
Abstract
Older adults with long-term drug use have long been overlooked in both drug research and aging research. More knowledge is needed about their experiences and needs. Drug use is often seen as a youth phenomenon and as something that with time leads to destructiveness and compulsion. A more nuanced picture of who uses drugs and what the use may look like over time is necessary. There is limited insight into what it means to age with drug use, based on individuals’ own stories and experiences. We conducted 27 semistructured interviews in Sweden with individuals aged 55 or older who reported current and long-term drug use. In this article, we demonstrate how the relationship with drugs evolves over time and how the interviewees contemplate stopping or continuing their use. Three themes were identified: (1) Aging out of drug use: Thoughts on drug cessation. Some expressed a desire to end their drug use. The reasons behind this varied, but there was a clear pattern related to older age. (2) Aging with drug use: Thoughts on continued use. Some had a desire to continue using drugs and expressed concern about how everyday life would be without them. (3) Age adapted drug use: A change in drug use. Several participants stated that their drug consumption had changed over time and with age. Drugs no longer dominated their lives as before but still served essential functions. The themes should not be seen as rigid categories, but as fluid narratives. Understanding this variation provides a deeper insight into people's often complex relationship with drugs.
Introduction
Most individuals who begin using drugs do so during their teens, and drug use is most prevalent among people under the age of 30 (Heyman, 2013; Sundin et al., 2018; Winick, 1962). Many of those who develop problematic drug use eventually stop their use, often through what is perceived as natural recovery and personal maturation processes, commonly referred to as “maturing out” (DiClemente, 2018; Jochman & Fromme, 2010; Prins, 2008; Winick, 1962). There is thus an assumption that with age, individuals acquire a certain level of maturity and possess a natural ability and motivation to discontinue drug use. This perspective has led to drug use being predominantly viewed as a youth phenomenon. Therefore, research on addiction and drugs centers primarily around younger populations (Beynon, 2009). Research in a Nordic setting has shown that treatment efforts for individuals with drug-related issues also tend to focus on young people (Selseng, 2015).
The focus of this article is on individuals aged 55 or older who have used drugs for a large part of their lives. Contrary to the notion that drug use typically diminishes with age or personal maturity, those in this group defy that expectation. They are therefore often given a “chronic disease” label due to their continued and long-term drug use (Heyman, 2013; Järvinen, 2014). Older adults run a risk of being deprioritized within the treatment system with the argument that they are not treatable—or that treatment appears pointless if the drug use has been ongoing for most of their lives—or that they are not expected to achieve treatment goals (Järvinen, 2014; Selseng, 2015). Consequently, older adults who use drugs often have low expectations of healthcare (Beynon, 2009) and that experiences of stigma and ageism are common (Ayres et al., 2012; Johnston et al., 2017).
Limited attention has been given to research on older adults who use drugs. However, the existing evidence strongly suggests that they are vulnerable in certain respects. Physical and mental comorbidity is high within the group, and age-related issues often manifest earlier than in the general population (Bachi et al., 2017; Han, 2018; INCB, 2020). Social isolation, poor finances, and housing problems are common (Atkinson, 2016; Johnston et al., 2017). Their social networks are often limited to other individuals who use drugs due to social exclusion in other contexts (Johnston et al., 2017; Roe et al., 2010). Experiences of grief and loneliness occur earlier than for others, as friends die prematurely from overdoses or drug-related health issues (Beynon, 2009; Roe et al., 2010). In conclusion, older adults with drug-related issues represent a growing population with intricate support needs, emphasizing the importance of understanding their living conditions (Beynon, 2009; EMCDDA, 2023; Han, 2018; Johnston et al., 2017).
The aim of this article is to investigate how older adults describe their drug use and how they reason about the meaning of drugs in their lives over time, as well as whether to stop or continue using drugs. Most researchers today agree that drug problems are multifactorial, involving biological, psychological, and social aspects (Assmusen Frank et al., 2013; Kalant, 2014; Keane, 2016). However, there is a dominant biomedical explanatory model in which drug addiction is often characterized by loss of control and a compulsive relationship with the drug (Volkow & Li, 2004; Volkow et al., 2016). This portrayal is further reinforced by an addiction narrative, which includes biographical accounts of extensive drug use and eventual decline, described as “hitting rock bottom.” These stories often conclude with individuals experiencing a personal insight and recognition of having a “spoiled identity,” leading them to stop using drugs (McIntosch & McKeganey, 2001). The relatively context-free biomedical explanatory model (Kalant, 2014; Reinarman & Granfield, 2014) and the prevailing narrative of loss of control and escalating problems can unintentionally create an image of people with extensive drug use lacking agency and the ability to make rational choices (Keane, 2016; Pienaar & Dilkes-Frayne, 2017).
In relation to the dominant narrative about drug use as a youth phenomenon and as something destructive or compulsive (Pienaar & Dilkes-Frayne, 2017), other voices need to be heard and made visible. What is referred to as drug addiction or abuse often comes with generalized notions of what it entails. This is particularly evident in Sweden, where repressive policies means that people who use drugs risk harsh punishments, and where all drug use has been pointed out as reprehensible behavior and a serious threat to society. The resulting strong stigma often leads to societal exclusion, affecting individuals’ lives and well-being (Johnson et al. 2023). A more nuanced picture of who uses drugs and what the use may look like over time is needed. Blomqvist (2002, p. 91, author's translation) describes the complexity of drug use: “…what we commonly summarize as drug abuse can have different meanings, manifest in various ways, and follow diverse courses over time, for different individuals and under varying external conditions.” To include this variation, we have chosen not to describe drug use only as problematic. In this way, more room is left for an open approach in relation to drugs, their use, and those who use them. Our aim is not to minimize the negative consequences many of our interviewees experienced because of their drug use, but rather to show varied stories.
