
Abstract
Opioid dependence is a chronic health condition with significant public health implications. Opioid dependence treatment (ODT) has evolved considerably over time. In New South Wales, Australia, ODT prescribing has been available since 1970, managed by both state health services and private practitioners, mostly general practitioners (GPs). This study investigated how various health initiatives influenced GP engagement in ODT prescribing in New South Wales. The research employed a mixed-methods approach, combining document review, key informant interviews, and quantitative prescriber data analysis. Findings revealed a substantial increase in GPs prescribing ODT since the 1970s, with GPs providing care for half of the ODT-treated population by 2022. However, only a small percentage of GPs offered ODT, resulting in limited access and unmet treatment needs. The ODT structure remained vulnerable to potential disruptions in prescriber availability. These results highlight the complex interplay between policy initiatives and clinical practice in addressing opioid dependence. The study underscores the need for long-term, diverse strategies to improve ODT access and support GP involvement in providing comprehensive care for individuals with opioid dependence.
Keywords
Background
Opioid dependence is a chronic condition that can cause significant harm (Australian Institute of Health and Welfare, 2018). Long-term opioid dependence treatment (ODT) with controlled access to opioid medications (i.e., methadone and buprenorphine) is highly effective (Degenhardt et al., 2019; Krawczyk et al., 2020; Larochelle et al., 2018; Molero et al., 2018; NSW Health, 2018c; Santo et al., 2021) and access to this treatment has been state-sanctioned in New South Wales (NSW), an Eastern State in Australia, since 1970. Both state health services and private prescribers including General Practitioners (GPs) are permitted to provide this treatment; however, it is likely that there continues to be a substantial unmet need for ODT (McDonough, 2013; Ritter et al., 2011).
Heroin became increasingly available in the late 1960s with long-term use driven by opioid dependence (McArthur, 2001). Opioid dependence prevalence estimates are imprecise; however, in 1978, maybe 20,000 people were opioid-dependent in Australia (Rowe, 2001), and by 2019, this may have been closer to 140,000 (Institute for Health Metrics and Evaluation, 2020). In 1970, in response to the need to treat opioid dependence, ODT was made available as a treatment in Australia, and it is estimated that 10 people commenced ODT at this time. In 1985, this had increased to 1,434 people (Hall et al., 2000), and by 2022, 48,900 people were on ODT Australia-wide (Australian Institute of Health and Welfare, 2022).
ODT programs are now run by all Australian States and Territories that, with varying rules, allow GPs, federally funded through Medicare, working in general practice settings to prescribe (Gowing et al., 2014). GPs are the focus of this research which sought to understand whether ODT policies, programs, and initiatives to support GP ODT prescribing have led to increased GP prescribing and use the state program in New South Wales (NSW), one of the Eastern States in Australia, as a case study to investigate this.
Past research suggests that GPs have been unwilling to prescribe ODT (Ezard et al., 1999; Jones et al., 2021). Currently in NSW, a number of large public ODT clinics and a small percentage of Medicare-funded GPs prescribe ODT (Bell et al., 2006; Penington Institute, 2023). The cessation of one prescriber, out of the small pool of ODT prescribers who provide the bulk of the care, can have a massive negative impact on program capacity (May, 2023; Penington Institute, 2023). In one region in NSW in 2023, the death of a prescriber and the retirement of another led to a sudden severe shortage of prescribers that left the system unable to cope. Prescribers from other regions in NSW took up the slack as best they could, some driving long distances or seeing people via virtual care and greatly expanding their patient numbers to support the continuation of care (Kamerman, 2023).
Australia has a tiered health system with divided responsibilities to fund and run health services between the Federal Government and six State and two Territory Governments. The Federal Government funds Medicare, a universal healthcare scheme, to support the cost of healthcare for all Australians. It also funds the Pharmaceutical Benefits Scheme (PBS), which subsidizes the cost of medications and partially funds state health services. Medicare funds GPs working in private general practice settings (Department of Health and Aging, 2019). Increasingly, Medicare funding for GPs has not been able to meet the cost of care and is supplemented with patient co-payments (Royal Australian College of General Practitioners, 2023b). This has led to decreased access to GP care for people of low socioeconomic status (Australian Bureau of Statistics, 2023). NSW Health is the state government entity that manages public health care for all residents in NSW from hospital to community health care (NSW Ministry of Health, 2023). This includes the NSW public ODT program (NSW Health, 2024), which provides access to ODT medications through multidisciplinary state-funded clinics. NSW Health also oversees the regulations for community ODT prescribers, most of whom are GPs, who are federally funded through Medicare.
NSW Health first permitted prescribed methadone for ODT in 1970 (McArthur, 2001) and has long been aware of the need to increase ODT prescriber and program capacity (NSW Health, 2022b). To do this, it has funded initiatives including education and support programs, refined legislation, and created policies and treatment guidelines to encourage prescribers, including GPs, to take up this work. It is unclear how well-targeted and effective these initiatives have been in supporting GP ODT prescribing in GP settings.
Research Aims
This research aims to explore and analyze the influence of programs, guidelines, policies, and other initiatives that sought to increase general practitioners’ participation in ODT prescribing from 1970 to 2023, using the state of NSW to draw out overarching themes. There are three parts to this research with individual aims.
Document review—aims to analyze the historical documentary evidence of NSW programs, guidelines, policies, and other initiatives with a focus on increasing GP ODT prescribing numbers. NSW prescriber and opioid dependence quantitative data—aims to assess if there is evidence that there has been a change in GP ODT prescribing numbers and how this has been compared to rates of opioid dependence in NSW. Key informant semi-structured interviews—aim to triangulate and enrich the documentary data and elucidate the political, human, and system factors that sit behind the documentation and affect the programs, guidelines, policies, and other initiatives that seek to increase GP ODT prescribing numbers.
Methods
This research uses a mixed methods approach (Creswell & Creswell, 2018) with three data sources; (1) documents; (2) quantitative data from “Clinical authority to prescribe ODT” applications and prevalence of opioid dependence data; and (3) Key informant semi-structured interviews (see Figure 1). These three separate data sources were used to build a richer understanding of some of the institutional and systemic aspects that may affect GPs’ participation in ODT prescribing.
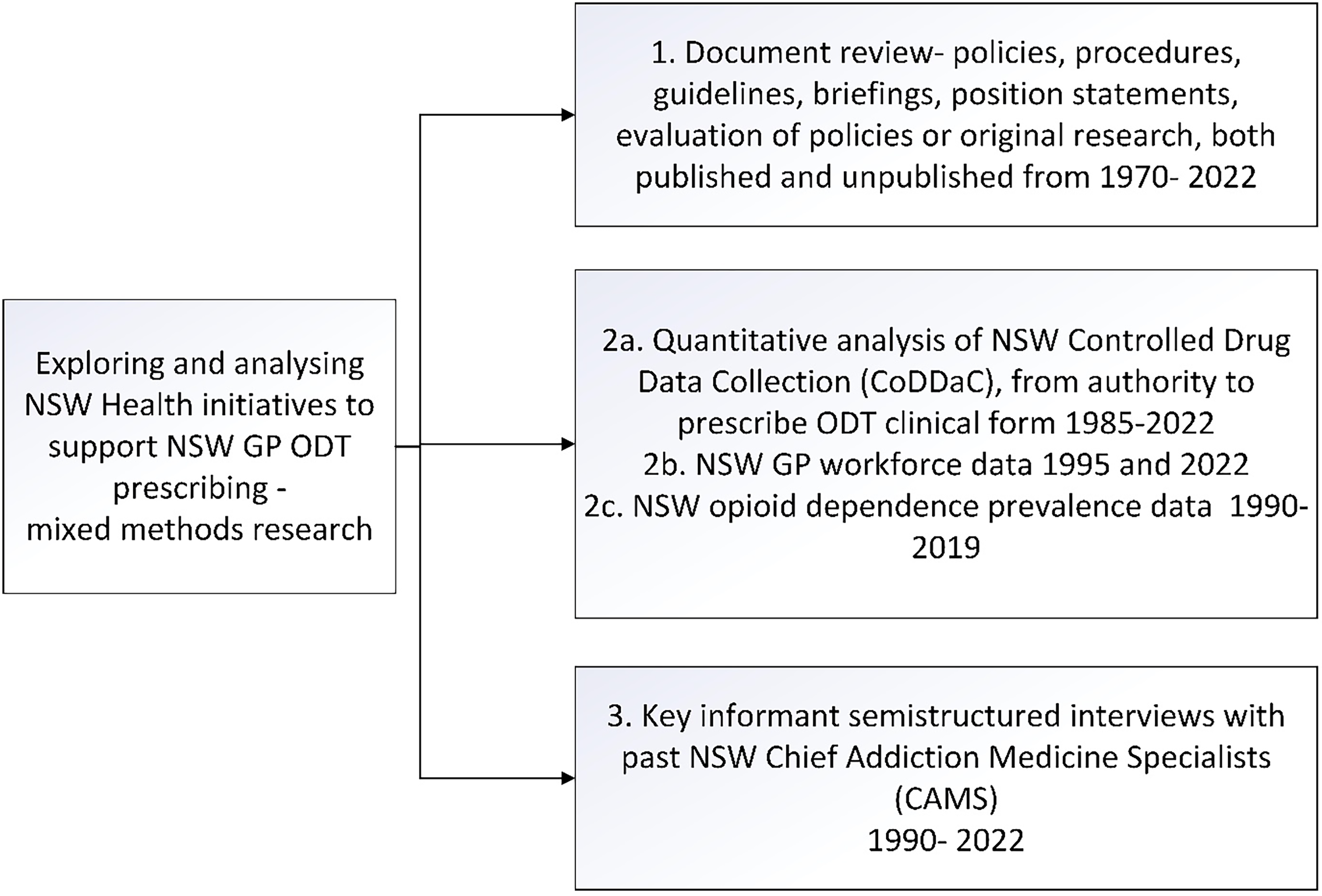
Overview of the data sources in this mixed methods study.
