
Abstract
Employees of faith-based international organizations have been shown to be uniquely at risk for mental health symptoms, including depression and posttraumatic stress, while social support has been demonstrated to be an important protective factor. Cultural humility, which is understood as an openness to appreciate and learn from others, has also been shown to contribute to wellbeing for cross-cultural employees. Eighty-eight cross-cultural faith-based workers completed the Hopkins Symptom Checklist, Social Provisions Scale, and Cultural Humility Scale as a part of a larger needs assessment conducted in late 2020 during the global COVID-19 pandemic. It was hypothesized that social support would relate inversely to mental health symptoms, and that cultural humility would moderate the relationship between support and symptoms. Path analysis confirmed this hypothesis. When participants reported moderate to high levels of cultural humility, there was a strengthened relationship between social support and lower mental health symptoms. Thus, cultural humility appears to activate the relationship between social support and reduced mental health symptoms. International organizations can contribute to employee resilience in traumatic contexts by promoting both cultural humility and social support.
Keywords
Faith-based nonprofits are religious organizations that work to promote holistic development both locally and internationally. Cross-cultural ministry workers are employees of faith-based nonprofits who work outside of their country of citizenship. While these workers may be sent on teams with others from a similar cultural background, their primary work involves daily cross-cultural interactions with national colleagues and depends on ongoing partnership with those from a variety of cultural backgrounds. Their work can include medical care in under-resourced settings, education and training, community development, aid work, church development, and pastoral care. Cross-cultural ministry workers face unique challenges, stressors, and benefits, including risks for mental health symptomology and potential for personal growth (Eriksson et al., 2015; Rosenbusch et al., 2015). Cross-cultural aid workers particularly have been shown to develop adaptive qualities when living under threat outside of their home cultures (Leder, 2019).
Risks for cross-cultural workers
Though cross-cultural ministry workers demonstrate adaptability, the complex nature of their work can put them at risk for mental health symptomology. For example, career health care ministry workers have been shown to be at risk for depression and anxiety symptoms (Strand et al., 2015). International aid workers have also been shown to be at risk for depression symptoms when exposed to traumatic events (Cardozo et al., 2005). “The challenges of aid work may also create internal consequences: depression, hopelessness, posttraumatic reactions, and/or work-related burnout” (Eriksson et al., 2009, p. 671). Given the potential mental health risks for cross-cultural ministry workers, factors contributing to wellbeing and resilience should also be considered. To more fully understand the experience of cross-cultural ministry workers, it is also important to understand depression and anxiety symptomology.
Anxiety and depression are two related but distinct mental health constructs. Early research on depression and anxiety indicated that anxiety and depression should be considered distinctly, but also considered as connected mental health experiences (Clark & Watson, 1991). More recent studies have demonstrated the importance of examining anxiety and depression symptomology as bifactors related to mood and mental health (Simms et al., 2008). Ongoing research has emphasized the frequent comorbidity of anxiety and depression symptoms (Simms et al., 2012). At times, stressors can increase the risk for anxiety and depression symptoms, and the outbreak of COVID-19 was a global stressor that impacted cross-cultural workers.
In late 2019, an outbreak of a new coronavirus (COVID-19) began to spread around the world (Xiang et al., 2020). Public health experts predicted potentially detrimental mental health outcomes for those impacted by COVID-19, and called for a response from the mental health care community (Xiang et al., 2020). Research has begun to emerge showing that COVID-19 has measurably increased anxiety and depression symptoms among certain populations (Bäuerle et al., 2020). In the past, research on cross-cultural workers and aid workers has looked at experiences of potentially traumatic experiences in a particular geographic location (i.e., places impacted by war, poverty, or a specific disease outbreak). COVID-19 uniquely impacted cross-cultural workers around the world. Although the experience varied widely around the world, COVID-19 had a global impact, thus creating a unique moment when cross-cultural ministry workers around the globe experienced a new shared stressor that could have increased their risk for anxiety or depression. Although cross-cultural ministry workers have been shown to be at risk for anxiety and depression symptoms, there are also factors that may be protective factors for ministry workers even in the midst of challenging circumstances.
Resources for wellbeing
Social support is one important factor in wellbeing. Social support, which is understood as felt support from other people, has been shown to be beneficial to overall wellbeing both by being directly beneficial and by serving as a buffer against stressful experiences (Cohen & Wills, 1985). Social support is understood both as a resource and a process that contributes to individuals’ experience of wellbeing (Hobfoll & Freedy, 1990). People who report experienced social support tend to report lower levels of depression and anxiety symptoms. Expatriate workers who report higher levels of felt social support have also been shown to experience lower levels of depression symptoms (Eriksson et al., 2013). Social support has also been shown to relate to decreased mental health symptomology, including burnout and secondary traumatic stress, specifically among ministry workers employed as chaplains (Galek et al., 2011). Cross-cultural workers have unique challenges in building and maintaining social support networks because they have relocated from their country of origin and the natural support networks found in that context; conversely, cross-cultural workers also have the unique opportunity to build diverse social support networks both in their country of origin and in their place of employment. To cultivate expanding social support networks, cross-cultural workers will need skills for building relationships in new contexts while living cross-culturally.
