
Abstract
Background
A government monopoly for cannabis sales may offer public health advantages over more commercial approaches. The monopoly governance and regulatory infrastructure can help avoid overcommercialization and related harms.
Aims
To examine the governance mechanisms in the cannabis retail monopoly managed by the Quebec cannabis corporation (Société québécoise du cannabis, SQDC), and how they restrain commercialization and attempt to reduce harms.
Methods
Thematic analysis of semi-structured face-to-face interviews with 34 key stakeholders from Quebec's public sector, academia, cannabis industry, and civil society. Field observations of government-run cannabis retailers and a review of the Quebec legislative framework.
Results
Formal and informal governance mechanisms to protect the cannabis monopoly from overcommercialization and reduce cannabis-related health harms were identified. Key formal governance structures include: (1) legislated not-for-profit mission of the SQDC; (2) allocation of SQDC profits to funding of cannabis prevention and research; (3) legislated independent health-focused oversight committee; (4) delegation of regulatory function to health and separation of oversight between health and finance agencies; and (5) the SQDC internal organization. Informal mechanisms include: (1) regular consultations between the SQDC and health ministry; (2) non-binding advice from high-profile health agencies; and (3) wider public opinion. The effectiveness of informal mechanisms is mediated by the SQDC leadership. Although key stakeholders with health backgrounds overwhelmingly viewed governance structures in the SQDC model as superior to the long-standing Quebec alcohol monopoly (SAQ), several weaknesses in the model were identified, including the limited formal powers of the oversight committee and the SQDC personnel’s links with the more profit-oriented provincial alcohol corporation.
Conclusion
The governance mechanisms adopted in the SQDC model compare favorably against the alcohol retail monopoly in Quebec in terms of reducing substance-related health harms. They could be improved by strengthening the power of the oversight committee, separating SQDC from SAQ networks, and formalizing reporting to the health ministry.
Keywords
Introduction
The legalization of non-medical (recreational) cannabis in the Americas since 2012 has stimulated significant international debate about the best model for cannabis law reform (Caulkins & Kilmer, 2016a; Decorte, 2018; Pardal et al., 2023; Queirolo et al., 2016; Rolles & Murkin, 2016; Rychert & Wilkins, 2019). The for-profit approach to cannabis sales implemented in all US states that have legalized non-medical cannabis supply (except Washington DC), has been criticized for its level of commercialization and potential associated negative consequences on public health, as previously well documented with alcohol and tobacco products (Adams et al., 2021; Caulkins & Kilmer, 2016b; National Academies of Sciences Engineering and Medicine, 2024; Rolles & Murkin, 2016). A state-run government monopoly model for cannabis sale is one alternative approach that has received attention from some policymakers and expert endorsement (Blanchette et al., 2022; Karbal, 2024; Pardal et al., 2023; Wilkins et al., 2022).
In the government monopoly market model for cannabis, the government (on national, provincial, or local level) is solely involved in the manufacture, wholesale, and/or retail sale of cannabis, typically through a state-owned cannabis corporation. For example, in the Canadian provinces of Quebec, Nova Scotia, and Prince Edward Island, government-owned corporations have an exclusive monopoly to operate cannabis retail outlets, both online and through brick-and-mortar stores. In the other Canadian provinces, brick-and-mortar stores are operated by private retailers exclusively (e.g., Manitoba, Saskatchewan), or the government cannabis corporation competes with privately run brick-and-mortar stores (e.g., British Columbia) (CCSA, 2024). Most Canadian provinces and territories implemented a government monopoly on the wholesale of cannabis within their jurisdictions. In Uruguay, a national government agency tightly manages the legal cannabis market by imposing limits on the licensed cannabis production volume, controlling retail prices, determining the products on offer, and monitoring compliance with an individual weekly purchase limit (10 g) in pharmacies allowed to dispense recreational cannabis. Although the approach in Uruguay is not an absolute government monopoly (i.e., private operators licensed by the state are involved in production and retail (Rychert et al., 2025), the legal market is tightly controlled by the state, with only 3 licensed cannabis producers, 40 pharmacy points of sale, and 4 types of cannabis flower products on the market a decade into the legalization (IRCCA, 2024). Despite few jurisdictions implementing such tightly regulated state-controlled models to date, a number of drug policy experts have suggested they are the preferred models for cannabis law reform among other options (Blanchette et al., 2022; Rogeberg et al., 2018; Wilkins et al., 2022).
The primary mechanism by which a government monopoly model for legal cannabis sales may offer public health and safety advantages over alternative more commercial approaches is largely by minimizing or removing profit-driven actors (Room & Cisneros Örnberg, 2019) and their incentives to increase sales through price competition and discounting to expand the consumer base and increase total consumption, and marketing strategies that appeal to youth (e.g., Moreno et al., 2022; Padon et al., 2025). Without the financial obligations to private owners and shareholders, public actors involved in the state-controlled cannabis markets are theorized to prioritize the noncommercial objectives of reform, fostering responsible sale environments that support lower-risk use (Fischer et al., 2022) and less negative health and social outcomes (Miller et al., 2006; Room & Cisneros Örnberg, 2019). In an exclusive government monopoly on retail legal cannabis sales, this may result in a lower number of retail outlets, comparatively higher prices, more conservative potency limits and product ranges, reduced advertising and marketing, and stronger overall enforcement of regulation—crucial levers of the public health approach to substance regulation (Fischer et al., 2019; Ghosh et al., 2015; Hall et al., 2019; Hammond et al., 2020). State control of the retail level of the supply chain (as opposed to a monopoly over manufacture and wholesale levels) has been identified as most critical to the public health outcomes of reform, as it directly impacts cannabis availability, retail prices, and the marketing environments where customers and sellers interact (Room & Cisneros Örnberg, 2019).
There is evidence from alcohol research to support the argument that retail monopolies confer positive public health outcomes. Reviews of off-license alcohol retail monopolies from jurisdictions in North America and Europe (Sweden, Finland, Norway, Iceland) concluded there is “quite strong” evidence (Babor et al., 2010) that off-premise monopoly systems limit alcohol consumption and alcohol-related problems at a population level (Her et al., 2002). A systematic review of studies of changes in the opposite direction (that is, replacing a monopoly with private retailers) found “strong evidence” of increases in excessive alcohol consumption (Hahn et al., 2012). A study modeling a hypothetical privatization of the alcohol monopoly in Sweden estimated a 20%–31% increase in per capita alcohol consumption (Stockwell et al., 2018).
However, the noncommercial orientation of state-owned corporations can become eroded, as evidenced by the history of alcohol and tobacco monopolies. For example, the alcohol monopoly in Sweden has undergone a number of changes to a more commercial direction in recent decades, including the abolishment of parts of the monopoly in 1994 and the legalization of alcohol advertising in 2003 (Ramstedt, 2010). Another example is China's state-owned tobacco corporation with a monopoly on production and sales, which has faced criticism for insufficient implementation of public health measures, including low taxes and weak health warnings on cigarette packaging (Chan et al., 2023). In Quebec, the state alcohol corporation (currently named Société des alcools du Québec, hereafter SAQ), originally established in 1921, has transformed from a tightly managed network of 64 “caged” stores to over 800 points of sale with a loyalty card system, concept stores, and advertising. Such “mission drift” in state-owned enterprises may occur as a result of changing governments and related priorities and a public sector increasing focus on the revenue-generating function of monopolies (Alexius & Cisneros Örnberg, 2015), alongside pressures from the for-profit industry operating within the model (e.g., private producers) (Hall, 2020), the changing vision of successive public agency management teams, and positive social norms and public pressure for greater accessibility (Rychert et al., 2020).