Theoretical Framework
The study's theoretical foundations lie in the lifestyle and life course perspectives. From the lifestyle perspective, individuals are seen as active subjects who act consciously to shape their lives through interactions with others. Their choices are influenced by how they perceive their surroundings (Svensson, 2007). Drugs are considered a meaningful part of people's lives, and for those with extensive and long-term drug use, drug consumption often becomes a “central activity” (Fingarette, 1988). The process by which drug use becomes prominent in an individual's life can be described as a “drug career.” This career trajectory involves transitioning to a more extensive drug use or gradually attaining illegitimate social roles (Becker, 1953). The life course perspective emphasizes how relationships and interactions are shaped by past experiences and future expectations (Hagestad, 1990; Walther et al., 2022). Different age categories come with ascribed expectations related to age-appropriate behavior. The life course is expressed in relation to a “social clock,” where norms guide us in timing various life events—such as starting a family or retiring. These events can occur either “on-time” or “off-time” (Neugarten, 1996, 1981). For individuals with extensive and long-term drug use, their life course may deviate significantly from the expected social timetables (Hser et al., 2007b). Not adhering to the anticipated life course can lead to exclusion, as it diverges from the established social order (Walther et al., 2022).
Theoretical Concepts in Research on Drug Use Among Older Adults
In their literature review, Zolopa et al. (2022) emphasize that previous research primarily focuses on group description, their health status, and access to care. The definition of “older” within in this group varies significantly, ranging from 35 years and up. Moreover, there are a lack of common theories and definitions related to long-term drug use with aging. Notably, some studies do address drug use in conjunction with aging, but most of these studies have been conducted within an American context, with a primary focus on opioid use. This study includes a broader group that, in addition to heroin use, also addresses the illegal use of amphetamines, benzodiazepines, and cannabis. Our ambition is to contribute to the existing literature with this qualitative and more comprehensive perspective on drug use.
Several studies explore aging in relation to drug use trajectories, emphasizing a life course perspective (Boeri et al., 2006, 2008, 2011; Grella & Lovinger, 2011; Hser et al., 2007a, 2007b; Levy & Anderson, 2005). Longitudinal research by Hser et al. (2007a) identifies three distinct heroin using groups: “stably high-level heroin users” (59%), “late decelerated users,” and “early quitters.” The first group faced the highest prevalence of legal and mental health challenges, with nearly 40% mortality during the study. Levy and Anderson (2005) explore the concept of “drug career” among older adults, highlighting evolving patterns of drug use over time. Aging can, for instance, lead to health-related challenges, resulting in a reduced ability to access drugs or money. Moreover, Boeri et al. (2006) propose a typology of the “drug career.” “Controlled users,” “marginal users,” “hustlers,” and “junkies” illustrating varying levels of control and social roles in drug use over time.
In her study, Wyse (2018) introduces the term “sober aged reflection” after interviewing men aged 49 and older who had recently been released from prison. This concept captures their life evaluation following enforced drug cessation during incarceration, resulting in behavioral changes. These men also became more aware of their mortality, motivating them to maintain a drug-free lifestyle and undergo a shift in identity away from drug use. A form of introspection, life evaluation, and identity change in relation to a recovery process is mentioned in several other studies (Best et al., 2016; Blomqvist, 1996, 2002; McIntosch & McKeganey, 2001; Prins, 2008; Robertson et al., 2021), as well as observed in older people who continue to use drugs (Levy & Anderson, 2005).
In the context of age and drug use, “maturing in” contrasts with the more familiar concept of “maturing out.” The latter term, first coined by Winick (1962), describes how individuals who used drugs from a young age tend to stop as they get older, typically in their 30s. For them, quitting drug use is part of an age-related maturation process rather than a treatment intervention. Researchers Boeri et al. (2008) introduced the terms “maturing in” and “aging into” for individuals aged 35 or older. In their study, they compared two groups: those who started using heroin in their teens (early-onset) and those who began in their 30s (late-onset). The “maturing in” group learned to navigate both the “drug world” and mainstream society with age, gaining better control over their drug use. However, they lacked information about safer injecting practices during their early drug use. In contrast, the “aging into” group had early access to harm reduction efforts and knowledge about risks associated with injecting. Consequently, they were better equipped to maintain their health. Cepeda et al. (2016) also delve further into the concept of “maturing out” and use the term “maturing in” in relation to older Mexican American men using heroin. Their findings show that instead of drug cessation, problems and challenges that came with heroin use were addressed through continued use.
Starting from the concepts of “maturing in” and “maturing out,” we have chosen to describe older adults’ relationship with drugs using the terms aging with, aging out, and age adapted. The term “maturing” might imply a simplistic division between immaturity and maturity, where the latter carries normative connotations of improvement and aspiration—something that does not align with our purpose. We do acknowledge that the concept of “aging” also comes with normative associations tied to chronological age. However, aging is a universal experience that transcends age boundaries (Baars, 2009). Therefore, our primary focus is not solely on chronological age but rather on lived experiences and age as a social phenomenon. Instead, the interviewees’ extensive drug experiences underscore an age- and drug-related process.
Method
To explore the implications of aging with drug use, we conducted semistructured interviews with a strategically stratified sample (Robinson, 2014) of older adults with long-term drug use. Between 2022 and 2023, the first author conducted 27 interviews with people aged 55 or older with current and long-term drug use. Typically, research on older people assumes an age threshold of 65 years or older. However, in this study, we deliberately set a lower age limit. Age-related conditions often emerge earlier and are more pronounced among individuals with long-term drug use (Bachi et al., 2017; Han, 2018; INCB, 2020). In accordance with Alvesson (2011, p. 11), we view the interview process as a “complex social event,” where the content is influenced by the expectations, interests, and motivations of both the researcher and the interviewee. Knowledge production, therefore, results from a collaborative effort (Alvesson, 2011; Holstein & Gubrium, 2016).
During the interviews, we utilized a semistructured interview guide designed around three main themes: (1) Everyday life, living conditions, and social relations, (2) Drug use, risks, and risk management, (3) Health, care needs, and contacts with authorities. Throughout the interviews, focus was maintained on the meanings of aging and changes over time. This approach allowed flexibility, giving interviewees the space to discuss what they deemed important. At the same time, the interview guide provided an overall structure that enhanced the comparability of the collected material. As a token of appreciation for their time, interview participants received a SEK 200 gift card for a grocery store.