Another factor that may contribute to experienced wellbeing in cross-cultural interactions is cultural humility (Paine et al., 2016). Cultural humility is a concept related to an individual’s openness to learn from and appreciate others with different cultural backgrounds, practices, and values. Cultural humility also includes a willingness to see one’s self and one’s cultural background in an honest way. Cultural humility is a construct understood within the larger concept of humility, which is defined as, “an interpersonal characteristic that emerges in social contexts that connotes (a) a manifested willingness to view oneself accurately, (b) a displayed appreciation of others’ strengths and contributions, and (c) teachability” (Owens et al., 2013, p. 1518). Humility has been shown to correlate positively with cross-cultural competence (Paine et al., 2016). Cultural humility has been shown to be inversely related to “prejudicial attitudes (and) perceived real and symbolic threat” specifically for American citizens expressing perspectives on Syrian refugees (Captari et al., 2019, p. 124). Cultural humility has been shown to predict less discrimination toward diverse populations (in this case, conservative Christians in the United States who demonstrated cultural humility also demonstrated less discrimination toward members of the LGBTQ+ population; Choe et al., 2019, p. 176). Although cultural humility has been examined from a more individualist perspective (i.e., looking at an individual’s cultural humility), there is emerging research within psychology that also considers the impact of perceived group cultural humility within group therapy settings (Kivlighan et al., 2019). This research explored the importance of perceived group humility for the effectiveness of the group itself. In addition, the research of Mosher and colleagues (2019) has explored implications of perceived cultural humility of religious groups instead of examining individual cultural humility.
Cultural humility is a factor in experiencing social support, particularly in cross-cultural relationships. There has been research indicating that cultural humility influences the way expatriate workers engage with social support (Caligiuri et al., 2016). “Expatriates higher in cultural humility benefit more from a supportive host national work environment to facilitate better performance” (Caligiuri et al., 2016, p. 10). Thus, cultural humility is related to experienced social support between expatriate employees and national employees. Cultural humility was shown to relate positively with relational satisfaction and commitment and negatively relate to ineffective arguing for interethnic couples while perceptions of a partner’s cultural humility is a mediating factor in the relationship between ineffective arguing and relational satisfaction (McElroy-Heltzel et al., 2018). This suggests that cultural humility plays a role in experienced social support in intimate cross-cultural relationships and may lead to increased experienced wellbeing.
While the influence of cultural humility on interpersonal relationships and work performance has been considered, little research exists evaluating the relationship between an individual’s experienced team cultural humility and mental health symptomology. Previous studies have explored the relationship between social support and depression and anxiety symptoms, particularly for cross-cultural workers (Eriksson et al., 2009). Given the unique impact of social isolation and restricted travel during COVID-19, there is a need for research exploring the relationship between felt social support and depression/anxiety symptoms for cross-cultural ministry workers during a time of global isolation. Previous studies have examined the relationship between cultural humility and interpersonal/social factors such as attitudes toward others, cross-cultural competence and work competence (Captari et al., 2019; Choe et al., 2019; Paine et al., 2016). Given the impact of felt social support on mental health symptomology and given the relationship between cultural humility and cross-cultural competence and positive relationships (Owens et al., 2013), there is a need to explore the relationship between cultural humility and depression/anxiety symptoms.
The present study
The aims of the current study are to explore the relationship between mental health symptomology (anxiety/depression), social support, and cultural humility among cross-cultural ministry workers during the COVID-19 global pandemic. First, based on past work by Eriksson and colleagues (2009), it was hypothesized that social support will have an inverse relationship with depression and anxiety symptoms. Second, building on previous work on cultural humility of religious communities, it was hypothesized that perceived team cultural humility will have an inverse relationship with depression and anxiety symptoms (Mosher et al., 2019). Third, drawing from Caligiuri and colleagues (2016), it was hypothesized that there will be an interaction effect between social support and cultural humility in relation to depression and anxiety symptoms for cross-cultural ministry workers during COVID-19. Specifically, it was hypothesized that benefits of felt social support on depression and anxiety symptoms would be strengthened in individuals who also reported high levels of experienced cultural humility.
Method
Participants
The present study includes 88 adult cross-cultural ministry workers employed by a Christian nonprofit organization that focuses on church-based work, community development, medical care, creative arts, and business development (see Table 1). A total of 48% of participants were between the ages of 35 and 44 years. The majority (94%) identified as white; 35 participants identified as male and 53 identified as female. Participants were working in a variety of geographic locations, including North Africa, sub-Saharan Africa, Europe, Asia, and South/Central America. Thirteen participants reported leaving their geographic area of residency due to COVID-19. The majority were married and had children. They worked in a variety of areas including healthcare, community development, education, church-based work, the arts, and business. About half of the participants (55%) reported also having a leadership role within their nonprofit organization. Organizationally, COVID policies sought to offer flexibility and support tailored to individual needs during the pandemic; there was not a universal policy regarding staying or leaving the country of service. However, ongoing changes in international insurance policies during the time of the survey meant that employees risked losing medical insurance coverage for COVID-related illness in their country of service if they made more than one trip to the United States during the pandemic or if they traveled to other countries outside of their country of service.
Demographic Information of Study Sample.
