
Abstract
People who use substances are disproportionately affected by both death and nondeath losses and have vulnerabilities that can hinder the processing of the associated grief. While there is an established and growing quantitative research base demonstrating the complexities between grief and substance use, the qualitative literature remains fragmented. This study aims to systematically review the grief experiences of people who use substances to enhance understanding and inform service delivery. A systematic search of four electronic databases identified 18 studies, which were quality assessed using the Critical Appraisal Skills Program. A thematic synthesis was conducted which involved line-by-line coding of findings, development of descriptive themes, and generation of analytical themes. This process identified three themes: Locked in Loss and Addiction, Defeated and Defended, and Routes to Recovery. Findings highlight the reinforcing relationship between grief and substance use, identify grief responses relevant to people who use substances, and offer an aggregated insight into their grieving experiences. This has important implications regarding the integration and provision of grief-informed support in clinical practice.
Introduction
Grief in the context of substance use is attracting increased research attention due to the recognition that people who use substances face complexities in their grieving experience. People who use substances are disproportionately affected by both death and nondeath losses, which is the experience of being deprived of someone or something significant (Abi-Hashem, 1999). People who use substances frequently report estrangement from family members, the removal of children and traumatic deaths of significant others (e.g., overdose, suicide, murder) (Furr et al., 2015; McComish et al., 1999). Research has found experiences related to death and loss are frequently mentioned by people in recovery as a significant aspect of their past (Robak, 1991), and the addiction experience itself is characterized by ongoing and cumulative losses including relationships, jobs and identity (Streifel & Servanty-Seib, 2006). Recovery itself holds the potential of further loss; namely the loss of social networks and substances as a coping strategy (Furr et al., 2015). These findings present loss as being a core characteristic of the addiction experience, and accompanying these losses can be grief, which is the emotional response to a loss (Abi-Hashem, 1999).
Typically, the grief that accompanies death and loss need not be pathologized. It is a universal and normative experience; accompanied by emotional, cognitive, physiological and behavioral changes to functioning which attenuate over time (Worden, 2018). However, research has found that people who use substances face challenges in this process and are significantly more likely to experience complicated grief reactions than those without substance use difficulties (34% vs 5%). This is considered to be due to difficulties in regulating emotions, stigma and limited access to psychosocial buffers (Masferrer et al., 2017; Parisi et al., 2019).
While there is variation in the definition of complicated grief across diagnostic frameworks (e.g., American Psychiatric Association, 2013; World Health Organization [WHO], 2024a), it generally refers to a grief that deviates from the expected course. Unlike typical grief, which gradually lessens over time, complicated grief is characterized by prolonged, intense emotional distress that can interfere with health, social and occupational functioning, and quality of life. It may manifest as chronic and persisting over time, delayed and emerging long after the loss, absent and inhibited or suppressed, or unprocessed and not emotionally integrated (Wilson et al., 2022).
While diagnostic terms, such as complicated grief, can be useful in identifying individuals who may benefit from additional support, labeling grief responses as pathological risks invalidating the lived experience of loss in contexts where grief is already unacknowledged (Granek, 2016). In addition, the term “complicated” grief can also be stigmatizing as it implies a distinction between “normal” and “abnormal” grieving, which may reinforce the othering of those whose grief does not align with expected trajectories (Thieleman et al., 2025). Nevertheless, the increased prevalence of complicated reactions for people who use substances suggests a heightened vulnerability to persistent and debilitating grief responses for this population, requiring research and clinical attention. Additionally, it has been theorized that addressing grief through the recovery process can help individuals process unresolved emotions, reduce relapse risk, and rebuild identity and self-worth (Furr et al., 2015).
Emotion Regulation
For grief to be processed, individuals must attend to and tolerate the intense emotional demands of despair, sadness, guilt, anger and blame (Eisma & Stroebe, 2021; Stroebe & Schut, 2010). This process requires a degree of emotion regulation capacity which is the ability to tolerate, experience, and engage with distressing feelings (Gross, 1998). However, people who use substances are evidenced to have reduced emotion regulation capabilities, often as a consequence of early adverse childhood experiences (Grummitt et al., 2022; Stellern et al., 2023; Weiss et al., 2022). As grief presents as an overwhelming and often intolerable emotional state, people who use substances may turn to, or increase consumption of, substances for immediate and short-term relief from distress within the context of diminished emotion regulation capacities (Baker et al., 2004; Eisma & Stroebe, 2021; Wong et al., 2013). While the use of substances provides temporary relief from painful affective states, it simultaneously impedes upon the cognitive and emotional processing of grief (Caparrós & Masferrer, 2021; Eisma & Stroebe, 2021).
Additionally, people who use substances are more likely to rely upon less helpful coping strategies such as emotional avoidance, social withdrawal, and self-criticism (Caparrós & Masferrer, 2021). While these responses often emerge in the context of stigma, marginalization, trauma, and repeated experiences of social exclusion (Livingston et al., 2012) they have been found to be implicated in the development of complicated grief (Peak et al., 2024).
Stigma
Grief can be further complicated by the stigma surrounding substance use, operating on both micro and macro levels (McNeil, 2021). Goffman (1963) described stigma as an attribution that reduces a person from a “whole and usual person to a tainted, discounted one” (p. 2). Building on this, Link and Phelan (2001) conceptualized stigma as the co-occurrence of labeling, stereotyping, separation, status loss, and discrimination, all of which occur in the context of power. These conceptualizations emphasize stigma as being a social process that leads to exclusion and disadvantage, and in the context of substance use, manifests through moral judgement, social distancing and diminished empathy (Hinshaw & Stier, 2008).
This has been found to lead to a positioning of people who use substances as responsible for their circumstances, rather than individuals navigating complex psychosocial and health challenges (O’Callaghan & Lambert, 2024). This perception can contribute to emotional distress, lower self-esteem and impede upon engagement with treatment and support services (Da Silveira et al., 2018). Structural stigma, including discrimination in healthcare, employment and housing, can reduce access to stabilizing resources such as employment and valued activities (Russinova et al., 2011; Wesselmann & Parris, 2021) that are essential for grief processing and recovery (Stroebe & Schut, 2016). The Dual Process Model (DPM) (Stroebe & Schut, 2010) of coping with grief suggests that adaptive grieving involves oscillation between confronting the emotional experience of loss and engaging in restorative activities that foster recovery. For people who use substances, both aspects of this process are disrupted: stigma, diminished social support, and reliance on less helpful coping strategies (e.g., emotional avoidance, social withdrawal, self-criticism) interfere with the ability to process grief in a way conducive to resolution.
