
Abstract
Background
Stigma towards people who use drugs (PWUD) is a dangerous phenomenon with far-reaching effects. Research shows that parents play a powerful role in the shaping of their children's views of people with mental illness, but no similar research exists to investigate the shaping of views towards PWUD. This qualitative study explores dynamics of intergenerational reinforcement and disruption of stigma towards PWUD.
Methods
Semi-structured qualitative interviews were conducted with eight people split equally into two categories: 1) Participant-children: people between 18 and 30 and 2) Participant-parents: people of any age with experience as a parent of a child. Participants had some experience of using drugs or alcohol, but this was not a criterion for selection. Interviews elucidated the influence of parents’ views, opinions, narratives, discussions, and disclosures on views towards PWUD. Interviews included questions about stigma and its intergenerational development. Grounded theory was used to analyze the data.
Results
Three major themes in theory development were elicited for their role in the reinforcement and disruption of stigma towards PWUD: 1) conflation of drug use with other stigmatized characteristics; 2) the telling of stories around problematic drug use; and 3) the use of secrecy or disclosure of personal drug use.
Conclusion
The results of the study provide an understanding of the dynamics of stigma reinforcement and disruption. Each of the actions described in the themes can work towards either reinforcing or disrupting stigma.
Introduction
Stigma towards people who use drugs (PWUD) is a dangerous and potentially deadly phenomenon internationally (Fadanelli et al., 2020; Kulesza et al., 2013). Stigma is exercised by power and characterized by status loss, discrimination, and isolation that are encountered by people with certain characteristics, in this case, PWUD (Link & Phelan, 2001). Stigma towards PWUD is sometimes quite visible; it is also pernicious, preventing PWUD from accessing housing, social inclusion, formal healthcare, employment, and more (Baker et al., 2020; Corrigan et al., 2006; Kenny & Barrington, 2018; Lancaster et al., 2015; McCurry et al., 2022). Because stigma is diffuse, it is impossible to isolate a particular institution, structure or site as conducive to embedding stigmatized views; however, it is noteworthy that most studies on stigma towards PWUD do not focus on dynamics within families. Stigma towards PWUD has been shown to be of higher intensity than stigma towards fatness or mental illness (Barnwell, 2019; Barry et al., 2014; Flood-Grady & Kellas, 2018; Mueller et al., 2016; Phillips & Shaw, 2013; Wilkens & Foote, 2019). While there is extensive research to characterize and quantify stigma towards PWUD, research to understand its mechanisms and potential solutions is less developed (Baker et al., 2020; Corrigan et al., 2006; Farrugia et al., 2021; Fraser et al., 2017, 2020; Kagan et al., 2023; Kenny & Barrington, 2018; Lancaster et al., 2015; McCurry et al., 2022; Treloar et al., 2022). Research is urgently needed to understand the mechanisms through which stigma towards PWUD is reinforced or disrupted within families (Brener et al., 2024).
Allport (1979) identified parents as the most influential players in children's development of prejudice. The intergenerational transmission of stigma has been shown to play an important role in the prevalence of stigma towards people with mental illness (Chatard & Selimbegovic, 2008; Mueller et al., 2016). Our anecdotal experience led us to conduct this study, where we investigate how an intergenerational dynamic of stigma towards PWUD may operate.
We conducted a qualitative exploratory study using in-depth, semi-structured interviews. In the original study, we aimed to answer the following questions: 1) What mechanisms reinforce or disrupt stigma intergenerationally towards PWUD? 2) What interventions could disrupt the intergenerational reinforcement of stigma towards PWUD? 3) What tensions exist in the development of interventions to address the intergenerational reinforcement of stigma towards PWUD? While the original study included the co-design of interventions, in this paper we focus in detail on our first question about the mechanisms of reinforcement and disruption of intergenerational stigma. In the paper, we show how similar tropes, behaviors, and stereotypes are relied upon by parents to either reinforce or disrupt stigma when relating to their children. We also discuss some of the strategies actively used by some parents to challenge stigma, including selective disclosure and provision of evidence-based information.