Recruitment and Participant Characteristics
The recruitment occurred in Scania County, Sweden, at various support services with which the target group had contact. These services included low-threshold housing, syringe exchange programs, and an OAT (Opioid Agonist Treatment) reception. To be eligible for the study, individuals had to meet the following criteria: (1) 55 years of age or older, (2) having current use of illegal drugs, and (3) a long-term experience with drug use.
A total of 27 people were interviewed—20 men and 7 women. The interview durations ranged from approximately 26 min to 145 min, with an average of 69 min. Four individuals were interviewed on two occasions, primarily due to practical considerations, such as other scheduled appointments. The interviews were conducted on the premises of the services, except for one interview that took place in a café (Table 1).
Overview of interview participants.
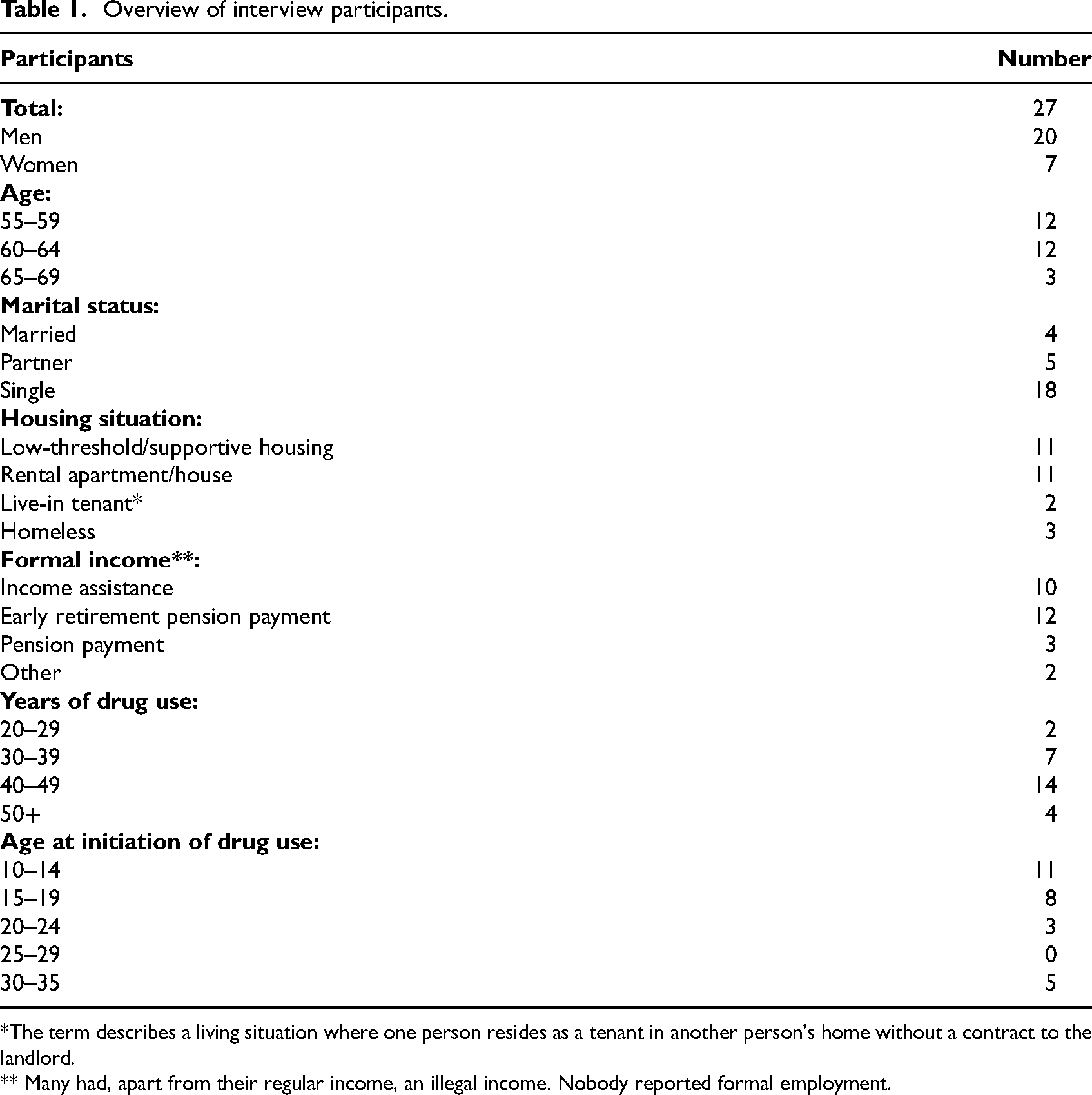
*The term describes a living situation where one person resides as a tenant in another person's home without a contract to the landlord.
** Many had, apart from their regular income, an illegal income. Nobody reported formal employment.
Among the men, a clear majority used amphetamine as their main drug (13 people). Another large group consisted of those who used heroin (six people). Other drugs that were also frequently used by the men included cannabis, alcohol, and benzodiazepines. Most women (five people) stated that benzodiazepines were their main drug. Other commonly used drugs among the women were heroin, cannabis, and amphetamine.
During the interview, 23 people reported regular drug use, ranging from daily use (most common) to a few times a week or month. The other four participants mentioned that they had stopped using drugs for a few months; one person reported stopping for up to 2 years. Fourteen participants had longer previous periods of cessation, spanning at least one year, while the remaining 13 participants had either never had periods of cessation or had had short periods.
The majority of the group injected regularly (14 people), while four people had never injected. The other nine had previously injected regularly, but three of them belonged to the group who did not use drugs at the time of the interview. These individuals indicated that they had injected while active. Five people had stopped injecting, mainly because they had ceased using heroin or amphetamine and at the time of the interview were mainly using benzodiazepines or cannabis in other ways.
There are several shortcomings in this study that should be considered when interpreting the findings. Firstly, the individuals who participated in the study were in some regard homogeneous. Most were men who used amphetamine, and all but two participants were born in Sweden. Since women were underrepresented in the group, the findings primary reflects men's experiences. A wider and more diverse group could have provided a more nuanced understanding of older adults’ drug use and living conditions. Furthermore, 11 individuals were undergoing OAT, and one was prescribed medication for attention deficit hyperactivity disorder (ADHD). These medical treatments may have influenced the results. It should however be noted that all individuals undergoing medical treatments continued to use nonprescribed drugs.
