
Abstract
One-third of older problem drinkers are late-onset. So called, because their problem drinking emerges later in life, however, little is known about the epidemiology of the population's drinking behaviors. By identifying the psychosocial risk factors that inform the adverse changes in the group's drinking behavior, the article aims to contribute to a better understanding of why this subgroup of older individuals begin drinking problematically in later life. Using an interpretative phenomenological analysis approach, semistructured interviews were undertaken to investigate the retrospective, “active” drinking narratives of nine late-onset problem drinkers and nine early-onset problem drinkers; individuals who began drinking problematically much earlier in their lives. All the participants are in recovery and are ≥50 years old. The interviews, which took place toward the end of the COVID-19 pandemic, were undertaken online and are predominantly framed within a UK context. The group themes that emerged, highlighted that comorbid mental health problems were prevalent across both groups, however, difficulties with emotional regulation were more prevalent among the early-onset cohort. The late-onset participants’ narratives suggest that excessive alcohol consumption may be a coping mechanism for the multifarious issues, typically associated with ageing, particularly retirement or changes in employment status. Regardless of the many differences in psychosocial characteristics between the early- and late-onset cohorts, the consequences of their problem drinking were similar. Nonetheless, challenges to identity, the impact of major life events, and the role of meaning and purpose in life among the late-onset group, has implications for many “social drinkers” as they age, particularly those approaching retirement.
Keywords
Introduction
In 2019, 3.7% (209 million people) of the world's adult population (over 15-years old) were alcohol dependent. Moreover, alcohol which is the seventh highest risk factor for mortality- and disability-adjusted longevity (Gakidou et al., 2017), was responsible for 2.6 million deaths worldwide (World Health Organization [WHO], 2024). It is clear that the consequences of alcohol-related harm are a burden on the human and financial resources of global healthcare systems (Manthey et al., 2021). In England in 2019, for example, the cost to the NHS was estimated to be £3.5 billion (NHS England, 2019) and £21 billion to wider society (Parliament. House of Commons, 2023). One of the major challenges to healthcare systems and society generally, is an ageing population, which arguably, is partially due to advances in healthcare and medicine. People over 60 will have almost doubled from 12% of the world's population in 2015, to 22% by 2050 (WHO, 2022). Additionally, older individuals are drinking more than previous generations, while young people are drinking less (Maclean et al., 2022). According to NHS England (2022), the generational divide shows that the frequency of alcohol consumption increases with age, that is, 16- to 24-year-olds are the least likely cohort to drink every week, while 55- to 64-year-olds are the most likely (31% vs. 59%, respectively). Similar, contrasting age-related alcohol consumption ratios (between younger and older cohorts) have been reported in the United States (Breslow et al., 2017) and Australia (Livingston et al., 2016), suggesting that this is an international trend.
Due in part, to the ageing process, the age group most affected by alcohol-specific deaths in the United Kingdom are 55- to 59-year-olds (Statista, 2024). The physiological changes that occur later in life, for example, greater sensitivity and reduced tolerance to alcohol (Crome & Crome, 2018), mean that the harms associated with excessive alcohol consumption also increase with age (Giordano & Beckham, 1985; Wadd & Galvani, 2014). The decline in physiological, cognitive, and mental functioning associated with ageing also means that older individuals are increasingly likely to use prescribed medications, many of which may be alcohol-interactive and associated with detrimental outcomes (Holton et al., 2020). In their response to the Commission on Alcohol Harm (Alcohol Health Alliance, 2020), Age UK (2020, p. 3) stated that “evidence clearly demonstrates that harmful drinking is a growing problem amongst older people,” something that has been recently exacerbated among the 50- to 70-year-old age group by the COVID-19 pandemic (Centre for Ageing Better, 2020; Seddon et al., 2021). Furthermore, because of the scarcity of alcohol and other drug services specifically purposed for older people in the United Kingdom, just 7% of older adults in need of treatment for problem drinking were seen in these services (Crome & Crome, 2018).
Additionally, in UK primary care settings, alcohol is currently not viewed as a priority (Madden et al., 2023). Indeed, the latest report on alcohol treatment services, managed by The Department for Health and Social Care, concluded that, “We are concerned that the Department is not taking alcohol harm sufficiently seriously” (Parliament House of Commons, 2023, p. 5). An under-stated summation, in an age of governmental-directed austerity, which has been estimated to have reduced UK public spending by half a trillion pounds in the years between 2010 and 2019 (Progressive Economy Forum, 2023). This is despite the National Institute of Clinical Excellence (NICE), recommending since 2010, that all adults be screened for harmful levels of alcohol consumption (NICE, cited in Mansfield et al., 2019). Bareham et al. (2021, p. e762) who reported, “That there are clear opportunities to support older people in primary care to make healthier decisions about alcohol,” have recommended training for healthcare professionals working in primary care settings, so that they are able to identify alcohol-related harm in older patients.
Many of these older individuals are “late-onset,” a distinct category who constitute one-third of all older problem drinkers (McGrath et al., 2005). Zimberg (1978), who identified this group of problem drinkers, coined the term “late-onset,” arguing that the change in their drinking behavior was “a response to the stresses of aging” (pp. 27–28), including retirement, isolation and bereavement (Emiliussen et al., 2019; Holley-Moore & Beach, 2016; McInerney et al., 2023; Wadd et al., 2011). The premise of the current paper is that these challenging emotional and psychological events culminate in late-onset problem drinkers experiencing a lack of purpose in life. Therefore, the study is framed within Viktor Frankl's (1963) theory of meaning (logotherapy), particularly his “existential vacuum” concept, a feeling that life is without meaning and purpose (MPL). Frankl (2011) proposed that the vacuum's symptomatology was comprised of “depression, aggression, and addiction,” adding that addiction could “at least partially be traced back to the feeling of meaningless” (p. 26).
Although a vast body of work has investigated alcohol harm comprehensively in a general context, limited research has been undertaken on late-onset alcohol use disorder (AUD)/problem drinking since Zimberg's (1978) first account of this unique cohort. It is important to address this dearth of reporting because problematic alcohol consumption among older adults is being under-detected and misdiagnosed (Taylor et al., 2014). The current paper, therefore, aims to contribute to a better understanding of the psychosocial characteristics of late-onset problem drinkers and associated risk factors, which in turn, can better inform healthcare professionals and recovery practitioners, why this group of older adults begin to drink problematically. The study's focus is on the psychosocial characteristics of late-onset problem drinkers before they found recovery. To that end, the study investigates and considers the differences and meaning contained within the retrospective, “active drinking voices” of early- and late-onset individuals, now in recovery. In contrast to their late-onset counterparts, early-onset individuals develop a problematic relationship with alcohol when they are considerably younger. This study aims to answer the following question: How do the psychosocial risk factors associated with AUD/problem drinking differ between early- and late-onset problem drinkers?
Method
Guided by Frankl's (2014) description of logotherapy as an adaption of “the phenomenological methodology” (p. xvi), semistructured interviews using interpretative phenomenological analysis (IPA) was considered to be the most appropriate method of investigation. The interviews took place towards the end of the COVID19 pandemic and therefore, were undertaken online, using Microsoft Teams.
