
Abstract
Drug checking services (DCS) allow people who use drugs to submit substances of concern for chemical analysis and then provide results and specialized counselling when needed. DCS intersect risk management, from a public health perspective, with an activist take that provides people who use drugs with agency over their use by helping them detect and avoid unwanted substances. This paper presents data from an exploratory study of people's motivations for using the Boom Festival DCS and the meanings attributed to their interactions with the service. Semi-structured interviews (n = 22; mean age 29 years, range 24–43; 68% cisgender men) were conducted, and an inductive approach was applied informed by Iterative Categorization and reflexive thematic analysis. Participant narratives were organized around three themes: “Drug Checking as a Responsible Practice”, “Drug Checking as a Care Practice,” and “Drug Checking as a (Mis)trust Practice”. Through these themes, the analysis focuses on the concepts of risk and the ideals of responsibility, care and trust among people using the DCS. Our findings expand the current literature that demonstrates the usefulness of DCS as an intervention to mitigate individual risks of drug use by demonstrating the more communitarian potential of this type of intervention as a means to expand the social networks of people who use drugs and support a “culture of care” among partygoers. Our participants relied on friends and trusted suppliers to get information about drugs and make informed decisions. Hence, there is a potential for those involved in drug use and supply to actively participate in harm reduction services, particularly DCS, as a way to disseminate information to a broader audience that does not want or cannot access the service.
Introduction
The emergence and consolidation of harm reduction responses in Western postmodern societies can be seen as a symptom of broader global transformations within new ways of managing human conduct in what Beck (1992) named “Risk Societies.” Risk has become a fundamental feature of everyday life, and its management is a considerable part of the mission of governments, civil society institutions and individuals (Lupton, 2006). Harm reduction services actively work to promote the management of risks but simultaneously propose a non-judgmental approach to drug use. One key aspect of harm reduction is its dedication to offering practical care, education, and health services without discrimination based on categories of deviance and pathology. This approach ensures all groups are included in public care and responsibility (Race, 2008). The implementation of harm reduction responses echoes this collective commitment based on notions of reciprocity and connection, grounded in the premise that people should be met where they are and their knowledge and experience should be valued (Marlatt, 1996). Different research has highlighted the feelings of solidarity and care among people who use drugs in different settings (Kavanaugh & Anderson, 2008; Kolla & Strike, 2020; Malbon, 2002; Van Havere et al., 2015), even in highly vulnerable social and economic conditions (Friedman et al., 2007). Solidarity works as a set of “shared practices reflecting a collective commitment to carry ‘costs’ (financial, social, emotional or otherwise) of human action” (Prainsack & Buyx, 2012, pp. 46–47).
The first harm reduction responses were born from collective action based on bottom-up strategies shared between certain groups historically oppressed by mainstream society, like activists from the LGBTQI + community or people who use drugs (Friedman et al., 2007). These groups designed their approaches to resist mainstream society's efforts to promote their “normalization” or disappearance (Race, 2008). Nevertheless, the successful implementation of these practices in the control of epidemics such as HIV / AIDS, as well as the fact that drug use has become a more pervasive issue for society, has led to harm reduction programmes to be implemented by government agencies and NGOs mainly as a complement to other socio-sanitary approaches to the use of drugs and sexual behaviors (Fernandes et al., 2006). This dissemination of harm reduction practices as a privileged public health strategy impacted its original nature and objectives, eventually rethinking its alternative and activist nature (Barratt et al., 2014; Roe, 2005).
The recent theory and practice of harm reduction have been building a particular drug-using subject: a conscious person with health literacy, capable of making rational decisions, self-determination and self-regulation. This category of people who use drugs is widely described in the literature as people for whom the use of certain drugs is a relatively regular and integrated feature within their life experiences (Duff, 2003; Parker, 2002, 2003) and are aware of the risks involved in their drug use (Gamma et al., 2005). They actively seek information about harm reduction strategies and employ a variety of behaviors to minimize the risks of their drug use (Baggott, 2002; Cruz, 2015; Measham et al., 2001; Valente et al., 2022a, 2022b). In fact, “most people who use drugs engage in drug use with an understanding that they are managing the interplay between the positive effects of a drug (pleasure maximization) and the risks associated with administering or taking a drug (harm reduction)” (Southwell, 2010, p. 101). Southwell (2010) conceptualizes these people who use drugs as “calculated risk takers.” While subjected to the moral principles of mainstream society regarding the reduction of risks from drug use, the “calculated risk takers” do so in a way that fits their objectives and choose the practices that better adjust to their life choices, being active in constructing, disseminating and applying care practices in their communities (Race, 2008).