Disenfranchised Grief
Additionally, a significant theme in the addiction literature is that of disenfranchised grief, which occurs when loss is socially invalidated, dismissed, or unacknowledged (Doka, 1989). Over time, this concept has been expanded to reflect the ways in which societal norms and stigma can limit access to mourning rituals, emotional support and acknowledgement of loss (Doka, 2002). In the context of substance use, the associated losses, such as the overdose of significant others or the removal of children, are often perceived as self-inflicted which can reinforce blame, moral judgment and exclusion from traditional grief supports (Feigelman, 2009; Turner & Stauffer, 2023).
From this, there has been a recent research response to the international drug-related death crises, exploring the experience of grieving a stigmatized death (Dyregrov & Selseng, 2022; O’Callaghan & Lambert, 2024). The research has found that grieving individuals experience marginalization from the community which can result in the emotional impact of such losses becoming unacknowledged and can block access to support (Dyregrov & Selseng, 2022; Lambert et al., 2021; O’Callaghan & Lambert, 2024; Titlestad et al., 2021). As such, bereavement following a drug-related death is often shaped by various interactional factors, such as alienation and limited access to support, which can leave individuals stigmatized, unable to express their grief and increasingly isolated (Stout & Fleury-Steiner, 2023). The lack of recognition and tailored support for these grief experiences may drive continued substance use, relapse, and disengagement from services (Duffy & Baldwin, 2013; Schlosser & Hoffer, 2022).
Current Evidence Base
While there is a recent research trend exploring the experience of being bereaved by a drug-related death for people who use substances, the wider research exploring the experience of grief within the context of substance use remains fragmented and lacks comprehensive synthesis. This presents a requirement to systematically review and integrate the available literature to provide an understanding of grief within this population and contribute to a more robust evidence base for this under-researched population. Doing so addresses the gap in the existing knowledge base; and ensures that the complex needs of this vulnerable and stigmatized group are understood and effectively supported.
Aim
The aim of this study is to conduct a systematic review and thematic synthesis of qualitative literature exploring the grief experiences for people who use substances.
Review Question
What are the grief experiences for people who use substances?
Method
Review Development and Registration
The Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) checklist (Tong et al., 2012) was used to guide the review. As per PRISMA guidelines, this systematic review protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) on December 11, 2023 (CRD42023491010).
Search Strategy
Following initial scoping searches, a specialist librarian consulted on the development of a search strategy using the SPIDER framework (Sample, Phenomenon of Interest, Design, Evaluation, Research Type). This was selected due to its applicability to qualitative research (Cooke et al., 2012). The full strategy (Appendix A) incorporated:
Key words related to the sample, for example, addiction, substance use Key words related to the phenomenon of interest, for example, grief, bereavement Key words related to the design, for example, qualitative studies 1 AND 2 AND 3
Four databases (EMBASE, CINAHL, MEDLINE and PsychINFO) were searched from inception until January 9, 2025. Google Scholar was used to complete a forward and backward citation check of eligible studies retrieved from database searches.
Eligibility Criteria
Eligibility criteria were derived from the SPIDER framework.
Inclusion criteria:
Adults (aged 18 years and older). Individuals who either:
Have a diagnosis of substance use disorder. Engage in regular, problematic, or dependent substance use as identified or implied in the study (e.g., descriptions of impaired control, social impairment, risky use or withdrawal effects). Have received addiction treatment. Studies exploring grief experiences in the context of substance use including reactions, help seeking behavior, coping mechanisms, and support experiences. Qualitative studies. Peer-reviewed qualitative or mixed-methods studies where qualitative findings are reported separately.
Studies were excluded on the basis of:
Non-English language publications. Quantitative-only studies. Unpublished, non-peer-reviewed studies. Studies focused on recreational substance use with no indication of problematic use or impact on functioning. Studies focusing on third-party experiences without exploration of the individual with problematic substance use.
Adolescents were excluded as their responses to grief are evidenced to be different than that of adults due to their emotional and cognitive development (Griffin, 2010; Palmer et al., 2016). Recreational substance use refers to the nonhabitual consumption of substances for social or leisure purposes, typically without causing significant harm or impairing daily functioning. In contrast, problematic substance use involves patterns of substance use that lead to negative consequences, such as physical, psychological, or social harm, and often aligns with the diagnostic criteria for substance use disorders (Okruhlica & Sieroslawski, 2006). Alcohol and drug use were included due to the established association with problematic use, psychological distress and functional impairment (Caparrós & Masferrer, 2021).
Only studies with a rigorous qualitative methodology (e.g., thematic analysis, grounded theory, narrative analysis) that provided rich participant data with direct quotes, in-depth theme development, and contextualized experiences within the context of substance use were included. Given the novelty of this research area, unpublished studies (e.g., theses, dissertations) were excluded due to the potential variability in design quality and lack of peer review.
No geographical restrictions were applied.
Study Selection
The process of study selection is shown in Figure 1. Database searches returned 731 articles, which were imported into Rayyan (https://www.rayyan.ai/) to support screening. De-duplication removed 245 articles, and title/abstract screening excluded a further 452. The remaining 34 articles were assessed for eligibility using the exclusion and inclusion criteria. A Trainee Clinical Psychologist, independent to the review, co-reviewed 15% of the articles (n = 5) with CD, achieving 90% inter-rater agreement. Disagreement related to the inclusion of Scott et al. (2017) and pertained to whether the study adequately explored the intersection of grief and substance use. Concurrently, the paper was excluded on the basis that the study's focus was related to participant's interactions with health care providers, as opposed to a detailed analysis of the grieving experience. The final synthesis included 18 studies.