Sample Size, Recruitment, and Participants
Participant criteria were individuals of ≥50 years old, in recovery from AUD/problem drinking. Jonathan Smith, a leading figure in IPA, has undertaken studies with a sample of nine (Osborn & Smith, 1998). Following Osborn and Smith's (1998) example and because the two cohorts were effectively, two heterogeneous groups (i.e., early- and late-onset), 18 participants were recruited, nine for each group. The current study is part of a broader project, which included a quantitative study that gathered data from an online survey/questionnaire (McInerney et al., 2024). The sample for that study was recruited by contacting several prominent recovery organizations, the R&D department of an NHS Trust, and posts on “recovery-focussed” Facebook groups. Survey respondents who wished to be considered for the qualitative phase of the research, that is, interviews, were invited to insert their email address in a box at the end of the demographic section of the survey; potential participants were then contacted by the research team. When interview times and dates had been arranged, Teams invitations and informed consent forms were sent to respondents. Before each interview was undertaken, there was a complete discussion of the study with the potential participants. If they were agreeable, participants signed and returned the informed consent form to the research team.
Data Collection
Before undertaking the interviews, the interview schedule was first piloted on members of Alcoholics Anonymous (AA) and amended accordingly (Appendix 1). The Teams transcription function was used to transcribe the interviews. However, the function tends to misinterpret speech and its effectiveness in producing accurate interview transcripts depends on the clarity, enunciation and accent of the interviewer and interviewee. Because of this flaw, the audio was also recorded. The transcripts were downloaded, and carefully corrected, whilst listening to the audio recording, to produce verbatim transcripts. Participants’ names were anonymized.
Analysis
It is important to note that typically, contained within the retrospective narrative accounts of problem drinkers are two, distinct voices: the “active drinking voice” and the “voice of recovery,” although these different voices are rarely acknowledged and/or analyzed separately. The current study, however, recognizes these two contrasting voices and in line with the study's aim, analysis of the participants’ narratives focussed on the “active drinking voice” only. Analysis followed recent IPA guidelines recommended by Smith and Nizza (2022). Additionally, Smith et al.'s (2009) original guidelines were a practical point of reference throughout analysis. Because of its idiographic approach (i.e., the interpretation of individual cases), IPA allows the researcher undertaking analysis insight into “how meaning making occurs” (Smith & Nizza, 2022). IPA is a time-consuming and iterative method. The first step involved reading each participant's transcript at least twice, to become familiar with the individual participant's data. While reading each of the participants' transcripts exploratory notes were recorded.
The overarching aim of notes, however, is not to identify themes, “but rather to consider a range of potential meanings” (Smith & Nizza, 2022, p. 38). During this phase, the interpretative phenomenon of the double hermeneutic occurs, that is, the researcher becomes immersed in the text and attempts to make sense of the participants, who in turn, are attempting to make sense of their own discourses. The final stage of analysis involved finding links between the individual participants in each group. With a focus on interpreting human meaning making, from the study's theoretical perspective, IPA is very much in accord with the overarching premise of Frankl's theory, that is, the primary human motivation is to find meaning in, and to one's life. From an empirical perspective, IPA can be advantageous; as Smith and Nizza (2022) point out, following their “systematic series of steps,” means that someone else is able to follow and review “the audit trail” of the process (p. 32).
A Note About Terminology
Smith and Nizza (2022) have revised IPA's analytical terminology to reflect IPA's primary theoretical focus, that is, the “lived experience” and “meaning making” of participants; again, this is in accord with Frankl's theory of meaning. “Emerging Themes,” are now Experiential Statements (ESs), “Individual Superordinate Themes” have become Personal Experiential Themes (PETs), while “Group Themes’” are Group Experiential Themes (GETs).
Results
Description of Sample
All of the participants live in the United Kingdom (with the exception of Steffen, who lives in the United States); the participants’ narratives, therefore, are overwhelmingly framed within a UK context. All the participants viewed recovery within an abstinence-based framework (e.g., Harrison et al., 2020). The mean age of the two cohorts was similar; the early-onset cohort ranged from 50 to 71 years old (m = 60 years old), while the late-onset cohort ranged from 53 to 67 years old (m = 61.7 years old). However, there was a considerable difference in recovery years between the groups. The length of time in recovery for the early-onset participants ranged from 18 months to 35 years (m = 12.27 years), almost three times as long as the late-onset group, which ranged from one to 15 years (m = 4.6 years). There were five females and four males in each group. Table 1 summarizes the participants’ personal characteristics.
Personal Characteristics of the Participants.
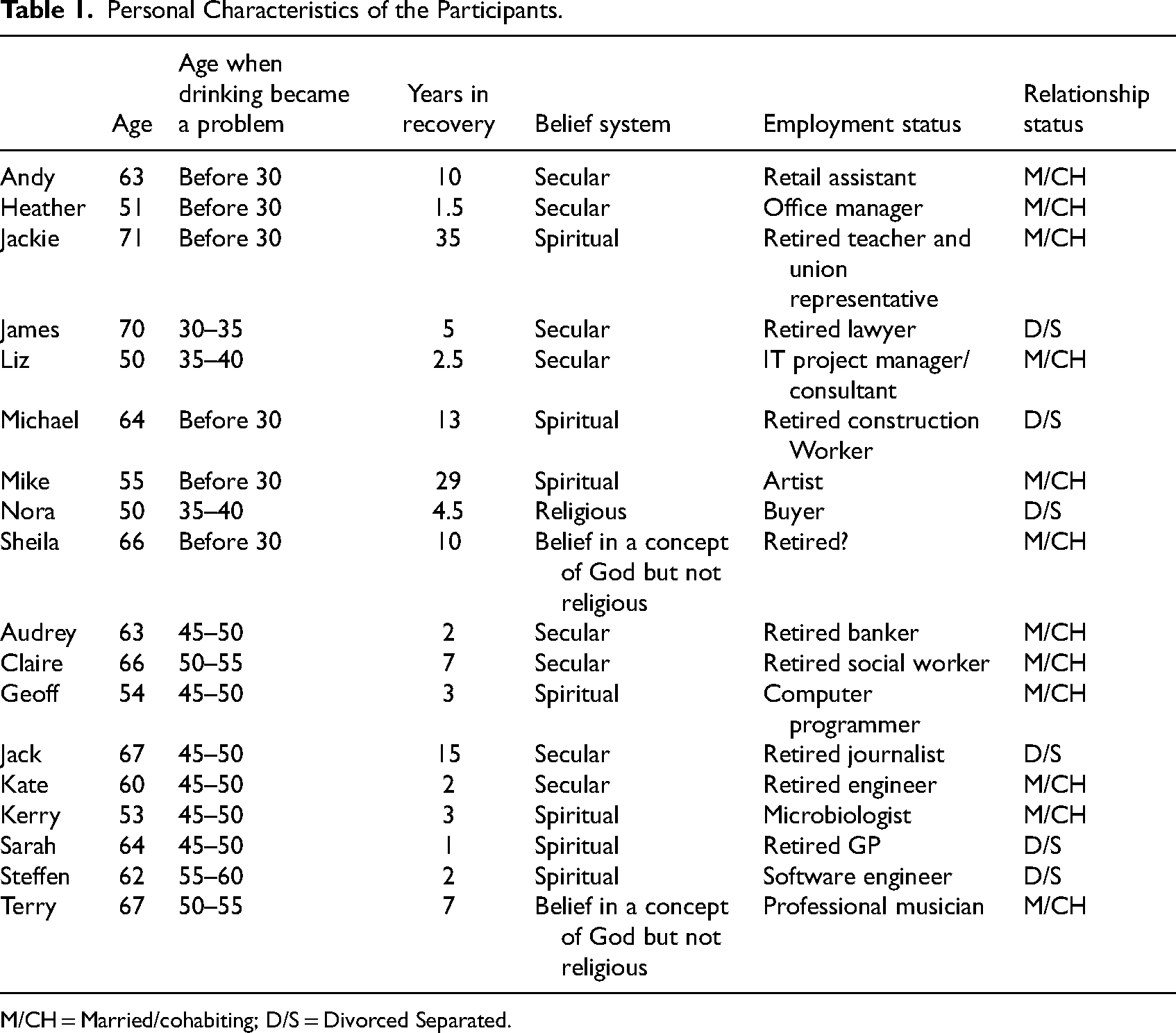
M/CH = Married/cohabiting; D/S = Divorced Separated.