Stigma Towards PWUD
Perhaps because of its encompassing nature, stigma has remained a popular concept to characterize the experiences of marginalized groups. Link and Phelan define stigma as “the co-occurrence of its components-labeling, stereotyping, separation, status loss, and discrimination-and…for stigmatization to occur, power must be exercised” (Link & Phelan, 2001, p. 363). Inspired by Link and Phelan, a fuller definition of stigma is provided by Bowen and Bungay (2016, p. 187) as “a socially constructed, context-specific experience of Othering that devalues one's identity, social contributions and potential in ways that limit how one can interact within one's world of socio-structural relationships. Stigma is a social process embedded in discourses and relations of power wherein dominant groups use it to select, impose and reinforce their ideals about the ways in which others are allowed to be in the world “. Stigma has widespread effects on the lives of PWUD, negatively impacting housing, healthcare, involvement in the criminal legal system, access to welfare, mental health, physical health, access to employment, and more. A study from the United States showed that stigma was associated with nearly two times the odds of experiencing a non-fatal overdose in the past year (Latkin et al., 2019). Room and colleagues described two bodies of literature that address stigma towards PWUD (Room, 2005). The first cluster look at stigma through a criminal lens and view it as social control that can effectively deter drug use; the second cohort observes this stigma by learning from the disability and mental health literature, perceiving it as a detrimental influence on PWUD. It is this second perspective that gained prominence in studies of stigma towards PWUD. A large subsequent body of work in critical drug studies has explored the dynamics and effects of stigma on PWUD (Farrugia et al., 2021; Fraser et al., 2017, 2020; Kagan et al., 2023; Treloar C. et al., 2022). However, this work does not particularly focus on internal family dynamics, but rather follows a more Foucauldian tradition of unpacking stigma dynamics within discourses (e.g., addiction) and medical institutions (e.g., treatment and the clinic). Some of this work draws on the twin concepts of biopolitics and biopower (e.g., Fraser et al., 2017; Treloar et al., 2022) to unpack the relationship between stigma and healthcare, particularly in terms of addiction and access to treatment technologies. Notwithstanding the contribution of this body of scholarship to our understanding of the dynamics of stigma, there are some blind spots, including the lack of focus on the family as a site where stigma is learnt but also challenged. In the discipline of social and developmental psychology, an extensive body of work has focused on the intergenerational transmission of stigma within families, particularly around the subjects of mental health stigma and obesity (though there is a broader literature on the dynamics of transmission of social and political attitudes). Due to the particularly entrenched moral opposition to substance use in society, much of the work on substance use stigma focuses on structural drivers and dynamics outside the family context. Perhaps, the family is a difficult site to access for research purposes. Still, it is valuable to engage with the family as a site where stigma can thrive, or be challenged, a focus that is lacking in stigma and PWUD related literature. Specifically, existing studies that focus on stigma and PWUD look at how families manage externally imposed stigma (e.g., Kenny & Barrington, 2018; Liahaugen Flensburg et al., 2023; O'Shay-Wallace, 2020) rather than internal family dynamics. While acknowledging the nuances and constraints intrinsic to employing these non-field specific perspectives for studying stigma against PWUD, we want to bring learning from this literature to bear on our understanding of the dynamics of stigma within families. We will summarize key takeaways from this body of literature in the below section.
Intergenerational Dynamics of Stigma
The seminal study that aims to describe the mechanisms through which the process of intergenerational transmission of stigma takes place is Gordon Allport's The Nature of Prejudice (Allport, 1979). Here, Allport describes two processes of socialization which occur simultaneously: first, children parrot the words and views of their parents, and second, parents create an atmosphere in which children can develop prejudice (Allport, 1979). Allport's descriptions of these mechanisms created a launching point for later work that aims to quantify this prejudice. Critiques of Allport have discussed his inadequate focus on structural features that affect interpersonal behaviors and interactions (Block, 2014). Perhaps, studies in the developmental psychology tradition privilege the family as a site of stigma transmission and reinforcement, to the detriment of other social institutions. Conversely, critical social research on stigma tends to sideline the family in favor of other structural forces (Degner & Dalege, 2013; Eckstein et al., 2018). We take Allport's work and associated critiques as a starting point for our study to characterize the mechanisms that drive the intergenerational reinforcement or disruption of stigma towards PWUD (Allport, 1979; Block, 2014; Dovidio et al., 2005; Pettigrew, 1979; Quillian, 2006). Psychology research frequently engages in discussion of the role of intergenerational transmission of negative views towards minority groups (Degner & Dalege, 2013). In much of this work, the terms stereotypes, views, prejudices, and stigma are used almost interchangeably. While the concepts are related, there are some important differences between prejudice and stigma, reflected in the dominance of either psychological or sociological explanations respectively.