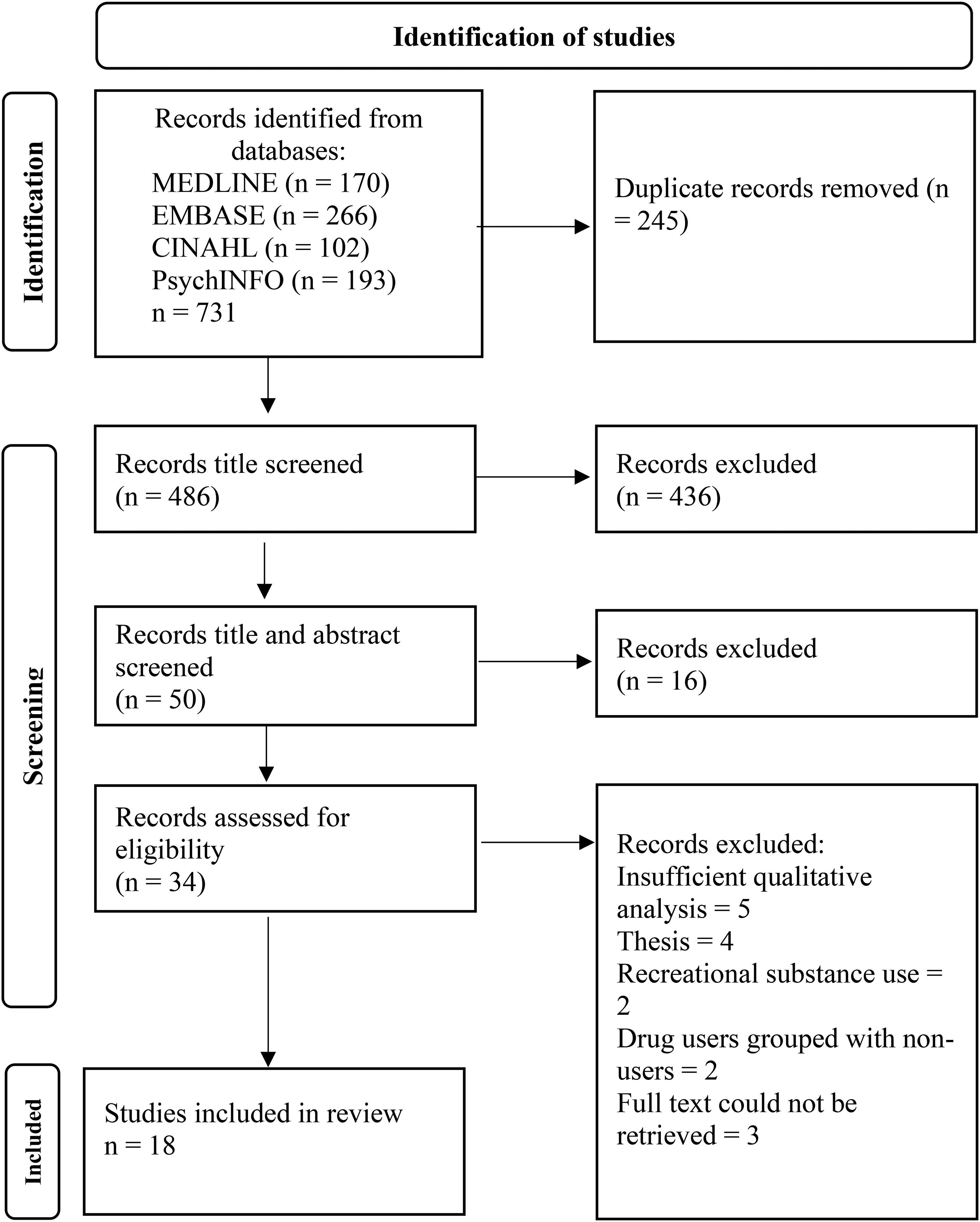
PRISMA flow diagram—process of identification to inclusion.
Data Extraction
A summary of study characteristics of the 18 studies is provided in Table 1.
Study and Participant Characteristics.
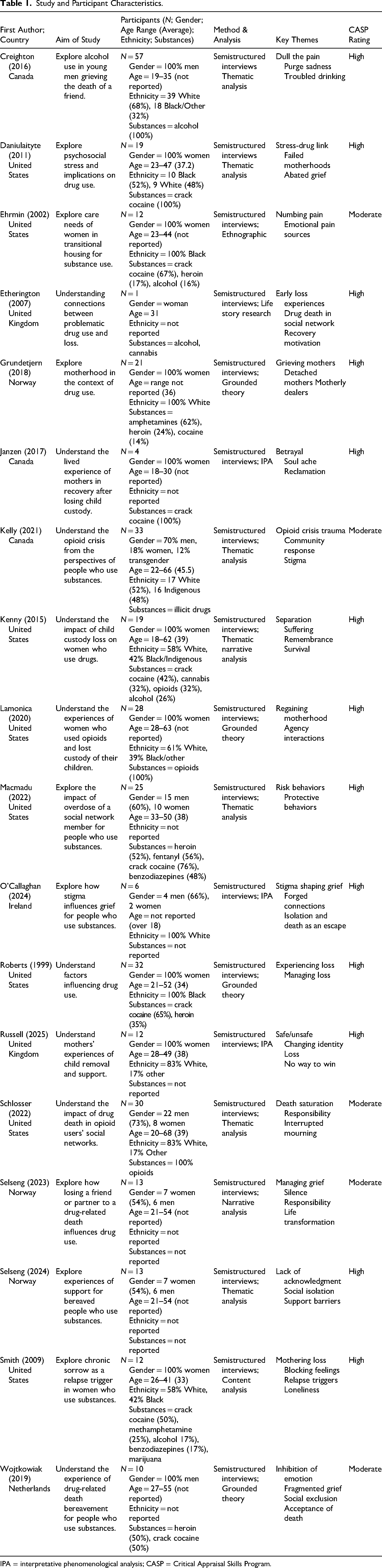
IPA = interpretative phenomenological analysis; CASP = Critical Appraisal Skills Program.