Analysis
The analysis was carried out based on Braun and Clarke's (2022) practical guide to thematic analysis. The analysis process aimed to produce themes rooted in a common understanding of a concept that reflected the interview material. In this context, the themes should be seen as analytical products and patterns built on codes. Our goal was to illuminate experiences expressed by the interviewees.
Initially, the interviews were transcribed verbatim to gain an overall understanding of the material. Following the principles of thematic analysis, analytical points and insights were continuously recorded in parallel with ongoing data collection (Braun & Clarke, 2022; Carey, 2017). The material was then coded using the support of the computer program NVivo. Subsequently, the transcription texts were revisited, and text fragments were organized into specific and analytically meaningful codes. During the analysis process, it became evident that many interviewees discussed their relationship with drugs in terms of continued use or cessation. This observation led to the idea of exploring these perspectives. In this phase, the material was reexamined, and theoretical concepts were tested. Earlier codes underwent transformation, being restructured and renamed. Finally, themes emerged and were clarified, aligning them with theoretical significance (Gibson & Brown, 2009). In the final stage, selective quotes were chosen to contextualize and exemplify the themes.
Ethics
The research project was approved by the Ethics Review Authority (diary number: 2022-00907-01). The participants were provided with verbal and written information before the interview and subsequently provided written consent. To safeguard the anonymity of the interviewees, we assigned them pseudonyms, and any other names or locations that could potentially reveal their identity were replaced.
Findings
In the interviews, different themes about drug use emerged, where the drugs played different roles and carried different meanings. Thoughts about past, ongoing, and future use varied among the interviewees. In the material, we could distinguish three main themes: (1) Aging out of drug use: Thoughts on drug cessation. Some expressed a will to end their drug use. The reasons behind this varied, but there was a clear pattern related to older age. (2) Aging with drug use: Thoughts on continued use. Some had a will to continue using drugs and expressed concern about how everyday life would be experienced without them. (3) Age adapted drug use: A change in use. Several participants expressed that their drug use had evolved over time and with age. Drugs were no longer a central activity in their lives but still served essential functions.
There was certain ambivalence among some interviewees when they expressed their thoughts. It is valuable to note that one and the same interview could contain all three of these themes. Instead of viewing the themes as rigid categories with clear boundaries, we consider them as fluid narratives.
Aging Out of Drug Use: Thoughts on Drug Cessation
In this theme, reasoning and thoughts related to the desire to stop using drugs became apparent. The reasons behind the interviewees’ common will to quit varied, but there was a clear pattern concerning older age. Older age could serve as motivation to quit, and some just expressed that they were “tired of it.” Others addressed the negative consequences associated with drug use, such as poor health or imprisonment. Often, they expressed their process in terms of age-related maturity and insight, valuing things differently now compared with before. This theme represents a form of aging out. The interviewees cited in this section had varying degrees of current drug use. Some had recently stopped, while others still engaged in daily use. The thoughts about cessation are interpreted, and in some cases, thoughts about the future may also come into play. The following quote reflects the reasoning of many interviewees, specifically regarding age in relation to drug use. Aging with drugs. I feel, I feel like this, that no, I must quit using drugs. I don’t want to become an old hag who's still on drugs at 80 years old. I don’t want to be that. Instead, I’d rather be that 70-year-old lady who managed to break free from long-term addiction and made something good out of it. That's how I feel. (Anita, age 61, had a history of drug use spanning over 40 years. By the time of the interview, she had ceased using heroin and was using benzodiazepines. She was undergoing OAT.)
For Anita, who was using illegal benzodiazepines daily, continued use would be perceived as a failure. Instead, she envisioned stopping and becoming someone who succeeded despite her older age. Her perspective on age is intertwined with societal expectations around drug use and the criminal lifestyle often associated with youth.
Britta, who stopped using amphetamine a few months ago, expressed how her view of the drug and the lifestyle that came with a constant hunt for drugs had changed. The quote highlights how her former identity linked to drug use played a smaller role today, allowing more space for other parts of life. Because when you started with amphetamine, when I started, it was good stuff [drugs], it was fun. You know, back then we were out and… But now, I can’t just run around today. […] I didn’t find it fun anymore or take anything at all [amphetamine]. Instead, I’d rather lie down, watch TV, and relax, cuddle with the dogs. (Britta, age 63, had a history of drug use spanning over 25 years. She mainly used amphetamine.)
Lars, like Britta, expressed that the identity associated with drug use had been set aside to make room for other social identities and roles. He had stopped using amphetamine for about a year but had relapsed shortly before the time of the interview. He wanted to distance himself from the social relationships that often came with using drugs. Socializing and the previous shared drug use no longer appealed to him. However, this change could also bring about a sense of isolation. You become quite isolated. Many of my friends, they’re the same age. Many have passed away. What should one do? I don’t want to socialize with the drug users anymore. It gives me nothing. They only talk about drugs all the time. […] You can’t socialize in the usual way. Not really. […] No, I mean, I don’t want my life to revolve around [using amphetamine]. I know others who are older than me and still keep at it. Like… running all over the city searching for drugs. Come on, there are other things that matter more, in my opinion. Yes. What are those other things that also feel important to you? Taking care of my nieces and nephews. Taking care of myself. Nurturing friendships. Being content with the little things. (Lars, age 59, had a history of drug use spanning over 40 years. He mainly used amphetamine.)
Lars was in the process of reevaluating what was important in life. Important relationships and taking care of oneself were something he considered important. The quote also reveals his view of people who were older than him and were still “running all over the city.” It reflects a notion that with age, one should stop using drugs, or at least alter certain behaviors.