Acknowledging the Possible Impact of Bias and Memory on the Data
The participants, predominantly, can be categorized as having a high socioeconomic status (SES; refer to Table 1), suggesting the possibility of self-selection bias. That is, people who volunteer to participate in research often share several characteristics: they tend to be better educated, have a higher SES, and are interested in the topic of the research they are volunteering for (Nikolopoulou, 2022). Additionally, the retrospective nature of the interviews gives rise to the likelihood of two confounding variables, (a) memory recall and (b) the probability that individuals may “deliberately falsify their answers” (Davies, 1997, p. 83); however, neither of these variables can be controlled for. Additionally, because many of the participants in the current study have been in recovery for a considerable time, particularly those in the early-onset cohort, memory recall is a major consideration.
Narrative Extracts
The remainder of the results section focusses on presenting extracts and analysis of the participants’ retrospective accounts (PETs) of their “active” drinking, which embody the GETs of the cohort they are affiliated to. There were four GETs for the early-onset cohort and three for the late-onset group (Figure 1). To make them more manageable, the third GET in each cohort was divided into two subthemes.
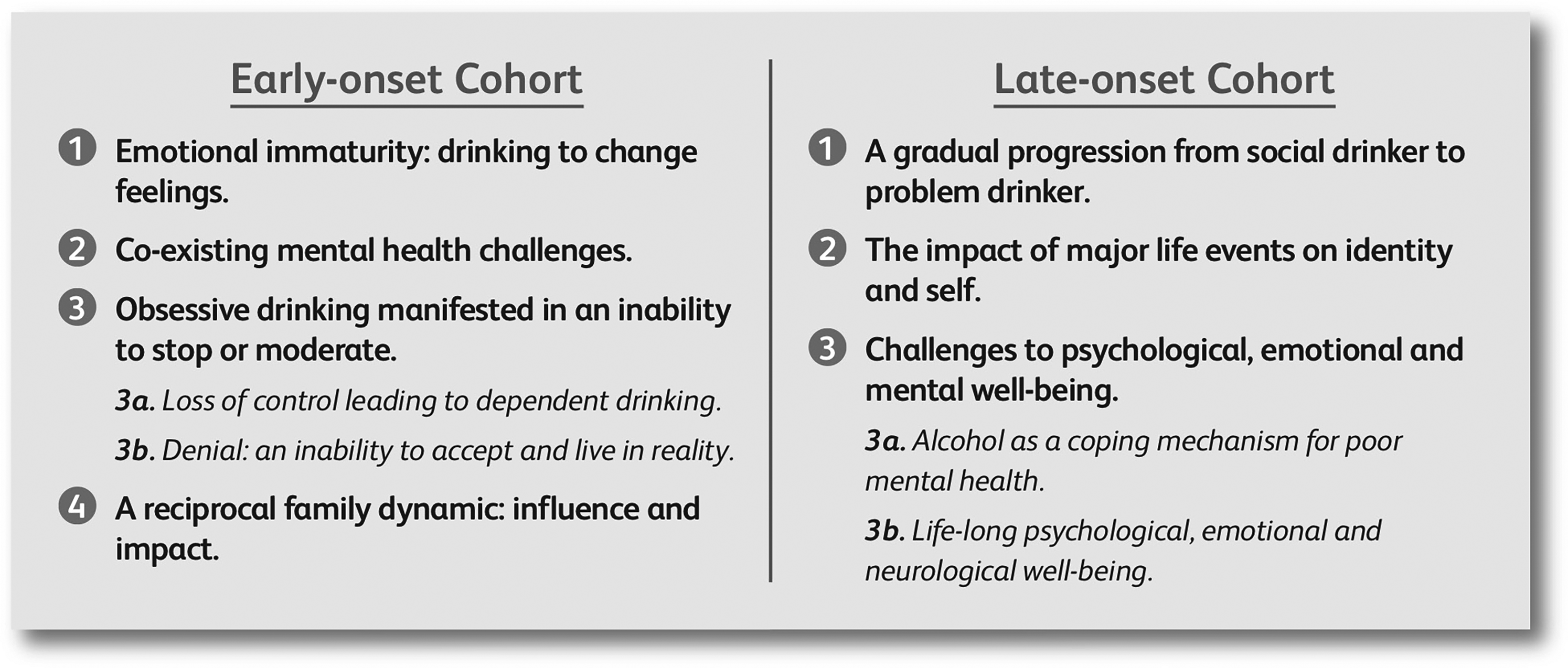
Early- and late-onset GETs.
Early-Onset Group Experiential Themes
Early-Onset GET 1—Emotional Immaturity: Drinking to Change Feelings
Mike talks about the agency that alcohol allowed him to change his emotions and feelings. Mike describes, powerfully, having a dramatic personality change when he drank excessively, comparing his own alcohol-induced transformation with the dual personalities of Dr Jekyll and Mr Hyde. In common with Dr Jekyll, who was aware of the chaos that ensued when he drank his potion and transformed into the sociopathic Mr Hyde, the sober Mike too, was aware of the chaotic consequences of his drinking.
It was, you know, I chose to do it, and I was in control of it. But in the same way, Doctor Jekyll picks the bottle up and drinks it. He knows what it's going to do to him, but chooses to pick it up and drink it, and that's why it's such a powerful story for me, because he knows.
So, I became the classic Doctor Jekyll, Mr Hyde story which all alcoholics identify with. So, I was a responsible, caring individual. Put the drink in me, I’ll become an irresponsible, uncaring individual, selfish more selfish. So, the demons were allowed out of the bag when I drank… (
In common with many people, Michael drank, partially, to relieve social anxiety. Alcohol enabled him to behave in a gregarious, uninhibited way, that was not possible when he was sober. Michael's social anxiety was accompanied by a multitude of negative emotions, including an ever-present feeling of fear. Michael talks about being “feared up as a kid.” So, when he came across alcohol at a young age, he found his antidote to fear; alcohol became the solution to Michael's emotional conundrum. The solution, however, eventually led to feelings of shame, which in turn, generated low self-worth.
I could do things, that I would probably be feared up to do, if I wasn’t, if I didn’t have a drink inside me, you know. I could talk to people, I could talk to anyone in the pub with a drink, but without a drink, I would have been in the corner minding my own business, too frightened to say anything.
… You took that drink out of me, I was, I was a frightened little lamb, you know. I couldn’t face anyone and at the end of the drinking, I don’t think I, I don’t think I ever saw a tree because I was always looking down on the floor because I was always ashamed of myself, the way I’d become. (
Conclusion to EO Theme 1
Most of the participants in the early-onset cohort found it difficult to regulate their emotions. Challenged by a plethora of negative feelings and emotions, including fear, anxiety, and low self-esteem, that had manifested very early in their lives, they soon discovered that alcohol removed these negative emotions and, temporarily, changed the way they felt.