Document Review
A preliminary search for existing reviews on the topic was conducted via MEDLINE and Embase in April 2022, which showed no results. Documents from 1970 to 2022, including policies, procedures, guidelines, briefings, position statements, evaluation of policies, or original research, both published and unpublished, with a focus on ODT in NSW were included (see Supplementary Table 1 for inclusion and exclusion criteria). Key articles and key indexed terms helped refine the database search. The following concepts: policy, procedures, guidelines, opioid, opioid use disorder, OUD, opioid agonist treatment, OAT, ODT, GPs, Australia, and NSW were searched, combining keywords, indexed terms, and phrases. MEDLINE, Embase, PsycINFO, Scopus, Emcare, CINAHL, Web of Science, and Google were searched (see Supplementary Table 2 for the search strategy). In addition, NSW and Australian Government and Department of Health websites were searched. All documents were manually searched and any documents identified either within the text or reference lists were searched for via the above databases and Trove (National Library of Australia, 2023). For any documents that could not be located online, a request was made to NSW Health staff for access to copies. One document was found in hard copy and shared by a GP colleague. All identified records were collated into Covidence (Covidence, 2022). Duplicates were removed and titles and abstracts were screened against inclusion criteria. Given the exploratory nature of this research, the risk of bias and rating of quality of evidence was not assessed and results were not graded. Overall, 223 full-text documents were reviewed. Fifty-five were included in the analysis while 168 contributed to background information (see Supplementary Figure 1 for PRISMA).
The documents were used to create a timeline of important developments and a history of the evidence of the role of GPs in ODT from the start of the ODT program in 1970 to 2023.
Quantitative Analysis of NSW Prescribers and Opioid Dependence Data
Quantitative analysis of NSW Controlled Drug Data Collection (CoDDaC)
Quantitative analysis of NSW Controlled Drug Data Collection (CoDDaC) – from the “authority to prescribe ODT” form, available from 1985 to 2022. Whenever an ODT prescriber elects to start prescribing ODT for a person in NSW, they need to apply for a state authority for that person using the “authority to prescribe” form from NSW Health. The form is used to support the State regulatory authority's decision on whether to permit the prescriber to provide ODT for the person. These data are publicly available via the National Opioid Pharmacotherapy Statistics Annual Data Collection (NOPSAD)(Australian Institute of Health and Welfare, 2022), which occurs on 30 June each year. For data fidelity, the original data, sourced from state “authority to prescribe” forms, were requested from the NSW Controlled Drug Data Collection (CoDDaC) in the Chief Pharmacist Unit of NSW Health in May 2023. CoDDaC data collection was first undertaken in 1985 and data points, quality of data, and data cleaning have changed over time.
The following de-identified data points by year, from 1985 to 2022 are reported on in this paper;
number of people in the ODT program by drug type, number of people in the ODT program by prescriber type, number of prescribers in the ODT program by prescriber type and number of unaccredited prescribers (prescribers who have not done specific ODT training in NSW).
The prescriber type for this data is reported as public, private, unknown, or correctional. Given the primary interest of this paper is GP prescribers, these four categories are merged into two categories GP (private) and non-GP prescribers (public, unknown, and custodial).
It is important to note the weaknesses of this non-research, “real world” data, (Liu & Panagiotakos, 2022) for example; the “authority to prescribe” forms may not have been accurately or fully completed, they were not collected in order to undertake this research and data collection methods and analysis have changed over time. In these data, there are a large number of “unknown” prescriber types prior to 2017, and GPs are part of a generic group of “private prescribers.” The private prescriber group, which is likely to be predominantly GPs, also includes a small number of psychiatrists, addiction medicine, and other specialists prescribing outside public or custodial systems. It is also likely that GPs make up a proportion of the “unknown” prescriber type. For this paper, the assumption is made that all private prescribers are GPs and that GPs are not part of the “public, unknown and custodial” group. With these data limitations, the results must be interpreted with caution.
NSW GP workforce data 1995 and 2022
The CoDDaC data were compared to the publicly available NSW GP workforce data sources available for 1995 from the Australian Institute of Health and Welfare (Australian Institute of Health and Welfare, 1997) and 2022 from the Department of Health and Aging (Department of Health and Aging, 2023).
NSW opioid dependence prevalence data 1990–2019
The estimated prevalence of opioid dependence is publically available from the Global Burden of Disease Network for Australia from 1990 to 2019 (Institute for Health Metrics and Evaluation, 2020). This was used to estimate opioid dependence prevalence in NSW for this time period based on NSW population data. These data assume that opioid dependence occurs equally throughout all states and territories in Australia. The data suggests a wide range of prevalence; for example, in 2019, it suggests that there may have been between 96,000 and 139,000 people in Australia with opioid dependence. As a result, the data must be interpreted with caution.
Key Informant Interviews—Chief Addiction Medicine Specialists
This research does not seek to generalize to broader populations but gain an in-depth understanding of how NSW programs, guidelines, policies, and other initiatives may have changed NSW GPs’ ODT prescribing. As a result, semistructured interviews are appropriate and help to create a richer understanding of the NSW ODT program and work to engage GPs by nuancing the context, including important political and human issues that exist for the program.
Interviews were undertaken in 2023 with all five past incumbents of the role of a NSW Chief Addiction Medicine Specialist (CAMS). This post, created in the early 1990s was, and remains, an advisory role. As leaders in NSW Health, CAMSs were able to bring their subject matter expertise and understanding of public specialist Alcohol and Other Drug (AOD) services to assist NSW Health staff to understand the implications of policies and programs (NSW Health, 2023a). CAMSs gained deep knowledge of the issues faced by NSW Health during their time as CAMSs.
One CAMS undertook the role in the late 1990s and again from 2019 to 2022. All five men were or had been Clinical Directors in metropolitan and regional public AOD services in NSW. At the time of their CAMS role, they had no experience working in general practice or in the private specialist AOD sector.
An interview guide with prompts and probes was used to assist the conversation (see Supplementary Table 3 for the interview guide in the COREQ checklist for qualitative reporting).
The principal researcher and interviewer is a GP, addiction medicine specialist, experienced clinical interviewer, and educator, and known to all the participants. All past CAMSs consented to the interview, and these were audio recorded and transcribed verbatim. The transcripts, analysis, and themes were member-checked by participants to ensure trustworthiness, validation, and credibility. (Lincoln & Guba, 1985) Participants were able to remove any comments they felt were incorrect or could pose a reputational risk.
The data was inductively re-iteratively analyzed using qualitative content analysis (Drisko & Maschi, 2015) of both manifest and latent content. (Graneheim & Lundman, 2004) The concepts or codes were grouped under higher-order headings or themes that were modified on transcript review, discussion, consensus, and agreement with the interviewees and the research team. An audit trail was used to record the decisions made during the study and to help researchers reflect on the influence of their positionality, assumptions, and disciplines (see Supplementary Table 3 for the COREQ checklist for qualitative reporting) (Tong et al., 2007).
The participants are high-profile, well-known individuals. They held the CAMS role for specific time periods, and to avoid potential reputational risk, the analysis needed to avoid linking comments to particular times to ensure they could not be attributed to individual participants.
The three data sources analyzed in this paper allow triangulation to build more robust results. The themes raised in the document review and semistructured interviews create the discussion, informed by both data sources. The quantitative data is then used to assess if aspects and themes raised in the other data affected the number of GPs who undertook ODT prescribing. Integration of the analysis is limited by the need to ensure the quotes from the key informant interviews are not attributable to individuals.
In this paper, we assume that the interpretation of reality is subjective, various, and influenced by our unique interpretations. The conversation between the researcher and key informants is bound by context and values (Lincoln & Guba, 1985). The text in the documents and interview transcripts may have multiple meanings and our interpretation is influenced by our positionality and worldview. We take a pragmatist approach, seeking to create knowledge that is practical and assists our understanding of how we make sense of complex issues and work towards ideas that may have practical application (Gillespie et al., 2024).
The categorical data were analyzed using univariate descriptive analysis through Microsoft Excel. Ethics approval was sought and granted by the University of NSW Sydney (HC No HC220487).
Results
The three mixed-method data sources were triangulated and analyzed from 1970 to 2022. This analysis found a number of important changes and developments since ODT medication became available in 1970 in NSW that could have influenced GP ODT participation (see Figure 2 for a timeline of important developments and changes).