Therefore, a key question for the new cannabis monopolies is whether, and how, the possible mission drift towards overcommercialization can be avoided. Public health experts have noted that institutional arrangements and governance mechanisms in state-controlled monopolies play a key role in protecting the health and social welfare function of monopolies, i.e.,: “how the monopoly is motivated, constructed and run, and where it is located within the government are crucial determinants of whether the monopoly makes a positive contribution to public health and welfare” (Room & Cisneros Örnberg, 2019). For example, the regulation of a state-owned cannabis corporation under the health agency rather than the business or economic development department may help sustain an institutional “culture of health.” In the tobacco control field, analysts suggested that the inherent tensions between revenue-generating and public health objectives of state-owned tobacco producers may be managed through institutional separation, and that “radically reprogramming” the objectives of state-owned tobacco companies may offer the best opportunities for public health (Hogg et al., 2016).
The aim of this study was therefore to identify and critically analyze Quebec governance structures implemented to safeguard the health and social missions of the largest state-run retail monopoly for legal cannabis and draw lessons for other countries that may be interested in a similar reform. We examine how the Quebec cannabis corporation (Société québécoise du cannabis, hereafter SQDC) is run, overseen, and motivated, using key informant interviews, field visits to cannabis retail outlets, and analysis of the legal framework. Quebec has decades of experience with the public monopoly arrangements in other sectors, including alcohol, gambling, and electricity, which makes it an insightful case study (Yin, 2018) of monopoly governance structures. Therefore, a secondary aim was to explore how the governance mechanisms in the legal cannabis monopoly model differ from the provincial approach to the alcohol monopoly, and what additional structures to protect the model from overcommercialization have been implemented for cannabis.
Methods
We began by reviewing the Quebec Cannabis Regulation Act, accompanying provincial regulations (Regulation C-5.3, r. 0.1 concerning products, Regulation C-5.3, r. 1 concerning staff training), relevant government reports (MHSS, 2021; Ministry of Finance, 2022), and SQDC annual reports and strategic plans (SQDC, 2023a, 2023b, 2024a). Nonsystematic field visits to the SQDC and SAQ retail outlets (14 stores were visited in Québec and Montréal) provided a first-hand understanding of how the retail environments for cannabis and alcohol differ (see Online Supplementary Material for a comparison of the retail environments in the SQDC and SAQ). This formative work informed the development of a semi-structured interview schedule used to conduct face-to-face interviews with key stakeholders (KS) in Quebec. For example, the retail differences observed during field visits (e.g., store location, layout and promotions) and legislative processes identified through the review of regulations were followed up and explored in the interviews, with specific questions aimed to identify decision-making processes (e.g., How does SQDC decide where to open a new store? What advice is sought prior to marketing of a new product?). A qualitative key informant interview method (Pahwa et al., 2023) was used to investigate the day-to-day operation of the cannabis monopoly model in Quebec and identify formal rules and informal practices implemented to preserve the social and health orientation of the model. The research process was iterative. As the interviews with KS progressed, participants’ insights were verified and compared with subsequent interviewees, and their accounts of formal rules were verified with the laws, regulations, and official documents, where possible.
In-depth face-to-face interviews were conducted with 34 KS involved in the development and implementation of the cannabis legalization regime in Quebec. Interviewees included civil servants and law enforcement personnel (6), health professionals and academics who acted in advisory roles for the regime (8), high-level representatives from the SQDC (2), independent researchers (4), harm reduction and community organizations (3), commercial licensed cannabis producers (4), cannabis activists (4) and legacy cannabis growers (i.e., cannabis growers who have experience of cultivation within the illegal and legal licensed market) (3). Sixteen of the interviewees worked in the public sector and had in-depth knowledge of the institutional arrangements and operation of the regime in practice, providing first-hand accounts of how the regime operates, including insights into the informal practices developed during implementation of the SQDC model. A few interviewees held multiple roles in the regime (e.g., academic/activist; academic/advisor) or progressed to unrelated roles since their involvement in the cannabis legalization process. Key stakeholders with significant roles and in-depth knowledge of the cannabis monopoly market in Quebec were identified from the initial review of documents, authors’ professional networks, and subsequent referrals, with invitations sent by email. To protect their identities, we refer to the general stakeholder type they represent based on the participant's primary role related to cannabis as identified in the interview and considering the context in which it occurred (e.g., in a public agency office). Explicit permission to attribute quotes to SQDC was sought from relevant interviewees, as these are attributed to the specific organization (rather than stakeholder type or sector).
A semi-structured interview guide was used to investigate KS experiences with the state-run cannabis retail model and their views on the governance of the regime. The interview schedule consisted of general questions about the model asked of all KS (e.g., perceived benefits and disadvantages of the model, assessment of the SQDC success in achieving their legislated mission) and questions specific to distinct KS types (e.g., civil servants were asked about the nature and frequency of contacts with the SQDC; SQDC managers were asked about their reporting obligations to health vs finance agencies). Interviews were conducted face-to-face in English by the first author, with the majority of interviews conducted one-on-one (except two interviews that involved pairs of stakeholders) and in-person in Quebec province (for logistical reasons, three interviews were conducted via Zoom video).
Interviews were conducted from June to August 2022, i.e., three and a half years into the cannabis legalization in Quebec. They lasted between 56 and 155 min, with a mean interview time of 84 min. All interviews were recorded and transcribed ad verbatim (with the exception of one interview where a KS agreed to participate in the study on the condition of non-recording, in this case notetaking was agreed). Transcripts were analyzed thematically (Braun et al., 2019), with the primary analytical focus on identifying the key governance structures and practices developed to preserve the health and social orientation in the Quebec cannabis monopoly. Deductive coding (informed by public health literature on the retail monopoly) was followed by inductive data-driven coding to identify both the legislated and informal practices developed to preserve the social orientation of the Quebec model. The first author led data analysis with assistance of NVivo qualitative software, following several discussions with the second author during the data collection period, and peer debriefing with the third author during data analysis, which informed the development and refinement of codes and themes. Additional techniques to ensure the validity and reliability of findings were member-checking (participants were offered the opportunity to review and correct their transcripts) and data triangulation (interviewees’ accounts of formal rules were verified with documents where possible). The authors have a background in public health, drug policy, epidemiology, and law, and the public health perspective—which is concerned primarily with health outcomes of cannabis reform on the population level and tends to favor precautionary approaches—guided the analysis. A reflexive approach was facilitated by seeking views of KS from a range of backgrounds, contrasting their views during the analysis, documenting methodological choices and unexpected insights in a logbook, and through peer debriefing.