Attitudes such as anti-fatness or negative views towards people with mental illness have been shown to transmit intergenerationally (Allport, 1979; Chatard & Selimbegovic, 2008; Holub et al., 2011; Mueller et al., 2016), but in keeping with the psychological tradition, most studies are based on survey and closed-experimental designs rather than narrative data and observations. Researchers in this field have mainly sought to quantify and spatialize the family socialization process whereby parents influence their children's views and values (Zagrean et al., 2022) of a particular group, such as ethnic minorities, and researching the direction of stigma transmission (Eckstein et al., 2018), the strength of the transmission (i.e., similarities of views between parent and child) (Degner & Dalege, 2013; Gniewosz & Noack, 2015), and whether stigma held by parents and children changes over time (Degner & Dalege, 2013). This body of research shows that there is intergenerational transmission of views towards stigmatized groups, but does not fully engage with the dynamics of stigma as qualitative explorations of the phenomenon.
In the mental health stigma transmission literature, following Flood-Grady and Kellas (Flood-Grady & Kellas, 2018, p. 607), “little is known about how families communicate and socialize younger members about MI (mental illness)”, but the stories heard and told within families are regarded as pivotal in shaping values, beliefs and attitudes. In a review of the literature on families stigma and mental illness, the key dynamics of communication about mental illness from parents to young children are summarized as follows by Mueller et al. (2016, p. 68): “Parents discuss mental health, but model taboo around mental illness”. Mueller and colleagues also found a dearth of literature focusing on what exactly is communicated to children about mental illness; in the available literature, they found that parents’ communication is implicit, scarce and contradictory. The dichotomy between mental wellbeing and mental illness is reinforced by parents through an ‘us versus them’ framing. Discussion of mental illness with children is characterized by avoidance and contradiction (e.g., through contrasting frames of empathy versus warning) (Corrigan et al., 2017; Flood-Grady and Kellas, 2018). Parents whose children use substances were found to incur judgments such as being enabling, being bad parents or dysfunctional (Wilkens & Foote, 2019). Family secrets, as a marker of stigma, are relied upon intergenerationally; these secrets often pertain to stigmatized activities such as mental illness, criminality, deviant sexualities or relationships (Barnwell, 2019). In this paper, we seek to address the following question: what mechanisms reinforce or disrupt stigma intergenerationally towards PWUD?
Methods
We targeted a purposive sample of eight participants above the age of 18 in the UK. We studied two categories of people: 1) young adults (age 18–30), to understand the perspectives of children; and 2) parents, to understand the perspectives of the people who are raising or have raised children. Within the definition of parent, we also included anyone who has cared for a child such as a foster parent or a grandparent. Our inclusion criteria for the study were:
Has lived in the UK for at least the past year; 18 or older; fits into at least one of two recruitment categories: (a) young adult (age 18–30) (“Participant-child”) or (b) previous or current caregiver (“Participant-parent”); and Agrees with the statement “stigma is an important public health issue”.
We included only people who had lived in the UK for the past year for the purpose of creating a sample of people who had some contextual understanding in common, although many of the people in the networks that we targeted for participation were not born in the UK or have not spent most of their lives in the UK. Criterion #4 is to ensure that we share common ground with participants for fruitful conversations, and that participants have an understanding about the importance of stigma in relation to public health. Some participants had experience of drug and alcohol use, but this was not a criterion for inclusion in the study. We utilized a poster for recruitment that included a brief description of the study, eligibility criteria, and a QR code link to a form where people could indicate their interest. We distributed the poster through professional networks via Twitter and email. Our professional networks are people who already have an interest in drug use, so the sample looks very different from the general population in the UK. Recruitment took place between June and August 2023. The first author conducted the semi-structured interviews, which lasted approximately one hour. The topic guide can be found in Appendix A. We used the first half of the interview to build a shared understanding of stigma towards PWUD and its harms, the potential development of this stigma in children, and the influence of parents and other institutions on stigma development in children. We used constructivist grounded theory as a data collection tool (Charmaz, 2013; Mills et al., 2006). Constructivism constitutes an epistemological stance positing the absence of an objective reality attainable through research. Instead, it asserts the existence of numerous individually constructed realities. We used grounded theory as an approach for data analysis in this investigation, because of the absence of current research delving into the examination of family stigma towards PWUD. We did, however, construct a shared understanding of stigma as a starting point during interviews. We began the interviews by discussing ideas around stigma towards PWUD, including examples for illustration when helpful. We continued to discuss theories of the development of stigma towards PWUD in children, also using examples when necessary. We then discussed sample-specific topics. With participant-children, we discussed the influence of their parents’ views on their views of PWUD. With participant-parents, we discussed the way that they parented children with respect to drug use and in relation to PWUD. Questions with both participant-children and participant-parents were designed to elicit an understanding of how stigma towards PWUD is reinforced or disrupted intergenerationally. Upon reflection, and in contrast to the psychological tradition, we decided to use the term reinforcement, rather than transmission, because we think it more accurately reflects the all-encompassing, non-linear nature of stigma and how it is expressed, overtly or latently, across domains and institutions.