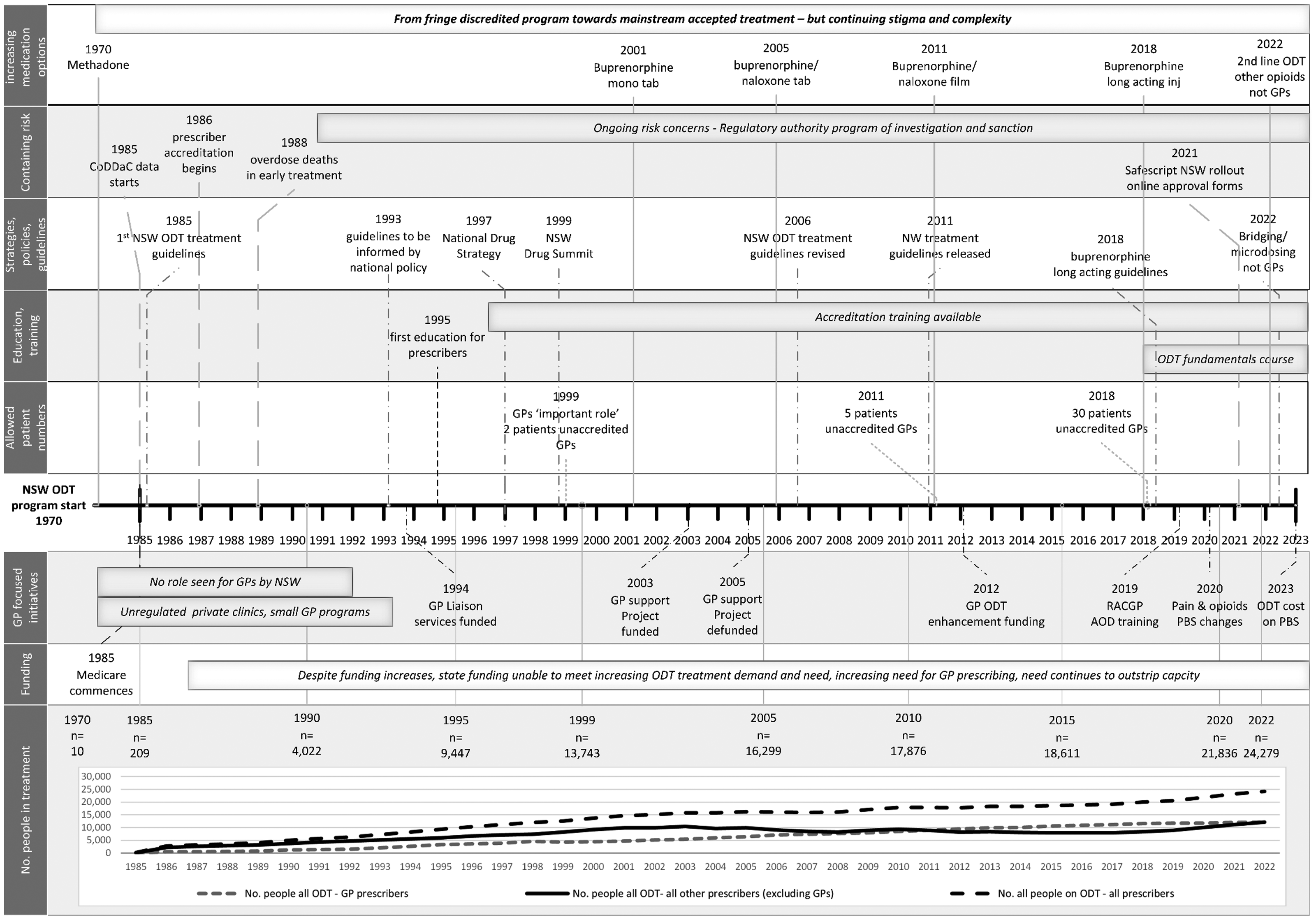
Timeline of important issues, developments, and changes in the NSW ODT program from 1970 to 2022.
These include
Increasing number of people in ODT treatment and GP prescribing Necessity to build GP prescriber numbers rather than an easy transition to GP care Increasing medication options Containing risk Strategies, policies, and guidelines Education and training GP focused initiatives Funding Politics of care—moving from discredited towards mainstream treatment
Increasing Number of People in ODT Treatment in NSW and GP Prescribing
When ODT medication first became an option in NSW in 1970, less than ten people accessed this care (Hall et al., 2000). It is unclear if any GPs were prescribers at this time. In 1985, 209 people in NSW were prescribed ODT of which 33 people (16%) were prescribed by three GPs. Since 2007, GPs have been the majority prescriber and by 2022, GPs made up 75% of all prescribers and were prescribing for 12,159 people, just over 50% (see Figure 3).
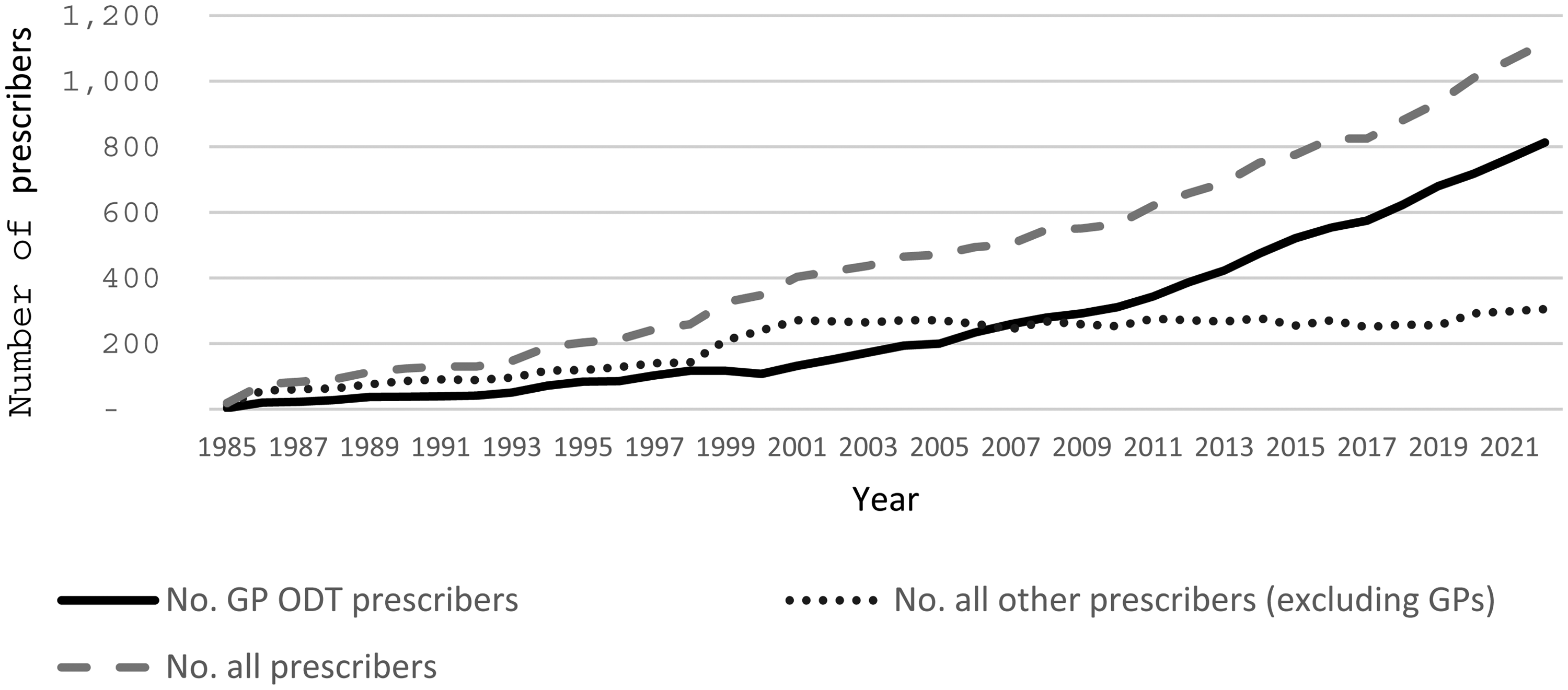
Number of GP ODT prescribers versus others and all ODT prescribers.
Between 1995 and 2022, the ratio of GP ODT prescribers to the total number of GPs working in NSW has more than quadrupled. This is from a very low base. In 1995, there were 5,220 GPs working in NSW (Australian Institute of Health and Welfare, 1997) and one in 62 of these GPs prescribed ODT. By 2022, with 12,438 GPs in NSW (Department of Health and Aging, 2023), one in 15 GPs (6.5%) prescribed ODT. CAMSs noted in their semistructured interviews that while NSW Health saw a need for GPs to prescribe, few undertook this work. There was a desire to see it (ODT) taken up by GPs and there was the evidence that this was not seen as a viable or exciting option by 95% of (general) practitioners… (CAMS.1dM)
In contrast to growing numbers of GP prescribers, the number of other (non-GP) prescribers has been flat since 2001.
The prevalence of opioid dependence in NSW grew rapidly in the 1990s and has stabilized since this time. (See Figure 4) The data suggest that treatment numbers have always been less than potential treatment needs (Institute for Health Metrics and Evaluation, 2020). By 2019, when 24,279 people were in treatment in NSW, the prevalence of opioid dependence was likely to be 36,242, with a range of between 30,482 and 44,014. This suggests an “unmet need” (i.e., people with opioid dependence who are not in treatment) of between 9,834 and 23,366 in NSW (32%‒53%, with a median of 43%).