Mehdi used heroin and benzodiazepines approximately once a month and talked about how, with older age, his relationship with drugs and the criminal lifestyle he had previously experienced had changed. He shared that when he was young, he could be arrested for a crime only to commit another as soon as he was released. Today, his perspective was different. “But now, I go in and buy a valve for a bicycle, I think it's bloody ridiculous, but now I have a goal to pay for it. Yes, I think now, I’ve grown a bit in my thoughts, I believe.” Furthermore, he explained how he had transitioned from living in the moment to being more mindful of time and planning. You’re just in the situation, living in the moment, you know. But now, I think, “Oh no, I’m 56, I don’t have time; I have to think about my child and the future and all that.” And my situation, how to improve it—I feel a bit stressed, I’m running late, I have to, well, this time, everything I missed before, I have to tackle it now, you know. All the problems, all those things, yes, debts and feelings of guilt to manage. So unfortunately. And now you think, like, “No, I don’t have time,” you know. (Mehdi, age 56, had a history of drug use spanning over 40 years. He mainly used heroin and benzodiazepines. He was undergoing OAT.)
Mehdi expressed how he felt delayed, as if age forced him to deal with both the past and the future. Previously, there was nothing but the present, and now that he had become older, he felt that time was short and experienced a certain anxiety about having time to deal with the new reality. His age and newfound outlook reminded him of being “off-time” when it came to spending time with his child and planning for the future.
This theme highlights how age and long experience with drugs can give a different perspective. It is about reassessing what is important in life and how you want to shape your future. In their youth, some experienced a sense of immortality, but with the passage of time, this feeling was gradually transformed into an awareness of mortality. At the same time, there is a strong opinion that older age and drugs do not go hand in hand. Many referred to their own age or that of others to point out that there is an age limit to a drug-centered lifestyle. These thoughts can be interpreted as part of the general narrative of drug use as a youth phenomenon. For many, the combination of drugs and older age is not compatible. Sofie, aged 55, expressed herself like this: “You can’t do drugs when you’re 50 years old, oh my God.” In the concluding theme below, however, it becomes clear that there is another experience of drugs where their function and positive properties continue to be important with aging.
Aging with Drug Use: Thoughts on Continued Use
Most interviewees who did not have a clear desire to stop using drugs stated that they did not experience any major consequences from their use. Instead, some expressed a concern about how everyday life would be experienced without the drug. The theme above exemplified how thoughts of quitting were associated with notions of age. This theme also shows this connection, but now in relation to a continued use and more tangible health awareness. Maintaining one's health or repressing age-related health problems were felt by some to require continued use. Many expressed how the drug had become part of self-medication, and stopping a drug use that made you function and feel good was not perceived as an attractive alternative. This theme reflects what we call aging with drug use. Now I have these numbness sensations; I have no feeling in my legs, from the knees down. And now I feel the same in my hands, and it's starting to spread throughout my body. It's like I’m aging too quickly. It's not just numbness; it also hurts. Heroin is the only thing that allows me to relax. (Ervin, age 66, had a history of drug use spanning over 40 years. He mainly used heroin and benzodiazepines. He was undergoing OAT.) I can only speak well of amphetamine. I probably wouldn’t feel as good as I do today if I hadn’t had access to amphetamine. Honestly, if I had lived differently, I might have drunk myself into oblivion. But now I’m afraid to quit [amphetamine] because it also keeps illnesses at bay. I haven’t been sick in 35 years; I haven’t been bedridden due to illness in 35 years. It's the amphetamine—it keeps illnesses away. (Anton, age 62, had a history of drug use spanning over 50 years. He mainly used amphetamine and alcohol.)
Ervin reasoned how the drug helped alleviate the ailments that come with aging and the feeling of aging too quickly. In his experience, only heroin could assist him in this regard. Anton expressed a conviction that he wouldn’t have felt as well without amphetamine; he visualized a decline in his health if he were to quit. Simultaneously, he expressed concern that in the absence of amphetamine, he might turn to alcohol more frequently, which he perceived as a worse alternative for his health and well-being. Amphetamine thus became an assurance against using other, “worse,” drugs. There is a clear link between the drug use and the perception of health. According to Anton, amphetamine even had a rejuvenating effect: “…it keeps you a bit younger or, if you will, keeps the body going.” Several others also stated that the body stayed active and energized with amphetamine and not using often meant struggling to get out of bed in the morning. Olle, aged 66, put it this way: “It's [amphetamine] what gives you the strength to get up,” and Olof, aged 61, said, “I can’t lift my head off the pillow if I don’t have it [amphetamine].”
Bengt also expressed how amphetamine helped him cope with everyday life. If I run out of amphetamine, well, I get damn breathing [trouble], *takes a deep breath*; it's even like when I’m tying my shoelaces. Now, as I’m [under the influence], I can run up and down the stairs, but if I go without [amphetamine], maybe I’ll have to sit down halfway or something. (Bengt, age 60, had a history of drug use spanning for over 40 years. He mainly used amphetamine, cannabis, and alcohol.)
For Bengt, the physical effects of amphetamine were important. With amphetamine, he could move freely, whereas the experience would be different without it. The drug can thus be interpreted as having the function of mitigating potential age-related physical impairments. The absence of the drug would instead heighten awareness of aging and health. The negative consequences often associated with aging shifted with the help of the drug, which can be seen to have a rejuvenating effect.
For others, the drug had more psychologically positive effects. Anita, aged 61, was undergoing OAT and used illegal benzodiazepines in addition to treatment: “The only time you feel good is when you have a ‘side addiction.’ 1 That's when you feel good.” Kurt, aged 69, described how heroin worked for him: “I mean, it's like a valve for release in the body and mind.” At the same time, he expressed how his daily life would become duller and more challenging without drug use.
For some, continued use was not primarily about a reluctance or lack of motivation to quit, but rather about simply not seeing it as a realistic possibility. For Oskar, there were no other options but to continue with his amphetamine use and the lifestyle he had maintained for most of his life. No, do you have any such desires to quit? I can’t do anything else. I mean, I have no education, I’ve never been to school. What am I supposed to do? Sit at the central station and just stare? I can only be a criminal; it's the only thing I’ve known my whole life. So … no, I’ll probably continue with this until it's over. (Oskar, age 58, had a history of drug use spanning for over 40 years. He mainly used amphetamine and cannabis.)