Quality Appraisal Process
The Critical Appraisal Skills Program (CASP) qualitative checklist (2024) was used to assess quality of the included studies due to its suitability for novice researchers completing qualitative research within health and social care (Long et al., 2020; Nadelson & Nadelson, 2014). The CASP evaluates study validity, quality, and relevance to practice and research using 10 questions.
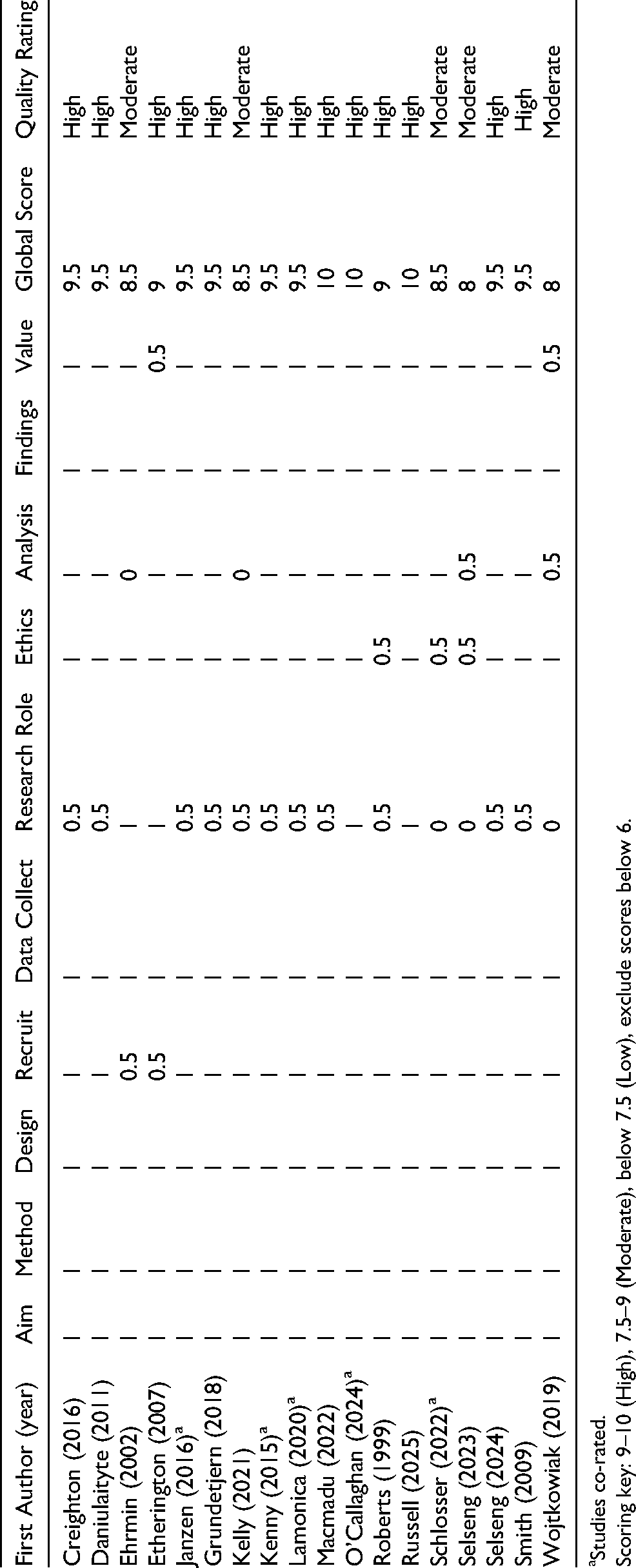
CD rated all included studies using the CASP grading system developed by Butler et al. (2016). This grading system was employed to facilitate clearer comparison between studies and increase the rigor of quality assessment. Criteria was scored as 1 (met), 0.5 (unclear), or 0 (not met), with total scores categorizing studies as low, medium or high quality.
A Trainee Clinical Psychologist, external to the review, independently rated five studies (28%), achieving 90% inter-rater agreement with the CD. Disagreements pertained to whether sufficient consideration had been given to the ethical implications of completing sensitive research in the context of substance use and if there had been consideration given to the relationships between the researcher and the participants. Discrepancies were resolved through discussion until consensus was reached. No studies were excluded based on quality rating. Overall quality rating of each study is provided in Table 1, with individual item ratings in Appendix B.
Synthesis Method
Thematic synthesis was the most suitable method for the current review as it facilitates the integration of data from a range of qualitative methods, accommodates cross-disciplinary perspectives, and is well-suited to novice reviewers (Flemming & Noyes, 2021).
The synthesis followed the three-stage approach outlined by Thomas and Harden (2008). Studies were imported into Dedoose software (https://www.dedoose.com/) and coded from “Results” onwards. Both participants’ accounts and author interpretations were coded to capture experiential and conceptual data. Coding was conducted inductively, with each line of text examined for meaning and assigned a conceptual code. While coding only participant accounts may have minimized bias given the novelty of the review and the high degree of avoidance within the research population, it was deemed appropriate to synthesize author interpretations. It was considered this would provide a contextual understanding of the data.
The studies were coded in no particular order; subsequent studies were coded into pre-existing codes and new codes were created when required to allow for flexibility and responsiveness to the content. Once initial coding was complete, the codes were grouped into conceptually similar clusters to form descriptive themes that captured recurring patterns across the data set. Descriptive themes were then interpreted to develop higher-order analytical themes and subthemes that addressed the review question. This process involved mind mapping and iterative discussion with a Clinical Psychologist (LR) and Consultant Clinical Psychologist (LM), with academic and clinical expertise within drug and alcohol services, to enhance rigor of the synthesis.
Theoretical Position and Reflexivity
This systematic review adopts a critical realist and interpretivist perspective. Interpretivism facilitates the exploration of the personal experiences of participants (Schwandt, 2000); while critical realism acknowledges that structural factors such as stigma, trauma, and access to support will influence experience (Maxwell, 2012). While the review is grounded in this perspective, a reflective stance was employed to consider epistemological diversity across the included studies with reference to similarities and differences in interpretations.