The results section starts with an overview of the regulatory framework with regard to the retail environment in Quebec, providing context about the types of decisions that SQDC can make within the bounds of federal and provincial laws. Next, drawing on analysis of KS interviews, we identify key legislative and informal mechanisms developed to preserve the health and social orientation of the SQDC. In line with the qualitative description approach (Chafe, 2017), rich descriptions of KS’s experiences with the model and their views on its governance are included. The study is part of a larger project investigating middle-ground options for cannabis law reform in Uruguay, Quebec, Jamaica, and New Zealand. It received ethical approval from the Massey University Human Subjects Ethics Committee (ref. 19/37).
Results
Cannabis Market Regulation in Quebec and the Role of the SQDC
The SQDC was first established in June 2018 with the passage of Bill 157 by the provincial government in Quebec. As a state-owned enterprise, SQDC shares are 100% owned by the provincial government (through the Minister of Finance). The SQDC legislated mission is “to ensure the sale of cannabis from a health protection perspective in order to integrate consumers into, and maintain them in, the legal market without encouraging cannabis consumption” (Bill 157 and the Act respecting the Société des alcools du Québec, n.d., s 16). The SQDC manages both the wholesale and the retail level of the market for legal cannabis products in Quebec. The retail operations by the SQDC involve both brick and mortar stores and online sales through the SQDC website, with delivery services subcontracted to Post Canada (which is a Crown corporation itself). The vast majority of transactions occur in stores; only 5.7% of overall sales in the last financial year (2023/24) took place on the SQDC website (SQDC, 2024a, p. 96). Twelve SQDC-branded stores opened in the province on the first day of cannabis legalization in Canada (17 October 2018), and the number increased to 100 as of October 2024. Among all Canadian provinces, Quebec has the fewest number of cannabis stores per capita, and over 16 times less than Alberta (i.e., 1.24 vs 20.38 stores per 100,000 individuals 15+ years) (Myran et al., 2023a). All cannabis sold by the SQDC is produced in Canada by private licensed producers (based both within and outside Quebec), as required under the federal legislative framework, the Cannabis Act (Fischer et al., 2020; Health Canada, n.d.; INSPQ, 2022).
In managing the network of cannabis retailers, the SQDC must comply with the federal framework, as well as the provincial Quebec Cannabis Regulation Act and related regulations that set out rules for the sale of cannabis in the province. Nationally, the objectives of cannabis legalization in Canada focus on public health and public safety protection, including protecting young people from inducement to use cannabis and enhancing public awareness of the health risks of cannabis use. The public health and safety rules established under the federal Cannabis Act (e.g., minimum purchase age, potency limits) can be enhanced (but not diluted) at the provincial level, and the provincial governments have a primary mandate over the regulation of retail sales in the provinces.
Quebec's approach to cannabis legalization has been described as the most restrictive among Canadian provinces (Lévesque & Benoit, 2020; Robinson et al., 2024). It imposes a higher legal age of 21 to purchase and use cannabis (rather than 18, as proposed under the federal Cannabis Act, higher than 19 which is the legal cannabis purchase age adopted in most other provinces and territories, and higher than 18 which is the legal purchase age for alcohol and tobacco in Quebec), prohibits personal cultivation (all other provinces allow cultivation of up to 4 plants as permitted in federal Cannabis Act), and includes a general ban on smoking and vaping of cannabis in public places with municipalities able to allow it in parks (INSPQ, 2023). The original version of the law implemented in 2018 legislated a purchase age of 18 and allowed public consumption of cannabis on rules similar to tobacco laws, but these provisions were tightened in 2019 by a new conservative government, alongside a change in prohibitions to open SQDC stores in proximity to educational establishments (National Assembly of Quebec, 2019). Unique among Canadian provinces, regulations in Quebec also restrict cannabis product potency to a maximum 30% THC and impose additional restrictions on edible cannabis products that must not be attractive to youth, essentially excluding all sweets, desserts, and chocolates from the market. Table 1 provides a summary of the federal and provincial regulations and the types of decisions that SQDC can make within this regulatory context.
Hierarchy of Rules and Decision-Making Relating to the Cannabis Retail Environment at the Federal, Provincial (Quebec), and Organizational (SQDC) Level.
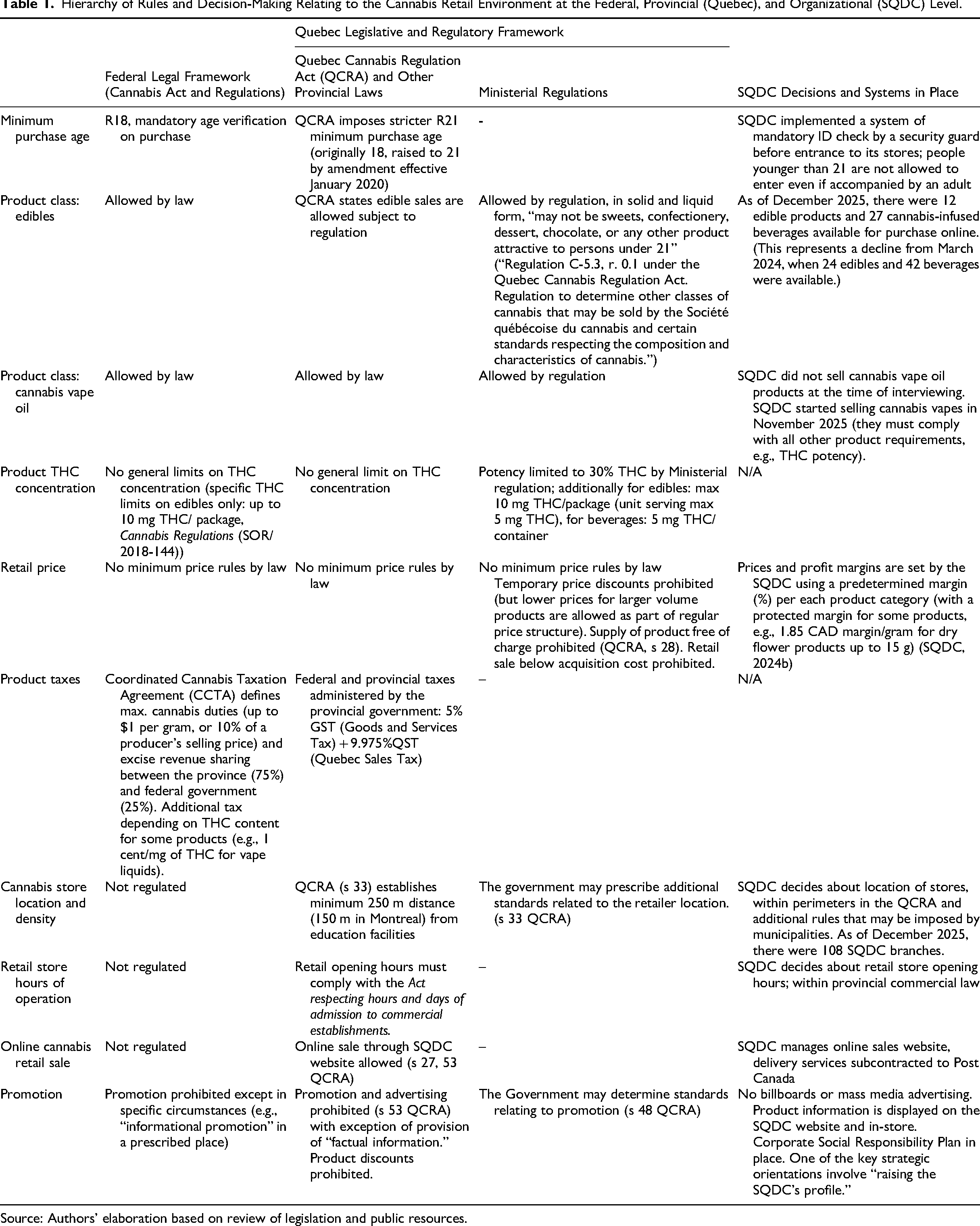
Source: Authors’ elaboration based on review of legislation and public resources.