Race (2008, 2009) goes beyond the terminology of harm reduction, using the concept of “counterpublic health” to describe these types of strategies put into practice by people who use drugs with the aim not only to minimize the potential risks of drug use but to increase the pleasure and well-being that drugs can bring to one's life. “Counterpublic health” is generally based on peer interventions and interactions built upon an embodied ethics that assumes that the drug-using subject seeks pleasure. The experience of pleasure serves as a conduit for the development of specific collective safety protocols, challenging the prevailing idea that placing importance on pleasure in drug-related activities conflicts with self-regulation and safety (Race, 2009). The notion of “counterpublic health” has several practical implications for prevention and harm reduction interventions. Most services available to people who use drugs are based on the essential principles of public health and have health promotion as the ultimate ideal (Hathaway, 2001; Lupton, 1995). Yet, these health-oriented discourses do not fit everyone, particularly because people consider several other factors besides health when deciding to use drugs, with pleasure one of the most relevant ones (Barratt et al., 2014).
Transformational festivals can operate as sites of resistance to dominant discourses (i.e., sites where “counterpublic health” may be operating), like the ones that emanate from public health interventions that usually depict drug use as inherently problematic. People who use drugs in these contexts might develop a resistance to strictly health-oriented discourses that are frequently associated with conformity to dominant values (Crossley, 2002). Different qualitative studies of people who use drugs have described such feelings of resentment toward the negative depictions of people who use drugs (Duff, 2008; Fox, 2002; Harling, 2007).
Drug Checking Services as a Harm Reduction Tool
From the moment the first prohibitionist movements were set in motion, one of the most relevant issues people who use drugs had to deal with was the high level of adulteration and substitution affecting the informal drug markets (Brown & Malone, 1973; Marshman & Gibbins, 1969). From the 1960s onward, universities and civil society organizations began offering drug checking services (DCS) (also known as pill testing) (as reviewed in Valente & Martins, 2019), allowing people who use drugs to submit psychoactive drug samples for chemical analysis and provide individualized feedback on results and specialized counselling when needed (Barratt et al., 2018).
DCS intersects risk management with an activist take, providing people who use drugs with agency over their use by helping them detect and avoid unwanted substances. Although the fast development of more advanced tools to perform drug analysis comes from the considerable investment made by governments worldwide in reducing supply, harm reduction collectives have appropriated these technologies and used them as “resistance practices to beat the system” (Campbell, 2021) and increase the agency and empowerment of people who use drugs. Analysing drugs illustrates a tension between preventing potential harm from drug use (when harm reduction services perform it) and avoiding drug use (when law enforcement agencies perform it) (Campbell, 2021). The knowledge produced via drug analysis by law enforcement and harm reduction collectives might be similar. However, its use and impact on people's lives differ significantly.
Recently, the number of DCS implemented for harm reduction purposes has been rising worldwide (Barratt et al., 2018; Giulini et al., 2023; Maghsoudi et al., 2022; Park et al., 2023) with different objectives. In Europe, DCS have been the cornerstone of harm reduction responses in party settings since the 1990s (Kriener et al., 2001). However, dramatic situations like the “overdose crisis” in North America (Suzuki & El-Haddad, 2017) have prompted a considerable number of DCS to be established as an emergency public health response in contexts like drug consumption rooms, community centers, hospitals and focusing on population segments living in situations of social and economic vulnerability (Park et al., 2023).