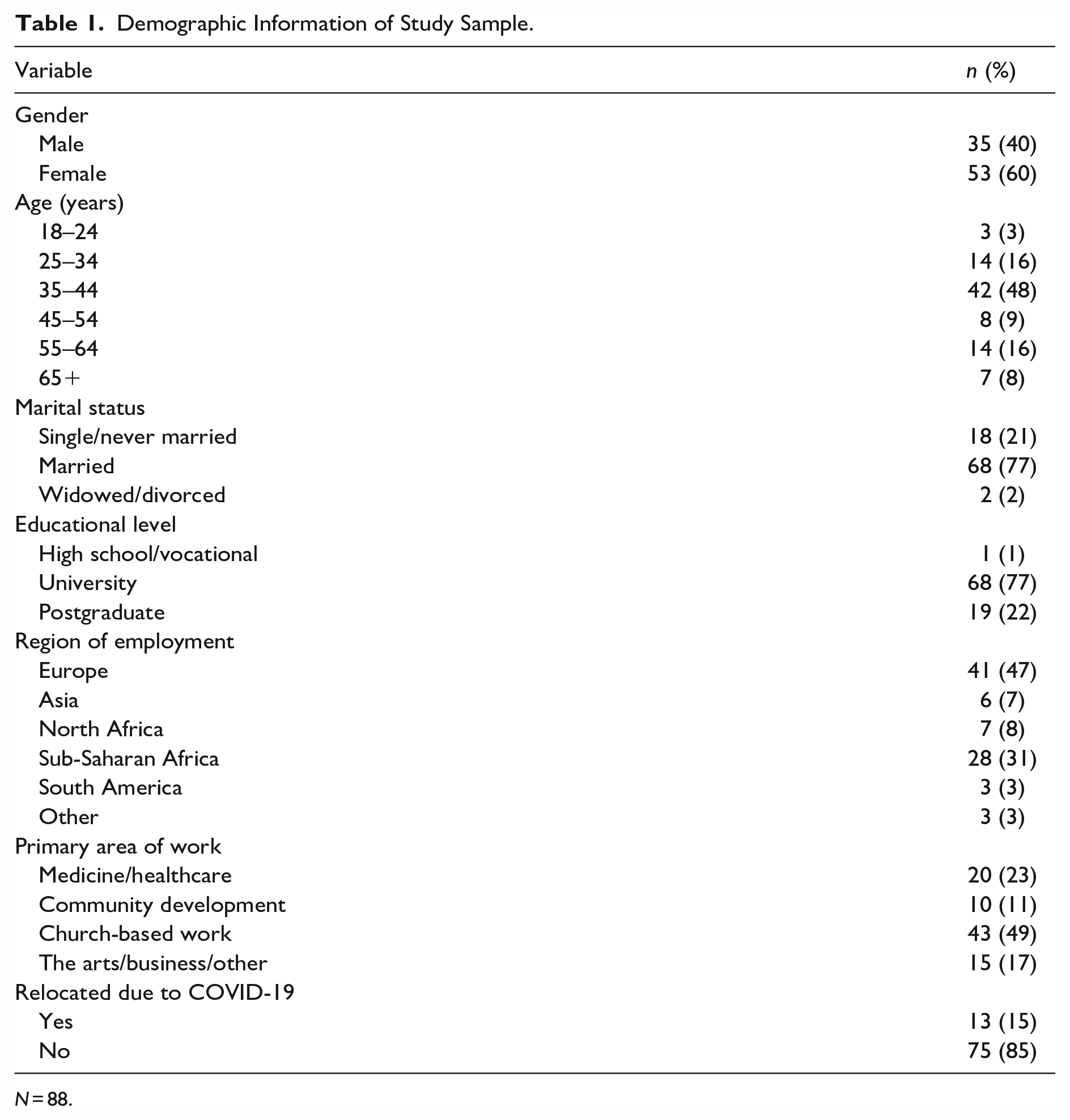
N = 88.
Procedure
Participants were recruited as a part of a needs assessment project for a faith-based international nonprofit organization. All participants were cross-cultural ministry workers who were employed by the nonprofit that was participating in the needs assessment. While the participants were all employees of one faith-based organization originating from the United States, all engaged in cross-cultural interactions as a part of their work. Similar to other research on cross-cultural employment (Caligiuri et al., 2016), all participants were expatriates whose jobs included working cross-culturally with nationals. Participants received e-mail and social media communication about the research project. This communication was distributed by the Human Resources (HR) department of the nonprofit that was participating in the needs assessment. The HR department ensured that all employees receiving the e-mail were eligible for inclusion due to being full-time employees of the organization whose job included living cross-culturally outside of the United States. Members of the organization whose job was based in the United States were not included in the survey. The international nonprofit organization’s leadership team and member care department reviewed the materials prior to participant recruitment and survey distribution.
Participants were asked to engage with a survey to inform their employer of felt needs and experienced resources in the context of COVID-19. Participants were informed that there would be no financial compensation for participation, but that de-identified data would be used to inform their employer of the needs of employees during COVID-19. Participants were also informed that the data would be used to contribute to the larger body of research related to risk and resilience factors influencing cross-cultural workers. Participants were informed of potential risks of taking the survey, and were told that the survey was optional, and completed an informed consent document prior to beginning the survey.
The survey measure was a self-report survey that combined various rating scales and written narrative responses. The survey was administered through Qualtrics. The link to the survey was delivered to participants via company e-mail addresses, and participants were given 4 weeks to complete the survey between early November and early December 2020. In all, 228 e-mails were sent out, and 105 surveys were completed or partially completed.
Measures
Depression and anxiety
The Hopkins Symptom Checklist (HSCL; Derogatis et al., 1974) was used to assess for symptoms of anxiety and depression. The HSCL is a screening measure including 10 questions related to anxiety symptoms (e.g., “how much has feeling fearful bothered you in the last month”) and 15 questions related to depression symptoms (e.g., “how much has feeling lonely bothered you in the last month”). The HSCL is rated on a 4-point scale ranging from 1 (not at all) to 4 (extremely). Internal reliability for the combined, overall score for the current study was .89. Other studies using the HSCL have demonstrated reliability and validity, with a good internal consistency (α = .90; Lee et al., 2008).
