healing beliefs. This equation involved regressing faith healing belief scores on the following independent variables: age, sex, education, marital status, Black ethnicity, the frequency of church attendance, and identification with the Conservative Christian faith tradition.
The data indicate that stronger belief in divine healing is found among people who are older (β = .043; p < .05), women (β = −.060; p < .01), individuals with fewer years of schooling (β = −.132; p < .001), Blacks (β = .077; p < .001), people who attend worship services more frequently (β = .333; p < .001), and Conservative Christians (β = .210; p < .001). In contrast, a statistically significant relationship between marital status and belief in faith health failed to emerge from the data (β = .036; b = .205; ns.). Altogether, the variables in this regression analysis explained 24.2% of the variance in divine healing belief scores.
We were intrigued by the relationship between Conservative Christian affiliation and faith healing beliefs because the binary correlation between the two measures (r = .325; p < .001) was smaller than we expected to find. This suggests that belief in faith healing is not exclusively a Conservative Christian phenomenon. We conducted some additional analyses to illustrate this finding in another way. These analyses reveal that 17.1% of Mainline Christians had scores that fell 1 SD above the mean divine healing score. This finding dispels the notion that belief in divine healing is a purely Conservative Christian phenomenon. In the process, it demonstrates the value of conducting descriptive analyses.
Faith healing beliefs and HbA1c
Tests of H1 are presented in Table 1. Two important findings emerge from these analyses. First, as the data provided by Model 1 indicate, the additive effects of faith healing beliefs on HbA1c are not statistically significant (β = .002; b = .001; ns.). Based on these data alone, it would initially appear that belief in divine healing is not associated with HbA1c values.
Assessing the Relationship between Faith Healing Beliefs and HbA1c (N = 1,770).
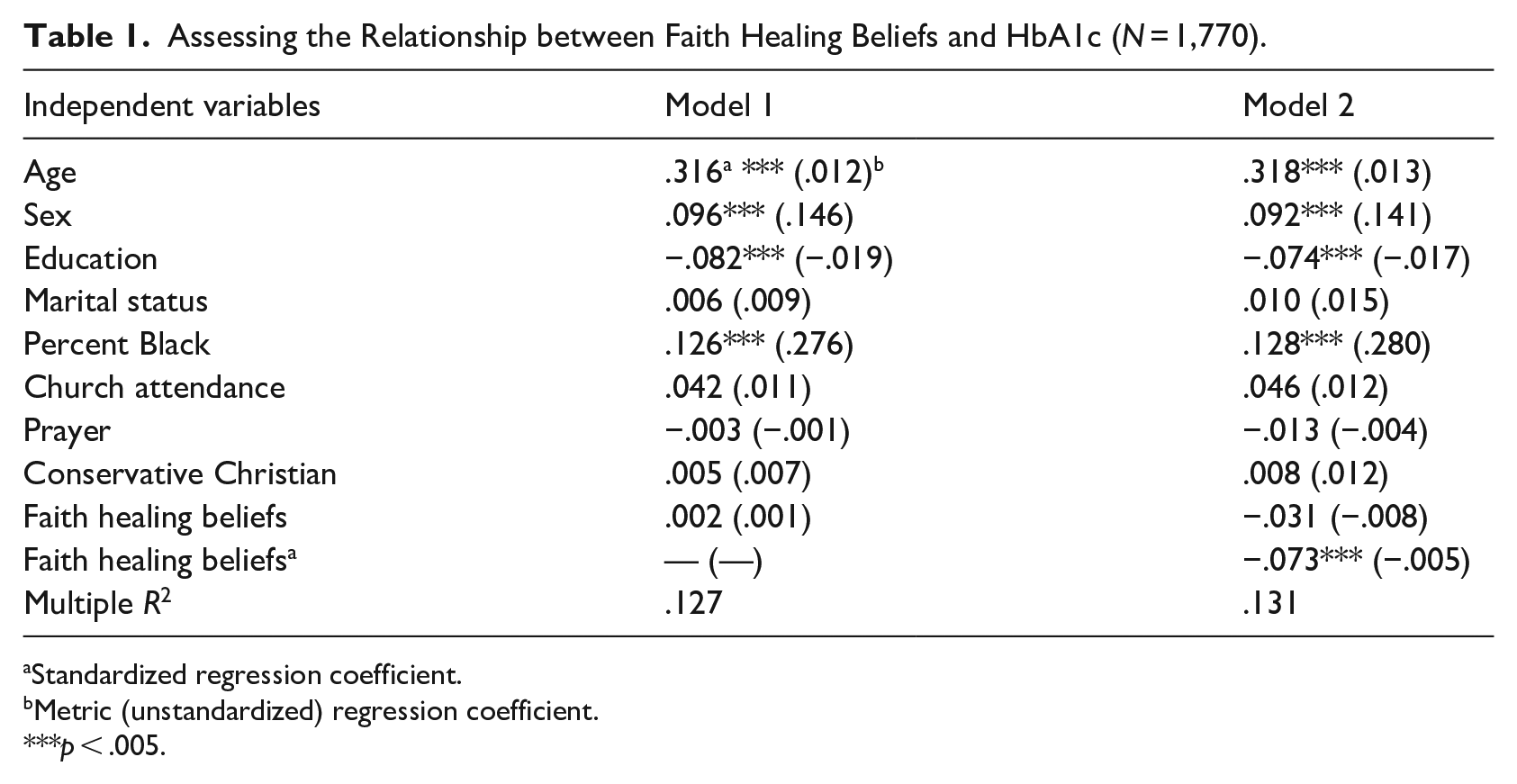
Standardized regression coefficient.