With the proliferation in the number of DCS worldwide, research in this field has also increased (Brunt, 2017; Giulini et al., 2023; Maghsoudi et al., 2022; Palamar et al., 2021), providing evidence of the impact of such services on the intentions (Benschop et al., 2002; Martins et al., 2017; Measham, 2019; Michelow et al., 2015; Olsen et al., 2022; Saleemi et al., 2017; Sage & Michelow, 2016; Valente et al., 2019) and behaviors of people who use drugs in recreational settings (Measham & Turnbull, 2021; Valente et al., 2022a). The studies focusing on the impact of drug checking on people's behavioral intentions and behaviors show that most people using drug checking services in festival and party settings report not using a substance when the result of the analysis is unexpected. Recently, Valente et al. (2022a) presented data collected at a large-scale music festival testing the validity of behavioral intention measures against reports of actual behavior and the adoption of harm reduction strategies by people using the DCS service at the festival. The results from this research supported the hypothesis that DCS promote the adoption of safer drug use practices. Also, a follow-up study of different behavioral outcomes after visits to a DCS was reported recently by Measham and Turnbull (2021). The results of this study were positive, with more than 50% of research participants destroying or disposing of substances other than expected, reinforcing findings that suggest that DCS can prevent the ingestion of unexpected and/or adulterated substances.
The available evidence also shows that people using DCS in party settings do not differ considerably from other partygoers, mainly white middle-class males with high educational levels who tend to use more drugs than the general population and engage in several harm-reduction practices. (Koning et al., 2021; Martins et al., 2017; Measham, 2019; Measham & Simmons, 2022; Valente et al., 2022a, 2022b). The study from Measham and Simmons (2022) which took place at several summer festivals in 2018 in the UK showed that partygoers using the DCS were significantly more likely to be younger, male and past month polydrug users with a wider range of drugs consumed in the last month compared with the general festival population. Valente et al. (2022b) compared a group of testers and non-testers at the Boom festival, and results showed that testers tended to adopt harm reduction strategies more frequently than non-testers. This data suggests that DCS are reaching a particular set of knowledgeable and responsible people, “well-adjusted and successful goal-oriented, non-risk taking young persons, who see drug taking as part of their repertoire of life” (Parker, 1997, p. 25). However, the focus on the effectiveness and utility of DCS has been measured almost exclusively by its impact on individual behaviors (Davis et al., 2022; Wallace et al., 2022). At the same time, the collective and communitarian meanings of DCS remain largely unexplored, as well as the importance of social ties and interactions for acquiring particular competencies vital to maintaining health and well-being (Fagg et al., 2008; Duff, 2009). To improve DCS access, it is crucial to understand what motivates people to have their drugs checked, their interaction with the services and how the information DCS provides is integrated into their drug-using practices.
Context
In 2001, Portugal moved forward with a pioneering legislative change, commonly known as the “Portuguese Decriminalization Model,” which changed the paradigm of intervention in the drugs field in Portugal (Greenwald, 2009; Hughes & Stevens, 2007). Possession and consumption of drugs are no longer crimes but administrative offences as long as the amount of illicit substances seized does not exceed the average dose for ten days of consumption.
At the same time, intervention responses in the area of drugs were reinforced via the Law Decree No. 183/2001 of 21 June of the Council of Ministers (2001), which recognized “the importance of developing programs and measures that contribute to the reduction of risks and minimization of harms from drug consumption and regulated various programs and socio-health structures” (p. 3594). This decree legally framed the possibility “on an experimental basis, that contact and information points (a type of harm reduction structure) may exceptionally be authorized to provide adequate information on the composition and effects of drugs, particularly new synthetic drugs (…)” being able, for this purpose, “to be equipped with instruments destined to test the composition and the effects of drugs” (p. 3597).
In 2002, soon after the drug decriminalization took place in Portugal, the Boom Festival, one of the world's most prominent cultural and musical psychedelic events, which takes place in Portugal every two years, introduced a small drug information booth at the festival (Carvalho et al., 2019). Since then, the festival's investment in caring spaces has increased consistently. In 2006, drug checking was available at the festival for the first time. In 2008, the festival created Kosmicare, a specific area of the festival to care for people undergoing difficult psychological experiences, usually related to psychoactive substances (Carvalho et al., 2015). Kosmicare's evolution into a full-spectrum harm reduction service has gradually happened at each festival edition through partnerships with the Portuguese Government, various NGOs, EU-funded projects, and universities. In 2016, Kosmicare became an NGO expanding its activities outside the festival grounds.