Formally established as a subsidiary of Quebec Alcohol Corporation (SAQ—Société des alcools du Québec), the SQDC is considered an “associated company” rather than a “daughter” company under SAQ, because it does not meet standard international criteria of a subsidiary. Namely, the SQDC is governed independently from SAQ and overseen by its own board of directors (Ministry of Finance, 2022). Importantly, the Ministry of Health and Social Services (rather than the Minister of Finance—as is the case with SAQ) is responsible for the implementation of the Quebec Cannabis Regulation Act, including the development of regulations under the Act (INSPQ, 2023). Quebec stood out from other Canadian provinces that delegated the development of a legalization framework to their justice departments. In Quebec, this work was delegated to health sector agencies; it was led by the Cannabis Legalization Directorate within the public health division of the Health department, and the Health Ministry maintains a significant role in the regime (Wesley & Salomons, 2019). Analyses of the policy-making process noted a significant influence of medical and public health expertise on the development of the cannabis policy framework in Quebec (Lévesque & Benoit, 2020; Wesley & Salomons, 2019).
Formal Governance Structures and Mechanisms to Prevent Overcommercialization
(1) The legislated nonprofit mission of the SQDC
Stakeholders across the sectors identified that the legislated mission of the SQDC was the key legal mechanism implemented to prevent the overcommercialization of the model. The law requires SQDC to provide responsible sales of cannabis and to migrate consumers from the illegal to the legal cannabis market without encouraging consumption. Many KS conceptualized this as a “public health mission” (e.g., KS13, advisor; KS22, civil servant) and emphasized the “not-for-profit” orientation of the cannabis retail model in Quebec. Namely, the SQDC has no obligation to generate profit for the government: The nonprofit mission – it is really important. I think it's the most important. We have a monopoly - true, but I think it's the most important that it's the nonprofit mission; because you can avoid the trivialization and the promotion, the increase of the use. I think it's really major. (KS8, civil servant) I have no objectives in terms of how much benefit [profit] I should give back to the company. I will never be thanked for giving more, if I destroy the mission. So, mission is really first and foremost, and (…) every decision we take is: is it good for the mission? (KS10, SQDC) SAQ have to push for the sale of alcohol because they have some aim…. Every year to give some…. Millions of dollars every year to the state but with this, SQDC, they don’t have this aim to have profit (KS13, policy advisor). We are passionate about our mission at the SQDC. They are passionate about wine and spirits at the SAQ. So, it's very different. The other thing is: we do not have a mission to sell, or we do not have sales targets, whereas the SAQ is really a standard retailer, still paying attention not to sell to people without the legal age…. But the SAQ does not care about, it's not its responsibility to handle responsible consumption. (KS10, SQDC)
While the majority of interviewed KS from diverse backgrounds were supportive of the transition mission, several expressed concerns over the SQDC ability to ever transition all consumers to the legal market. KS from the cannabis industry viewed the “lack of consumer choice” (KS17, industry), lack of “product innovation” (KI14, industry), and limited number of stores (KI34, industry) as main obstacles to fully achieving the mission. On the other hand, some KS with a public health background were concerned that the SQDC's focus on their mission may lead to gradual erosion of public health protections in the future. For example, to attract more consumers from the illegal market, SQDC may need to diversify its conservative product offerings. One KS questioned the mission's emphasis on transitioning consumers, suggesting the focus should be on harm minimization and patterns of consumption: I think that [SQDC] wants to do a good job. But they are evaluated for their capacity to reach people to the point that makes it eventually impossible for the black market to do business. (…) In a perfect world, yes – 100% legal and more or less 20% [of the population] would be] consumers. But I think that even if we have 80% legal consumers, or 70%…. And even if 30% still wants to buy illegal products - because they want to have a 90% THC concentration in their products - that we shouldn't sell those kinds of products here. (KS16, public health advisor) SQDC have this mandate of not having new users, but it doesn’t matter if my mom wants to use cannabis, if she never has but she wants to try it, it doesn’t really matter. If she wants to use it seven times a week then that's a whole other issue… (KS1, independent researcher)
(2) Dedicated funding for cannabis prevention and research from SQDC profits
The allocation of SQDC profits to fund cannabis prevention, harm reduction, surveillance, and research activities was another key mechanism to protect the model from overcommercialization, identified by the KS. By law, profits from cannabis sales and the revenue from the share of federal excise taxes 2 are transferred to the Fund to Combat Addiction (originally named the Revenue Fund) administered by the Minister of Finance (Act respecting the Société des alcools du Québec, n.d., s 23.30). Importantly, the majority of revenue from this Fund (at least 51%) must be transferred each year to the Cannabis Prevention and Research Fund (CPRF) (Act respecting the Société des alcools du Québec, n.d., s 23.34; Ministry of Finance, 2022, p. 17). CPRF is managed by the Ministry of Health and Social Services, and money held in the fund is to be spent for research and monitoring, health promotion, harm reduction interventions, and prevention-related activities related to cannabis (Cannabis Regulation Act, s 58). Of note, the remaining revenues in the Fund to Combat Addiction may be used to finance activities that can be part of the broad umbrella of prevention, health promotion, harm reduction, and supply reduction—such as law enforcement activities targeting the illegal drug market or financing of low-threshold residential drug treatment services.