Metric (unstandardized) regression coefficient.
p < .005.
However, a different conclusion emerges when the nonlinear effects of belief in divine healing on HbA1c scores are taken into consideration. As the data provided by Model 2 suggest, there is a statistically significant nonlinear relationship between the two variables (β = −.073; b = −.005; p < .005).
Although a significant nonlinear effect is present, it is important to perform the additional calculations that were discussed earlier to see whether this relationship is in the hypothesized direction. Keeping in mind that high scores on the HbA1c measure denote worse health, the additional computations (not shown in Table 1) reveal that at −1 SD below the mean belief in divine intervention score, belief in faith healing is associated with higher HbA1c values (β = .107; b = .028; p < .001). At the mean of belief in divine health intervention, the relationship between beliefs in faith healing and HbA1c values is no longer statistically significant (β = −.030; b = −088; ns.). The fact that the sign of the coefficients changes suggests that the threshold effect of the relationship between beliefs in faith healing and HbA1c must be close to this point. The additional computations further indicate that at 1 SD above the mean, the effects of belief in divine healing are statistically significant (β = −.177; b = −.036; p < .005). At this level, increments in divine health beliefs are associated with lower levels of HbA1c. Taken as a whole, the data presented here provide support for the first hypothesis (H1).
Further analyses that have not been discussed so far make it possible to identify where the sign of the coefficient associated with faith healing beliefs and HbA1c changes (see Aiken & West, 1991, p. 65, for the formula that is used for this purpose). These additional computations (not shown in Table 1) suggest that the change in signs occurs when belief in divine healing scores are 10.47, which is just below the mean faith healing belief score of 11.27.
Just because the sign of the relationship between faith healing beliefs and HbA1c changes it does not necessarily follow that it is statistically significant, as well. Consequently, we need to know more about where the negative relationship between belief in faith healing and HbA1c values becomes statistically significant. As we just indicated, the relationship is statistically significant at 1 SD above the mean. This corresponds to a raw score of 14.117. We computed the relationship at a raw score of 12. These additional analyses (not shown in Table 1) suggest that the nonlinear relationship between divine healing beliefs and HbA1c values is not statistically significant (β = −.058; b = −.015, ns.). We then computed the effect of faith healing beliefs at a value of 13. These additional analyses (not shown in Table 1) suggest that the nonlinear relationship between the two measures is finally statistically significant (β = −.095; b = −.025; p < .05). Keeping in mind that the range of raw belief in divine healing scores is 3−15, the fact that a significant effect does not emerge until faith healing scores reach 13 is consistent with the notion that more intense levels of belief in divine healing are needed to produce meaningful changes in biological functioning (as measured by HbA1c scores).
An additional step was taken to illustrate the nonlinear relationship between faith healing beliefs and HbA1c values. The nature of this nonlinear relationship is depicted in the graph that is contained in Figure 1. As this figure shows, the relationship between faith healing beliefs and HbA1c takes the shape of an inverted-U (i.e., a curve that is concave downward). Initially, there is a very slight increase in HbA1c scores for study participants with relatively low faith healing beliefs. However, as stronger faith healing beliefs are examined, the relationship declines, as the data provided above reveal.