We qualitatively coded our data using NVivo software starting at the very beginning of data collection for the purpose of constant comparison and the identification of outlier cases (Ezzy, 2002). We split the analysis of data that applied to theory development into first cycle coding, where data was categorized and extracted, and then second cycle coding, where data was interpreted analytically (Saldaña, 2016). In the first cycle codes we used vivo coding, for its ability to center the language of the participants and hold the researcher accountable to listening to the exact words being spoken and initial coding, for its ability to allow the researcher to code in an open-minded manner (Saldaña, 2016). We employed the second cycle coding technique of Focused Coding to discern and cluster prevalent themes (Saldaña, 2016). We present these common themes in the results section of this paper.
This study has been approved by the London School of Hygiene and Tropical Medicine Ethics Committee (reference #: 28537). We used all standard procedures to ensure that the study was conducted to ethical standards including attention to the anonymization, storage, and usage of data. There were some important ethical concerns that we addressed in conducting the study. First, there was a concern that we were recruiting participants from our own personal and professional networks. Most of our professional networks have previously engaged in or been adjacent to research and therefore we felt confident that they had the tools to feel comfortable electing not to participate. Second, the topic of our interview was on drugs and family experiences, which are personal and triggering topics. To ensure the safety of our participants during and after the interview, we allowed them to stop at any point or skip any questions that made them feel uncomfortable. We also provided a mental health and other resource sheet that offered options for participants to reach out for support after the interview. Finally, because the community of people who work in harm reduction and substance use in the UK is small, we did not share any demographic details of the participants in this paper, only whether they are a participant-child or participant-parent.
There are limitations to our study, beyond the obviously very small participant sample size, which significantly affect the applicability of our findings. As such, we are only making tentative and modest claims that will need further exploration. One limitation is that the parents and children of the sample are not related, so they cannot reflect on shared experiences from different perspectives. Another key limitation of this study was its convenience sample. Participants already understood stigma towards PWUD as an important public health issue and were considerably more knowledgeable about stigma towards PWUD compared to our expectations of average knowledge on these subjects among the general population. As such, we see our participants as experts, both in terms of their lived experience and familiarity with and understanding of the subject matter. Therefore, we do not expect that their views and experiences are in any way common. Yet, the fact that our participants are much less likely to hold stigmatizing views towards PWUD does not mean that their parents did not hold them and shared these views with them in turn. The authors have combined experience of volunteering in drug services for several years in the UK and US, and within these communities, there is a shared understanding that some of the stigmatizing views present in society are learned from parents and carers. In these contexts and between us, we often exchanged stories about our own parents’ stigmatizing views towards PWUD and our attempts at challenging their views, disrupting stigma through our combined academic and professional knowledge and our lived experience. As people who have worked around harm reduction and drug research, we share important characteristics with our participants such as similar professional backgrounds - particularly with the participant-children group, as neither of us has experience of parenting or caring for a child. The first author is a 25-year-old white cisgender woman from the United States who has lived in London for the past year. The second author is a 37-year-old white cisgender woman from Italy living in the UK for 20 years. We are embedded in the community of drug policy and harm reduction researchers, writers, and experts in the UK. We have also experienced stigma because of our own drug use. However, we have never experienced stigma as a result of some of the most stigmatized drug-use-related activities: seeking treatment for drug dependency, injecting drugs, or using highly stigmatized drugs daily.
Results
We conducted online video interviews with eight participants (four participant-parents and four participant-children). Three major themes in theory development were elicited for their role in the reinforcement and disruption of stigma towards PWUD: 1) conflating drug use with other stigmatized characteristics 2) the telling of stories of problematic drug use; 3) the employment by parents of selective secrecy or disclosure of personal drug use.
Conflating Drug Use with Other Stigmatized Characteristics
Participants shared several examples of what stigma looks like. Frequently, these examples involved the conflation of drug use with other stigmatized characteristics such as homelessness, criminality, abuse perpetration, or mental illness. Definitions of stigma towards PWUD were extremely similar between interviews. Both participant-parents and participant-children described this stigma to be about how people consider PWUD to be unclean, lazy, and less-than-human, aligning with common views as shown in the literature (Sumnall et al., 2023). One participant-child defined stigma as:
any type of interpersonal and/ or systemic belief that a certain group or quality or aspect of a person or group of people is bad, immoral, less than and therefore should be treated in the eyes of the law, the criminal justice system, and other societal institutions as inferior and shameful.
…about two weeks ago, [my mom] gets a WhatsApp scam, which is going round, which is the one that says, “hi mom- I'm messaging from my friend's phone because my phone's been smashed to pieces. I really need some money from you to replace it. Please call me.”