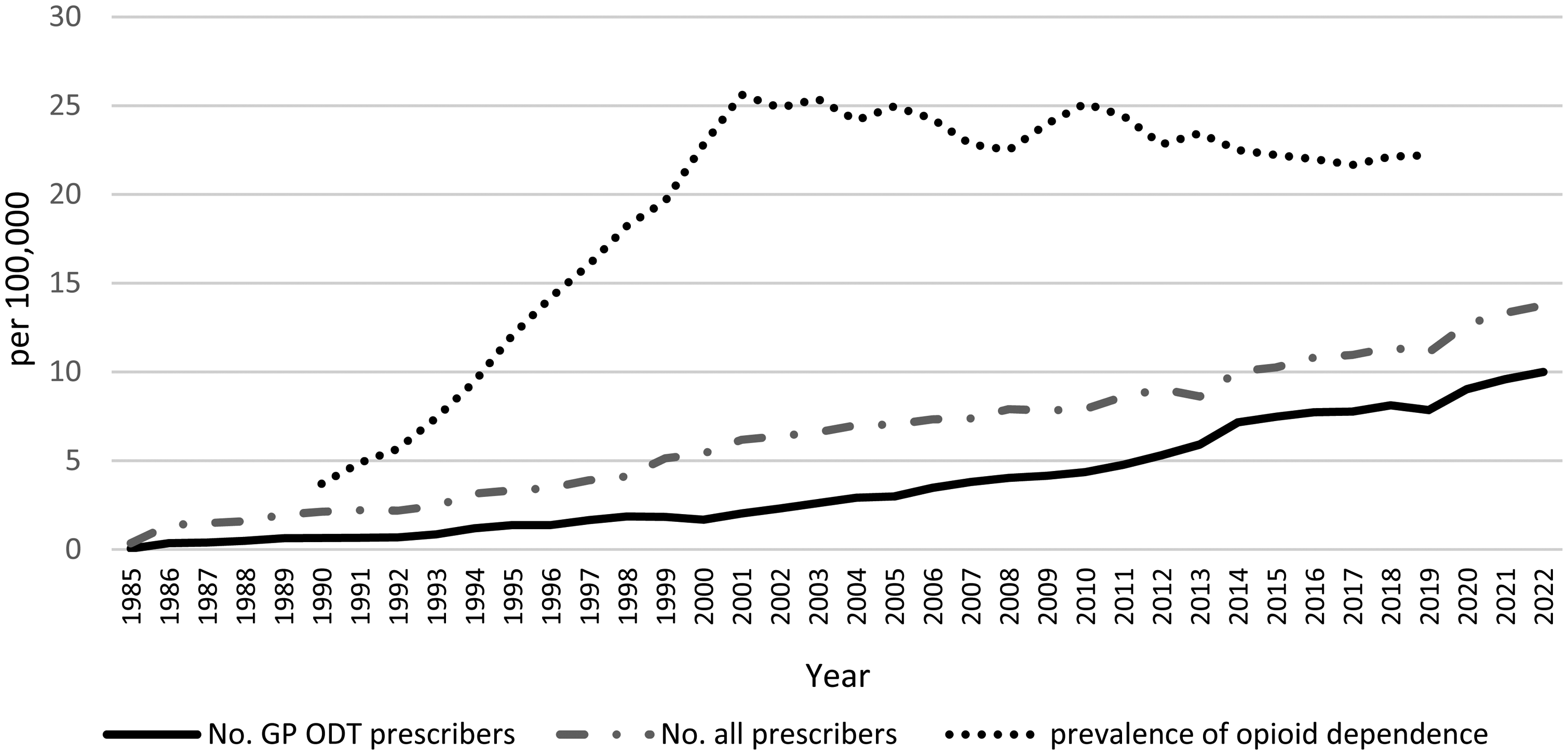
Prevalence of opioid dependence, and no. of people prescribed ODT by the prescriber type per 100,000 from 1990 to 2019 in NSW.
Necessity to Build GP Prescriber Numbers Rather Than Easy Transition to GP Care
Demand for ODT treatment has outstripped capacity for the entirety of the program (Hotham et al., 2003; Penington Institute, 2023). NSW public ODT services have always had limited funding and staffing. CAMSs pointed to this limited capacity and the need for the program to engage with GPs to manage demand. I think for a long time now there's been this push for GPs to prescribe because essentially the public system hasn't been able to manage the demand and the need… (CAMS.1dS)
The approach was reactive to need; GP ODT was not core to the public program. One CAMS suggested that NSW Health tried to portray GP ODT prescribing as a prize for GPs, something special that GPs were being allowed to do. In reality, GPs were seen as a way to relieve the burden on the public system rather than GP ODT being positive and a core activity for GPs. You can't offer this up as a prize when in fact it's (…) passing the ball to keep the system happier… (CAMS.1dM)
The CAMS agreed that it was the role of public AOD services to manage people presenting with complex clinical issues and to support GPs by taking over if a person's care became complex and beyond the capacity of the GP. …it's in the nature of our services that we have to pick up the pieces when they say, “I'm sorry I can't manage you because I don't trust what's going on”. (CAMS.1dZ)
While public services needed to work with GPs, this often didn’t work well in practice. Structures and processes were not well developed, and this led to GPs not being able to access the support they needed. Public AOD services were often unable or unwilling to respond, leaving the GP to manage on their own. …when we did try and say, you take these patients from us or you take some new ones and the minute you got a problem, we'll take them back. So often when the GP rang up to get them back in, the public (clinic) said ‘Oh look, no, sorry, we don't have a spare prescriber on. No, we can't do that.’ And they were left carrying the can. And I think that's just not good enough. (CAMS.1dM)
The majority of ODT-prescribing GPs (57%) in 2022 were unaccredited (untrained), and 65% prescribed for five or fewer people. This left a small subgroup of GPs prescribing for a large number of people with 79 (7%) of all prescribers (GP and all others), prescribing for more than 100 people each. CAMSs described the risk for these prescribers, who may be overwhelmed by patient needs and complexity. … those that did take it up,(…) they became totally consumed by it and overwhelmed by it and that was tragic. (CAMS.1dM)
The quality of prescribing and the retention of the small group of high-caseload ODT GPs providing care to more than 100 people remain unclear, and anecdotally, large caseloads are associated with stress and dissatisfaction and risk of prescriber attrition (Hotham et al., 2005; Hotham et al., 2003; Jones et al., 2021).
The fragility of the system was noted by CAMSs, creating a system at ongoing risk of collapse. Well, the whole structure is knackered, it could still explode. It really could. (CAMS.1dM)
Increasing Medication Options
Core to the NSW ODT program are the medications, methadone, and buprenorphine. Methadone first became available for ODT in NSW in 1970 (McArthur, 2001). Data on GP methadone prescribing is available from 1985, showing an ongoing increase in GP prescribing since this time, with GP methadone prescribing surpassing all other prescribers in 2012 (see Figure 5).
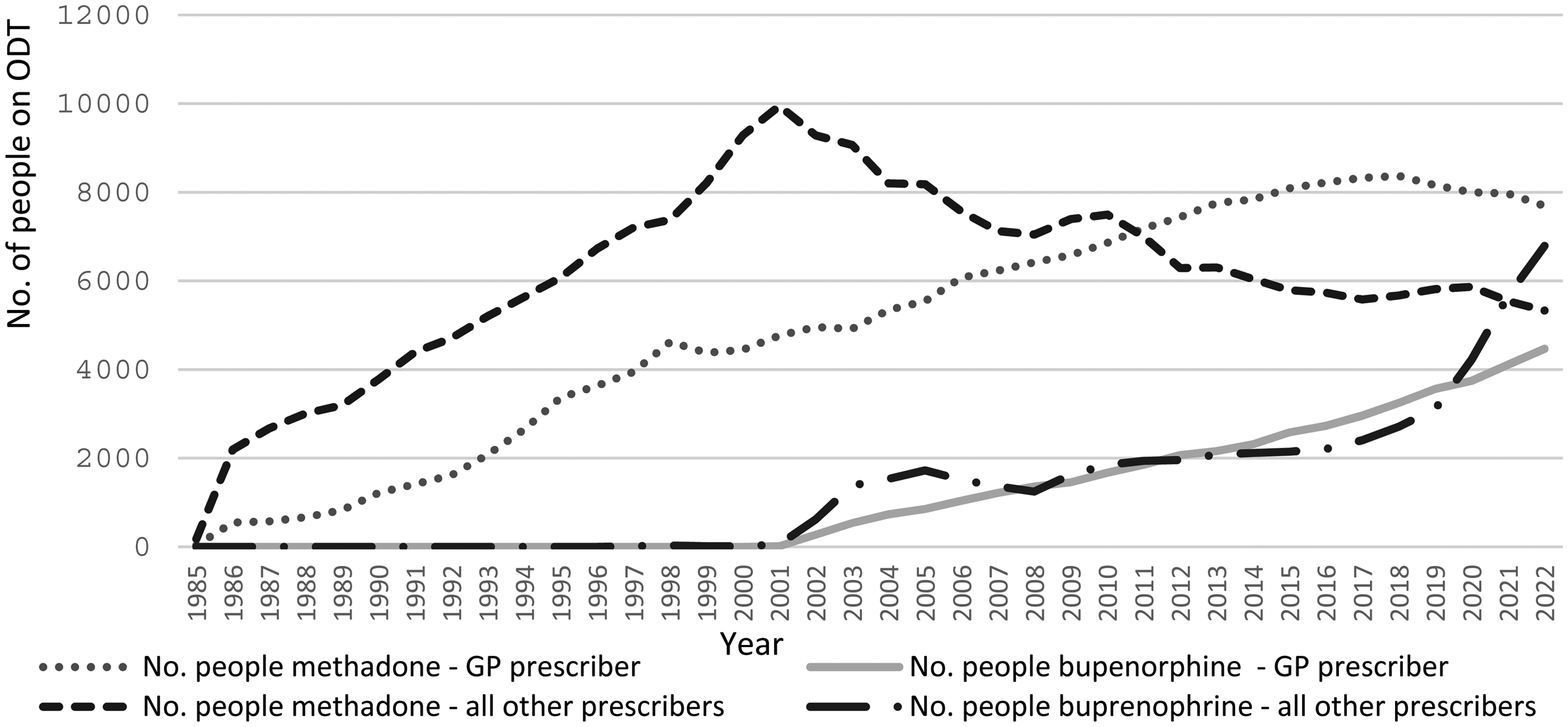
No. of people prescribed ODT by medicine and by the prescriber type in NSW from 1985 to 2022.