Social support
Social Provisions Scale (Cutrona, 1989; Cutrona & Russell, 1987) is a 12-item scale that assesses participants’ experience of perceived social support (Cutrona, 1989; Cutrona & Russell, 1987). Participants rate their experience of support in the areas of “attachment, social integration, reassurance of worth, reliable assistance, guidance, and opportunity for nurturance’’ (Cutrona & Russell, 1987, p. 49). Responses are given on a 5-point scale (1 = strongly disagree, 5 = strongly agree). Based on previous studies, the scale was adapted to include a midpoint of 3 (unsure; Eriksson et al., 2009). The internal reliability for the current study was .84. Previous studies have demonstrated internal reliability and validity for the measure (α = .79; Eriksson et al., 2009).
Cultural humility
Cultural Humility Scale (CHS; Hook et al., 2013) is a 12-item measure that was used to assess perceptions of cultural humility. Seven of the items relate to positive aspects of cultural humility, and five of the items relate to negative aspects of cultural humility. The CHS items were modified to assess perceptions of cultural humility in a cross-cultural team. Sample items include, “My team asks questions when uncertain,” and “My team is genuinely interested in learning more.” Responses are given on a 5-point scale (1 = strongly disagree, 3 = neutral, 5 = strongly agree). The Cronbach’s alpha for the present study is .88. Previous studies have demonstrated strong validity and internal consistency, with a recent study demonstrating a Cronbach’s alpha of .93 (Mosher et al., 2019).
Results
After distributing the survey to 228 individuals in early November 2020, 105 participants began the survey. Ten people did not complete the informed consent page, six people did not complete any of the survey questions (i.e., only completed the demographics section), and one individual did not complete the social support or cultural humility measures. After the respondents who failed to complete more than 5% of the survey items were removed, 88 participants remained. This means that approximately 46% of those who received the survey attempted to start it, and 39% completed the survey. This response rate was considered sufficient given organizational emphasis on the voluntary nature of the survey and the fact that all applicable geographic regions, age ranges, and years of employment were represented by respondents. All of these remaining participants answered 100% of the survey questions, meaning no item replacement was necessary for this analysis. In the sample, 13 (15%) needed to relocate due to COVID-19 and 75 remained in their field of service. A univariate ANOVA did not demonstrate a distinct difference of distress or felt social support between the groups (HSCL: F [1, 87] = 2.73, p = .102; Social Provisions Scale: F [1, 87] = 0.47, p = .495).
Table 2 includes the means and standard deviations for study variables along with correlations between variables. The mean score on the HSCL was 1.71, which was higher than in previous similar studies conducted with cross-cultural workers (Eriksson et al., 2009) and indicates that participants were generally reporting some distress for each item. The mean score on the Social Provisions Scale was 4.39, indicating that participants generally reported accessing social support. The mean score on the CHS was 3.75, indicating that participants generally perceived their team as demonstrating cultural humility. As expected, intercorrelations showed that perceived social support was negatively and significantly correlated with mental health symptoms (r = −.26, p < .05). Thus, cross-cultural ministry workers who experience higher levels of social support during COVID-19 also experience lower levels of depression and anxiety. Second, contrary to the original hypothesis, the correlation between mental health symptoms and cultural humility was not significant. Finally, social support and perceived team cultural humility were shown to be significantly correlated (r = .35, p < .01; see Table 2).
Means, Standards Deviations, and Correlations of Study Variables.
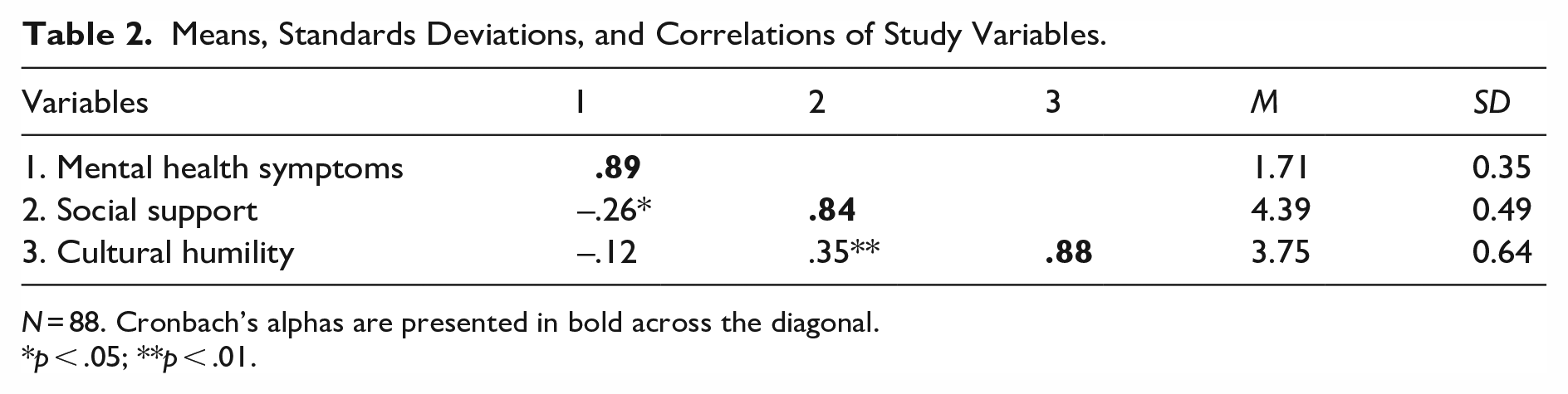
N = 88. Cronbach’s alphas are presented in bold across the diagonal.
p < .05; **p < .01.