Early-Onset GET 2—Co-Existing Mental Health Challenges
It is common for early-onset problem drinkers to experience comorbid mental health challenges (e.g., depression and anxiety); seven of the participants in the early-onset cohort reported experiencing poor mental health. In common with Michael's narrative (above), Heather started using alcohol to cope with her emotional immaturity and social anxiety when she was young. Clinically diagnosed with depression and anxiety, Heather self-medicated to anesthetize her intrusive and negative mental activity, using a cocktail of alcohol and prescription drugs. So, in the back of my mind, I’ve always had … worried about… I’ve suffered about three terrible bouts of depression, emh, also one that led me to quite bad suicidal thoughts, again, all the way through this, even though I’m taking medication apart from after I’d had Zoe because I was like, zombified, I would drink along with my medication because it, it turned my brain off. So, a lot of my drinking, I would say, did start off from self-medicating, to try and turn off my brain, to do with depression or psychosis … (
The term “self-medicate” is a linguistic thread, used throughout the participants’ narratives. Nora, for example, used alcohol as a method of self-medicating the mental anguish she had experienced while trying to conceive.
And, ehm, then I had a rough time because I had, I had an ectopic pregnancy, and I also had, ehm, a cyst at the same time, which ended up me having two operations and then not being able to conceive another child.
… and I did start to self-medicate, you know, I started to feel very depressed, ehm, ‘why me?’ Ehm, had time off work to recover from the operation. Ehm, but then my drinking really took off around that time. (
Sheila had a multitude of mental health and neurological issues, including obsessive compulsive disorder (OCD), anxiety and paranoia. In truth, like many people who experience mental health and neurological challenges, Sheila's OCD, anxiety, and paranoia were mutually supportive; Sheila still experiences OCD but finds it is manageable in recovery.
Ehm, I didn't ‘wanna go out the house, so it made, it made my OCD even worse, as well.
My, my physical, my physical well-being was very, very jittery… I went to private, private counselling, ehm, way before joining A.A., and I’ve also had private counselling since […] it's, it's less than, now. When I was drinking, it was, it was, it was on me the whole time. (
Conclusion to EO Theme 2
The theme confirms the high prevalence of co-occurring mental health problems in individuals who experience AUD/problematic drinking, with depression and social anxiety disorder the most prevalent condition among the group. Very early in life, in common with the first theme, the early-onset cohort found that they could self-medicate their poor mental health with alcohol.
Early-Onset GET 3—Obsessive Drinking Manifested in an Inability to Stop or Moderate
3a: Loss of Control Leading to Dependent Drinking
The third early-onset GET is divided into two subthemes. A prominent characteristic of the early-onset cohort during analysis was an all-consuming obsession with alcohol (in varying degrees). In this group of early-onset drinkers, the obsession often returned after varying periods of sobriety, accompanied by an irrational plan. After a period of sobriety, Nora, for example, decided that drinking only at weekends was a good plan. I’m going to drink, you know, just at weekends, I’m ‘gonna drink safely and I’m ‘gonna have alcohol-free days. I’m gonna do all this, and I’m not ‘gonna go back to it, how I was before. But it didn’t take very long for me to go back to old habits. Ehm, so, as soon as I picked up that first drink, I was wanting my second, and me third and me fourth. And, you know, I slowly then started to drink secretly, because, you know, here's me, I've been through recovery, you know, I’ve been for a detox, and I’ve started drinking again and then it all went downhill from there. So, the shame, the guilt, the remorse was all over me again. (
Conclusion to EO Theme 3a
The loss of control and obsessive alcohol cravings that are typically associated with alcohol dependence that emerged in the discourses of all the early-onset cohort (with the exception of Mike) are, in part, the consequence of the emotional and mental challenges, apparent in the first two themes.
3b: An Inability to Accept or Live in Reality
Heather normalized her drinking, comparing it to a constructed version of a typical “alcoholic,” convincing herself, and others, that her drinking did not fit into the same category. Heather's version of a problem drinker was an individual who drank every day, especially in the morning. But we, we made rules up to say we’re not alcoholics, I don’t drink on a Monday, and I don’t drink on Thursday, and if I was an alcoholic, I would drink every day of the week, wouldn’t I? … And, and if you’re not having vodka on your cornflakes then you can’t be an alcoholic… ( I remember a woman at work saying to me, Janet, you’re really lovely and you know, you’ve got a lot going for you, but you really don’t need to drink as much. And I remember thinking, what a bloody stupid thing to say. You know how? What a ridiculous, non-sensical … So, at that point I just had no idea. The denial was so massive, I would just wasn’t going to hear it. (
Conclusion to EO Theme 3b
This second subtheme described the difficulty that some members of the cohort faced in accepting a shared reality, instead creating their own version of reality, reinforced by denial. The second extract (Jackie) illustrates how the perception of the early-onset problem drinker and that of the person observing them, are contrasting constructs, whereby the denial of the early-onset problem drinker, automatically filters out the reality perceived by the observer. The two subthemes that constitute the third theme show that the use of alcohol to cope with negative emotions and poor mental health, eventually stopped working, and that the early-onset cohort's inability to stop or moderate, was confirmation of alcohol dependency.
Early-Onset GET 4—A Reciprocal Family Dynamic: Influence and Impact
The influence and impact on the family featured in the accounts of six of the participants. The relationship between the participants and their families, in the context of alcohol, was a dynamic one. That is, not only was their drinking influenced by growing up in a family environment that normalized alcohol, but their own drinking behaviur had a reciprocal negative impact on their friends and families. In Mike and Heather's narratives, for example, attitudes towards alcohol are normalized and even encouraged.
I had an alcoholic family … My whole family was riddled with people who drank. My nan used to get a bottle of brandy and three bottles of whiskey every week, and she used to pour it in her tea, pour it in the teapot. You know, it was just everywhere. It was awash, awash with it.
So, it was not strange I was drinking as a child. They would give me drink because that's what we all did. And they thought it was well, you might as well be drinking now because you’re going to be drinking later. So, you know, they used to put it in my bottle when I was a baby. ( I used to go and drink wine in the precinct with my friend, my dad made homemade wine … Ehm, and going back to my dad, even when I first passed my driving test and I was eighteen, my dad actually taught me to drive and as a present, he bought me a bottle of vodka. I mean, who would do that for a daughter who's eighteen years old, buy her a bottle of vodka to say congratulations for passing your driving test? (
The negative, emotional impact that Nora's drinking behavior had on family relationships was evident. The shame, remorse and guilt she was feeling was further magnified by her family openly questioning her behavior.
So, the family was starting to say, you know, take it easy today, you know. Ehm, my husband had said, “just take your time when you’re drinking”… Ehm, family started to notice, you know, get togethers, I’d, I’d be drinking. Ehm, I ruined my ex-husband's mum's birthday because I turned up drunk.
… Ehm, I got found on a roundabout, on the middle of a roundabout, smashed all my face in, ended up in hospital, through drink. Ehm, I had my brother crying. You know, asking me to stop. (
Conclusion to EO Theme 4
Theme four highlights the influence and impact that family drinking cultures can have on early-onset problem drinkers, as well as the reciprocal negative impact the behavior of the problem drinker has on the family.