Given that many of the interviewees had used drugs for more than half of their lives, it is understandable that their scope for exploring alternative paths was perceived as limited. For some, most of their knowledge, skills, networks, status, and everyday life were connected to a lifestyle centered around drugs, and they saw little opportunity to leave this behind and change their way of life. Simultaneously, there needs to be an acknowledgment that the lifestyle and drug use also yield positive experiences. Social relationships, engagement, and excitement still thrive within the “drug world,” aspects that they might miss out on if they were to quit. Olof, age 61, expressed it like this: “I am an amphetamine user and I will always be one, and I enjoy it.” Their lifestyle and relationship with the drug had become a form of security—a routine of everyday life that they had come to cherish.
Pervasive throughout the interviews was the expression of a somewhat controlled relationship with drugs. It was something they believed they could change, quit, or continue, although not entirely without difficulties. This control had, in some cases, developed over time due to extended drug experience, aging or altered perspectives, or perhaps it had always been present. This may indicate why these individuals had survived a life with high health risks. One person stood out in comparison to many others. Viktor, aged 56, shared that he “took everything” but preferred amphetamine, cannabis, and alcohol. Even though the drugs available to him were not his preference, he took them. He had experienced several overdoses in older age, revealing a significantly more destructive relationship with drugs than many others. He exhibited a certain resignation regarding his situation. He had no plans to quit but rather intended to “keep going until I die.” It is essential to highlight that many face significant consequences from drug use, and in numerous cases, it leads to fatalities. On the other hand, Viktor's relationship with drugs, as some of the other interviewees’ stories of a continued drug use, could also be interpreted as an act of resistance against societal norms and expectations of abstinence as the only reasonable goal.
The theme aims to highlight the perspectives of individuals who express a desire or need to continue using drugs for as long as possible. However, in some narratives, it becomes evident that a life without drugs is not enticing enough for them to quit, even if they don’t fully enjoy their current life situation. Older adults with long-term drug use who plan to continue their usage have aged alongside drug use and see few reasons to stop. The drug has acquired a significant role in their lives and continues to hold central importance. The opportunity for changing their lives may be interpreted as having diminished, parallel to the fact that the allure of quitting drugs was not substantial enough. The theme also highlights a form of resistance against living as an “average Joe” and an active choice to pursue an alternative lifestyle.
Aged Adapted Drug Use: A Change in Use
Several of the interviewees reported changes in their drug consumption. Some expressed that their drug consumption was reduced, that their former main drug was replaced or that they did not inject as frequently. A shift in priorities could also be identified; drugs no longer dominated their lives as before but still served essential functions. The reasoning behind these changes in drug use appear to be intertwined with aging and lived experience, leading us to use the term age adapted drug use. The following quote resonates with the experiences of many others. Today, when I take [amphetamine], well, I feel calmer today. I haven’t… If I can’t get hold of it, it's not as important anymore. The obsession has probably disappeared. It's the obsession, you get caught up in an obsession, and right then, the drug is the most important thing you have. And then you turn everything upside down if you can’t find it; I did that when I was younger. Nowadays, if I make a call and can’t get hold of it, I set it aside. It's not that crucial to me anymore. (Lilja, age 60, had a history of drug use spanning for over 30 years. She mainly used amphetamine.)
Lilja expressed that her relationship with her primary drug changed over time. The same allure or motivation to use drugs was no longer present. Lilja described her previous connection with the drug as an obsession, whereas today, it held less importance and could be set aside. For Allan, age 62, who mainly used amphetamine, the euphoria had transformed into a familiar routine;“…like having a cup of coffee in the morning.” As a result of the damage to his veins, he had also altered his method of drug consumption: “I try three or four times [to inject], then I don’t care. Then I drink it or take it in some other way.” Kurt, age 69, who mainly used heroin and alcohol, on the other hand, conveyed how aging had distanced him from the world of drugs, and the actual feeling associated with the drug had diminished in impact. “I’m not as inclined to drug myself anymore; you get older and older, and you distance yourself more from it.”
Continuing Kurt's account, it became evident that his drug consumption and lifestyle had changed in synchronization with a deteriorating physical health and ability. This had led to a heightened awareness of the risks associated with drug use, and he adjusted his consumption accordingly. Kurt used heroin when he felt the urge, which happened once or a couple of times a week. He consumed alcohol daily but no longer excessively, and he avoided mixing alcohol and heroin—“That's dangerous.” When taking heroin, he did so in the company of a friend, ensuring they kept an eye on each other to prevent anyone from taking “too much.” Back then, you know, you used to sell drugs to finance your own addiction. But now, I don’t use as much damn stuff; I’ve gotten older. No, I had a heart attack and all that crap about a year ago. […] Then I messed up my hip and all that—the joint, the hip there—it got crushed, you know. So it's hard to go out, spin around, steal, and chase money when you’re not well, right. So no, I have to… I take it [heroin] occasionally. Not the same amount and not as often? No, I’m damn careful with it, you know. I’ve overdosed so many times and all that crap. I don’t dare. No. (Kurt, age 69, had a history of drug use spanning for over 50 years. He mainly used heroin and alcohol. He was undergoing OAT.)
Ervin also talked about how his heroin use had decreased with age. Although he still used it occasionally, he found himself turning more often to illegal benzodiazepines to aid his sleep. Like Kurt, Ervin became increasingly aware of the toll his heroin use had taken on his health. For Ervin, this physical damage and these health risks were primarily associated with injecting the drug. He expressed a desire to quit injecting, but he also recognized that it was a challenge to do so since the specific effect he sought could only be achieved through injection.
You know, it's enough. I’ve damaged my body so much, both intravenously and in my muscles. I don’t have many muscles or places left to inject. If you’ve been a needle addict, it's incredibly hard to quit. Because you feel the high all at once. And that experience can only be achieved by taking a hit. […] Honestly, that's the one thing I feel I’ve done wrong—damaging my body like this. I’m contemplating whether I should really throw away all the syringes and everything and stop injecting, because that doesn’t work either. All I get is infections and such. (Ervin, age 66, had a history of drug use spanning for over 40 years. He mainly used heroin and benzodiazepines. He was undergoing OAT.)
It should be noted that both Ervin and Kurt have undergone long-term OAT treatment; this can also be seen as a reason for their reduced heroin intake.