A hierarchical linear regression analysis was conducted to examine the relationship between mental health symptoms, social support, and cultural humility while controlling for gender and age. B, SEB, and β for each predictor at each step of the equation are presented in Table 3. Age and gender were entered into the first step of the regression. The overall model for step one was significant, R2 = .17, F(2, 85) = 9.94, p < .001. Age was significantly associated with mental health symptoms (β = −.38, p < .001), indicating that younger age was related to higher symptoms. Gender was marginally, but not significantly, associated with anxiety and depression symptoms (β = .19, p = .06) with males trending to report higher symptoms. In the second step, social support was entered into the model resulting in a significant change in R2, ΔR2 = .04, F(1, 84) = 4.84, p < .05. This significant change in R2 was anticipated by the original hypothesis. However, in the third step, cultural humility was entered into the model. Contrary to the original hypothesis, adding cultural humility to the model did not result in a significant increase in R2, even when controlling for other study variables.
A Hierarchical Multiple Regression Analysis Predicting Mental Health Symptoms from Gender, Age, Social Support, and Cultural Humility.
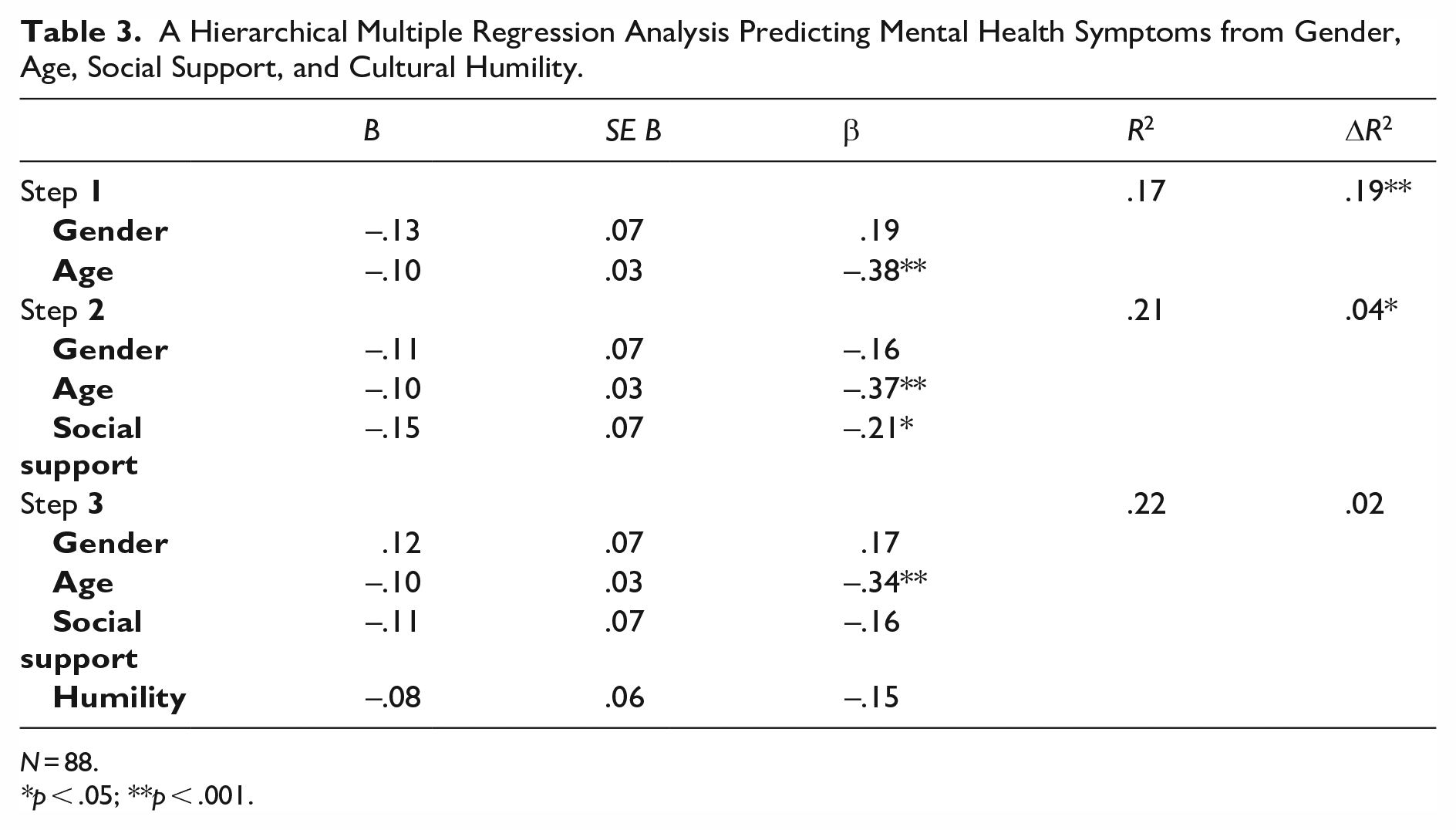
N = 88.
p < .05; **p < .001.