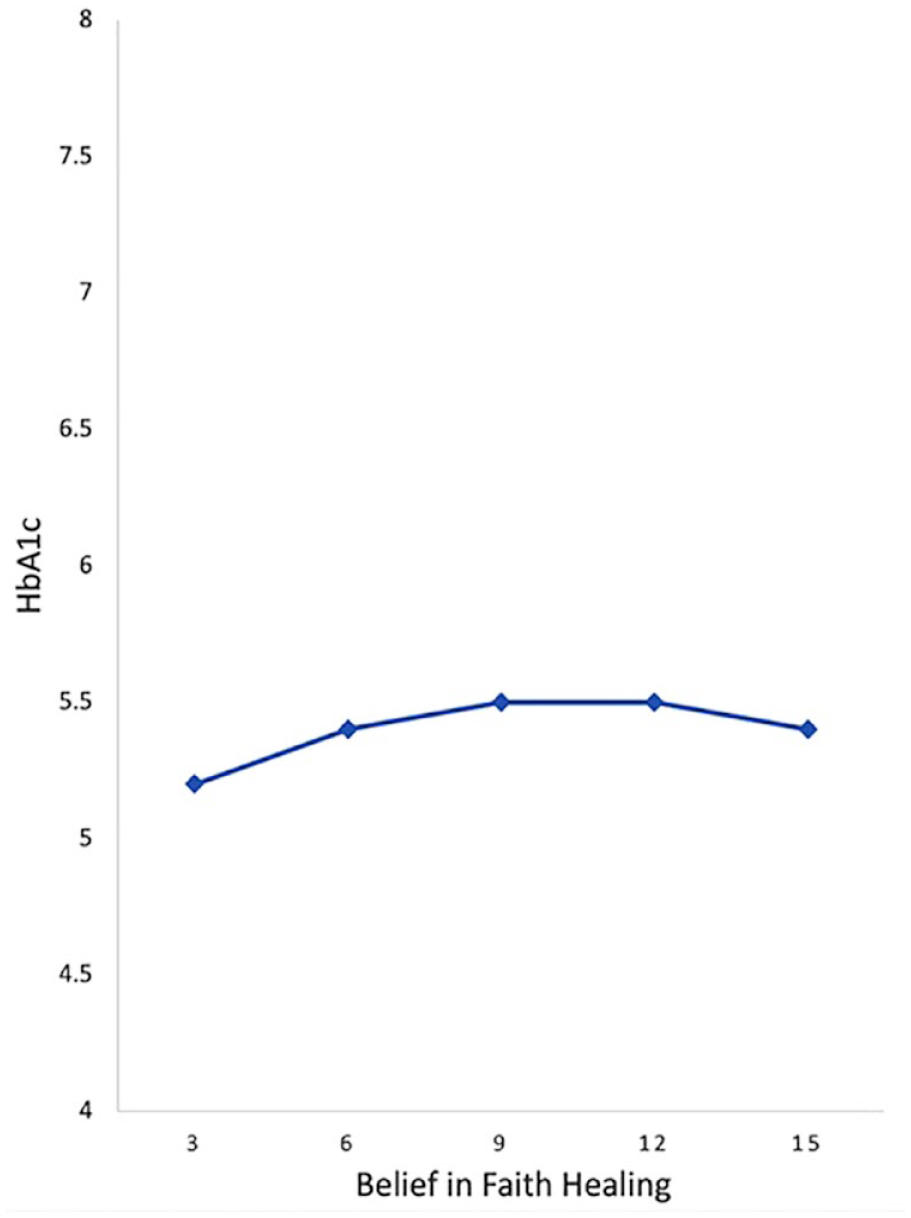
Depicting the nonlinear relationship between faith healing beliefs and HbA1c.
Assessing the mediating role of meaning in life
To demonstrate that a mediating effect is present, we must show that faith healing beliefs are associated with meaning in life and that meaning in life is, in turn, associated with HbA1c values. The purpose of this section is to report the findings from these tests. Recall that we measured meaning in life in two ways: a general sense of meaning and an explicitly religious sense of meaning.
Tests for mediating effects were performed with the PROCESS software subroutine (Hayes, 2022). However, before running the PROCESS analysis, we had to determine whether a general sense of meaning in life and a religious sense of meaning should both be included in the final mediation estimation model. A separate OLS model was estimated for this purpose. The same independent variables that are listed in Table 1 were included in these models, with the exception of the quadratic term. The quadratic term was not included because we could not find a convincing theoretical rationale for why there should be a nonlinear effect of faith healing beliefs on the meaning in life outcomes. These analyses (not shown here) suggest that a religious sense of meaning in life is associated with lower HbA1c scores (β = −.090; b = −.024; p < .01). However, a general sense of meaning in life was not significantly associated with HbA1c values (β = −.040; b = −.008; ns.). Consequently, a religious sense of meaning in life, but not a general sense of meaning was included in the model estimated by PROCESS (Hayes, 2022).