In the 2018 edition, Kosmicare provided a complete harm reduction structure approved by the General Directorate for Intervention on Addictive Behaviors and Dependencies, providing different Harm Reduction Services: specific information on drugs and sexuality, counselling and harm reduction materials to promote the well-being of the Boom Festival patrons, in particular those who use drugs, and a chillout space to welcome those who need to rest. Kosmicare also offers an analytical service coupled with a short motivational intervention aimed at promoting people's reflection on drug use and market adulteration (Valente et al., 2022a). This service allowed the timely detection of adulterated and/or toxic compounds that may endanger the health of the Boom Festival patrons (Kosmicare, 2018). In addition to these services, Kosmicare created a Psychedelic Emergency Hub, where people undergoing difficult psychological experiences, drug-related or not, could find specialized help (Carvalho et al., 2019).
Aims
This paper presents data from an exploratory study performed to collect data grounded in people's experiences and voices regarding their motivations to use Kosmicare's DCS and the meanings they attribute to their interaction with the service. The quantitative data presented and analysed here were collected as part of a more extensive longitudinal study on the impact of the Boom Festival 2018 DCS on the behavioral outcomes of the people who use the service (Valente et al., 2022a). Testers were invited to participate in the three empirical phases of the research project: while at the festival, six months after through an online survey, and a semi-structured interview a year after the festival. This paper will focus exclusively on data collected via semi-structured interviews, which were included to understand the personal meanings attributed to the DCS by those who use it, particularly their motivation to have their drugs chemically analysed.
Methods
Procedure
Invitations to participate in the study were sent to everyone who used Kosmicare's DCS and agreed to share their email address to be contacted for an interview (N = 75). More information about sampling methods for the broader project can be found elsewhere (Valente et al., 2022a, 2022b). These participants were contacted via email twelve months after the festival and seven months after the online follow-up. Due to several delays related to COVID-19 social restrictions and work limitations, the interviews only took place between February 2020 and May 2020. The first author conducted the interviews via Zoom, an online platform. Interviews were scheduled via email, and twenty-five people accepted to participate to reflect on their practices, experiences and attitudes regarding Kosmicare's DCS. Three people did not appear at the scheduled time for the interview and have not engaged in any further contact. Twenty-two interviews were completed, with an average duration of 75 min, all taking more than 60 min and less than 90.
The interview only took place after the informed consent and the authorization to audio-record it. The possibility of not turning the camera on was offered, but all the participants decided to turn it on. A semi-structured script was used to collect primarily open-ended qualitative data on the respondents’ involvement with the Boom festival, drug use history and background, experience with harm reduction, and drug checking services with a particular focus on Kosmicare's DCS offered at the Boom Festival 2018 edition. At the end of the interview, a concise questionnaire was used to collect participants’ sociodemographic characteristics. This research received approval from the Ethics Committee of the Faculty of Psychology and Education Sciences of Porto University.
Data Analysis
All interviews were audio-recorded and transcribed verbatim. Seventeen interviews were recorded and transcribed in English, and five were recorded and transcribed in Portuguese and posteriorly translated to English. The first author performed all the interviews, transcriptions, and translations which the second author and the fifth author revised. The first and fifth authors are native Portuguese speakers and fluent English speakers, and the second author is a native English speaker. In accordance with Twinn (1997), we have proceeded to use only one translator to maximize the reliability of the data. This is particularly relevant in this research because the first author was present during all stages of the research process. The first author is also very familiar with the cultural context of the Boom Festival and its patrons and can be considered a peer in these contexts, having attended every festival edition since 2006. This follows recommendations that mention the importance of recruiting local community members to participate in the translation process to comprehend better how the language is tied to specific cultural and social contexts (Temple, 2006). The translation process was performed to respect textual, semantic and content equivalence.
An inductive approach was applied to the data informed by Iterative Categorization (Neale, 2016) and reflexive thematic analysis (Braun & Clarke, 2006, 2023). We followed Iterative Categorization procedures from coding to descriptive analysis as a method of familiarization and systematization of the data. We followed the six analysis phases proposed by Braun and Clarke (2006, 2023). For the complete data analysis, we deductively developed an initial coding frame according to our interview script, which was created based on our research questions and the data derived from the quantitative research. However, the sub-analysis described in this paper refers to specific reports that emerged through the coding in an inductive way.