Methadone was the sole medication used until buprenorphine sublingual tablets became available in 2001. Sublingual buprenorphine/naloxone combination tablets were first available in 2006, sublingual buprenorphine/naloxone combination film in 2011, and long-acting injectable buprenorphine (LAIB) in 2018–2019. Rates of buprenorphine prescribing for NSW GP prescribers have steadily increased since 2001. In 2019, there was a slight decline in the number of people prescribed methadone by NSW GP prescribers. However, GP buprenorphine prescribing continued to increase at this time. There was a sharp increase in buprenorphine prescribing for all other prescribers from 2019. While the CoDDaC data does not delineate different buprenorphine formulations, it is likely that LAIB drove much of the increase in buprenorphine prescribing from 2018 (see Figure 5). LAIBs may have resulted in increased access to treatment (Lintzeris et al., 2024; Penington Institute, 2023), however, this formulation was only allowed in GP settings in NSW from late 2020, so the impact of this formulation on GP ODT prescribing may be underestimated.
Containing Risk
The early ODT program was ad hoc without guidelines (McArthur, 2001). The state considered it a specialist, short-term, inpatient, abstinence-focused program (Capelhorn, 1996; McArthur, 2001; Nicholas, 2022) for only the most “hardened” “addict” (McArthur, 2001). However, private outpatient programs were in operation at this time (Ward, 1995).
From 1985 to 1995, there was a rapid expansion of ODT in Australia (Bell, 1995; National Drug Strategy, 1997), and private outpatient programs increased in number. Standards were low, with little oversight of care quality or outcomes (Ward, 1995). Prescribers were untrained and unmonitored by authorities beyond requiring an individual state authority for each person prescribed. Inappropriate prescribing led to non-opioid dependent people commencing methadone and overdosing (Reynolds et al., 1976). In 1989, in Victoria, a number of methadone overdose deaths occurred in the first few days of treatment due to toxic serum methadone levels (Drummer et al., 1990).
While GPs were needed, CAMSs suggested that they were seen as risky by NSW Health, with concerns about their ability to safely manage methadone in their setting. The feeling was that methadone was probably not something we felt (could)…be prescribed by a significant number of private practitioners. So even though we mouthed the mantra that it would be good to have more GP prescribers, I think there was the sense that methadone came with real risks, that sticking to policy and that was the other thing that was underpinning all discussions. (CAMS.1dM)
To control risk, the NSW government began to limit the number of people an individual prescriber could treat (NSW Health, 2001). Accredited (trained) prescriber numbers were capped at 10–120 people and over time this was increased to 200–300 people per prescriber on training completion (NSW Health, 2001, 2018a). Untrained (unaccredited) prescribers could only prescribe for up to two people and each approval came with onerous conditions; a discussion with an AOD specialist, initial dosing at a specialist unit, a case manager, and AOD service support (NSW Health, 2001). In 2011, the unaccredited prescriber requirement to link with AOD services was removed and numbers were increased to a maximum of five people stable in treatment (NSW Health, 2011; Puplick, 2014). In 2018, the number limit was increased, and nonaccredited prescribers were permitted to prescribe up to 30 people (10 on maintenance methadone and 20 initiated and/or on maintenance buprenorphine) (NSW Health, 2018b). CAMSs noted that the increases in unaccredited prescriber numbers were seen as a huge shift for the program and for NSW Health but did not really assist GPs in prescribing ODT for more people. …at the time, it seemed a huge hurdle, maybe a sociological hurdle or practical hurdle to have GPs prescribe, like, unaccredited GPs to prescribe for 10 patients, so that, I don't think it ended up being a great leap forward, but it was psychologically a great leap forward. (CAMS.1dF)
CAMSs reported that NSW Health was thought to have little control over GP ODT decision-making, potentially leading to poor practice. Basically, as long as you have a permit (the regulatory approval for each patient for all ODT prescribers). You're kind of untouchable, you know, unless you're talking gross negligence. (CAMS.1dH)
Conversely, minor infringement may have led to censure for some prescribers for small differences in clinical practice not clearly linked to risk. CAMSs suggested that hearing about these experiences of censure from their colleagues deterred potential GP ODT prescribers. In this field we were given that sense that, oh no, if you're giving 5 takeaways a week after 12 months, you are almost criminal and that was coming through to GPs and clearly they would talk to each other (…) and then they just look at their friends being picked off. (CAMS.1dM)
Buprenorphine with a lower risk profile may have driven increased interest in GP prescribing; however, the hurdles to prescribe were an ongoing issue. Both methadone and buprenorphine are considered high-risk medicines by NSW Health, and the policies guiding the use of both medicines have high administrative barriers. CAMSs suggested shifting this and creating policies appropriate to the medication risk level. But I don't think we can continue to roll out the same models of care. But when we talk about, let's decouple buprenorphine for methadone, it's interesting because (…) the government has a very different understanding of what that means. And, they're not really decoupling it at all. (CAMS.1dH)
Another initiative, real-time prescription monitoring, SafeScript NSW, was introduced in NSW from April 2021 to early 2022 (NSW Health, 2023b) to assist risk management. This tool, used by prescribers/pharmacists to guide safer high-risk medicine prescribing and dispensing (Wilson & Hargreaves, 2022), remains voluntary in NSW and not all GPs use it. There is some evidence that this tool has increased GP aversion to opioid prescribing for pain (Prathivadi et al., 2021), and this is likely to have made ODT prescribing even less attractive.
Strategies, Policies, and Guidelines
Strategies, policies, and guidelines have not well articulated the role of GPs. The National Drug Strategy in 1997 noted the need to create public-private partnerships to create access and equity and supported training and routine data collection, including prescriber attributes (National Drug Strategy, 1997). It did not discuss the role of GPs.
National and NSW State guidelines became available in 1985 and have been revised over time (National Drug Strategy, 1997). The guideline focus was on the safe commencement and continuation of treatment, providing guidance on doses, patient stability, and provision of supervised and takeaway dosing to provide effective treatment (Gowing et al., 2014; NSW Health, 1999b, 2011, 2018a). Guidelines were updated as various buprenorphine formulations became available (Lintzeris et al., 2019b; NSW Health, 2001, 2011). The guidelines detail appropriate settings based on patient complexity (Lintzeris et al., 2019a; NSW Health, 1999b, 2011, 2018a). There has been little focus on prescriber attributes, whether they are GPs or specialists, or the workplace environment (Gowing et al., 2014; Lintzeris et al., 2019b; NSW Health, 1999b, 2011, 2018a).
The health system tried to manage risk with regulations and policies. Regulations and guidelines limited the GP role and it is likely this approach made ODT less attractive to GPs. CAMSs suggested that they were inward-focused, and the experience of other jurisdictions suggested that the program could be more flexible. [the guidelines were] over controlling and rigid. You know the idea that a GP could not start a patient at a pharmacy. Like it's not possible, you can't do it safely (…) then you cross the border and there's nowhere that anyone can start other than a GP at a pharmacy. So, there was a lot of (…) .weird stuff that was historical in NSW ODT system that was very much about, it had come from the public ODT system. (CAMS.1dH)
Most opioids (excluding those licensed for ODT) are medications that GPs prescribe regularly without the need to do further training. The rigid regulatory approach of ODT may have impacted GPs' willingness to prescribe as the complexity of training and accreditation may have signaled to GPs that ODT was difficult. CAMSs reported that the guidelines were too long and detailed, creating a hurdle for GPs, becoming a text book on treatment targeting specialist services rather than practical prescribing guidelines. So, in the end we start writing major documents about two drugs, which is the same group of drugs that GPs are writing scripts for without any of this claptrap… (CAMS.1dM)
Recently, short guides abbreviated from the full guidelines have been created to assist busy prescribers, potentially with a focus on GPs (Lintzeris et al., 2019a; NSW Health, 2018b). In 2022, the NSW ODT “authority to prescribe” form was updated, providing more information and links to clinical advice to support inexperienced prescribers (NSW Health, 2022a).
Education and Training
No ODT education supported the early program. In 1995, 61 doctors had completed an ODT accreditation course, with 83% commencing ODT prescribing, mostly in public settings (Bell, 1995). In a post-training survey, participants suggested the course was inadequate for GP settings (Bell, 1995). The NSW Pharmacotherapy Accreditation Course (PAC) commenced in the late 1990s. A day-long course included a written examination, 2–3-h clinical placement with a specialist ODT prescriber, a written case discussion, and approval from NSW Health (NSW Health, 2011). After the 2001 introduction of buprenorphine (mono) sublingual tablets, the PAC was amended and accredited ODT prescribers were given a 15% increase in patient numbers after completing additional training (NSW Health, 2001). The training has been re-iteratively updated, with online and in-person options (University of Sydney, 2024). Focused on the accreditation of prescribers, it was renamed the Opioid Treatment Accreditation Course (OTAC).