Reflexivity was maintained throughout to consider positionality. CD brought prior clinical experience of working with individuals experiencing complicated grief and research experience in qualitative methods which may have shaped the development of the research question and interpretation of findings. To mitigate potential bias, the researcher engaged in reflexive journaling to explore assumptions, emotional responses and decision-making. Supervision with experienced clinicians and researchers in the field (LR and LM) was used to explore interpretations and enhance transparency of the analysis. Additionally, the researcher had recently conducted her own study exploring the perspectives of people who use substances which may have increased her sensitivity to ethical issues and influenced her CASP assessment.
Results
Study and Participant Characteristics
In total, 18 studies were included in the review representing the grief experiences of 334 participants. While the studies from Selseng et al. (2023, 2024) used the same participant sample; both were included as they had distinguishable focuses that were relevant to the research question. The majority of participants were women (58%). Some studies omitted details regarding participants’ ethnicity; however, where reported, participants were predominantly identified as either Black or White. This indicates limited ethnic diversity across the sample. Age ranged from 18 to 63 years. Substances ranged and included heroin, crack cocaine, alcohol, and benzodiazepines.
Six studies explored the experience of loss and grief generally (Creighton et al., 2016; Daniulaityte & Carlson, 2011; Ehrmin, 2002; Etherington, 2007; Roberts, 1999; Smith, 2009). Seven studies explored grief related to drug-related death (Kelly et al., 2021; Macmadu et al., 2022; O’Callaghan & Lambert, 2024; Schlosser & Hoffer, 2022; Selseng et al., 2023, 2024; Wojtkowiak et al., 2019). Five studies explored the experience of grief following the removal of children (Grundetjern, 2018; Janzen & Melrose, 2017; Kenny et al., 2015; Lamonica & Boeri, 2020; Russell et al., 2025). Studies were published between 1999 and 2025; with the majority published within 10 years of the review (n = 13). The studies exploring grief following drug-related death were, primarily, the most recent studies which is reflective of a research response to the global drug-related death crises (WHO, 2024a). Studies were conducted in the United States (n = 8), Canada (n = 3), Norway (n = 3), the United Kingdom (n = 2), Ireland (n = 1) and the Netherlands (n = 1). All studies collected data using semi structured interviews although, analysis approaches varied.
Quality Assessment Results
All studies were of good quality. They presented clear aims and rationales. All studies adopted an appropriate research design and data collection method. Consideration of ethical issues was present in all studies and was evidenced by the provision of ethical approval statements. However, no studies appeared to consider how obtaining informed consent may be more difficult within the context of substance use or made reference to how they could manage potential distress.
Some authors considered their role as a researcher (Ehrmin, 2002; Etherington, 2007; Lamonica & Boeri, 2020; Macmadu et al., 2022; O’Callaghan & Lambert, 2024; Russell et al., 2025; Selseng et al., 2024) and made appropriate accommodations to encourage participation. Few studies explicitly discussed researcher positionality and its influence on data interpretation, although O’Callaghan and Lambert (2024) and Russell et al. (2025) addressed it by use of a reflexive journal.
While most studies (n = 14) focused on individuals already engaged in harm reduction or treatment; Ehrmin (2002), Kenny et al. (2015), Lamonica and Boeri (2020), and Roberts (1999) recruited participants who were not necessarily engaged with services. This provides perspectives of those disconnected from care. All studies provided rich data, using direct quotes, and supporting interpretations. All studies contribute meaningfully to practice and research.
Given that all papers were assessed as good quality, the quality appraisal did not significantly influence the analysis or findings. This consistency in quality allowed for a more confident synthesis of the evidence, ensuring that the conclusions drawn were based on robust and reliable studies.
Thematic Synthesis Results
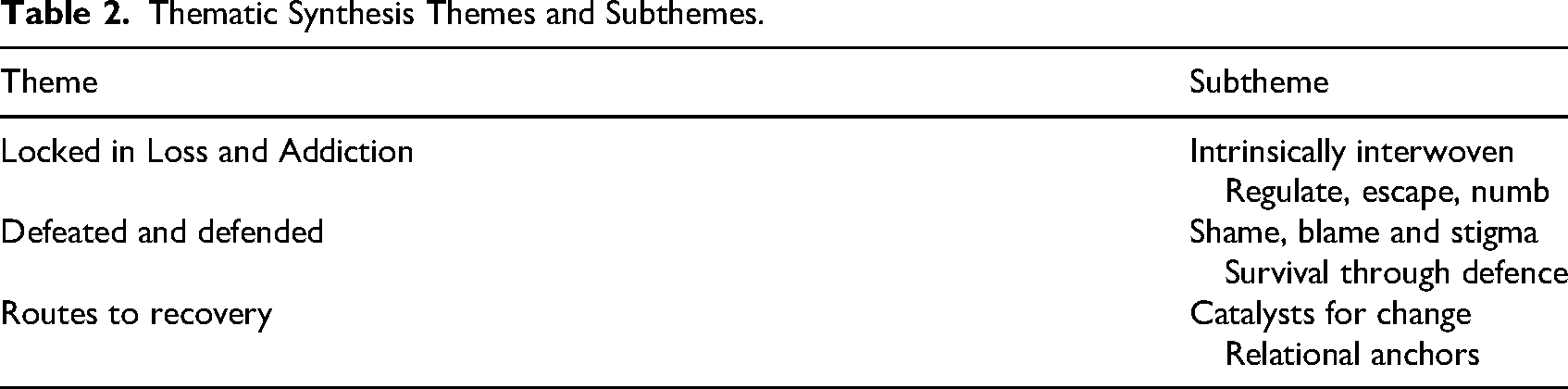
Three themes were identified: Locked in Loss and Addiction, Defeated and Defended, and Routes to Recovery (Table 2). The prevalence of themes across studies is outlined in Table 3.
Thematic Synthesis Themes and Subthemes.
Prevalence of Themes and Subthemes Across Studies.
Locked in Loss and Addiction
This theme explores the interconnected relationship between grief and substance use. It illustrates the impact of ongoing and cumulative loss that precipitate and perpetuate substance use, creating a cycle of ongoing distress.