And after this event had happened:
…my 12 year old says, “grandma thought that some of the crackheads you work with had beaten you up and nicked your phone”
This participant-parent shared here what they felt was their mother's implicit association between PWUD, or crackheads as their mom pejoratively uses here, and people engaged with offending. Here, the grandmother used stigmatizing language, associating use of a heavily stigmatized substance (crack cocaine) with criminal behavior. It is interesting that there was no mention of crack cocaine in the message, and yet the thought association was immediate. Granted, this reaction was shaped by the context in which the participant-parent worked, though it can be gleaned that the participant-parent's mother (grandma) held stigmatized views about PWUD despite their daughter working with them.
One participant-child shared that in their family, there was an association between drug use and physical abuse because:
…the person in our family who has been addicted to the most drugs and has the highest level of drug use, he is also an abuser and he's my uncle…And he is just a really harmful person. He's caused so much harm in our family and so much abuse that has been pushed under the rug…And he is also a heavy user of opiates and alcohol. And so for the longest time, I associated those two things together. And my parents associate those two things together… And I think that their image of a drug user is him.
In this example, there is an association between drug use and being ‘an abuser’, so that when the image of a PWUD is conjured in this family context, drug use and being abusive appear together. This does not mean that the participant-child cannot question such an association through acquired knowledge and experience, though it might indicate that such a negative image was dominant and perhaps relied upon as an implicit warning - that “if you do drugs you will end up becoming an abuser like your uncle”. It is also interesting that the participant notes that the abuse ‘has been pushed under the rug’, which is reminiscent of the discussion about secrecy as a marker of stigma (Barnwell, 2019), and the struggles in families to address difficult, challenging conditions (e.g., mental illness, substance use, deviant sexual practices) and behaviors, so much so that they end up communicating in ways that are implicit, scarce and contradictory (Mueller et al., 2016).
Another stigmatized feature that was conflated with the status of PWUD was people who are unhoused. When asked about the visibility of drug use during their childhood, respondent-children frequently referred to unhoused people. One participant-child spoke about the ‘homeless drug user’ stereotype, sharing that:
…people do not look at or interact with people who are visibly homeless or unhoused on the street or give them money often because they think that they are using drugs or are going to use that money to buy drugs.
The assumption that people who are unhoused are also PWUD, and that their main motivation to ask for money is to buy drugs, is founded on a stereotype, while stigma informs many people's decision of not giving money for something that is considered an immoral choice (Krajewska-Kułak et al., 2016; Sumnall et al., 2021).
On the other hand, participant-parents frequently referred to people who are unhoused when asked about opportunities to disrupt stigma towards PWUD:
…if we go into the cities, you know…I'll chat to the sellers, give money to people who are begging, I'll ask if they know where the hostels are, if they know where to go for support. They hear me asking people, random strangers sat on the pavement if they've got Naloxone. So I think that kind of role models it.
Similarly, another participant-parent shared:
…my kid will put a hand in her pocket and give 10 pounds to somebody begging any fucking day of the week even if that's all she's got because she knows she's got somewhere to sleep when she gets home.
Here, the choice of participant-parents to engage with a stigmatized group and role-model non-stigmatizing behavior for their children appears as a promising way of disrupting stigma. In a study by Sumnall et al. (2021), the research team found that engaging with the life histories of PWUD leads to less stigmatizing public attitudes. This is in line with findings from literature in the mental health stigma transmission field, that humanizing and personalizing people with mental illness leads to less stigmatized views in children (Flood-Grady & Kellas, 2019).
As is shown in this section, both participant-children and participant-parents responded to the question of stigma towards PWUD with answers about stigma towards people who are unhoused. The same tropes are used by parents to either encourage stigmatization or challenge it. In this case, through the parent role-modeling, the child is enabled to challenge the stigma associated with people who are unhoused and use drugs.
The Telling of Stories of Problematic Drug Use
Many participant-children shared stories of people who had used drugs problematically or in a way that had been perceived to be problematic within their families. They shared how these stories had influenced their views of drugs and the people who use them. Some stories within families reinforced stigma. For example, one participant-child shared that in their family, there was a narrative about one of their uncles having experienced a psychotic break due to psychedelic use. They also shared that having gotten older and reflected on this, they felt that this was a false story of causation because “it seemed like actually lots of the things they were talking about and symptoms occurred much more prior to the drug use.” In early childhood, parents are often perceived as all-knowing, and their authoritativeness on any given subject is usually only questioned in hindsight. This participant shared that their parents enforced a narrative about psychedelics being particularly dangerous for mental health not explicitly, but implicitly. The implicit nature of stigmatizing narratives, as noted in the literature (Mueller et al., 2016), can lead to confused, contradictory ideas based on stereotypes rather than formed through explicit qualification and explanation, as might be expected in the context of less stigmatized subjects. On a similar note, another participant-child shared:
We have a lot of alcoholism in our family, and honestly, the way that that manifested in my parents was like, tons of moralization of drug use. And I learned that from a really, really early age.