Many KS with public policy and health expertise expressed the view that this dedicated funding mechanism, particularly the establishment of CPRF administered by the Ministry of Health and Social Services, is key in reducing the risks of prioritizing profits over public health and safety aims. Namely, the ringfencing of profits from SQDC reduces risks of the government prioritizing sales to increase the general budget. They contrasted this approach with the alcohol monopoly and the commercial regime for tobacco, where revenues from sales and taxes go directly to the general budget: The idea is “cannabis pays for cannabis”. It's not “cannabis pays for everything”. (…) What we didn’t want is that the profits [would] go … like in the SAQ [alcohol monopoly], the profits go in the consolidated general fund - which is a concern. So, it's not the case [in the cannabis model] … the majority of the profits returns to health. (KS18, public health advisor) … different from tobacco [tax revenue] which are used to build bridges, infrastructure, and things like that. The money is not invested like that for cannabis. So it does not make us [government and public service] dependent on people using cannabis. (KS33, civil servant) At first, I looked at my colleagues and said “you know what, we gained something but we created ourselves a problem, are we able to deliver?” (KS22, public health advisor) Because if the government doesn’t have enough money at some point, and if public health [sector] is not able to spend the money they got from the SQDC, it's gonna go back to Ministry of Finance…. That's what I’m afraid of. (KS11, public health advisor) For example, if we have 300 million of profits – which is possible in a few years – we don’t need that kind of money in prevention. So – once we’re there of course there will be some reflection at the government level. The pressure will increase to have access to that money. (KS33, civil servant) [The governments] will see that there are millions of dollars of profit that they could put in let's say the roads or to the education system and things like that, rather than going only in the prevention and research. So, I’m afraid that lets say in 10 years they will say okay we need this money for other important activities of the government (…). And then they might want to push the sale of cannabis in order to have more money to fund say the universities. (KS13, academic) That's the main risk: politicians being more and more sensitive to money, and less to public health. (KS4, activist) (3) Independent legislated Oversight Committee
The Oversight Committee (Comité de vigilance), an independent advisory body to the Minister of Health and Social Services, is another key institution established by law to protect the model from commercialization. It is unique to the cannabis retail monopoly system. The Oversight Committee members (appointed by the Minister) must have expertise in health, substance use, and public safety matters (Cannabis Regulation Act, s 65) and their role is to advise the Minister on cannabis-related matters. While the Oversight Committee member selection process has been described as “political” (KS12, civil servant), the Committee acts independently and can advise the Minister on any cannabis matter, either on request of the Minister or on its own initiative. This broad advisory mandate is unique, as illustrated in the quotes below: They can submit any kind of report to the Ministry. That's quite interesting. There is not a lot of committees that have this kind of power in other matters.” (KS33, civil servant) The Committee role is really to “conseiller”, to advise the minister. So of course, [the Committee] tries to stay on topic that he will be receptive to, and that will be helpful for him. So sometimes, he gives [the Committee] some topics to work on, but also they can choose own topics. So it can be top to bottom, or bottom to top.” (KS31, advisor) We are not sure that it's a very powerful instrument, it is here but are the decision makers really listening to what they [the Oversight Committee] say? I’m not sure. (KS19, researcher) “The Committee can recommend and bring some attention on different subjects to the minister, but it's up to his own decision after [that]. And some of the subjects - he's not really interested in. (…) We have to be careful because if the committee is not taken seriously by the minister, or is not really active or accountable, it might not serve its mission in a few years. (KS24, civil society organisation) “There was some research where non-consumers mentioned that if there were more [edibles] on offer, maybe they would be tempted to try them. So, [the Oversight Committee] recommendation was that there is not enough data for the moment to develop edibles [market]. That was presented to the ministry, and a week later the edibles were on the market. But when the Committee presented the advice to the ministry, nobody said anything. (…) Nobody said: “yes, but they [SQDC] are already working on this [edible] market and at the end there will be edibles”. So, what is the purpose of [these] reports?” (KS18, advisor)
(4) Delegation of regulatory function to health agency and separation of oversight between finance and health agencies
The SQDC organizational structure and its position within government departments are other key aspects of legislative framework designed to protect the model from overcommercialization. First, health agencies have been given significant roles in the cannabis legalization process: the implementation of
Quebec Cannabis Regulation Act
and the development of regulations are delegated to the Ministry of Health and Social Services (rather than the Ministry of Finance—as is the case under the province's alcohol monopoly). Although SQDC is technically a subsidiary of SAQ (which falls under the Ministry of Finance), it is managed independently from SAQ and has its own Board of Directors. The regulations also specify areas that require cooperation between the Ministry of Health and the SQDC, for example, the agencies must work together to develop and deliver training to all SQDC employees (“Regulation C-5.3, r. 1 under the Quebec Cannabis Regulation Act. Regulation respecting training on the retail sale of cannabis and information to be communicated to a purchaser in the course of a cannabis sale.,” n.d.). Many KS from the public sector emphasized how these institutional arrangements may help prevent overcommercialization of the cannabis monopoly, for example: The alcohol monopoly is linked to the Ministry of Finance. For us, it was a big battle to make sure that it was the Ministry of Health [that] would be very … leader of the policy, engaged in the process of legalisation. (KS22, advisor) In the origins of the legislation in Quebec [it was] really the Health Ministers or the Health side [of public sector] who took the ownership at the beginning of … when the legislation was tabled, to analyse what kind of model we should have in Quebec. (KS29, SQDC) We are very critical about SAQ as a state monopoly because in no way they consider the risk of the product they sell. We are not at the same place with the SQDC. But the influence of the SAQ is real because most people who work at the SQDC come from the SAQ. So, there's a risk of certain “banalisation.” (KS16, advisor) That it is the same person [Chair of the Board of Directors of the SQDC and SAQ] who works on really, really different missions… (KS31, advisor) I have to say there was two major components for what I would qualify as a success in Quebec. First, the leadership of the health authorities in the build up of the frame, and second – the expertise of the SAQ. Without that we would have failed miserably. (KS33, civil servant) It's clear that the commercial function, i.e., the way the system functions as a “seller of products”, is a question of the commercial affair sector. And I think that the Ministry of Health doesn’t have the know-how of that. So, they [the Ministry of Health] have to make sure that the law is respected, but the law is clear about the commercialization: it has to be supervised, organized, controlled by the SAQ which is a state monopoly and has the know-how, and that's why the SQDC for the commercial function is under the SAQ, and under the Ministry of Finance. (KS16, advisor)