Intrinsically Interwoven
This subtheme captures how grief and substance use become entwined in people's lives. Across all studies, participants’ described life histories replete with cumulative loss, trauma, and adversity. Losses included parental figures, family members, children (through removal or death), and peers. These losses were often accompanied by feelings of abandonment, shame, guilt, and worthlessness (Daniulaityte & Carlson, 2011; Ehrmin, 2002; Etherington, 2007; Janzen & Melrose, 2017; Kenny et al., 2015; Macmadu et al., 2022; O’Callaghan & Lambert, 2024; Roberts, 1999; Russell et al., 2025; Schlosser & Hoffer, 2022; Selseng et al., 2023; Smith, 2009; Wojtkowiak et al., 2019). Julie described this ongoing loss: When I was 18, mom died. My older brother is gay. Never see him; never knew my father. I loved my daughter's daddy. He left after she was born. [Social services] took her away when she was a baby. She grown now, and I’ve not seen her since she's adopted. It still hurts. (Roberts, 1999, p. 627)
With limited psychological or social buffers, grief did not exist as a singular event, but rather a persistent emotional state (Daniulaityte & Carlson, 2011; Ehrmin, 2002; Etherington, 2007; Grundetjern, 2018; Kelly et al., 2021; Macmadu et al., 2020; O’Callaghan & Lambert, 2024; Roberts, 1999; Schlosser & Hoffer, 2022; Selseng et al., 2023; Wojtkowiak et al., 2019). Across studies, grief precipitated or led to increased substance use to cope which exacerbated instability and contributed to secondary losses.
This cycle of loss and addiction created emotional stagnation in which grief could not be processed and hopelessness took root (Janzen & Melrose, 2017; Kenny et al., 2015; Macmadu et al., 2020; O’Callaghan & Lambert, 2024; Schlosser & Hoffer 2022; Selseng et al., 2023; Roberts, 1999; Wojtkowiak et al., 2019). To cope, emerged a “neutral death acceptance” (Wojtkowiak et al. 2019). This was characterized not by an active desire to die, but an ambivalence towards living as participants contended with insurmountable emotional pain (Janzen & Melrose, 2017; Kenny et al., 2015; Macmadu et al., 2020; O’Callaghan & Lambert, 2024; Schlosser & Hoffer 2022; Selseng et al., 2023; Roberts, 1999; Wojtkowiak et al., 2019).
Regulate, Escape, Numb
This subtheme explores participants use of substances to soothe overwhelming internal distress. Across all studies (except Kelly et al., 2021), and irrespective of the source of grief, participants described an escalation of, or relapse into, substance use after loss. Substances were used to regulate the intensity of grief, “I guess the drug use has actually increased to suppress pain and feelings” (Schlosser & Hoffer, 2022, p. 6); numb distressing emotions, “I not only relapsed but I doubled the use … the hole, the empty spot … there was this big gaping hole that can't be filled, but you try to fill it with drugs” (Smith, 2009, p. 408); or escape an intolerable reality: In the early aftermath of separation, almost all women described trying to numb and detach from memories of what had occurred. Women almost universally explained responding to suffering through increased use of drugs (e.g., cocaine, heroin, opioids and cannabis) and alcohol. Women also described binging as a strategy for immediate sedation from pain. (Kenny et al., 2015, p. 1162)
Across studies, participants’ accounts highlight that the destabilizing nature of loss led to a reliance on substances to provide short-term relief from emotional pain.
Defeated and Defended
This theme examines participants’ experiences of interacting with services in the aftermath of loss. It also explores how participants externally attempted to manage grief through withdrawal and defensive coping. These responses could be shaped by repeated trauma and a lack of opportunity to access supports.
Shame, Blame and Stigma
This subtheme explores participants experience of social isolation in the aftermath of loss, with grief often unacknowledged, minimized or dismissed (Daniulaityte & Carlson, 2011; Ehrmin, 2002; Janzen & Melrose, 2017; Kelly et al., 2021; Kenny et al., 2015; Lamonica & Boeri, 2020; O’Callaghan & Lambert, 2024; Roberts, 1999; Russell et al., 2025; Schlosser & Hoffer, 2022; Smith, 2009; Wojtkowiak et al., 2019). Some experiences of stigma and disenfranchisement were passive, there was a sense that it had not been considered that participants would be impacted by death (Kenny et al., 2015; Russell et al., 2025): He was visiting a close friend, spending the night there, and found him dead from an overdose the following day. Stian said that he called the police (…) After Stian had quickly explained what had happened, one policeman said: “yes—you can just go” (Selseng et al., 2024, p.430).
The author's interpreted the indifference in response as reflecting a sense of social devaluation for people who use substances as grieving individuals (O’Callaghan & Lambert, 2024).
Indeed, across six studies (Creighton et al., 2016; O’Callaghan & Lambert, 2024; Roberts, 1999; Russell et al., 2025; Schlosser & Hoffer, 2022; Selseng et al., 2024), drug use overshadowed grief in service responses which reinforced the notion that substance use, rather than loss, was the primary issue requiring intervention: “The clinic is busy, it's full, so sometimes the appointment would be just in, get your script [prescription] and out the door again. So there was, you know, minimal supports offered and available” (Russell et al., 2025, p. 8). The authors’ interpretation of these accounts emphasized how dismissal reinforced feelings of disenfranchisement and made it more difficult for these individuals to access support for their grief.
Survival Through Defence
When grief was unseen, dismissed, or overshadowed by substance use, individuals were left to process their losses in isolation (Creighton et al., 2016; Macmadu et al., 2022; O’Callaghan & Lambert, 2024; Selseng et al., 2024; Wojtkowiak et al., 2019). This could result in blocked grieving and the intensity of unresolved grief could lead to individuals becoming emotionally detached: The detached mothers’ almost nonchalant way of describing the event, and laughing instead of crying, may have been a defence mechanism resulting from having lost a child (Grundetjern, 2018, p. 405).