Some changed their former main drug to another, like Said, who stopped using amphetamine 3 months ago but continued with his daily cannabis use. Said was not motivated to stop using cannabis as he experienced no negative consequences. However, he could perceive that society's view of cannabis and its use as punishable had indirect consequences. As an adult, Said was diagnosed with ADHD, and both amphetamine and cannabis had become part of managing this. According to him, cannabis was more of an aid than a drug. I don’t see hash as a drug; I see it as a helping hand. I haven’t harmed anyone by smoking hash, nor have I harmed myself. The only negative consequences I’ve faced are indirect, imposed by others because of my choice. But as for hash itself, I’ve never experienced any negative consequences whatsoever. (Said, age 59, had a history of drug use spanning for over 40 years. He recently ceased using amphetamine and was using cannabis.)
However, Said's relationship with amphetamine was different. He expressed a clear desire to quit because of the social and health-related consequences he felt the amphetamine led to, much in accordance with aging out.
This theme highlights various aspects of what aging with drug use can entail and how the relationship with drugs can change over time and with experience. The interviewees’ accounts revealed that not only had their drug consumption changed but so had their lifestyle. Many testified that the drug used to be a central activity in their lives as their social interactions and everyday lives revolved around drugs, but today, its role had been deprioritized. There is an expression of distance from the drug that can be interpreted as arising with age. Some accounts also speak of health awareness, often expressed in connection with deteriorating physical ability. It wasn’t necessarily the drug itself that was seen in relation to health risks but also the practices that accompany its use, such as injection.
Discussion
In this article, we have explored the significance that older adults attribute to drugs and how this influences their drug consumption. Life entails diverse paths, transitions between various phases, and turning points. The trajectory of one's life is influenced by different life events which are continually interpreted through new experiences (Hagestad, 1990; Walther et al., 2022). In relation to drug use, life course considerations include the timing of an individual's initiation into drug use, the duration of their usage, and the impact drug use has had during different life stages (Boeri et al., 2008; Hser et al., 2007b). The lifestyle influenced by drug use, with its habits, unique values, knowledge, livelihood practices, and social networks (Becker, 1953; Svensson, 2007), significantly shapes the trajectory of the life course (Hendricks & Russell Hatch, 2009). In this context, we put an emphasis on long-term drug use in relation to older age as a new experience, an experience impacting lifestyle choices, drug use trajectories, and transitions. Overall, we want to shed light on the complex relationship between drug use and aging, emphasizing individual experiences and motivations.
Aging and drug use can be seen as intricately intertwined and inseparable, which we have tried to highlight through the concepts, aging out of drug use, aging with drug use and age adapted drug use. The themes and concepts should not be understood as mutually exclusive or fixed. Rather, they together reveal a myriad of different motives for drug use, and the diverse ways in which older individuals relate to their current and long-term drug use. However, aging appears to exert a significant influence on the interviewees’ relationship with drugs. The themes can be understood as different strategies for managing aging and drug use. A common thread in the interviews was a desire to delay negative consequences of aging, maintain good health, and practice less risky drug use. In some cases, aging directly prompted changes in drug use. In summary, the evolving relationship with drugs as people age is influenced by physical changes, lifestyle adjustments, health considerations, and dominant norms around aging and drug use.
The concept of aging out of drug use highlights how age and its associated normative expectations compel a shift in perspective on life. There is an interplay between age, societal norms, and individual behavior. This shift includes, with older age, an increased desire to stop using drugs, a change often referred to as a part of newfound maturity and different perspectives (Blomqvist, 2002, p. 159, “Finding yourself”; Wyse, 2018, “Sober aged reflection”; also see Levy & Anderson, 2005; Prins 2008). This leads to a gradual replacement of the drug as other everyday activities and alternative identities, distinct from those associated with drugs, gain more importance (Best et al., 2016; McIntosch & McKeganey, 2001; Robertson et al., 2021; Svensson, 2007). Numerous interviewees also expressed an exhaustion of the lifestyle, social relationships, and hustle associated with drugs and the illegal economy (Best et al., 2008; McIntosch & McKeganey, 2001).
The “social clock” (Neugarten, 1981, 1996) underscores the idea that certain behaviors are deemed appropriate or inappropriate based on age. The social judgment of drug use not being age-appropriate behavior was manifested in the lives of the interviewees, signaling that they were “off-time.” Active drug use often leads to short-term perspectives and difficulties in long-term planning (Nordstedt, 2023; Svensson, 2007). However, as they aged, awareness of time, seemed to intensify. Some expressed a feeling of “running late” or as if they “didn’t have time.” The immediacy of living in the moment seemed to diminish, replaced by an increased sense of mortality. This shift in perspective had an evident impact on the meaning they ascribed to drugs and their use (Wyse, 2018). Some individuals explicitly set age limits for their drug use, claiming it did not longer align with their current life stage. Aging out underscores how our perception of drug use is influenced by broader social structures, a heightened awareness of time, and health. Consequently, the meaning and function of drugs were questioned and often viewed more negatively. Despite expressing a desire to quit drugs, many individuals continued their drug use, illustrating the challenges of altering one's drug use and lifestyle, even when the intention to do so exists.
The theme of aging with drug use, on the other hand, suggests that some older individuals continue using drugs despite societal norms and health risks (see Hser et al., 2007a “Stably high-level heroin users”). This behavior can be seen as a form of resistance to treatment options and a drug-free life (Dennis & Pienaar, 2023). Many stories reflect a lifestyle in opposition to restrictive Swedish drug policies and narrow notions of drug use as something solely risky and problematic. Rather than emphasizing negative consequences coupled with drug use the concept underscores a concern about how everyday life would be without the drug. The trajectory of drug use unfolds through various transitions (Becker, 1953; Boeri et al., 2006; Levy & Anderson 2005), during which drug-related activities become more central (Fingarette, 1988). Drug use still had a purpose in the interviewee lives and created a well-known everyday routine. Having familiar routines helps maintain a sense of stability. Moreover, routines contribute to our identity—they shape who we are and how we perceive ourselves. By maintaining habits and everyday activities, we create a buffer against the effects of aging and provide a sense of control and familiarity, making the aging process feel more manageable (Alftberg, 2012). The loss of routines reminds us of their importance to our identity and the organization of our everyday lives (Ehn & Löfgren, 2020). The continued use of drugs can be interpreted as a strategy for maintaining a sense of control over an unstoppable aging process, as well as preserving one's sense of self and everyday familiarity, and taking a stand against conventional ways of living. For some, drug use was also connected to pleasure and relaxation, something not usually associated with long-term drug use among older people.