The coding frame was discussed and approved by Authors 1,2,3 and 4 and evolved throughout the coding process. All transcriptions were read and reread to ensure familiarization with their content. Coding involved reviewing all data, line by line, identifying key issues (codes) and then attaching segments of the original text. We coded all the interviews manually using paper cards and Microsoft Word documents. After the first coding and the summary of key ideas, the material was reviewed several times, grouping similar ideas and reviewing and re-grouping ideas after each code was analysed (Neale, 2016). Finally, we collated all summary files to review the summarized data and allow connections across different codes.
Of the several themes identified during the analysis process, this paper focuses on motivations to use DCS, interaction with service and drug-using identity. We have used expressions that spontaneously emerged from the participants’ discourses to organize and report the data.
Results
The results of this paper will focus on three main themes that emerged from participants’ narratives: a) “Drug Checking as Responsible Practice,” b)“Drug Checking as a Care Practice,” and c) “Drug Checking as a (Mis)trust Practice.” Participants have explored these ideas while signifying their relationship with the DCS and their motivation to have their drugs tested.
Participants
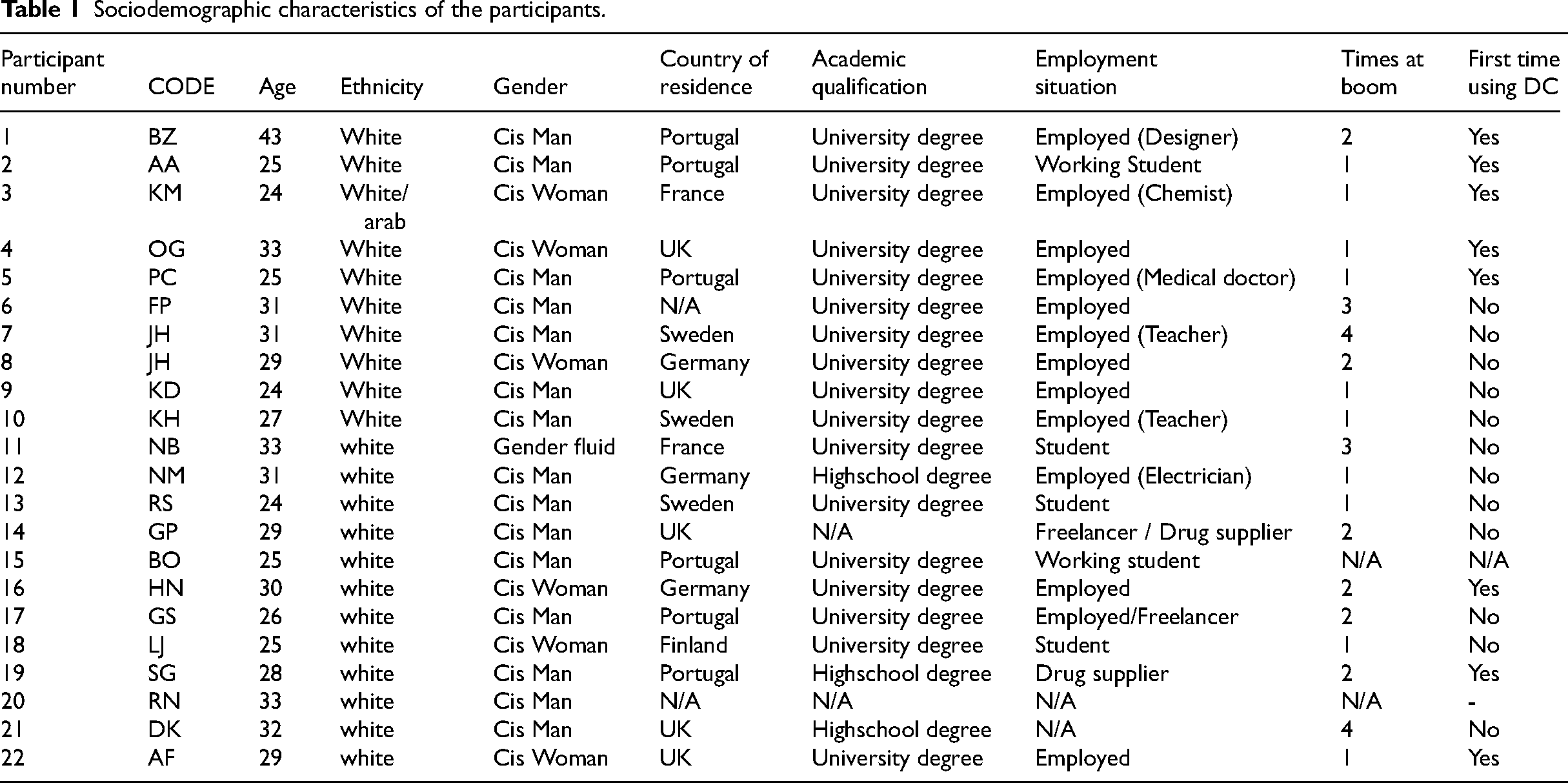
Twenty-two people who used the DCS participated in this study, ages 24 to 43 years old, with a mean age of 29. Fifteen people identified as cisgender men and six as cisgender women; only one person identified as gender fluid. All the participants identified as white Europeans. Seventeen reported having a university degree, three stated they had a high school education, and two did not reveal that information. All the participants were employed, and only two reported engaging in drug-selling activities. Twelve people had tested their drugs before the Boom 2018, and ten were using a DCS for the first time. [Table 1]
Sociodemographic characteristics of the participants.