A moderation analysis was then conducted to examine the extent to which the relationship between social support and mental health symptoms was impacted by experienced team cultural humility. This analysis was run using the Statistical Package for the Social Sciences (SPSS) macro, PROCESS (Hayes, 2012). PROCESS also provides conditional effects of the dependent variable on the independent variable at multiple levels of the moderator, which assists in creating interaction plots necessary to understand the moderating relationship.
Results of the current analyses revealed that, while controlling for age and gender, cultural humility moderated the relationship between mental health symptoms and social support (β = −0.33, p = .003, 95% CI = [−.547, −.113]). As shown in Figure 1, when participants reported low levels of cultural humility, there is a nonsignificant relationship between social support and mental health symptoms, (β = −.07, p = .476, 95% CI = [−0.27, 0.13],). When participants endorsed high levels of team cultural humility, there is a significant inverse relationship between mental health symptoms and social support (β = −.59, 95% CI = [−.90, −.27], p < .001). Thus, consistent with our hypothesis, perceived team cultural humility moderated the relationship between perceived social support and mental health symptoms. When experienced team cultural humility was high, the relationship between felt social support and lower mental health symptomology was strengthened; when the experienced team cultural humility was low, there was no significant relationship between felt social support and mental health symptoms.
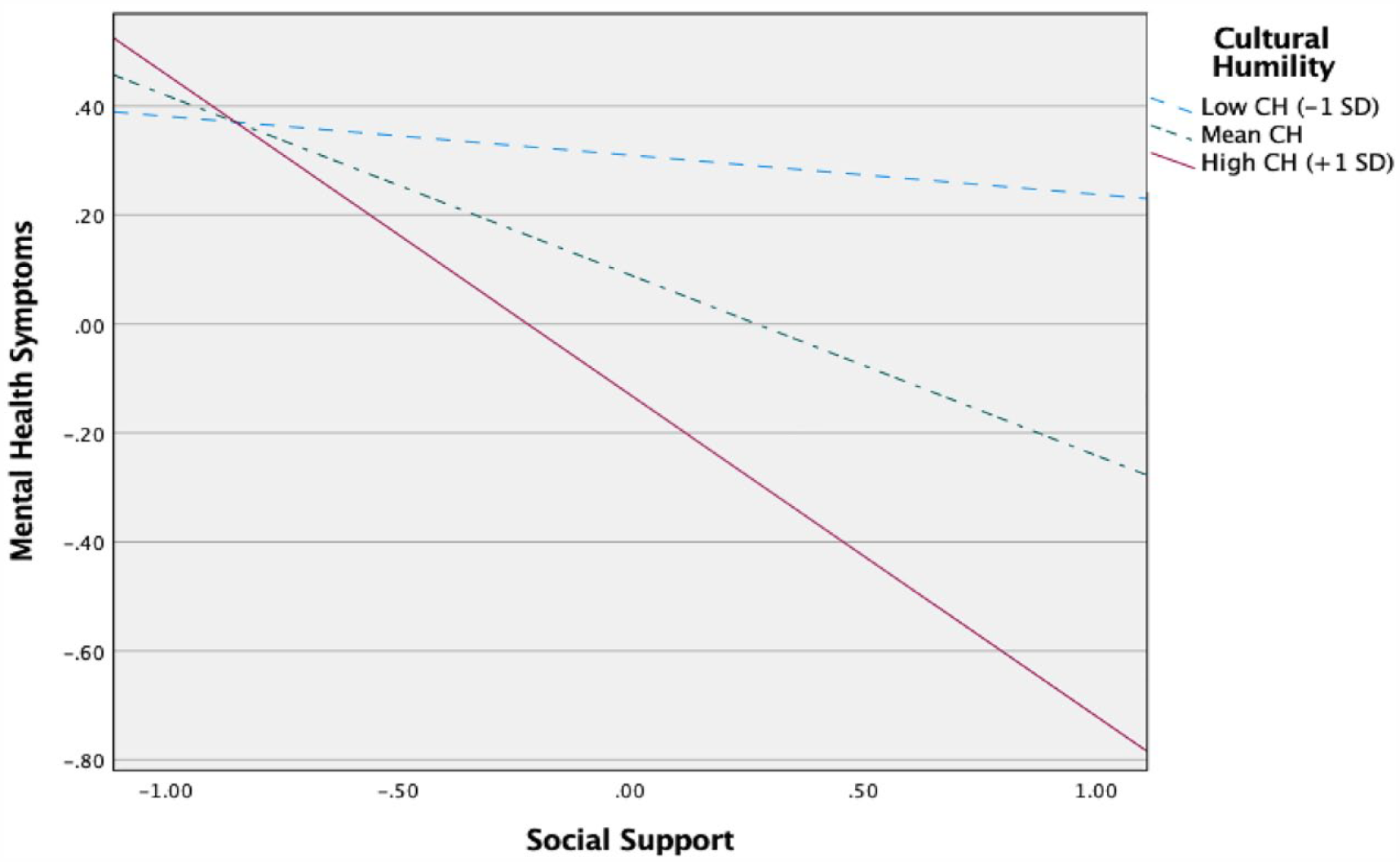
The impact of cultural humility on the relationship between social support and mental health symptoms.