Interestingly, participants indicated that stories of family members using drugs problematically can also normalize and destigmatize drug use and PWUD. One participant-child shared that because of family members who had struggled with alcohol use, their parents provided nonjudgmental and evidence-based information on the harms of overconsumption of alcohol. In this case, the parent's reaction to struggles with drug dependency in the family was to seek evidence and information to transmit to the child, rather than moralization. Here, it appears that the provision of evidence-based information can disrupt stigma, though such an approach may be more challenging for parents when discussing substances other than alcohol, which are more stigmatized due to their illicit status and position in the drug hierarchy.
The Use of Secrecy or Disclosure of Personal Drug Use
The relationship between stigma and secrecy is well documented, with secrecy acting as a marker of stigma within families (Barnwell, 2019). Literature on mental health stigma indicates that disclosure of personal experience of mental illness within families helps to humanize and destigmatize mental illness (Flood-Grady & Kellas, 2018). There has also been a debate about whether disclosure of personal drug use is impeded by stigma (Kiepek & Beagan, 2018) and if disclosure can in fact disrupt stigma (Ross et al., 2020; Walker, 2021; Zampini et al., 2021).
During interviews, participant-children expressed anxieties around the sharing of drug consumption stories with their peers. One participant-child said that they “would've felt uncomfortable for them [peers] judging me.” Another participant-child shared that they were worried about potential dangers and vulnerability associated with non-disclosure of drug use as isolating. They said about people in their life:
they won't tell their flatmates they're using a particular type of drug or they won't tell their parents, or they won't tell even […] their really close friends because that's like a secret and they're worried about being stigmatized or ashamed, I guess.
[lying to our kids about our personal drug use] was one thing that we decided in our house we weren't ever gonna do…being honest to your kids should not be seen as being radical.
Participant-parents thought that not being open with children, or even lying to them, was disingenuous:
…every generation thinks that they invented cannabis because their parents don't necessarily talk to them about the fact that they did cannabis growing up and probably still do.
Another participant-parent shared a concern that their co-parent might lie about their drug consumption if asked. The same participant-parent shared that they felt that disclosure must be contextualized to protect children from harmful experiences:
I think that honesty is important, but I think it's gotta be contextualized because I think, you know, there is that wider influence like music. They're really into nineties music and rave stuff and nineties type music, which obviously was completely tied in with the drug scene. And, you know, they talk really flippantly about cocaine.
Participant-children shared that they were not cognizant about their parents’ drug experiences because parents were not open about this with them, unless they considered their former use to be problematic, in which case they were more likely to share it in order to set an example or as a cautionary tale. This is in line with a culture that is accepting of people being open about past drug use, particularly if propped up by a recovery and abstinence narrative of redemption, rather than current drug use (Wakeman, 2014; Zampini et al., 2021). When participants were asked why they think their parents chose not to disclose their drug use, several participant-children felt that the topic would make their parents uncomfortable. This making-uncomfortable, as a product of stigma, was regarded as something to be avoided. One participant-child shared about their dad:
I think he'd be uncomfortable talking about certain types of drug use. Like, very uncomfortable about it. And he would, He wouldn't, I don't think he would engage in the conversation.
The experiences of participant-children here indicate that stigma prevented honest conversations between them and both their parents and peers. On the other hand, some parents in the sample are actively employing strategies of selective and contextualized disclosure which has the potential to disrupt stigma and promote harm reduction.
Discussion
In our several years’ experience of volunteering within drug treatment and harm reduction services and studying drug policy, we have seen repeatedly the harms of stigma towards PWUD. Stigma is so often what prevents people from accessing services or utilizing basic harm reduction techniques that can keep them alive and well, such as not using drugs alone, or accessing naloxone. Research has shown that parents can transmit stigma to their children, but there has been no research to answer the question of how this stigma, particularly towards PWUD, is reinforced or disrupted. Using a grounded theory approach to data analysis, we identified three main mechanisms through which stigma is reinforced or disrupted intergenerationally. Our data showed that PWUD are often associated with other stigmatized groups such as people engaging with criminal activities or people who are unhoused. This conflation can then be wielded as a tool to stigmatize PWUD. At the same time, this conflation was also used to humanize and help people who are unhoused and use drugs. Due to their visibility, caregivers can use this as an opportunity to role model compassion and empathy towards people who are marginalized in front of their children. Thus, children can learn to either stigmatize or be compassionate from their parents through the very same associations.