The training was seen as core but not well adapted to assist GPs as it was more focused on the environment and needs of prescribers working in the public clinic setting. GPs weren't a core part of that new (opioid treatment accreditation) course. (CAMS.1dF)
CAMSs noted the need to make training more accessible for GPs. We knew that there would be a greater role for GPs without all the OTAC (Opioid Treatment Accreditation Course) bells and whistles and all that kind of stuff. So, there was a recognition that (…) we created a hurdle that may have been putting some doctors off. (CAMS.1dH)
From 2018, the course included greater emphasis on prescribing in GP settings. The offerings included the “Fundamentals of Opioid Treatment” course, a short online course available 24/7 covering basic understanding of ODT as well as the longer Opioid Treatment Accreditation Course (University of Sydney, 2023). An analysis of the courses in 2018 found that 70% of participants worked in metropolitan settings and 49% were GPs (Winter et al., 2018). It is possible the greater training options have positively impacted GP prescribing.
GP Focused Initiatives
Early ODT programs did not see a role for GPs (O'Neill et al., 1985), and only a small number of GPs prescribed (Ward, 1995). In 1993 there was a move towards mainstreaming and normalizing ODT “including the management of prescriptions by general practitioners, dispensing in community pharmacies and the integration of methadone services into the activities of primary health care centres and hospitals” (Ward, 1995, p. 62). It was suggested that GP settings might be beneficial and preferred by people accessing treatment (Ward, 1995).
Over time, GPs were increasingly seen to have a role (NSW Health, 1999a, 1999b, 2000; Ward & Mattick, 2005). As demand for ODT increased, improving access to ODT depended on increased GP involvement (Ward & Mattick, 2005). GPs could provide a continuum of care, and aftercare as external providers (NSW Health, 2000). CAMSs suggested that being seen in GP settings could reduce community concerns and stigma by reducing crowding on the streets outside ODT clinics. getting general practitioners (…) stops the crowding around clinics. It makes for a more invisible, less stigmatized system… (CAMS.1dZ)
There was recognition that people on ODT needed general health care which could be better achieved by GPs than specialist AOD services. part of it too was, you know, that notion of well, looking after the whole patient. (CAMS.1dS)
While GP ODT has been part of the narrative since the 1970s, there has been little strategic engagement with GPs with few actual mechanisms to do this. CAMSs noted that there were few resources, forums, networks, or strategies that could support GPs and a concern that current initiatives would make little difference. …there was no resourcing and there was no clear action. (CAMS.1dS) It's also been an absence of any mechanisms for NSW Health to actually engage with private healthcare. So, there are no forums to talk to private psychologists. No forums talk to the private drug and alcohol services. No forums to talk to GPs. There's no network of GP prescribers for ODT. Nothing has been put in place to engage support, listen to, guide what happens in private practice. (CAMS.1dH)
The system was described as “a mess.” It was fragile, with an ongoing risk of a significant decrease in treatment access if a small number of prescribers stopped providing ODT. There was seen to be little real strategy that would increase ODT program capacity by greatly lifting GP prescribing numbers. …we have no strategy for engaging GPs and I look at what the Ministry (NSW Health) have at the moment, their ODT strategy, you look at all that and think, even if you did everything you said you were gonna do. Is it going to shift the dial on the big problem here? And it's kinda like, I don't see how if you did all this stuff, I don't understand how it's gonna get us out of the mess we're in. (CAMS.1dH)
Local GP share care programs have received time-limited state funding but without implementation strategies. …we got the enhancements for shared care positions. I think every LHD got funding for one or two positions (…) but no guidance, no instructions, no what are you supposed to do with this? No performance targets, nothing, so, you know, the sense that we got is that the LHDs just took the money and absorbed it into routine ODT, so (…) it's not like that created in any sustainable positions. (CAMS.1dH) In the end, the funding for (…) those positions got stopped. (CAMS.1dS)
From 1994 to 2000, the NSW Central Coast public AOD service GP Liaison team supported local GPs. Forty GPs were willing to prescribe and by 2001, 22 GPs (11 accredited through training) provided ODT for 321 people in the local area (Astolfi & Willey, 2001). Sometime before 2003, NSW Health funded a statewide GP Support Project to increase the number of GPs attending ODT prescriber training (Hotham et al., 2003). This funding ceased in 2005 (Winstock et al., 2008).
A 2007 review of NSW public ODT services found low levels of engagement with local GP Divisions and short-term localized strategies (Winstock et al., 2008). ODT services reported transferring stable patients to GPs and some ran GP clinical placements (Winstock et al., 2008). There were variable assessment processes and tools to support transfer (Winstock et al., 2008). GPs continued to have roles as prescribers, case managers, multidisciplinary team members, and providers of general health care (Gowing et al., 2014; Lintzeris et al., 2019b; NSW Health, 1999b, 2011, 2018a).
In 2012, public specialist ODT services in NSW were given ODT enhancement funding. Generally, this was used to employ additional staff to assist with ODT medication administration. Some LHDs employed nurses to liaise with GPs (Wilson et al., 2022a). Federal funding from 2016 for Primary Health Networks (PHNs) to commission services (Department of Health and Aging, 2016b) has led to some funded ongoing public specialist AOD GP liaison programs (Central Sydney Primary Health Network, 2024).
NSW Health also funded a 24-h telephone AOD advisory service. While this was not specific to ODT, GPs could ring this service for ODT advice. GP knowledge of this service may be low (Wilson et al., 2022b).
External organizations have created support tools for GPs. In collaboration with NSW Health services, federally funding Primary Health Networks (PHNs) have introduced an online clinical decision-making tool; HealthPathways (HealthPathways Community, 2023) with localized referral pathways and clinical information for many health conditions, including opioid dependence. The Royal Australian College of General Practitioners (RACGP) guidelines on drugs of dependence, including opioids, focused on the safe prescribing of opioids (Royal Australian College of General Practitioners, 2017). The management of opioid dependence was out of scope; however, it is mentioned as sequelae of opioid use and links to further information. The RACGP has a specific interest group in addiction with 2500 members, some with an interest in ODT (Royal Australian College of General Practitioners, 2024). Both RACGP and the Australian College of Rural and Remote Medicine (ACRRM) were federally funded from 2019 to 2023 to train GPs in AOD and ODT prescribing. The impact of this training on GPs and ODT is unclear (Royal Australian College of General Practitioners, 2023a).
Funding
Early funding for ODT in all settings was low. Additional funding in the 1980s increased NSW public ODT program capacity (Ward, 1995), but demand outstripped supply (Bell et al., 2006). From the mid-1980s, universal health insurance, Medicare, funded private doctors/GPs to provide community care, including, but not specifically, ODT treatment (Department of Health and Aged Care, 2024). As a result, Medicare-funded private doctors/GPs in unregulated, private, for-profit, ODT programs proliferated, and patients were charged $6–7 per daily dose (Capelhorn, 1996). Doctors/GPs working in these clinics were likely to limit care to ODT medication alone (Capelhorn, 1996). In addition, small Medicare-funded programs, often less than 10 patients, ran from GPs’ private rooms with community pharmacy dosing (Capelhorn, 1996). ODT prescriber and service funding options remained largely unchanged throughout this time. NSW public health continued to encourage Medicare-funded doctors to provide ODT (Ward & Mattick, 2005), a strategy driven by cost, the need to increase capacity, and to encourage people to address general health needs.
State ODT services were small with limited capacity and CAMSs suggested that there was a need to shift to Medicare-funded GPs to take financial pressure off the state system, cost shifting from state to federal funding. …the State government looked at the idea, maybe we should be getting general practitioners to do that and I thought, great idea because that has all the benefits of cost shifting to Medicare… (CAMS.1dZ)
Unfortunately, Medicare rebates for GPs are not seen to be sufficient nor an encouragement to take on ODT prescribing in the GP setting (Penington Institute, 2023; Ward & Mattick, 2005).