Late-Onset Group Experiential Themes
Late-Onset GET 1—A Gradual Progression From Social Drinker to Problem Drinker
The first late-onset theme is common to eight of the participants. Two strands run through the theme. Firstly, the participants’ narratives suggest that the transformation in their drinking behavior was not a sudden event. The second strand highlights that the transition from social drinking to problematic drinking was like crossing an invisible line. The baseline for the participants’ alcohol consumption, before it became a problem, can be described as social drinking, whether it was occasional, regular but moderate, or sometimes drinking above the recommended guidelines. Kerry's extracts highlight both, her status as a typical social drinker and her gradual progression toward crossing the invisible line to problematic drinking.
I think I always was a drinker; do you know what I mean? I, I was a social drinker and I suppose it was just like, I looked around at my peers and it was, yeah, I’ll go for a few, for a few drinks on a Friday night and things like that.
And then it went to drinks a couple of evenings a week and then it was every night and then it was, you know, every afternoon, and then it was all day. (
Claire's narrative is similar, however, whereas Kerry admitted to “always being a drinker,” Claire went further, by declaring that she was “always a heavy drinker.” When Claire described the progression of her drinking from heavy social drinker to problem drinking, she was reluctant to describe it as dependent, framing it rather as a “habit.” Big habit, it was getting more and more and more, and it was hard to get out of the habit of not having a drink. Ehm … in spite of it causing me difficulties. Ehm, and I did all the usual things that people do, you know, try to stop, try to reduce, have a little go at stopping, and picked up again with a couple of hospital spells. (
In contrast to Claire, Audrey had not been a heavy drinker. She admitted drinking every day “but not to excess”; Audrey and her husband would have one or two drinks at home in the evening after work. Audrey's transition from social to problematic drinking began when her husband stopped drinking in the evening; Audrey realized that she couldn’t do the same. I suddenly started secretly having a bottle hidden that I could have a small amount on Monday through Thursday […] a unit or two of vodka would be enough for me at the end of the day, but I needed that unit or two and eventually it wasn’t quite enough. (
Terry believed his drinking was social, even though as a musician he used alcohol to self-medicate his performance anxiety. Terry recalls the progression of his drinking, however, there is no anecdotal memory of a time when he “crossed a line” from social to problematic drinking. Indeed, his social drinking “just vanished.”
I tried to control, umm that uh, self-medication. In the ensuing years, and by and large, I did control it, but of course the level of medication went up.
That self-medication gradually, more and more it took over as absolutely the main drinking. They ran side by side the two types, but in the end, the other type, the social drinking, just vanished altogether. It was self-medication and nothing else. (
Jack, another heavy social drinker for much of his working life, believed that he had control over his drinking, which had become a part of his everyday life. He recalls that his drinking changed later in his career when he began to use alcohol to cope, after his contract as a freelance journalist was not renewed. This may have been the point when Jack crossed an “invisible line.”
… for most of my working life in journalism and in public relations, alcohol was there, but I feel it was controlled. Ehm, you know, I used my car for a lot of my PR working and a lot of journalism, so, I was careful in what I was drinking.
… alcohol was probably just a normal part of my life but always on a controlled basis, it was only when the thing about, the lack of security that came from the contract not being renewed that I began to use alcohol as a crutch to get me through, that kind of day-to-day basis […] coming home and my first port of call was the whiskey, in the cabinet, which became, eventually over a course of about five years, a bottle of whiskey per night … (
Conclusion to LO Theme 1
As indicated by the theme's title, the late-onset group's descent into problem drinking was a gradual process, even though a few members of the cohort were heavy social drinkers. That said, although the change in drinking behavior was gradual, most of the group experienced an event, or series of events, that acted as a catalyst for a considerable increase in alcohol consumption, which in most instances were associated with a change of job role, or loss of job, and a subsequent impact on their professional identity. In contrast, the problematic relationship the early onset cohort had with alcohol was more sudden, mostly a reaction to a lack of emotional regulation. The early-onset group's drinking could never have been described, at any time, as social drinking. This theme highlights one of the major differences between the groups, that is, the gradual emergence of problematic drinking in the late-onset cohort, which in most instances culminated with a tipping point event, compared to the earlier and seemingly more sudden descent into problematic drinking, of the early-onset group, which was due, partially, to an inability to regulate and manage emotions.
Late-Onset GET 2—The Impact of Major Life Events on Identity and Self
Major life events impacted considerably on seven of the nine late-onset participants. This theme permeates the other themes and can be seen in Jack's experience of not having his contract renewed (highlighted in the previous theme). Challenges to their professional identity, as experienced by Jack, affected all seven participants; five of them talked directly about the impact that major changes in their professional working lives had on their identities and consequently their drinking behaviors. For example, Sarah, a high achiever, had been to medical school. It wasn’t a part of my identity it was my identity (Sarah emphasises this statement). Being a doctor, being a working mother was my identity (again emphasised). (
Identity had always been an issue for Claire, who grew up in care. When Claire, a social worker, changed from a role that she had been doing for a long time, to a more demanding role, her ego and her identity were challenged. Previously, she had “operational contact with people,” whereas the new role was purely administrative. There was also a change in power dynamics. Whereas once she “had authority to say to people, whether you like it or not, you’ve ‘gotta do it”; her new role meant that she didn’t have the same level of power.
When, you know, when I got to the point, “I need a drink”, that was fairly late on. Ehm … And on top of that, I would say that, coupled with the identity thing, that there's a lot of stuff around that, you know, stuff about, “Is that what I was doing?” Was I doing it to dampen things down or to buck me up or, you know, whatever?
(
Kate's identity was also challenged by changes to her employment status. Due to bullying, Kate resigned from a role she had since leaving school. Her professional role was the core component of her identity. Even though she won an industrial tribunal case on the grounds of sexual discrimination and harassment, no longer having her professional role, had such a negative impact on her sense of self, she began drinking to “oblivion.” Kerry, on the other hand, had to give up her job because of her health; more than anything else, losing her professional role affected her identity and her drinking. I, ehm lost my job, and it's a job that I had since I had left school … It was something that it, it was something that I used as my identity, “I’m a woman engineer”, I was rare […] I started drinking heavily then and the only word in my brain was oblivion. For years after that was oblivion. That's all I wanted to do just find oblivion because I’d lost my identity. ( I didn’t go to university ‘till I was twenty-three. Ehm, and then I, I kept studying and studying, got two degrees and then did my masters, and it was all, you know, break the glass ceiling all that sort of thing, and then suddenly I couldn’t work anymore, and it just robbed my … I had nothing to do. I probably felt adrift, I had absolutely nothing. I had no concept of myself outside of my job and my work, you know […] I had absolutely no idea of who I was. (
Conclusion to LO Theme 2
Affecting seven participants, the theme is unique to the late-onset cohort. The participants’ narratives suggest that major events, mostly relating to challenges around their work and professional identity, had a considerable impact to their sense of self, which in turn impacted on their alcohol consumption. This theme highlights, that in this cohort of late-onset problem drinkers, professional identity made a considerable contribution to a cohesive sense of self.