Table 2 contains the results of the OLS models that were included in the PROCESS analyses (Hayes, 2022). The data in the left-hand column contain the relationship between a faith healing beliefs and a religious sense of meaning in life. The results in the right-hand column show the relationship between faith healing beliefs, meaning in life, and HbA1c scores.
Evaluating the Mediating Effect of Religious Meaning in Life (N = 1,319).
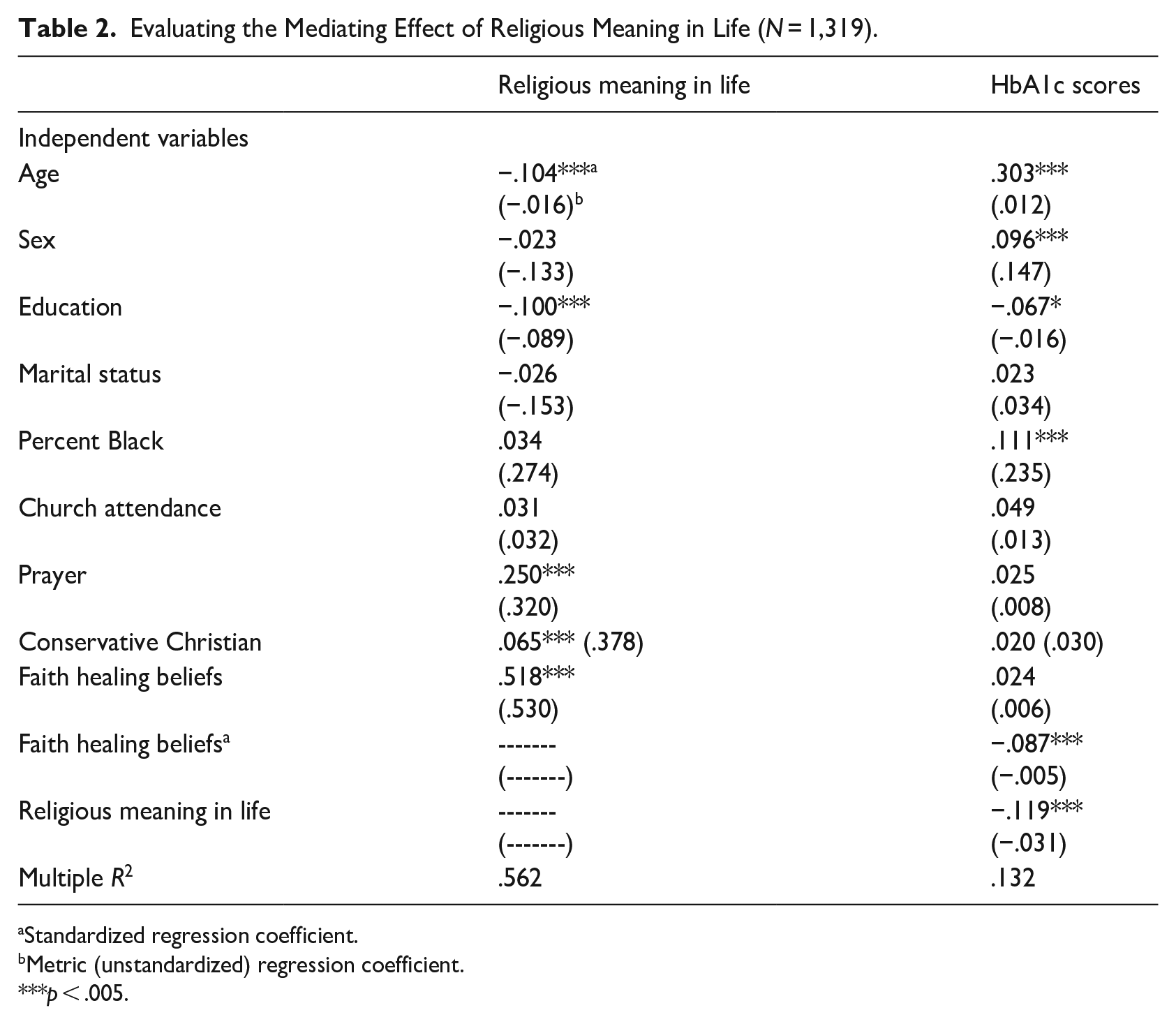
Standardized regression coefficient.