GPs do not sit easily under the NSW Health umbrella. They are not employed or funded by the NSW Government but rather funded by the federal government and patients themselves through Medicare and patient co-payments. CAMSs suggested that the state versus federal funding divide caused fragmented governance and responsibility, leaving NSW Health with little power or ability to work effectively with GPs to support ODT prescribing. New South Wales will say that's Commonwealth. And to a large degree, they’re right. So, who's responsible for opioid treatment in NSW? Well, on the one hand, some things are state responsibilities. On the other hand, you know what GPs do; it's got very little to do with the state. (CAMS.1dH)
Given the state-federal funding and responsibility divide, CAMSs suggested that it was difficult to think of what else NSW Health could have done to increase GP ODT prescribing. I think it's a really tough area to think about what else the Ministry (NSW Health) could have done (to work with GPs). (CAMS.1dS)
The Politics of Care—Moving from Discredited Towards Mainstream Treatment
CAMSs suggested that ODT has been seen as politically risky by a number of NSW state governments. Politicians may share the prevailing stigmatized views of the general community, and lack of support is an issue. …the greatest challenge for the for opiate treatment is the lack of political support for it and the fact that (…) there isn't public support by Health ministers or premiers in NSW. That's sort of, quite notable… (CAMS.1dF)
As a result, there has been ongoing concern that ODT programs were at risk of closure if there was seen to be harm. This has driven some of the anxieties about the risk of GPs undertaking this work in the GP setting. …it was a very political treatment that we were dealing with and whilst bupe (buprenorphine) is safe and all the rest of it, at that stage, it hadn't proven itself absolutely, so we were concerned that if it ran rampant and there were a few deaths, the whole program would be shut down. So that was an underpinning fear that the Minister could close the program and remove a lifesaving treatment from the number of people who needed it. (CAMS.1dM)
NSW Health was seen as having different priorities with GPs not high on that list. They were an afterthought. It (GP prescribing) was not a high priority. (CAMS.1dF) GPs were never front and centre was my way of looking what's happening in New South Wales, always been an afterthought when it comes to everything. (CAMS.1dH)
There was seen to be limited understanding of GPs and the GP environment by NSW Health, public clinic staff, and prescribers. We haven't really refined it that well at a very practical down to earth level in a clinic or in a GP practice. (CAMS.1dM)
GPs were often thought of as a homogenous group. CAMSs suggested that there needed to be different approaches for different GPs. We can't keep thinking of general practice as general practice. We've gotta think about, well, which groups in general practice do we wanna really try and engage and then work with? … And I think that's probably where we're gonna get more value. (CAMS.1dS)
NSW Health did not have a policy or framework for prescription opioid issues that clearly delineated the role of GPs. High on the agenda, no. Even medium on the agenda, no. You know, probably could get mentioned if we were brainstorming or something (…) clearly this is an environment where there's no state drug and alcohol plan or policy or framework and there were efforts to have a framework (…) and primary care would have been mentioned in that(…) but it was never adopted, so it didn't matter. (CAMS.1dF)
Instability in NSW Health itself with the shifting political landscape impacted the effectiveness of State programs and their ability to work with GPs. …it was a period of change within the Ministry, lack of stability (…) that inevitably, at some stage, had an impact. (CAMS.1dF)
Nationwide, limited GP capacity due to the level of demand for GPs, limited GP numbers, and the negative impact of Medicare policy leading to limited GP funding were noted. This was seen to negatively impact GPs' willingness to take on ODT. People accessing ODT may experience poverty and have multiple health and social needs. Limited federal health funding leads to the need for GPs to charge patients directly rather than offering universal free access to care. I think general practice is burdened, thin, stretched, overstretched and people don't want to take on difficult patients because they don't have to because there's not enough GPs (…) the 10 years of Medicare freeze it's really such a slap in the face and well, it's heading towards American medicine. It's basically denying universal healthcare as you've gotta charge fees and it's very demoralizing. (1dZ)
Participants reported that the current model was created years ago and has not changed or adapted to the changing environment. It has no real strategies to engage with GPs. The sense was that the regulations were set up, the policies in place, and training available and as a result, GPs would want to do this work without any real attempt to put in place the support GPs needed. We set up the model 30 years ago. And (…) just basically (…) it's locked in and it's kind of the assumption is, well, that's the way we do it. We've got OTAC (opioid treatment accreditation course). You get credentialed. You're allowed to prescribe. Job done. And the assumption is that these doctors will just keep coming somehow for some reason. (1dH)
With the increased prescribing of opioids for chronic pain and increasing risky opioid use, (Campbell et al., 2015) several policy and regulatory changes have occurred. In 2010 codeine was moved to Schedule 3 (pharmacist-only medicine) to stop unregulated sales without pharmacist input (McCoy et al., 2018). In 2016, codeine became Schedule 4 (prescription only) (Department of Health and Aging, 2016a). In 2020, TGA and PBS conditions and indications for the use of opioids in chronic pain were tightened (Wilson et al., 2020). People seeking treatment for pharmaceutical opioids were increasingly seen in AOD services (Campbell et al., 2015). This may be due to GPs decreased prescribing associated with concern about prescribing risk (Fetene et al., 2020) and fear of censure from regulatory processes (Hendrie, 2018). This may have increased GP reluctance to prescribe ODT. …the resistance, the reluctance, the anxieties about opiates are enormous and those anxieties have increased since then, as has the awareness of overdose awareness of diversion. (CAMS.1dZ)
Discussion
This paper describes a complex and fragile program. One with limited capacity, easily overwhelmed by small changes. It is “knackered,” worn out, broken and tired (Collins, 2024) with continuing unmet needs. These issues are replicated in other jurisdictions and countries. In 2022, in the United States, only 25% of those who needed ODT were able to access treatment (Dowell et al., 2024). While in Europe, ODT was not available to all (Vranken et al., 2017) and coverage varies across countries, with many below the WHO target of 40% coverage (European Union Drugs Agency, 2024).
With no net increase in NSW-funded public ODT prescriber numbers and even a potential decrease (Jones et al., 2021), a necessary and conflicted cost-neutral solution to increase capacity has been increasing GP ODT prescribing in the GP setting. In 2022, 75% of NSW ODT prescribers were likely to be GPs, most unaccredited (without additional training). These GPs provided ODT for just over 50% of people accessing ODT. GP ODT prescriber numbers have increased from a very low base by 400% over many years from 1985 to 2022. With nearly 12,000 GPs working in NSW (Department of Health and Aging, 2023), 93.5% do not prescribe ODT. It would appear that there may be a greater capacity for GPs in NSW to provide ODT care, but this has not occurred.
Ongoing funding limitations for GP ODT prescribing are an important barrier and remain unaddressed. GPs bring a unique, holistic approach to patient care and, federally funded by Medicare, they are core to primary care in Australia. They can have a long-term role in both prescribing ODT and providing general health care, but this potential has not been fully realized. Medicare funding has stalled and in 2023, GPs remain inadequately funded by Medicare (Butler, 2023). This has resulted in increased patient contribution (Australian Institute of Health and Welfare, 2023). Many people who could benefit from ODT live in poverty (Tran et al., 2022) and are unable to afford a patient contribution (Australian Bureau of Statistics, 2023; Australian Institute of Health and Welfare, 2020), leading to decreased access to care. Some GPs continue to provide care without patient contribution. However, this necessitates short consultations for business sustainability, which may not allow GPs to assist patients with chronic conditions (Timms & Young, 2023). There has never been state funding for GPs to provide ODT in GP settings, and Medicare remuneration has long been considered inadequate for the administrative and clinical requirements of the sometimes complex nature of ODT (Abouyanni et al., 2000; Ward & Mattick, 2005).
In 2023, the cost of dispensing ODT medicines was included for the first time on the Pharmaceutical Benefits Scheme (PBS), decreasing medicine costs from $140–200 to $7.30–30 a month (Tsirtsakis, 2023). This funding, while mainstreaming ODT medicines and a financial win for people accessing ODT, does not provide funding for prescribers.
Early program illegitimacy, the 1989 Victorian overdose deaths early in ODT treatment (Drummer et al., 1990; Ward, 1995), and opioids; high-risk medications, being core to the program, fuelled concern that poor prescribing risked the program falling into disrepute. If people overdosed, if these medicines reached the informal markets, were sold to young people, if people with opioid dependence were seen as benefiting, getting things for free, rather than being punished, there was a risk that the ODT program could become politically unpopular and a fear this could lead to closure. This may have stymied engagement with GPs. This issue still echoes today.
The NSW State Health System does not employ or fund GPs and has limited control and power to influence GP decision-making. They have limited coercive power to control quality and safety if GPs choose to undertake ODT prescribing. The competing demands of supporting state-funded services and concerns about lack of power and influence have been and continue to be live issues, and, as a result of these complexities, the state's ability to effectively support GPs has been muted.
To mitigate risk, NSW specialist services have led new treatment development and updated guidelines to support GP ODT prescribing. A process has been repeated as each new formulation of buprenorphine became available in NSW. Updated guidelines focused on patient presentation with little focus on the clinical setting. They were extensive, seeking to provide all needed information. While the information in the guidelines is excellent, the length and complexity can be a barrier for the busy GP and infer that treatment is complex and dangerous, that ODT is risky and can only be done in specialist settings. Recent guidelines have included summaries of the guidelines directed at generalists, but they do not provide practical information for GPs (NSW Health, 2018b). NSW Regulatory authorities work to control risk with state-based accreditation and approval processes. These have been necessary historically, but the complexity of these processes may be a barrier. Heavy-handed regulatory responses may encourage GPs to disengage from prescribing (Payne, 2024; Prathivadi et al., 2021). Technological (e.g., electronic medical records and prescription monitoring systems) have improved over time, providing more information for GPs, streamlining and integrating procedures with Safescript NSW, increasing patient numbers for unaccredited prescribers and easy access to a continuously available, online, free, ODT fundamentals course. The impact of these recent initiatives is unclear.
NSW Health has funded education, guidelines, training, and support for GPs; however, GPs have never been the main focus of the NSW Health ODT program, and the shift to ODT in the GP setting has not been an easy or natural progression for ongoing care. State-based initiatives have likely had some impact to date. The suite of changes over time, including training, support, access to new medications, and simplifying prescribing applications, have supported GPs to do this work, and we see this with the steady increase in GPs over the program's history.