Late-Onset GET 3—Co-Existing Mental Health Challenges
3a: Alcohol as a Coping Mechanism for Poor Mental Health
With the exception of Jack, the late-onset participants, in common with their early-onset counterparts, used alcohol to self-medicate co-occurring mental health problems; challenges that manifested mostly as anxiety and depression. Familiar with the symptoms associated with both conditions, Sarah, a qualified medical doctor, self-diagnosed. … alcohol took my anxiety away […] I thought “I’m depressed”. I had all the symptoms I had early morning waking as well, I had all the classic symptoms of depression. I thought I needed to take a couple of months off work or whatever, and I went and got some anti-depressants. ( … in my marriage we started, ehm, had started drifting apart. You know, we had some issues, so I was … I didn’t really have anything going for me and alcohol became the, you know, I, I became depressed, you know, I would say very depressed, ehm, I just, you know, gradually went from, ehm, you know, drinking on the weekends to also drinking after work in the evening to, ehm, you know, always having a drink. (
Conclusion to LO Theme 3a
As a whole, this theme is congruent to the second early-onset theme, once again highlighting the comorbid relationship between poor mental health and problem drinking, regardless of the age of onset. With the exceptions of Jack (late-onset) and Mike (early-onset), all participants in this study reported poor mental health and using alcohol to self-medicate.
3b: Life-Long Psychological, Emotional and Neurological Challenges
The last late-onset subtheme highlights the psychological, emotional, and neurological challenges. When he was 62 and in early recovery, Steffen was diagnosed with attention deficit hyperactivity disorder (ADHD) and was prescribed the appropriate medication (Adderall). For Steffen, the medication was a “game changer.” Before his diagnosis, he described his life as, “like having, I don’t know, fifty televisions going, all at the same time, right?” Importantly, his diagnosis also explained the difficulty he had experienced in his inability to regulate emotions, confirming what he had suspected when he was drinking, that alcohol was a symptom of something more deeply ingrained. Interestingly, Steffen's discourse, once again, picks up the “emotional” strand that unites all the themes of the participants in both cohorts.
I knew, like, it wasn’t just alcohol was the problem, you know? I knew it was more than that […] my childhood wasn’t so great, right? And the problem I had with opiates in my teens was really the first time, the only time I didn’t have this, like emotional pain, sort of thing, it was like, definitely self-medicating. And so, for me, the alcohol just eased the tension and the stress and numbed me out, so, it sort of lifted that weight that I was feeling all the time. You know, I could, I could zone out and not have to deal with how I was feeling, so that's, that's really why I drank,
I think. (
Her epilepsy and poor mental health means that Kerry has experienced acute neurological and psychological challenges for most of her life. For example, she had been diagnosed and hospitalized with anorexia when she was a teenager and has been taking antidepressants since she was 18. Kerry believes that the relationship between addiction and mental health is “like a co-dependency.”
Yeah, it's that strange relationship of co-dependency because you can have one without the other, but, you know, once the two get together…
I have suffered poor mental health all my life, you know, I’d say from when I was twelve, thirteen.
Ehm, emotionally I …. You know, I don’t think at the end, I don’t think that I really could register emotions. You know, everything was just, ehm, I don’t even know …
I, I can’t even, I can’t even say that I was sad, I think I was numb. I think I was just completely inured to anything. (
Conclusion to LO Theme 3b
The inability to regulate emotions, is evident in this theme, and is congruent with the first early-onset theme, Emotional immaturity: drinking to change feelings. However, the noun “emotion,” which appeared in various syntactic forms (i.e., emotion, emotional, and emotionally) in eight of the 12 PETs that constituted the early-onset theme, appeared in only three of the 15 PETs in the corresponding late-onset theme, suggesting that difficulties with emotional regulation were more prevalent among the early-onset cohort than the late-onset group. Moreover, verbatim extracts like, “I was feared-up as a kid…” (Michael early-onset), “I had this kind of series of marriages. I mean, I was married at eighteen…” (Jackie, early-onset), suggest that an inability to cope with emotions, when they were young, were more likely to manifest early in the lives of the early-onset cohort than the late-onset group.
Poor Mental Health: A Shared Comorbidity
Comorbid mental health was prevalent among both cohorts, who shared a theme: Co-existing mental health challenges. A recent systematic review concluded that individuals with common mental disorders (CMD), for example, depression, were twice as likely to drink problematically than people without a CMD (Puddephatt et al., 2022). That said, the direction of the relationship between poor mental health and problem drinking is a complex one. Depression and anxiety were prevalent across both groups; eight of the nine participants in each group reported experiencing either depression or anxiety, or both. Formal, clinical diagnoses of depression were almost equal across both groups (four early- and five late-onset). However, only one of the late-onset group had received a clinical diagnosis for anxiety compared to five of the early-onset cohort. Three other mental health disorders were clinically diagnosed across both groups; anorexia, bi-polar disorder and OCD. Additionally, Steffen (late-onset) received a diagnosis of attention deficit hyperactivity disorder (ADHD*) later in life, when he was 62 and in rehabilitation. Similar to the relationship between problem drinking and CMDs, there is a complex relationship between emotional dysregulation, ADHD and substance use disorders (Zulauf et al., 2014). However, because Steffen lived with ADHD all his life, and his drinking only became problematic in his late 50s, whether Steffen's ADHD is associated with his problematic drinking is questionable. Table 2 summarize the mental health disorders reported by the participants.
Discussion
The current paper has focussed on analyzing the retrospective “active drinking voices” of late-onset problem drinkers and those of their early-onset counterparts. By identifying the similarities and differences in psychosocial characteristics and risk factors between early- and late-onset problem drinkers, this article contributes to a better understanding of why some older individuals start drinking problematically later in life. The participants’ retrospective narrative accounts show that regardless of the onset age of problem drinking, the devastating consequences associated with excessive alcohol consumption are similar. For example, a difficulty managing and negotiating emotional challenges permeated the narratives of both cohorts, highlighting the well documented and inextricable link between poor mental health (summarized in Table 2) and problematic drinking (e.g., Bell & Britton, 2014; Jacob et al., 2021). UK government statistics, for instance, show that almost two-thirds (64%) of people receiving treatment for problematic alcohol use, reported comorbid mental health problems; 25% of whom, were not receiving any treatment for their mental health condition (Office for Health Improvement & Disparities, 2021).
Mental Health Disorders* Reported in the Participants’ “Active” Drinking Narratives.