The incongruent reaction is interpreted as an attempt to emotionally distance herself from her pain. As participants relied upon avoidance to cope, this created an internal conflict in which they desired support but struggled to articulate their needs (Russell et al., 2025; Schlosser & Hoffer, 2022; Selseng et al., 2024): I would love to be able to just come and go like ‘Look I am feeling like s*** and need somebody to talk to’, but I just really struggle with that. I mean maybe just now my barriers have come down a wee bit, but I still feel that I can’t open up like with [addiction worker]. (Russell et al., 2025, p. 5)
When interacting with services, this made it difficult for grief to be recognized: “Several of the bereaved mentioned that typical situations they encountered were helpers asking, “How are you?” or “Are you okay?” The bereaved answered in the affirmative, and thus the follow-up ended” (Selseng et al., 2024, p. 434). Thus, unexpressed and unacknowledged grief reinforced avoidance-based coping and emotional detachment.
Routes to Recovery
This theme explores how participants navigated recovery in the aftermath of grief and substance use. Recovery is presented as a fragmented and nonlinear process shaped by moments of insight, relational support and a search for meaning.
Catalysts for Change
For some, recovery could begin with a significant event, often the overdose of another within ones social network (Macmadu et al., 2022; O’Callaghan & Lambert, 2024; Schlosser & Hoffer, 2022; Selseng et al., 2023). This could be a “wake-up call” (Macmadu et al., 2022), that prompted reflections around one's own substance use and mortality, “Just, you don’t wanna overdose. You don’t wanna risk having that happen to you” (Macmadu et al., 2022, p. 8).
However, without alternative coping mechanisms, long-term recovery was not sustainable: I thought it would be enough for me to like, “Okay, this is it. I gotta get my shit together,” and whatever. And it was for a year and a half. It was enough for me to kind of think about it every day and use it to benefit, but it wasn’t—it wasn’t enough to keep me sober. (Schlosser & Hoffer, 2022, p. 6)
Nevertheless, in the authors’ interpretation, this change was seen as a temporary avoidance strategy rather than a sustainable coping mechanism, as the underlying grief remained unresolved.
Relational Anchors
Within the context of grief and loss, participants who developed greater control over their substance use did so when they had some form of support or stability in their lives (Creighton et al., 2016; Daniulaityte & Carlson, 2011; Etherington, 2007; Janzen & Melrose, 2017; Kenny et al., 2015; Lamonica & Boeri, 2020; Macmadu et al., 2020; Roberts, 1999; Russell et al., 2025; Schlosser & Hoffer, 2022; Selseng et al., 2023).
Across six studies (Etherington, 2007; Lamonica & Boeri, 2020; Macmadu et al., 2020; Schlosser & Hoffer, 2022; Selseng et al., 2023; Roberts, 1999) caring for someone else could be a motivating factor, “As a disincentive to using heroin intravenously, she had her children's names tattooed on her arm” (Lamonica & Boeri, 2020, p. 11). For others, witnessing the ripple effect of grief on loved ones prompted reflections on the potential consequences of their own death: If I continue to do drugs, and I die, it's actually not about me, because it is those left behind who have to live with my death. So, perhaps it's okay to live life a bit for someone else too. (Selseng et al., 2023, p. 466).
It was noted that having a structured job (Creighton et al., 2016; Daniulaityte & Carlson, 2011; Janzen & Melrose, 2017; Kenny et al., 2015; Lamonica & Boeri, 2020), and supportive workers, peers and community members (Daniulaityte & Carlson, 2011; Janzen & Melrose, 2017; Roberts, 1999; Russell et al., 2025; Selseng et al., 2023) could support recovery. This was considered essential for emotional processing: I have support people now that I call when I’m going through something (…) even if I was to take a drink, my problem would still be there. So if something is bothering me very badly, I pick up the phone and talk about it. (Daniulaityte & Carlson, 2011, p. 6)
When these supports were in place, participants were more likely to adopt harm reduction practices (Lamonica & Boeri, 2020; Macmadu et al., 2020; Roberts, 1999). When these relationships and supports did not exist, substance use escalated as a means of coping with grief. The authors emphasized that emotional and social support networks were essential for preventing relapse and supporting long-term recovery.
When self-compassion remained blocked, the recognition of the impact upon others fostered a sense of responsibility and reason to live. As participants were socially isolated and emotionally disconnected, acts of caregiving became an avenue towards meaning and recovery: I can make a difference, even if it's just little (…) for another lady that probably is going to come in here needing the room that I paint, she can use it. Little things like that with my recovery that keep me going, for another person, to help them out, that is much more. (Janzen & Melrose, 2017, p. 245)
The authors interpreted these small acts as a way of reconnecting to a sense of purpose and belonging.
Discussion
This review is the first comprehensive synthesis of qualitative literature exploring the grief experiences of people who use substances. Eighteen studies were analyzed, producing three themes: Locked in Loss and Addiction, Defeated and Defended, and Routes to Recovery. Despite variability in study contexts the findings are cohesive thus, offering an aggregated insight and nuanced understanding of the grief experience for people who use substances.
Regulation of Grief
This synthesis provides substantive evidence that increased substance use is a grief response for people who use substances and identifies grief as a relapse trigger. These findings contextualize quantitative reviews and provide qualitative depth, demonstrating substance use as an emotion regulation strategy (Stellern et al., 2023; Weiss et al., 2022; Wong et al., 2013). As postulated by the DPM, coping with grief is a complex regulatory process characterized by a fluctuating pattern of confrontation and avoidance (Stroebe & Schut, 2010). From this perspective, substance use serves as an accessible, albeit harmful, means of navigating this regulatory process. This positions substance use as an understandable emotion regulation strategy developed in the context of chronic stress and adversity, offering a destigmatizing understanding.
Additionally, this review clarifies psychological mechanisms that may underpin substance use as a grief response and offers intervention targets. Namely, attempts to downregulate the intensity of grief, substance use to avoid distressing thoughts, emotions and memories, and appraisals regarding one's ability to cope without the numbing effect of substances. The finding that initial substance control is unsustainable following loss evidences the importance of interventions that equip individuals with helpful coping strategies to support recovery (Caparrós & Masferrer, 2021).