Aging with, and a drug-related lifestyle constituting a “central activity” (Fingarette, 1988) can result in a sense of limitation of choices and alternatives. Additionally, the ability to change one's lifestyle is closely tied to personal and social resources—what Cloud and Granfield (2008) refer to as “recovery capital.” Negative recovery capital tends to be associated with older age and poorer health (LaBarre et al., 2021). Furthermore, aging with emphasizes an assumed connection between ongoing drug use and maintained health. Some individuals associated drug use with positive health effects, even youthful effects. For others, there was an element of alleviation of health problems. In many ways, the relationship with the drug was framed as self-medication. The drug facilitated everyday functioning and contributed to a sense of well-being (Heilig, 2019; Johnson et al., 2023). The drug served as a remedy, easing pain, and seemingly reversing the feeling of aging. Continued drug use can reduce or hide health problems that become noticeable to those trying to quit (Shaw et al., 2022). In many ways, they coped with the challenges and health decline associated with drug use by continuing to use drugs (Cepeda et al., 2016). Consequently, several factors perpetuated their current lifestyle and drug use, leaving them with limited pathways toward a transformed existence as older adults.
As presented in the findings, the concept of age adapted drug use entails a changed relationship with drugs as individual’s age. This change involves a greater distance from drugs as their central role is reduced, and a heightened awareness of health and risk as declining physical ability, coupled with aging, prompts precautions to mitigate negative health effects related to drugs and lifestyle (see Levy & Anderson, 2005). In many ways, age adapted drug use can be seen as a combination of the two previous themes. There is a noticeable newfound detachment from the drug, similar to aging out. Simultaneously, the drug continues to serve a purpose, and the option of discontinuing its use is not expressed as desirable, which is similar to aging with.
The process of age adapted drug use could be interpreted as a turning point in a life course and drug career perspective on drug use (Boeri et al., 2006; Hser et al., 2007b; Levy & Anderson, 2005). This turning point, influencing changes in the trajectory of drug use, should not be seen as abrupt but as an ongoing change over time. The changed drug behaviors of individuals as they age, along with their personal experiences, define what the “drug career” can entail with older age. Often it is a process of a reduced or less risky drug use and lifestyle while continuing to use. It is common for a gradual reduction in drug use to precede a more definitive decision to quit, making it a long-term process (Blomqvist, 1996, 2002). Levy and Anderson (2005) discuss how methods of obtaining drugs and living a drug-related lifestyle tend to shift with age from tactics that require youthful strength to approaches better suited to their older physical condition. In this study, these changes were sometimes necessitated by physical impairments, while in other cases, it was an active choice. Additionally, the lifestyle changes may be attributed to a shift away from central roles within the drug scene as individual’s age leading them to withdraw to the periphery, assuming a more passive role (Anderson & Levy, 2003).
In conclusion, contrary to popular belief, drug use is not solely a youth phenomenon. Older people use drugs for a variety of reasons and their relationship with drugs can change significantly over the life course, even late in life. The result revealed a sense of agency. Many reported or indicated that decisions about altering consumption, whether to quit entirely or continue, were choices mastered and controlled, even if challenging. However, in some cases, there was a perception of limited opportunities for alternative paths and ways of living without drugs (Fingarette, 1988; Svensson, 2007). For many, drugs still held a clear significance in their lives. They served as a means of pleasure and relaxation and a valuable part of their daily routines, and this was despite the fact that the drugs and associated lifestyle posed many risks and challenges for them. The process of aging out, aging with drug use, or age adapted drug use should not be viewed as passive; rather, it is an integral part of a complex chain of events driven by active agency in relation to aging. Stopped, continued, or changed drug use are not trajectories bounded by age (Heyman, 2013), but could be seen as playing an important role behind older adults’ drug-related motives and meaning-making. By understanding the variety of stories, we gain deeper insight into people's often multidimensional relationships with drugs and their everyday lives.
Implications
We believe that the concepts of aging with, aging out, and age adapted drug use can illuminate a process that is closely linked to aging, drug experience, and the life course. Consequently, these concepts can contribute theoretically to this relatively unexplored field of research. We aim to emphasize that aging and drug use can manifest in diverse forms. By embracing various perspectives, we can foster a more inclusive and empathetic understanding of drug use moving beyond ageism, stereotypical beliefs about addiction and misconceptions that older adults are helpless victims of their drug use or set in their ways. This is particularly important in a Swedish context where all drug use (regardless of type, amount, and purpose) has been regarded as abuse, where zero tolerance toward drugs has been the norm and where harm reduction efforts have long been controversial. A broader understanding is essential to better address the needs of this group. By expanding the perspective, a wider variety of more effective and inclusive treatment options can be offered. However, we want to encourage further research and much needed development within the field.
In social work and healthcare with older adults who use drugs, it is important to listen to their future goals. For some, the drugs are essential, and they may not want to stop using them. For this group, it is primarily about reducing risks linked to drug use and improving their social situation. At the same time, we should be open to the fact that older individuals with long-term drug use may be motivated to reduce their drug use or leave it behind altogether.
Footnotes
Acknowledgments
The authors are very grateful to the interviewees who kindly shared their experiences with us.
Data Availability
The data that support the findings of this study are not publicly available due to ethical restrictions. Sharing the data could compromise the anonymity and confidentiality of the participants involved in the research. Therefore, the data cannot be shared.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
The research project was approved by the Ethics Review Authority (diary number: 2022-00907-01). The participants were provided with verbal and written information before the interview and subsequently provided written consent. Consent for publication was not applicable.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from FORTE, The Swedish Research Council for Health, Working Life and Welfare.