Stories of problematic drug use were used in two ways. First, by caregivers, either on purpose or by accident, to instill fear, caution and warning in children and encourage them not to use drugs, to fear drugs, and to fear PWUD. At the same time, these stories were also used as a starting point to enable the sharing of practical, evidence-based information about substances, disrupting stigma. Most participants in the study were characterized as choosing to keep their personal drug use secret, under the guise of their discomfort talking about drugs. While parents remain the main source of information about drugs for their children in the UK, closely followed by teachers (NHS, 2022), children often lack good, evidence-based information about drugs or the people who use them and are left to figure out this information on their own. To address this, some participant-parents provided evidence-based information (though this only happened with reference to alcohol), or they employed selective and contextualized disclosure of personal drug use to the end of normalizing and destigmatizing it. If secrecy is a marker of stigma, then disclosure, or the personalizing and humanizing of stigmatized identities, works to disrupt stigma (Barnwell, 2019; Flood-Grady & Kellas, 2018).Yet, disclosure may be especially difficult for parents with drug dependence due to the fact that their drug use is particularly stigmatized (Barnard & Barlow, 2003; Rhodes et al., 2010).
Due to the sample's limitations in terms of its size and characteristics, including the lack of shared experiences among the parents and “children” in the sample, and the very specific group of people who participated to the study being professional and professional-adjacent in the drugs field, our findings are tentative and should be expanded upon and corroborated through further research. We believe it would be particularly interesting to investigate how stigma is reinforced or disrupted within families with shared experiences, what mechanisms external to the family enable children to question their parents’ views, and also whether and to what extent grown up children are able to disrupt and challenge their own parents’ views.
Conclusion
This study provides an understanding of the dynamics of stigma reinforcement and disruption towards people who use drugs within families. The same tropes are used by parents to either encourage stigmatization or challenge it. In our study, stereotypes appear as culturally shared starting points used by parents to role model. They are either unquestioned, cautionary tales acting as a warning, or purposefully challenged. In this way, stigma is either reinforced or disrupted. As a small-scale qualitative exploration with expert participants who hold a critical view of stigma towards PWUD, this study has obvious limitations. For example, it is hard to ascertain whether, in a less expert sample, participant-children may have been more likely to continue holding stigmatized views into adulthood. Yet it provides crucial insight on disruption mechanisms that may have otherwise been less apparent in a less expert sample. Understanding the mechanisms through which stigma towards PWUD is passed or challenged intergenerationally opens new avenues for further research, but also for the design of targeted interventions. There is mounting evidence of the deleterious role that stigma plays on the lives of people who use drugs. It is perhaps time to edge towards a more action-oriented research agenda that moves beyond acknowledging and evidencing the stigma, to intercept and directly challenge its pernicious mechanisms. We want to draw attention to two key implications of our findings which inform a research agenda that works towards co-creating interventions to challenge stigma with affected communities, including families, beyond traditional public health settings. These could include principles and guidelines that directly address schools and families, two core institutions in the development of children's views. We also suggest that if selective, careful and contextualized disclosure that humanizes PWUD is shown to be effective in disrupting stigma within families, as it has been for mental health, then such disclosure becomes part of a strategy for responsible parenting.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Appendix
Topic Guide.