The synthesis also illustrates the role of cumulative trauma; people who use substances often experience a loss with pre-existing emotional vulnerabilities shaped by early adversity, structural stigma, and social exclusion. These contextual factors may heighten the likelihood that grief precipitates a return to or escalation of substance use due to regulatory resources being eroded by marginalization (Casiano et al., 2025). Cumulative loss was a particularly significant finding, with repeated exposure contributing to emotional overload, detachment and neutral death acceptance. While participants did not actively seek death there were consistent reports of ambivalence towards life (Wojtkowiak et al., 2019). This may reflect a protective coping response in the context of trauma and marginalization, whereby persistent exposure to stigmatized loss fosters fatalism and apathy. The prominence of this finding across studies spanning over 25 years provides evidence of this being a significant feature of the grief experience for people who use substances.
These insights have important implications for intervention delivery. Ambivalence towards life diminishes self-care while bolstering powerlessness to change (Butler et al., 2015). This is compounded by limited opportunities for restoration and healing, particularly in the context of trauma, homelessness, poverty and stigma (Aldridge et al., 2018; Russinova et al., 2011; Wesselmann & Parris, 2021). This suggests that people who use substances may be less responsive to grief support that focuses on future-orientated goals. The finding that connection to, and concern for, others can motivate individuals to adopt safer using practices and engage in recovery suggests that grief interventions with a relational and values based approach may be more beneficial (Lamonica & Boeri, 2020; Patton et al., 2022). Given the dearth of validated grief interventions for people who use substances (Parisi et al., 2019), this presents an avenue for clinical implementation and ongoing research.
Social Support and Meaning
While the importance of social support in recovery is well evidenced (Best et al., 2015; Tracy & Wallace, 2016), this synthesis illuminates the protective role of social support, meaningful relationships, and purpose in mitigating grief. The finding that caregiving roles, such as parenting or supporting peers, can instill a sense of value, meaning, and self-worth corroborates the literature evidencing the restorative power of peer support roles for those in recovery (Scannell, 2021). This has particular relevance within the current global drug-related mortality crises and grieving population of people who use substances (WHO, 2024b). Findings from the synthesis suggest that responses to drug-related deaths must incorporate grief support as well as providing opportunities for connection, belonging and meaningful contribution within communities. These findings challenge narrow models of grief intervention that focus solely on individual pathology and instead emphasize the therapeutic importance of relational and systemic contexts.
Disenfranchised Grief
Across studies, grief among people who use substances was consistently unrecognized and unsupported. Participants described being positioned as drug users rather than grieving individuals, leading to their emotional needs being overlooked. This was evidenced in the oldest (Roberts, 1999) and most recent (Russell et al., 2025) studies, suggesting the disenfranchisement of grief for people who use substances is a persistent systemic issue.
Stout and Fleury-Steiner (2023) argue that bereavement following a drug-related death is shaped by interactional stigma, including alienation, limited access to support, and judgmental service responses. People who use substances describe internalized shame, self-blame, and emotional withdrawal, which may be interpreted as personal deficits rather than as adaptive responses to stigma, trauma, and exclusion. This underscores the importance of recognizing stigma as a mechanism that shapes behavioral patterns rather than viewing these behaviors as inherent characteristics of people who use substances. To address these inequities, frontline staff require training to deliver grief-informed care, particularly given that grief may not be verbally expressed (Russell et al., 2025; Schlosser & Hoffer, 2022; Selseng et al., 2024). Practitioners may benefit from support in identifying nonverbal expressions of distress including withdrawal, irritability, or substance use escalation (Lavelle et al., 2024; Offor et al., 2024). Further research is also required to examine how stigma perpetuates the disenfranchisement of grief for people who use substances and how this may be dismantled in service delivery and guiding policies.
Strengths, Implications and Future Directions
This review is the first to systematically synthesize qualitative literature on the grief experiences for people who use substances, providing evidence that grief is a significant but often overlooked feature of the lives of individuals accessing support within alcohol and drug recovery services. The methodological rigor of the included studies enhances the credibility of the synthesis.
The consistency of themes across 25 years of research highlights the persistent challenges of addressing grief needs for people who use substances. This has individual implications, supporting the notion that those accessing treatment are likely to have unaddressed grief needs requiring clinical attention (Furr et al., 2015; Parisi et al., 2019). Also, within the context of global public health, these findings hold urgent clinical and policy relevance (WHO, 2024b). By collating the experiences of this stigmatized group, this synthesis enhances clinical awareness and reinforces the need for grief-informed care in services. The synthesis also provides avenues for such care: caregiving and peer support opportunities, and relationally orientated grief interventions. Future research should prioritize the development and integration of grief-informed care into service delivery and clinical practice.
Limitations
Due to the ambiguity of “loss” as a construct, the search strategy prioritized specificity, potentially omitting relevant studies. From this, a limitation of the review is the narrow scope of loss types represented in the literature. Although the search strategy was designed to capture a broad range of grief experiences among people who use substances, the literature identified in the search predominately focused on death and child removal. This reflects a gap in the existing research rather than a selective focus of the review itself. As such, other significant forms of loss, such as identity disruption or symbolic loss, may be under-represented. Future research should explore these constructs to provide a more comprehensive understanding of the range of grief experiences within the context of substance use. Limiting the review to English language studies has resulted in a synthesis that predominantly reflects Western experiences of grief. Future research should explore variance in the intersection of grief and substance use across cultures. This is important as minority groups experience significant structural barriers that can block their access to care (Mantovani & Evans, 2019).
Although the studies were methodologically robust, the exclusion of dissertations and gray literature may have omitted valuable insights. As people who use substances are under represented in research, future reviews should incorporate unpublished studies.
Conclusion
This review has collated the experiences of a highly stigmatized, complex, and often silenced community to offer an understanding of their grief experiences. The findings illustrate the complex relationship between grief and substance use; and reinforce the need for grief informed approaches in services. This review found evidence of the intervening potential of caregiving and meaningful relationships in mitigating distress and substance use. This highlights community belonging, relational support, and purposeful activity as being integral to grief informed care. Importantly, diminished grief recognition remains a systemic issue and ongoing research is required to understand how this may be dismantled.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No primary data were generated during this systematic review. The articles reviewed are available in the public domain and references are provided in the manuscript.
PROSPERO: As per PRISMA guidelines, this systematic review protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) on December 11, 2023. An update was submitted on November 19, 2024, January 29, 2025 and May 15, 2025 (CRD42023491010).