Discussion
The present study considers the relationships between social support, perceived team cultural humility, and mental health symptoms for cross-cultural ministry workers during COVID-19. Given the potential challenges of accessing social support in a cross-cultural setting, this study also investigates the influence of team cultural humility on mental health symptoms (Bäuerle et al., 2020; Pfefferbaum & North, 2020). Although the relationship between social support and mental health symptoms has been established, the role of team cultural humility related to mental health symptoms had not yet been explored. In light of cultural humility’s impact on accessing social support, this study explores whether cultural humility directly relates to mental health symptoms and whether perceived team cultural humility moderates the relationship between experienced social support and mental health symptoms.
In the course of this study, three important findings emerged. First, the study findings suggest that cross-cultural ministry workers who experience higher levels of social support during COVID-19 also experience lower levels of depression and anxiety. This is consistent with previous research that has shown that cross-cultural workers who experience social support report lower levels of mental health symptomology (Eriksson et al., 2009; Galek et al., 2011). This is also aligned with previous research that has shown cross-cultural ministry workers are at risk for mental health symptomology but also have unique opportunities for growth (Eriksson et al., 2015; Rosenbusch et al., 2015). Specifically, this study examines social support as a concept related to experiences of emotional closeness, shared social activities, offered guidance, and giving and receiving help when needed. This type of social support is particularly important during a global pandemic when isolation, political uncertainty, and health risks all may increase the felt need for support from others. In this study, experienced social support relates to lower reported symptoms of depression and anxiety symptoms for those living cross-culturally in the midst of a pandemic. Potentially, social support could serve as a protective factor for those at risk of mental health symptomology. It is also possible that a person who is depressed or anxious may become more withdrawn from social relationships and thus may have more difficulty accessing social support.
Second, the study suggests that cross-cultural workers’ experienced team cultural humility does not directly significantly impact mental health symptoms during COVID-19, thus disproving the second hypothesis. Previous research has established the relationship between mental health symptoms and social support while highlighting a relationship between social support to cultural humility (Caligiuri et al., 2016; Paine et al., 2016). However, it appears that, for cross-cultural ministry workers during COVID-19, perceived team cultural humility does not account for a change in mental health symptoms apart from the impact of social support on mental health symptoms. This may be because an individual could potentially experience team cultural humility, but other factors may inhibit the strength of or opportunity for cross-cultural relationships or one’s experience of mental health symptoms (i.e., lack of language fluency, isolation from cross-cultural relationships due to COVID-19, a history of depression or anxiety symptoms). As the third hypothesis will demonstrate, the relationship between social support and mental health symptoms instead seems to be impacted by the level of perceived team cultural humility.
Third, cultural humility significantly moderated the relationship between social support and mental health symptoms for cross-cultural ministry workers. When cross-cultural workers reported low levels of cultural humility in their teams, there was no significant relationship between social support and mental health symptoms. However, when cross-cultural workers reported high levels of experienced team cultural humility, social support was significantly related to lower levels of reported mental health symptoms. The current study suggests that experienced team cultural humility activates the relationship between mental health and social support, allowing individuals to access the mental health benefits of social support. Thus, individuals who reported high levels of both team cultural humility and social support experienced lower levels of depression and anxiety symptoms. This supports previous research which demonstrated the relationship between social support and cultural humility along with research that demonstrated the relationship between social support and mental health symptoms (Caligiuri et al., 2016; Eriksson et al., 2009).
Since cross-cultural ministry workers are living outside of their home cultures, building cross-cultural relationships is an important component of both their work and personal lives. Team cultural humility, which includes an openness to learn from other cultures, may impact a cross-cultural worker’s ability to access social support (Caligiuri et al., 2016). Thus, cultural humility may increase the quality of supportive relationships for expatriates. Cultural humility has been shown to positively correlate with cross-cultural competence, to be inversely related to feeling threatened by those of other cultures, and to be related to experienced social support (Captari et al., 2019; Choe et al., 2019; Paine et al., 2016).
Cultural humility is a factor connected to an individual’s openness to learn from those from other religious and cultural backgrounds. This perspective of perceived openness and curiosity within a team may enable individuals to receive help and support from those who are culturally different while also reflecting an openness to consider challenges from different cultural perspectives. When an individual experiences that their cross-cultural team is interacting in a culturally receptive way, this attitude toward others may activate the capacity to receive social support from those who are culturally different. It would be particularly important for individuals living through challenges in a cross-cultural setting to be able to access social support from those outside of their home culture, and cultural humility may be a factor that activates this capacity. As Caligiuri et al. (2016) discussed, cultural humility is a factor that influences an expatriate’s ability to receive support from those who are culturally different, which in turn seems to increase work productivity and satisfaction. Thus, access to social support may influence mood, which in turn may influence job and life satisfaction.
It is important to note that this research was collected between Nov. 1 and Dec. 31, 2020. This was in the first year of the COVID-19 pandemic prior to wide distribution of vaccines and also during a time of political transition and unrest in the United States (Pfefferbaum & North, 2020). Data are beginning to emerge about the impact of COVID-19 on mental health symptomology, but there is much that is unknown. Historically, research has shown that experiences in quarantine often relate to increased anxiety and depression symptoms for those who are quarantined as well as caregivers and healthcare workers (Hossain et al., 2020). While the ongoing risks and losses associated with COVID-19 likely impacted the mental health symptoms of participants, it is as yet unclear in what ways COVID-19 has impacted mental health. A normed cutoff of 1.75 has been indicative of elevated depression or anxiety (Cardozo et al., 2012; Coyne et al., 2000), and the average reported HSCL-25 scores (M = 1.71) in this sample indicated elevated depression or anxiety symptoms. These scores are also higher than in previous similar studies conducted with cross-cultural workers (Eriksson et al., 2009), suggesting the unique stress and strain of the pandemic. Yet, even in the context of COVID-19, this study shows that team cultural humility may strengthen an individual’s perception of social support which then relates to lower levels of anxiety and depression symptoms.