The data from the interviews corroborates the findings from previous quantitative studies (Valente et al., 2022a, 2022b), showing that people using Kosmicare's DCS report using a wide variety of substances. All the participants reported beginning their drug-using careers with alcohol and cannabis. Most of them (n = 18) began using alcohol and cannabis in their early teens and, later started using other psychoactive substances, particularly psychedelics and stimulants, in recreational settings: The first time I did pot (cannabis), I thought it was when I was 14 because I just wanted to try. Then, I did molly (MDMA), when I was maybe 15 or 16, and I tried a bunch of things, like coke, speed … I have never been interested in ketamine or these kinds of things because I don’t like what I hear from it, and that's all. And then I tried a bunch, and I was like Okay, I’m done. I’m tired of partying every weekend. That's why I’m young, but I don’t party anymore because I started young, so then I’m like, yeah, partied a lot. I’m 24, I don’t want to party anymore. I’m tired. (KM) I’ve started early, yeah. It's not legal, but I think I was about 15 when I first smoked cannabis and then, and 18 I first took LSD, and then I moved to London when I was 18 to study and there, it was until my early twenties. Uh, yeah, again, just the classics, basically ketamine, LSD, MDMA. (KD)
Drug Checking as a Responsible Practice
The idea of responsible use is an important part of our respondents’ drug-using identity and self-representation as a person who uses drugs. The results showed that although our participants spoke freely about their drug use as one of the life choices they enact according to their will and personal goals, an internalized idea of responsibility and control cut across their narratives about themselves. They perceived themselves as experienced, knowledgeable and careful about their drug use: I'm experienced, you know, I've done a lot of it, and I also know a lot about it. So, there's hardly anything I don’t know. (BZ) I would call myself a psychedelic veteran. I’ve seen a lot of shit. (NM) What they [kosmicare workers] told me about harm reduction I already knew. My master thesis is about that […] opioids. I search a lot about harm reduction. I didn’t become interested in drugs because I am a doctor, I became a doctor because I was interested in drugs. (PC) I am an experienced user, but I’ve always been cautious. (FP) We are quite knowledgeable because we are a little nerdy. I like to know what I put in my body. I would say I’m pretty educated. I know the substances I use. I don’t take things I don’t know. (LG)
All of our participants spoke about becoming more responsible in their drug use and more selective with the substances consumed as they transitioned to adulthood: As I’ve gotten older, I’ve realized there's more chance of me having a good experience if I choose the safer setting and maybe the parties, or festivals, aren’t always the right settings. (KD) I think it has just kind of naturally happened over time, getting older perhaps, and also getting better at making the sensible decisions and realizing that when I'm at a party, I can have a great time with, or without drugs, but maybe if I take them, there's a higher risk that maybe I won't have a good time, even with psychedelics. (RS) My relationship has changed very much in the last five years, that I'm much warier of dose and I don't go to so many parties really. So I'm, I have a more sort of, hum, psychonautic relationship to substances at the moment. (DK)
These findings are consistent with research that shows that during that transition period, alcohol and drug use decreases (Parra et al., 2003; White et al., 2005). Most adolescents who use drugs mature as they move into adulthood and transition to role responsibilities such as marriage, parenthood, and career establishment (Bachman et al., 2014; Measham et al., 2011). Our respondents referred to age as a relevant factor in changing their drug use patterns and motivations. The separation between their work, family and party life was also present in the discourse of several respondents: I don’t speak with my family about this. My family thinks all drugs are bad. (FP) If someone could see me or recognize me because of the profession that I work in, I think it would be very dangerous in terms of my career. (OG) I think age was a plus, you know, my drug use had to change … I have children with two different women and with one of them I went through court battles and stuff, you know, and it was a lengthy court battle for custody and care of children… (BZ)