(5) SQDC organizational structure
In addition to the unique positioning of the SQDC within the public sector, several internal organizational structures in the SQDC have been established to support its health orientation. For example, the law requires that the SQDC Board of Directors (responsible for the strategic direction) includes members with health expertise, and permanent observers on the Board include a representative appointed by the Minister of Health and Social Services (alongside representatives from the Ministries of Finance, Public Security and Municipal Affairs). In addition, the SQDC internal Health Protection Committee was created to support the SQDC health mission
3
. However, several interviewed KS questioned the effectiveness of these mechanisms, including the membership and orientation of the SQDC Board of Directors and the role of permanent observers who don’t have voting rights. They wanted to see greater representation of health and civil society expertise on the Board, for example: There's a very good epidemiologist there, but he's never been involved with cannabis. (…) We wanted to have a public health person as a member of the board. The national director of public health sits as an observer, but then again, he doesn’t deal with cannabis very often. That board I don’t believe is useful from a public health perspective. (KS26, researcher) If you look at the people that are there…. There's [sic] no real public health representatives on that board (KS31, advisor)
Informal (Non-Legislated) Practices to Prevent Overcommercialization and Reduce Harms
(1) Communication between SQDC and government health agencies
Although there is no formal direct link or reporting line between the SQDC and government health agencies, interviewees from these organizations emphasized continued efforts to maintain regular communication. The origins of this relationship—despite it is not required by law—date back to the early stage of legalization when the public health agencies took leadership in the development of the model. For SQDC stakeholders, maintaining regular communication with the Ministry of Health and Social Services had both practical and performative functions, as it is used to validate market decisions and to build trust and relationships with their “stakeholder ecosystem” (KS29, SQDC). The quotes below are a testament to the close relationship between the SQDC and health agency stakeholders: Every time we want to change some material components of the business [we are] validating with them [Health Ministry]. It was important to make sure you, you stay in tune with your eco system, with your stakeholders so…. And on top of that every Friday morning, we had a meeting with someone in health, public health, every week. Just to inform that person how things are going, what we are doing … and that was also helping to keep the proximity. So, it is just on the willingness basis, it is not mandatory, it isn’t part of the law. It was just obvious to do that, to do the right thing - we need to do that. To create the trust as well between the two entities. (KS29, SQDC) This morning, I was speaking with the Health Minister. We are speaking every two weeks just to update on what is new on their side, what is new on our side. Sometimes some things pop up and they say, “Okay, have you heard about that?” (…) So, the line of communication is very open. (KS10, SQDC) I think another benefit is the collaboration that we can have between the SQDC and the Health and Social Services Ministry. We try to collaborate, to understand and make sure we have the same vision on the mission, product conformity and things like that. (KS8, civil servant) [SQDC] don’t have the obligation to do anything other than to respect the law, and after that it's “discussions” and “conversations”, but … I think it's fragile. I think that it depends a lot on who is in charge. If you have a CEO that has a very strong health vision, it can be easy to pursue that goal. But if you have a CEO that has more marketing vision… (KS18, advisor) We are in the context [where there is] a really good collaboration and all that. But at the same time, I’m realistic too. Maybe it depends on the person that runs it [SQDC] We can have, we could have someone say: “I don't care about health, I want to make money”. (KS7, public sector) At SQDC I think there are some people that are, you know, legitimately trying to have a balanced approach. But I think it relies on people, on people having good values. (KS27, researcher, advisor)
(2) Non-binding advice from independent (health) bodies
Publicized statements and recommendations from independent health organizations and stakeholders may also contribute to preserving the social and health orientation of the model. Although such recommendations are not legally binding, KS identified instances where advice from independent bodies has influenced SQDC into more conservative decisions. For example, in November 2019 Quebec Public Health Director issued advice not to sell cannabis vaping products in the SQDC outlets, a recommendation made in the context of the EVALI outbreak in the US (Quebec Public Health Director, 2019). As illustrated in the quotes below, the SQDC has followed this advice (at the time of interviewing), but several KS expressed uncertainty about the impact of this advice in the long term: It was the [provincial] Public Health Director who made the recommendation to not develop those kinds of products [vaping]. But this recommendation has been made like four years ago… (KS18, advisor) By law, we could sell vaping products, but there is a directive from the Public Health that is saying that we should not sell vape. It's not mandatory. We could go beyond that. But we’ve decided to follow the directive for the moment. (…) There is a lot of pressure from the customers, so we need to understand that. (KS10, SQDC) It could be very politically bad to disrespect this [recommendation]. (…) But if vaping is, say in Quebec [in the future], it can’t be flavoured [because regulation prohibit the sale of products attractive to children]. You [also] have to respect the 30% THC potency [limit]. (KS8, civil servant) (3) The influence of public opinion
Public opinion and the level of community support for SQDC's operations are another powerful influence on the company's decisions, and consequently on the extent of overcommercialization of the model. The importance of maintaining public mandate for the reform and model is explicitly recognized in the SQDC strategic plans that set a target of 75% public approval rating (SQDC, 2023b). To this end, SQDC regularly commissions customer experience and public opinion surveys, inquiring about support for the SQDC sales model and consumer experiences and expectations. 4