Limitations
This study has several limitations. First, a small sample size and somewhat homogeneous group (only one participant had not completed college, and 94% were white) mean the findings may not be particularly generalizable beyond the participating organization. The experience of white Americans living outside of the United States is likely different from those of other racial and ethnic groups, and so both cultural humility and social support may be perceived differently by individuals from different cultural backgrounds. Similarly, openness to difference and ability to access support resources may be expressed differently by those from different educational backgrounds. A more diverse sample could reveal differences in the impact of cultural humility for those who are not white or those who are not college educated.
Similarly, the participants were limited to the employees of one organization and participating in the survey was optional for employees. Since the participants were limited to one employer, it is possible that the participants represent particular values connected to social support or cultural humility which may not be shared by employees from other organizations involved in cross-cultural work. Thus, the study is limited by only relying on self-reports of individuals from one organization who opted to complete the survey.
Finally, all of the measures are self-reported. Specifically, the cultural humility measure represents the cross-cultural ministry worker’s perception of a ministry team’s cultural humility but does not include any other measures of cultural humility. For those working cross-culturally, there may be a strong desire to be perceived as culturally competent or as open to others; the social desirability of being culturally competent may lead to a bias in reporting cultural humility. Another factor impacting the self-reporting of cultural humility is that this survey was administered between 1 November and 31 December 2020, during a time of political unrest in the United States due to racial and cultural injustice. There is the potential that some participants had more awareness of their own cultural bias, and so reported cultural humility in a different way due to growing awareness of cultural and racial divides around the world. While not a limitation, the specific context of the survey administration is notable when considering ongoing research into the relationship between social support, cultural humility, and mental health symptoms.
Clinical applications
Overall, the hypothesis that social support relates to mental health symptoms was supported. Conversely, the hypothesis that cultural humility would relate significantly to mental health symptomology was not supported. However, the hypothesis that cultural humility would impact the relationship between mental health symptoms and social support was supported. Moderate and high levels of perceived team cultural humility were shown to strengthen social support’s relationship with lower reported levels of anxiety and depression.
There are several applications of the findings of this study. One particular application is for employers of those working cross-culturally. These employers should consider assessing for cultural humility and providing training to promote team cultural humility for those employed in cross-cultural ministry work. It should not be assumed that an employee who seeks to work cross-culturally has already developed cultural humility, and the importance of team cultural humility should be considered. Caligiuri and colleagues (2016) suggest that companies use interviews and validated assessment measures to assess for candidates’ levels of cultural humility before they are employed as cross-cultural workers. They suggest that the results of the assessments be shared with employees before they are sent to work in a cross-cultural situation to promote dialogue and insight. For employers who hope to promote greater mental health among employees working cross-culturally, factors related to strengthening team cultural humility and experienced social support should also be considered. Thus, organizational policies that support building team relationships and maintaining communication with friends and family in their country of origin may be important for the flourishing of cross-cultural workers (Cardozo et al., 2012). Research has shown that both emotional and instrumental (i.e., information or “tangible needs”) social support from cross-cultural colleagues is important for cross-cultural workers, so organizations should consider prioritizing team work and trainings that incorporate those in the local community in addition to cultivating support from teammates and loved ones from their country of origin (Caligiuri et al., 2016, p. 6).
Another application is for mental health practitioners working with cross-cultural ministry workers. Mental health practitioners should consider social support and team or organizational cultural humility factors when treating clients with mental health symptomology. When considering interventions to support cross-cultural ministry workers, clinicians should seek to offer culturally informed care to promote cultural humility in clients and to more fully understand the factors that may be influencing mental health symptoms. There also may need to be a particular focus on what cross-cultural relationships are like for a cross-cultural ministry worker who is experiencing depression or anxiety symptoms. For example, clinician could explore how teams handled conflict, differing perspectives, and value differences within the team and throughout the community. Clinicians could consider the cultural and communal implications of psychosocial stressors faced by the client, and explore how the team’s values impacted the client’s experience of psychosocial stressors. This would allow the clinician to address factors of cultural humility and experienced social support that have been shown to relate to reduced anxiety and depression symptoms.
Future directions
Future research could expand to other types of cross-cultural workers and could also consider these same research questions for cross-cultural workers after the COVID-19 pandemic is over. Longitudinal research that assessed cross-cultural workers prior to deployment, during deployment, and after deployment could also add to the body of knowledge about the relationships between social support, cultural humility, and mental health symptoms. Further research into the experience of other immigrant groups, including those who relocate for educational, economic, or relational reasons, could expand understandings of the relationship between mental health symptoms, social support, and cultural humility for those living outside of their home cultures.
Conclusion
The present study demonstrates that social support relates to reduced mental health symptoms for cross-cultural ministry workers in the midst of COVID-19, and that the presence of cultural humility activates the benefits of social support. Cultural humility appears to have facilitated cross-cultural ministry workers’ ability to access social support, which in turn relates to reduced mental health symptoms. While this study is limited by the sample size, self-report measures, and participants representing only one organization; the results still enrich understandings of the cross-cultural connection and support, particularly during challenging times. Future research can continue to explore ways cultural humility allows individuals and groups to connect across cultures, and the factors that contribute to reduced mental health symptoms for those living cross-culturally.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.