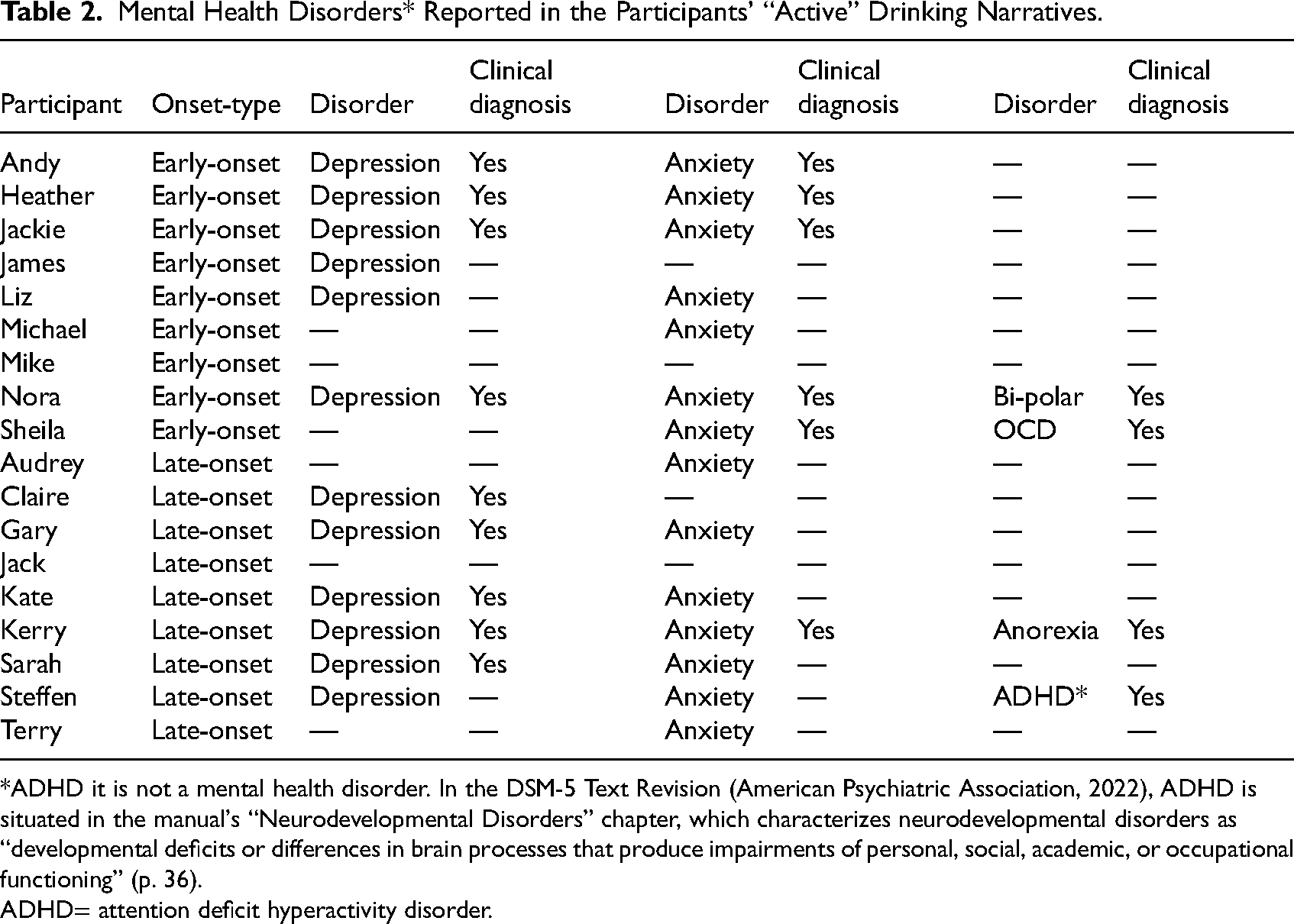
*ADHD it is not a mental health disorder. In the DSM-5 Text Revision (American Psychiatric Association, 2022), ADHD is situated in the manual's “Neurodevelopmental Disorders” chapter, which characterizes neurodevelopmental disorders as “developmental deficits or differences in brain processes that produce impairments of personal, social, academic, or occupational functioning” (p. 36).
ADHD= attention deficit hyperactivity disorder.
The participants’ narratives further suggest that the complex relationship between late-onset problem drinking and poor mental health is similar to that of the general problem drinking population. Moreover, late-onset individuals may be more resilient to mental health problems than early-onset problem drinkers, until they are faced with major challenges in later life. In common with the relationship between problem drinking and poor mental health in a general context, the links between social anxiety disorder and problem drinking are equally complex (e.g., Buckner et al., 2008; Thomas et al., 2008). Typically, social anxiety disorder emerges between early- and mid-adolescence (Child Mind Institute, 2023), and the participants’ narratives, which for many, included receiving clinical diagnoses, suggest that the early-onset cohort experienced social anxiety disorder and began using alcohol as a coping mechanism much earlier in life than the late-onset group. It has been suggested that individuals who experience social anxiety disorder, experience greater challenges in recovery because their fear of social interaction prevents them from engaging in interventions that involve socialization, group membership, and participation (Book et al., 2009).
The major difference between the two onset-types that emerged from their narratives, was the degree of control that each group had over their alcohol consumption. The narratives of the early-onset participants, in the main, showed that any semblance of control they had over their drinking or ability to moderate it was short-lived, quickly followed by dependent drinking. Whereas, for most of the late-onset cohort, loss of control over alcohol and eventual dependency, was a gradual process rather than a rapid event. At this point, it may be worth considering the impact of SES bias and memory on the participants’ data (highlighted earlier). Some late-onset participants, for example, reported being heavy drinkers earlier in life but did not report their drinking as being problematic until between the ages of 50 to 55 yearsold. Their accounts emphasize the individual differences between people, regarding sensitivity and tolerance toward alcohol. They also suggest there may be a subcategory of late-onset drinkers, who drink heavily earlier in life and perceive problem drinking differently than other late-onset problem drinkers. However, the participants who reported drinking heavily earlier in life, had been in recovery for several years at the time they were interviewed and parts of their recall may have been constructions (Davies, 1997). Arguably, however, their recall and perception of their drinking would have been very different had they been in recovery for a year (or less) at the time of their interviews. Of course, it is also possible that their high SES and access to social capital meant that the adverse health consequences of problematic alcohol use, emerged later in life rather than earlier. Additionally, a recent review of late-onset problem drinkers found that family members and friends of late-onset problem drinkers reported an earlier age of onset than that given by the problem drinkers themselves (McInerney et al., 2023).
The narratives from the fourth and final early-onset theme, a reciprocal family dynamic: influence and impact, show that the early-onset cohort, influenced by the family environment they had been nurtured in, were more likely to develop normalized attitudes toward excessive alcohol consumption. That is not to say that late-onset participants were not exposed to and affected by negative alcohol behavior within the family environment in which they were nurtured, something that was highlighted in two of Sarah's (late-onset) PETs, that is, growing up in an alcoholic family and transferring her childhood experiences to her own children. Nonetheless, being nurtured in a family environment, in which alcohol was normalized, was more prevalent among the narratives of the early-onset cohort; confirming that growing up in a family where alcohol is normalized is a risk factor to individuals developing both problematic drinking behaviors (Huurre et al., 2010; Sorocco et al., 2015) and poor mental health (Ellis et al., 1997).
The penultimate late-onset theme highlighted “The impact of major life events on identity and self.” Many of the papers in McInerney and colleague's (2023) review reported that negative issues around identity/self-concept, linked to retirement, was among the most prevalent risk factors associated with late-onset problem drinking. The same challenges to identity, also emerged as a major risk factor for the late-onset participants in the current study. Losing one's professional identity, which gives one's life meaning and purpose, has a negative impact on one's sense of self (Howie et al., 2004; Shinebourne & Smith, 2009; Teuscher, 2010), and can be particularly challenging to professional women (Borrero & Kruger, 2015; Price, 2003). This was apparent among the study's late-onset female participants but is applicable to all late-onset problem drinkers, particularly in the context of experiencing a lack of purpose in life and subsequent meaning.