Community opposition to products or stores has informed SQDC management decisions on a few occasions, leading to reduced availability and product offerings. KS gave several examples of such influence, including the negative press and public concerns about cannabis vaping products at the time of the EVALI outbreak (supporting the SQDC decision not to sell cannabis vapes at the time), and local community opposition to the opening of an SQDC store in one neighborhood (terminating SQDC plans to operate in the locality). SQDC interviewees expressed they need to “demonstrate (…) the ‘good citizen’ [they] are” (KS29), when faced with community opposition: The SQDC agreed [not to sell vapes], I guess you know, it would have been difficult for the SQDC to go against it because it was really spinned around in the papers and people were worried at that point (KS2, adviser) Some citizens were feeling that we [SQDC] were [planning to open a store] too close to one school (…) But rather than calling us and speaking with us and the municipality, they’ve gone the other way which is press and made a little bit of noise. They can do whatever they want. (…) It was during an election also…. There was a lot of different events. But just after the election we said, “Okay, you have the opportunity to decide to change the [local] rules for your city, and if you decide to change the rule for your city, if we’ve not yet opened the store we will follow the rules.” And so, they’ve decided to change the [local] law and to say at the end there will be no cannabis stores in Outremont. We will never push to be somewhere if we feel like we are not welcome. (KS10, SQDC) The only structure that's preventing [commercialisation] is not the formal structure, it's an informal structure called stigmatisation. I really believe that. I think when cannabis is normalised, and it will be eventually, and I’m “for” [in support of] normalisation (…) you don’t want to further stigmatise people that use drugs. [But] you want to be cautious with that. When it is normalised I don’t see [what] will prevent it to become like the SAQ. (KS1, independent researcher)
Discussion
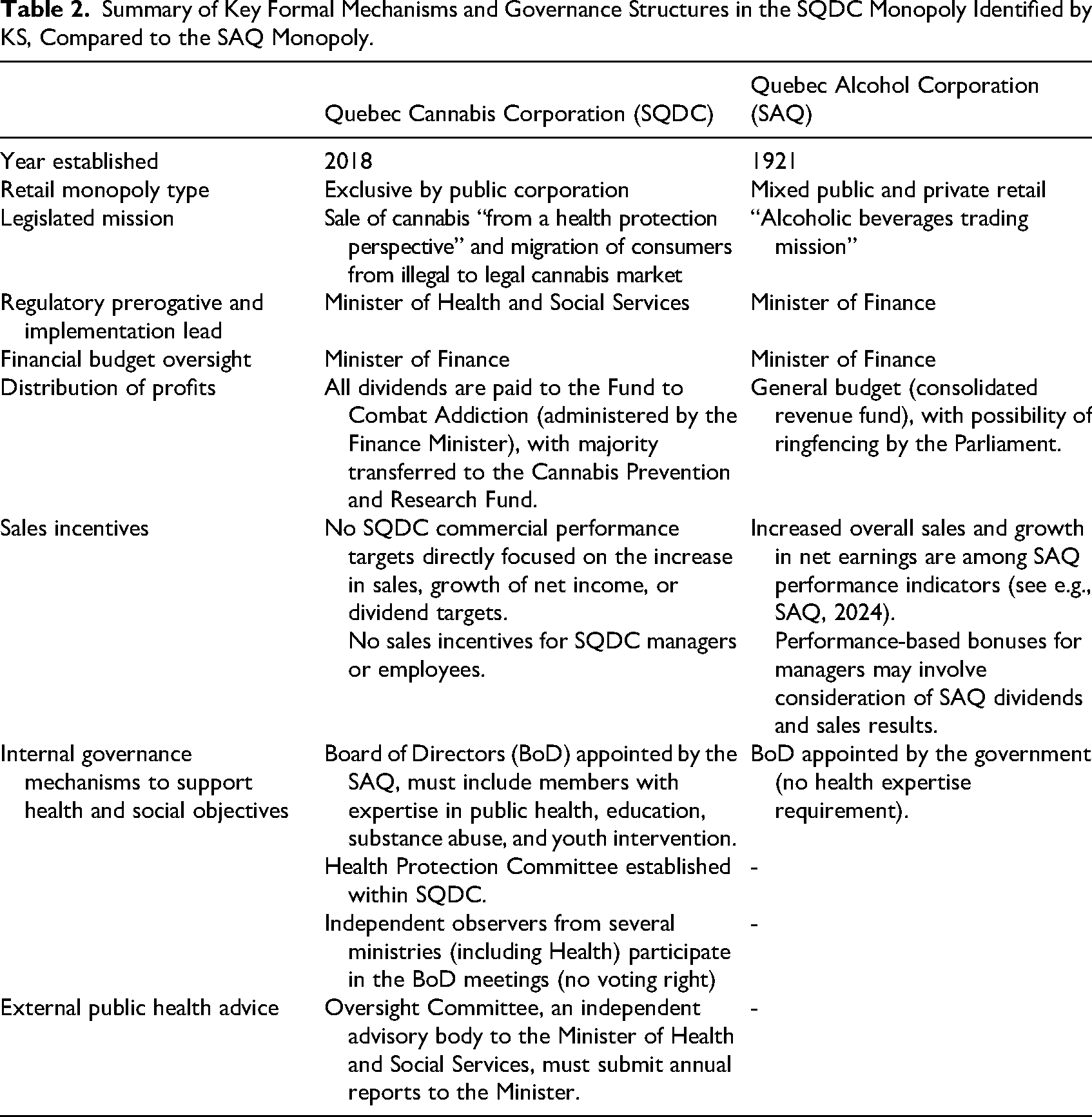
We identified key legislative, regulatory, and informal governance mechanisms developed in Quebec to protect the government retail monopoly for legal cannabis sale from overcommercialization and support its stated public health, safety, and social mission. From the public health perspective, the governance mechanisms in the SQDC model are stronger than in the similar SAQ monopoly system for alcohol. Key differences were the non-profit mission of the SQDC, the legislated Oversight Committee, the leading role of the Ministry of Health and Social Services in the development of the law and regulations, and the ring-fenced allocation of the SQDC profits to fund cannabis-related research, intervention, and prevention (see summary in Table 2). However, despite these measures, several weaknesses in the regulatory design were identified. These include the limited formal powers of the Oversight Committee, the risk from personnel linkages between the SQDC and more commercially driven SAQ, and the lack of formal reporting between SQDC and health. These concerns demonstrate that the government monopoly model for cannabis sales is not immune to influences that could steer it into greater commercialization.
Summary of Key Formal Mechanisms and Governance Structures in the SQDC Monopoly Identified by KS, Compared to the SAQ Monopoly.
There are important learnings from the Quebec model for policymakers considering a monopoly approach to cannabis legalization. First, the Quebec case study provides examples of specific legislated governance mechanisms that appear effective at protecting the health orientation of the publicly run cannabis retail corporation, at least in the short term. Key safeguards include ensuring health agencies formal input into regulatory decisions, adequate oversight mechanisms, and, importantly, the legislated public good mission of the corporation. Second, even with the legislated governance mechanisms in place, it remains important to safeguard key market levers through top-down regulation (e.g., ban advertising, regulate product classes, impose potency caps, and price controls). This top-down regulation helps protect the legislated public mission against pressures for greater availability and product offers from consumers, producers, or successive governments and management teams who may prioritize commercial rather than health outcomes. Importantly, the separation of regulatory function from the commercial function is a key feature. Third, the Quebec case study demonstrates the value of nonbinding rules, recommendations, and practices that help strengthen the overall institutional culture of public health. While these are more fragile than formal legislated protections and regulations, the Quebec regime demonstrated how these nonbinding efforts support environments for collaboration between the public cannabis retailer and health agencies and community groups.
Several formal mechanisms to prevent overcommercialization in the Quebec model identified by KS are controversial. For example, in other sectors involving risky commodities, there is a significant academic debate over the benefits and disadvantages of the hypothecated funding. On one hand, ringfencing revenue from alcohol, tobacco, or gambling to support public health and public good causes provides more stability from changing government priorities than relying on ad hoc funding mechanisms from the general consolidated fund (Doetinchem, 2010; Hancock, 2016; Room, 2016). On the other hand, critics of hypothecated levies in the gambling sector have argued that the system contributes to the community organizations becoming dependent on the success of the very industry it seeks to mitigate (Adams, 2016; Livingstone & Adams, 2016). They have also identified the risks of wasteful spending (as the actual spending is decoupled from needs) and the practical challenges of sacrificing the government's fiscal flexibility (Doetinchem, 2010). In our study, the allocation of profits from cannabis sales for prevention, harm reduction intervention, and research was not questioned by the KS interviewees in Quebec, perhaps demonstrating a more forgiving approach to the fledgling cannabis industry. However, the KS did identify some issues with the transparency and allocation of funding, illustrating the many challenges of implementing this solution in practice, consistent with experiences from other addictive industries (Rychert & Wilkins, 2020; Wilkins, 2018).
The institutional positioning of the SQDC within the public sector is another expression of a pragmatic approach to cannabis sales regulation in Quebec. By establishing SQDC as a subsidiary of SAQ, existing organizational structures, know-how, and expertise in retail management could be built on. The administrative burden involved in the creation of an entirely new entity was reduced. KS in our study recognized that this market experience was essential to the SQDC's success in the early years of legalization. In the long term, however, personnel linkages between SQDC and the commercially driven SAQ, and the mixing of different institutional cultures, may increasingly present a risk to the public good mission of the SQDC. This could be addressed by implementing new organization rules (e.g., prohibition on the holding of positions on SAQ and SQDC boards concurrently). The SQDC managers voluntarily developed regular communication with relevant staff at the Ministry of Health and Social Services, but preserving these practices in the long term may depend on the personalities of health authorities and successive SQDC managers, illustrating the fragility of such arrangements. While the law requires the SQDC Board of Directors to include members with expertise in public health and epidemiology, their actual influence on the SQDC strategic direction is yet to be assessed (Canadian Centre on Substance Use and Addiction, 2019). Additionally, the law on governance of state-owned enterprises establishes conflict of interest rules that help preserve the independence of the board from private interests. It requires that a minimum of two thirds of the board members must qualify as independent, i.e., they must not have any direct or indirect relationship or conflicts of interests including of a financial, commercial, professional, or philanthropic nature (s. 4). Cannabis-specific law imposes additional rules for the Oversight Committee whose members must not have any direct or indirect links with the cannabis industry.