The State approach to supporting GPs to commence and maintain long-term ODT care in Medicare billing settings has, unfortunately, been haphazard. It has been dogged by a lack of strategy and focus, with minimal resourcing, short-term approaches, and poor understanding of the practical needs of GPs working in Australian general practice. The transition of people stabilized on ODT from the specialist setting to GPs has generally been serendipitous. There have been attempts to support and engage GPs with GP Liaison and shared care programs (Wilson et al., 2022a), these have generally been short-term, with limited funding and probably of mixed effectiveness with unclear or not fully realized outcomes and little independent, rigorous evaluation. Initiatives, such as training and supporting GPs for a short period of time, sought to drive change in culture and model of care for long-term change. This approach misunderstands the complexity of issues that face Medicare billing GPs. In specialist AOD services providing ODT, ODT is core to the service, while for GPs, it is just one of the many tasks and conditions managed in the GP setting. It cannot be assumed that a short-term project will drive sustained change as ODT is not a core or common business for most GPs.
Systems barriers matter. In NSW, 6.5% of GPs provide ODT. In the US, methadone can only be prescribed in specialist settings (Calcaterra et al., 2019), and 3% of US GPs, who need a specific license, prescribed buprenorphine in 2015 (Goodnough, 2018). This contrasts with the UK where 50% of GPs prescribed ODT in 2005 (Strang et al., 2005), Ireland where 54% of GPs trained in ODT in 2018 (Collins & Homeniuk, 2021; Delargy et al., 2019) and France, where, with minimal regulatory structures, 43% of GPs treated ODT in 2012 (Poloméni et al., 2015). GPs will not automatically prescribe ODT and systems barriers compound the issues of stigma, poor remuneration, low knowledge, confidence, and lack of specialist support reported in the literature (Barry et al., 2009; Barry et al., 2010; Holliday et al., 2013; Kennedy et al., 2019).
Strengths and Limitations
This research is strengthened by the positionality of the researchers. The credibility of the researchers as colleagues and insiders enabled honest conversations in the interviews. The interviewees spoke frankly about the issues they saw because they knew the researchers and there was awareness of a shared understanding of the clinical and practical challenges faced. This increased interpretive authority. Each of these data sources have limitations and triangulating through different methods and sources strengthens the analysis. CAMS interviews only canvassed the views of five senior doctors. Other staff working in NSW Health may have had differing views. GPs undertaking ODT may have experienced the program differently. NSW ODT documentation may be incomplete and may not explicitly state the role of GPs. Superseded documents are no longer publicly available. The CoDDaC data has serious limitations. It has four categories of prescriber type; public, private, correctional, and public/private (unknown). GPs are likely to be private prescribers. The number of “unknown” prescriber types (listed as public/private) is very high at 74% of all prescribers in 1985 decreasing to 49% of all prescribers in 2003. It is not until 2015 that the “unknown” prescriber category drops below 10% of all prescribers. From 2017, the percentage of “unknown” prescribers is 2% or less. This means that comparing prescriber types is particularly inaccurate until 2017. This paper assumes all private prescribers are GPs. It is likely that a proportion of the “unknown” prescribers are also GPs, and as a result, the figures on GP prescribers may be conservative up until 2017.
Conclusions and Implications
The issues of risk, funding, and politics have limited capacity for this lifesaving treatment. Strategies to respond to this have included regulations, guidelines, training, and short-term support programs. Despite this, capacity has not ever met demand. More GPs are prescribing ODT; the numbers speak to that, but unfortunately, not enough to ensure that ODT is available to all who need and want it. Most GPs who prescribe ODT are non-accredited and likely prescribe for a small number of patients, with only a small number of GPs prescribing ODT for large patient numbers (Penington Institute, 2023). This creates a fragile “knackered” system constantly at risk of collapse as high caseload GPs retire and cease prescribing (Kamerman, 2023). Without shifting the dial on funding, to address capacity and the complexity of ODT management in GP settings, these numbers are not likely to change.
The NSW ODT program has strongly linked the riskier medication, methadone, to the safer medication, buprenorphine, and emphatically decoupling these medications may be a benefit. Long-acting injectable buprenorphine may be more attractive to GP prescribers as they perceive more control over the use of a long-acting medication that is administered in a health setting and less risk of the medicine being used in unintended ways or given or sold to others (Wood, 2015).
The system is adversely impacted by low public funding for addiction medicine specialists, pharmacists, nursing, and allied health (Penington Institute, 2023). Increasing ODT prescribers to meet unmet needs requires long-term initiatives that build capacity and collaborative options for GPs, other primary health clinicians, specialists, and specialist services. GPs want specialist support (Wilson et al., 2022b), and to do this, the specialist system needs more capacity.
ODT medicines were made more affordable for patients in mid-2023, when the cost of dispensing ODT medicines was included for the first time in the Pharmaceutical Benefits Scheme (PBS), greatly decreasing medicine costs for people prescribed ODT, from $5–7 AUD a day to $7.30 AUD a month (Tsirtsakis, 2023). While this initiative may encourage more people to seek care, this increased medication funding does not fund prescribers. Access to buprenorphine, including the long-acting injectable formulation, may positively improve GP ODT engagement in the future. But without adequate funding for prescribers and the services that support them, any positive change is likely to be small.
The themes of lack of funding, lack of support, and lack of collaboration in poorly integrated siloed systems for a treatment that is seen as a high risk for a group of people highly stigmatized and “othered” are likely to be mirrored in other jurisdictions and services across Australia and the world.
A suite of long-term strategic options is needed to continue to build on current success with rigorous independent evaluation. These programs need to be codesigned by all prescribers, potential prescribers, service providers, and most importantly by people accessing or wishing to access ODT. While improving GP knowledge and skill is core, this is unlikely to have an impact unless policies and programs decrease red tape and administrative burden. They must address concerns regarding possible legal censure and perceptions of the risk of managing people in marginalized and stigmatized groups. They must address the complexity of care for people with this chronic condition. It is critical that funding bodies work together to adequately support the diverse healthcare environments that can provide this care, from specialist services to community generalists, to ensure that ODT, a highly evidence-based and lifesaving program, is available to all who could benefit from it.
Supplemental Material
sj-docx-1-cdx-10.1177_00914509241309109 - Supplemental material for “The Whole Structure Is Knackered, It Could Still Explode, It Really Could”: A Mixed Methods Study of Initiatives to Increase General Practitioner Prescribing in an Opioid Dependence Treatment Program from 1970 to 2022 in New South Wales, Australia
Supplemental material, sj-docx-1-cdx-10.1177_00914509241309109 for “The Whole Structure Is Knackered, It Could Still Explode, It Really Could”: A Mixed Methods Study of Initiatives to Increase General Practitioner Prescribing in an Opioid Dependence Treatment Program from 1970 to 2022 in New South Wales, Australia by Hester Wilson, Ben Harris Roxas, Nicholas Lintzeris and Mark Harris in Contemporary Drug Problems
Supplemental Material
sj-docx-2-cdx-10.1177_00914509241309109 - Supplemental material for “The Whole Structure Is Knackered, It Could Still Explode, It Really Could”: A Mixed Methods Study of Initiatives to Increase General Practitioner Prescribing in an Opioid Dependence Treatment Program from 1970 to 2022 in New South Wales, Australia
Supplemental material, sj-docx-2-cdx-10.1177_00914509241309109 for “The Whole Structure Is Knackered, It Could Still Explode, It Really Could”: A Mixed Methods Study of Initiatives to Increase General Practitioner Prescribing in an Opioid Dependence Treatment Program from 1970 to 2022 in New South Wales, Australia by Hester Wilson, Ben Harris Roxas, Nicholas Lintzeris and Mark Harris in Contemporary Drug Problems
Supplemental Material
sj-docx-3-cdx-10.1177_00914509241309109 - Supplemental material for “The Whole Structure Is Knackered, It Could Still Explode, It Really Could”: A Mixed Methods Study of Initiatives to Increase General Practitioner Prescribing in an Opioid Dependence Treatment Program from 1970 to 2022 in New South Wales, Australia
Supplemental material, sj-docx-3-cdx-10.1177_00914509241309109 for “The Whole Structure Is Knackered, It Could Still Explode, It Really Could”: A Mixed Methods Study of Initiatives to Increase General Practitioner Prescribing in an Opioid Dependence Treatment Program from 1970 to 2022 in New South Wales, Australia by Hester Wilson, Ben Harris Roxas, Nicholas Lintzeris and Mark Harris in Contemporary Drug Problems
Supplemental Material
sj-docx-4-cdx-10.1177_00914509241309109 - Supplemental material for “The Whole Structure Is Knackered, It Could Still Explode, It Really Could”: A Mixed Methods Study of Initiatives to Increase General Practitioner Prescribing in an Opioid Dependence Treatment Program from 1970 to 2022 in New South Wales, Australia
Supplemental material, sj-docx-4-cdx-10.1177_00914509241309109 for “The Whole Structure Is Knackered, It Could Still Explode, It Really Could”: A Mixed Methods Study of Initiatives to Increase General Practitioner Prescribing in an Opioid Dependence Treatment Program from 1970 to 2022 in New South Wales, Australia by Hester Wilson, Ben Harris Roxas, Nicholas Lintzeris and Mark Harris in Contemporary Drug Problems
Footnotes
List of Abbreviations
Acknowledgments
The authors acknowledge the semistructured interview participants who generously gave their time to participate in this research. HW acknowledges the support from the University of New South Wales for her PhD candidature.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.