The participants narratives indicate there is a link between identity and addiction. On the one hand, challenges to identity can lead to addiction; conversely, reconstructing identity informs the positive process of a move away from addiction (Dingle et al., 2015). In other words, the negative retrospective “active drinking voices” investigated in the present study undergo a transformative process toward the participants’ current “voices of recovery.” This finding is relevant for late-onset problem drinkers, evident in the narratives of the study's late-onset cohort, which showed that their identities and sense of self were deeply challenged and affected by major late-life events, particularly to professional or employment status. For many problem drinkers then, the “cognitive shift from drinker to non-drinker” (DePue et al., 2014, p. 38), begins with the reconstruction of identity. However, such a dynamic process of identity transformation must be driven by having a new life purpose. For many late-onset individuals, this process can begin simply by engaging with community activities, or mutual-aid groups; late-onset problem drinkers tend to be more receptive to mutual-aid groups than their early-onset counterparts (Book et al., 2009). Healthcare professionals who treat older problem drinkers, therefore, should encourage and direct the people they are supporting, not only to mutual-aid organizations, but also other group-focussed and community-orientated activities and recovery pathways; volunteering, for example, promotes a salient identity and wellbeing (Thoits, 2012); all of which are pragmatic suggestions and interventions, that give one's life purpose, subsequential meaning and importantly, help in sustaining recovery.
Conclusion
Typically, the narratives of individuals in recovery include two temporally situated voices, the “active drinking voice” and the “voice of recovery.” Both voices express how the individual experiences life and its meanings in each of these temporal states of being. To answer the question posed earlier (How do the psychosocial risk factors associated with AUD/problem drinking differ between early- and late-onset problem drinkers?), the current study's analysis focussed on the participants’ retrospective “active drinking voice.” The analysis showed there were more points of divergence than convergence between the two groups. The two main points of divergence between the two groups were comorbid mental health challenges (experienced by 16 of the study's 18 participants) and difficulties with emotional regulation. However, difficulty in being able to manage emotions was far more prevalent among early-onset participants. Whereas the late-onset group's problem drinking and alcohol dependence was gradual, the early-onset participants experienced a rapid loss of control and dependency on alcohol. Growing up in a family environment, where drinking and attitudes toward alcohol were normalized, was more prevalent among early-onset participants. Of interest, analysis showed that within the late-onset group, there was a subgroup who were heavy drinkers for a considerable time before perceiving their drinking as being a problem. Of course, these accounts are retrospective and as such, the possibility of the data being affected by problems associated with memory recall, should be acknowledged, as too, should the shared SES status of the participants and the possibility of self-selection bias. By far the biggest psychosocial risk factor for increased alcohol consumption among the late-onset group were challenges to identity and self-concept, following retirement and changes to job/employment role and/or status. In accord with Frankl's theory of meaning, these negative events and identity challenges were accompanied by a loss of life purpose and a lack of meaning.
Implications for Practice and Research
The findings summarized above, contribute much-needed knowledge to an “invisible” cohort of older problem drinkers. By confirming what is already known about problem drinking and comorbid mental health in a general context and emphasizing the inextricable relationship between addiction and poor mental health, the study reinforces a familiar call to health and social care professionals to view and treat recovery from both addiction and mental health, from a more holistic perspective rather than as two separate conditions, as they so often are. That many of the study's late-onset participants experienced challenges to identity and self-concept, as well as a lack of life purpose, following retirement or changes to professional status, is a crucial finding from the perspective of recovery. Importantly, it can inform addiction/recovery practitioners and healthcare professionals that the most effective interventions and recovery pathways for late-onset problem drinkers (indeed all problem drinkers) are those which recognize that finding MPL, is an essential component of effectively treating the feelings of meaninglessness and purposelessness, resulting from problematic drinking (i.e., Frankl's existential vacuum concept).
Recovery capital (RC; Cloud and Granfield, 2001) and CHIME (Leamy et al., 2011) are two contemporary models of recovery that are appropriate in this respect. CHIME, for instance, is a conceptual framework with five constituent parts, including identity and meaning in life, while Cloud and Granfield's RC model is comprised of eight domains, one of which, importantly, is (re)discovering MPL. Moreover, the challenges to identity and self-concept that late-onset problem drinkers experience pre- and post-retirement, along with the role that finding or (re)discovering MPL plays, may have implications for many older “social drinkers,” and also the general population of older individuals, as they too, approach and enter retirement. Therefore, further investigations are needed in the context of the dynamic relationship between identity, retirement, and MPL. Finally, that there were individuals within the late-onset cohort who had been heavy drinkers for many years before they perceived their drinking as being problematic, highlights two problems. Firstly, the issue of memory recall associated with self-reports in addiction studies and secondly (which may well be related to the first problem), the difficulty in defining a precise age range for late-onset problem drinking.
Footnotes
Originality Statement
We, Kevin McInerney, David Best and Philip Hodgson declare this report to be our own work. Wherever we have referred to the work of others, we have accurately credited their work using the American Psychological Association (APA) referencing system. The submitted work follows Leeds Trinity University advice on good academic conduct and practice.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval Statement
This study was approved by The College of Business, Law and Social Sciences Research Ethics Committee, at the University of Derby (application ID: ETH2122-2604) on March 14, 2022. Additionally, because data was collected from the National Health Service (NHS), additional ethical approval was granted by The NHS Health Research Committee (HRA) Research Ethics Committee (reference 22/EM/0162s) on August 15, 2022. All participants provided signed informed consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Appendix 1 Interview Schedule
The purpose of my research is to understand why some people, who have used alcohol moderately (or not at all) for most of their life, start drinking problematically later in life (late-onset drinkers). To that end, I am interviewing both late- and early-onset drinkers, with the aim of investigating the similarities and differences between the groups, in the context of their lived experiences of both active problematic drinking and recovery. If you feel uncomfortable about any of the interview questions, you do not have to answer them, and you can stop the interview at any time you wish. You can also go back and revisit questions. At the end of the interview, you will have the opportunity to ask questions and express any further thoughts. Are you happy to begin the interview?
At what age, roughly, did you begin to drink problematically, and why do you think that was? For instance, were you experiencing any difficulties in your life at the time? Had anything changed? People who drank problematically often say they drank because it changed the way they felt. What did alcohol do for you? How did it make you feel? How did your problematic drinking affect you psychologically and emotionally? (This question may need specific prompts, see page 2). When you were drinking heavily, what other problems did you experience? What made you begin to question your drinking? For example, was it a single event, or a culmination of events? What was your experience of stopping drinking and coming into recovery? What difficulties did you experience? Was it hard for you? How did your drinking affect your family relationships? How were you encouraged and supported by family and/or friends to in your efforts to stop drinking? And now that you are in recovery, how supportive are they? What meaning and purpose does your life have now that you are in recovery? How would you describe your spiritual beliefs, and how important are they to you?
Closing remarks
Is there anything else you would like to add before the interview finishes? Thank you for taking part in this study.
Prompts
If subject is tentative about sharing, briefly share own experience of triggers: If talking about deceased spouse/partner/loved one:
What impact did xxxx have on your life?
What do you miss most about xxxxx?
How did you meet?
How long were you together?
If talking about work pre- and post-retirement:
How much do you miss work?
What did work mean to you?
How important were your relationships with your colleagues?
How has retirement and not going to work affected your identity?
How has not going to work affected financial security?
If talking about pain:
How long have you experienced chronic pain and what are your coping mechanisms?
General prompts to encourage the interviewee to respond in greater detail and depth:
Prompt: Can you expand on that a bit please? Prompt: How important is_______ in your life then? Prompt: What do you mean by that? Prompt: How important is that to you? Prompt: Can you elaborate on that? Prompt: In what way/s have you changed? Prompt: How does that make you feel? Prompt: In what ways was/is it different?
Prompts for question 4:
For example, did your life have meaning and a purpose to it? Was boredom and apathy a trigger to drink more?