The evaluation of SQDC strategy and market decisions to date, e.g., price settings, product offer, density of retail outlets, is outside the scope of this article. Several studies have started to evaluate the early health and social impact of Quebec's approach compared to more commercial approaches in other Canadian provinces. These have identified operational benefits of the monopoly retail system compared to an open competitive market model, e.g., retail outlets are distributed strategically to ensure retail accessibility to the greatest number of clients but without undue concentration and visibility (Gibbs et al., 2021). Some studies found lower rates of cannabis-related pediatric hospitalizations, likely due to Quebec's conservative approach to edible sales (Myran et al., 2023b; Varin et al., 2023). Consumers of dry flower products in Quebec have been found to be more likely to source all flower products legally compared to those in British Columbia and Ontario (Wadsworth et al., 2023), perhaps due to the fact that SQDC has had some of the lowest prices for legal cannabis products among Canadian provinces (Gibbs et al., 2021). While low prices may seem counterintuitive from the public health perspective, maintaining the prices competitive with the illegal market may be particularly important in the early years of legalization (Armstrong, 2021), explaining Quebec's success in the illegal market capture. Conversely, vape oil and edible consumers in Quebec have been found to be less likely to access cannabis edibles and vapes legally compared to other provinces (Wadsworth et al., 2023), and the use of extracts/concentrates in Quebec was lower than in less restrictive market in Alberta (Robinson et al., 2024)—these trends likely reflect the more limited product offer in the Quebec monopoly. The ability to displace competition from the illegal market may be hindered both by the conservative regulations (as is the case with Quebec's regulations on edibles and higher legal purchase age) and SQDC market decisions (as has been the case with the non-sale of vapes to date) (Koning & Mcardle, 2021; Wesley & Murray, 2021). Overly restrictive market regulation may add to harms from the use of unregulated cannabis products and exacerbate health inequities by excluding some consumers from safer tested legal cannabis products. This illustrates the challenge of enhancing the safety of cannabis consumption via strict market control and regulations (e.g., potency cap) versus maintaining an attractive product offer to attract people away from the illegal market. Current health research and evaluations do not suggest that restrictions in Quebec have been counterproductive (Myran et al., 2023b; Nguyen & Mital, 2022; Robinson et al., 2024).
There are indications that the retail government monopoly on cannabis sales in Quebec seems to work well in meeting consumer needs and creating a responsible sales environment. Perhaps the biggest barrier to the adoption of a similar model in other jurisdictions is its inconsistency with the wider competitive market philosophy, and societal and political disapproval of state intervention in the economy (i.e., reduced government paternalism). This would explain why state-controlled and government monopolies for cannabis so far have been adopted in jurisdictions with prior experience with the model in other sectors (e.g., alcohol and gambling monopolies in Quebec; water infrastructure, electricity, and energy in Uruguay). Other explanations for low uptake of the model by policymakers may include governments wanting to minimize the risk of being perceived as “endorsing” cannabis use or reducing the risk of potential legal liability for the sale of products that may cause harm.
Our analysis has identified key legislative and informal measures that may help protect the health and social orientation of the public monopoly for legal cannabis sales in Quebec against pressures for greater availability, product range, and revenue generation. The Quebec case study demonstrates how policymakers can learn from the history of alcohol retail monopolies and their decline in many countries and establish protections for the public good mission of state cannabis corporations.
Strengths and Limitations
This study drew on in-depth interviews with a range of government and nongovernment KS involved in the legal cannabis retail monopoly in Quebec, including public officials involved in the development and day-to-day operation of the monopoly. Participants’ assessment of the model will naturally be influenced by their respective roles and experience of the regime, although the confidentiality of the interviewees’ identity provided opportunities for critical reflection. We interviewed a range of stakeholders from a variety of public, private, research, and civil society backgrounds in an effort to provide a balanced assessment, although of course the group cannot be wholly definitive and others may have different views and perspectives. Like the authors, many interviewees had backgrounds in health, facilitating discussion of the monopoly model from the public health perspective. Nearly half of the interviewees (16 of 34) had experience of working in the public sector and deep knowledge of institutions, providing first-hand insights on the non-legislated measures and practical operation of the regime. By virtue of their professional roles, many KS also had experience in the alcohol policy, research, and prevention, providing comparative insights. Where possible, we triangulated information from the interviews with the law and public reports. In addition to data triangulation, techniques to strengthen study credibility included member-checking (participants were offered the opportunity to review and correct their transcripts) and peer debriefing. The authors’ public health and drug policy background shaped the study design and analytical lens. While this strengthened the analysis of public health and safety issues, it also carried the potential for under-representing other framings of drug use and policy change. As a single case study, findings are context-specific and translating lessons from the Quebec experience to other jurisdictions needs consideration of unique social, policy, and legal contexts. The focus of analysis was on identifying and critiquing the governance mechanisms and decision-making powers to preserve the public health and social orientation of the cannabis monopoly in Quebec, rather than understanding how different stakeholders view specific SQDC decisions or evaluating public health and social impacts of the retail monopoly model. Impact evaluations should be the focus of future research and analysis.
Conclusions
The legislated and informal governance mechanisms adopted in the SQDC monopoly retail model for legal cannabis compare favorably with the retail monopoly for alcohol in Quebec (SAQ). Key protections against SQDC overcommercialization include the legislated not-for-profit mission of the SQDC, the establishment of an independent Oversight Committee, the leading role of the Ministry of Health and Social Services, separation of regulatory function from market decision-making, and the ringfencing of profits to a dedicated fund for cannabis research and prevention. The model could be improved by formalizing and strengthening the powers of the Oversight Committee, separating the SQDC from past networks with SAQ, and formalizing reporting to the health agency.
Supplemental Material
sj-docx-1-cdx-10.1177_00914509261416113 - Supplemental material for Preventing Mission Drift and Commercialization of Government Cannabis Monopolies: Insights From a Qualitative Analysis of Governance Structures in Quebec
Supplemental material, sj-docx-1-cdx-10.1177_00914509261416113 for Preventing Mission Drift and Commercialization of Government Cannabis Monopolies: Insights From a Qualitative Analysis of Governance Structures in Quebec by Marta Rychert, François Gagnon, Chris Wilkins and Beau Kilmer in Contemporary Drug Problems
Footnotes
Acknowledgments
We thank all stakeholders who agreed to be interviewed as part of this research. We are grateful to Professor David Hammond for his comments on earlier drafts of this manuscript.
Ethical Approval
The study received ethical approval from the Massey University Human Subjects Ethics Committee (ref. 19/37). It is part of a larger research project investigating middle-ground options for cannabis law reform in Quebec, Uruguay, Jamaica, and New Zealand.
Author Contributions
MR—conceptualization (lead); funding acquisition (lead), investigation (lead), writing—original draft (lead), writing—review and editing (equal); FG—investigation (supporting), data collection (supporting), writing—review and editing (equal); CW—funding acquisition (supporting), conceptualization (supporting), writing—review and editing (equal); BK—funding acquisition (supporting), writing—review and editing (equal).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Marsden Royal Society Te Apārangi of New Zealand (MFP-MAU1813). BK’s work on this project was partially supported by NIDA (R01DA039293).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.