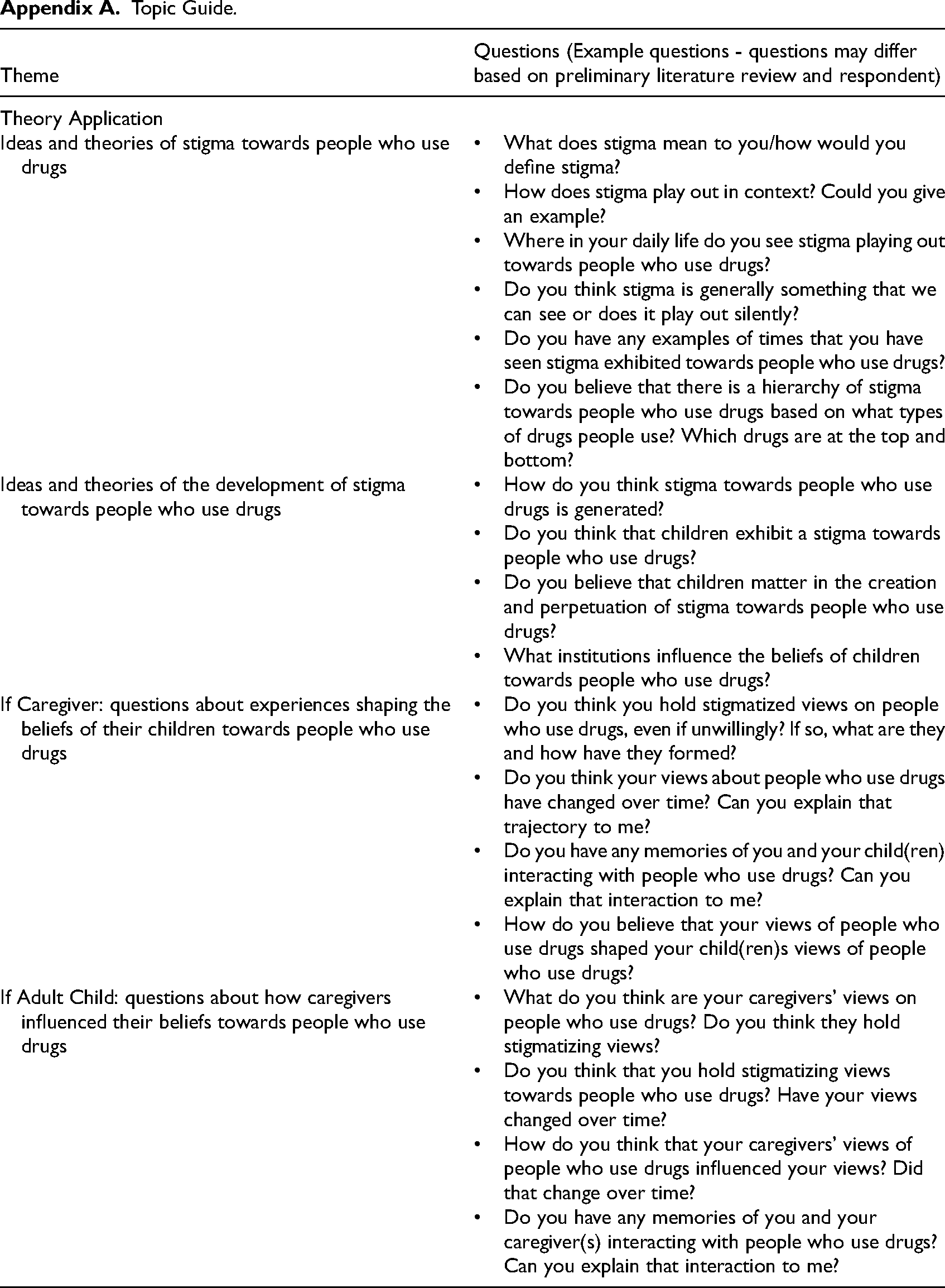
| Theme | Questions (Example questions - questions may differ based on preliminary literature review and respondent) |
|---|---|
| Theory Application | |
| Ideas and theories of stigma towards people who use drugs |
What does stigma mean to you/how would you define stigma? How does stigma play out in context? Could you give an example? Where in your daily life do you see stigma playing out towards people who use drugs? Do you think stigma is generally something that we can see or does it play out silently? Do you have any examples of times that you have seen stigma exhibited towards people who use drugs? Do you believe that there is a hierarchy of stigma towards people who use drugs based on what types of drugs people use? Which drugs are at the top and bottom? |
| Ideas and theories of the development of stigma towards people who use drugs |
How do you think stigma towards people who use drugs is generated? Do you think that children exhibit a stigma towards people who use drugs? Do you believe that children matter in the creation and perpetuation of stigma towards people who use drugs? What institutions influence the beliefs of children towards people who use drugs? |
| If Caregiver: questions about experiences shaping the beliefs of their children towards people who use drugs |
Do you think you hold stigmatized views on people who use drugs, even if unwillingly? If so, what are they and how have they formed? Do you think your views about people who use drugs have changed over time? Can you explain that trajectory to me? Do you have any memories of you and your child(ren) interacting with people who use drugs? Can you explain that interaction to me? How do you believe that your views of people who use drugs shaped your child(ren)s views of people who use drugs? |
| If Adult Child: questions about how caregivers influenced their beliefs towards people who use drugs |
What do you think are your caregivers’ views on people who use drugs? Do you think they hold stigmatizing views? Do you think that you hold stigmatizing views towards people who use drugs? Have your views changed over time? How do you think that your caregivers’ views of people who use drugs influenced your views? Did that change over time? Do you have any memories of you and your caregiver(s) interacting with people who use drugs? Can you explain that interaction to me? |