Metric (unstandardized) regression coefficient.
p < .005.
The findings in the left-hand column of Table 2 suggest there is a strong linear relationship between belief in faith healing and a religious sense of meaning in life: stronger beliefs in divine healing are associated with a deeper sense of religious meaning in life (β = .518; p < .001). Two important findings emerge from the data in the right-hand column of Table 2. First, the data indicate that a greater sense of religious meaning in life is associated with lower (i.e., better) HbA1c scores (β = −.119; p < .005). Second, the results reveal that, as reported earlier, there is a nonlinear relationship between belief in faith healing and HbA1c values (β = −.087; b = −.005; p < .005).
The results that have emerged up to this point indicate that stronger faith healing beliefs are associated with a greater religious sense of meaning in life and a religious sense of meaning as well as strong beliefs in divine healing are, in turn, associated with is associated with lower HbA1c scores. The PROCESS (Hayes, 2022) analysis is especially useful at this juncture because it provides an estimate of this indirect (i.e., mediating) effect as well as a test of statistical significance for this coefficient. Data from the PROCESS model (not shown in Table 2) reveal that there is a statistically significant mediating effect of religious meaning in life in the relationship between faith healing beliefs and levels of HbA1c (β = −.043; p < .05).
Conclusion
Although faith healing has been a part of the American religious landscape for over 100 years, relatively few studies have examined this phenomenon empirically with survey data. This is especially true with respect to research on religion and health. The purpose of our study was to explore the relationship between belief in divine healing and HbA1c values. Three blocks of findings emerged from our analyses.
First, a set of descriptive analyses reveal that belief in faith healing is associated with a range of social demographic variables. The results involving affiliation with Conservative Christian denominations are especially noteworthy. The data suggest that contrary to our initial expectations, divine healing beliefs are not the sole province of Conservative Christians. Instead, belief in faith healing is more widely spread across the general population. This appears to be the first time this issue has been empirically examined in the literature.
The second block of findings involve the relationship between belief in divine healing and HbA1c scores. The results reveal that there is a nonlinear relationship between the two. Relatively weak belief in faith healing is associated with higher (i.e., worse) HbA1c levels. However, the sign of this relationship changes as divine health beliefs rise, indicating that belief in divine healing is associated with a decline in HbA1c levels. The tipping point in this relationship suggests that these potential benefits only emerge at fairly intense levels of belief in divine health intervention. This is, to the best of our knowledge, the first time this nonlinear relationship has been evaluated. The fact that we link belief in faith healing with a biomarker of health (HbA1c) is especially noteworthy, because there do not appear to be any studies in the literature that examine this type of health outcome. The fact that these results were generated from a nationwide survey adds further credence to our findings.
The third block of results emerged from a preliminary search for mediators of the link between divine healing beliefs and HbA1c levels. Meaning in life was the focal point of these analyses. The data indicate that a religious sense of meaning in life, but not a general sense of meaning, performs this mediating function. Once again, this appears to be the first time this issue has been explored empirically.
Although our research may have contributed to the literature, a considerable amount of research remains to be done. The logical next step involves delving more deeply into the factors that promote belief in faith healing in the first place. We suspect that the potentially important influence of social relationships that form in religious institutions may be especially ripe for further inquiry, because the extensive research program by Krause (2008) reveals that social ties with fellow church members shape an incredibly wide array of religious beliefs and practices.
In the process of exploring new ground, researchers should pay careful attention to the limitations in our work. Issues involving the direction of causality are especially important in this respect. Although we find it difficult to argue that levels of HbA1c determine beliefs in divine healing, we cannot rule out the possibility that both faith healing beliefs and HbA1c values are a spurious reflection of other omitted variables. Clearly, a carefully crafted series of longitudinal analyses are needed to address this complex issue.
Although there are shortcomings in our research, we hope the broader themes that emerge from it do not go unnoticed. Chief among them is the century-old debate over mind−body dualism (i.e., the belief that mind and body are separate and distinct entities; for a recent review of this issue see Burgmer & Forstmann, 2018). Cast within the context of our study, this debate suggests that merely believing in a phenomenon, like divine healing, is sufficient to produce measurable changes in body chemistry. This reveals, in turn, that the interface between mind and body is porous. When viewed in this light, our work directly addresses one of the most fundamental questions about human existence and as a result, we found that delving deeply into it has been fascinating.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the John Templeton Foundation (40077).
Data Availability Statement
The data used in this study are available from the first-listed author upon request.