Sixteen participants also described a change in their motivations for using drugs over time. They described moving from strictly fun, pleasurable and socializing practices to experiences of personal growth and spiritual development: Psychedelics gave me a way to change my perception of reality, and when I got off from this experience, I realized that it changed my way of considering my realities, and it was really helpful in my relationship with a lot of people. I decided to become a vegetarian and to be more, aware of the world where I am living and through the experimentation of this crazy large, you know, round world … you know, after my first experience with LSD, I had this feeling of being reborn. After taking MDMA, I’ve decided to never lie again in my life. (NB) When I first started with psychedelics it was just to get high at parties and make new friends and have wonderful experiences. And then as I've gotten older, now I pretty much only used psychedelics, and not too often. … Now it's definitely changed to being a tool to become a better person. (AA) Nowadays is, less about the party and more about some sort of spiritual thing. (KD)
It also became clear from our respondents’ discourses that they established a correlation between responsibility and knowledge about drugs. Our participants value drug information infused with scientific vocabulary, the use of words and expressions like: “addictive potential,” “drug interaction,” “molecules,” “common adulterants,” etc. Several (n = 7) participants referred to PubMed as a preferred source of information: I start with Wikipedia or Erowid because everything is there, and you have the molecule and the mechanism, and then if I want to know more, I can go on PubMed or something like that to… (HN) I am a doctor, I prefer to search in PubMed. (PC) I search on the internet normally. For example, when I was interested in mescaline, I searched before using the internet about how much you should take or what the interactions could be. (AA)
Research participants attributed much value to exchanging what they perceive as scientific information, particularly in their interactions with friends and suppliers. The use of this more hermetic language seems to provide them with a sense of security within the risky and unpredictable drug-using experience, a way to achieve control (Ruane, 2018). I like to know how it affects my brain, what molecules are going in. (KM) I look at the addictive potential. I know that alcohol is banalized, but it is something you can get addicted to … I remember that when I was a teenager, I looked at ecstasy addiction potential, and it was really low compared to alcohol, so that's why I decided more to go toward ecstasy than toward alcohol because I wanted to be able to just stop whatever I wanted. (KM)
Narratives around the experience and knowledge about drugs and individual responsibility are typically present in our participants’ discourses. These ideas are reflected in the adoption of several harm reduction strategies to avoid harm but also having fun and experiencing pleasure (Taylor et al., 2020). To achieve their desired outcome, our participants reported setting in motion a series of specific practices that they have learned and that work for them. The most commonly referred strategies are “buying from a trusted source,” “avoiding buying in festivals and parties,” “using test kits,” “starting slow and waiting for the effects,” “searching information about drugs,” and “planning their drug use sessions.” First, I took a quarter and then a half, and then … you know, going with the flow, and if it weren’t enough, then we would do more because we really don’t want to have a bad experience. (LJ) Yeah, at Boom, we didn't have a scale. So it was, hum, I think we would divide a gram by 10, and then we would have, hum, more or less a hundred milligrams per dose. And nowadays, I have a scale, so I would prefer to use a scale, obviously […] We're organizing small, small parties as well, and then we'll have these easy tests available as well. (KH) I make sure I've eaten well, I try not to have a big night out on an empty stomach. Um, I make sure I just feel good in general and that there's nothing like, like subconsciously really bothering me. Um, and I guess I always make sure I have enough weed, And then I just make sure I don't have any responsibilities coming up or anything, any tasks that I should be, you know, very clear for. (JH) I’m kind in a control freak, so, I’m not … I’m kind of fun, but I’m not the funniest person in the group because … I’m the one who is going to say “No, I’m not going to snort with the same tube that you did.” I’m kind of the mum of the group, every time. (KM)
As Race (2008) states, pleasure is not inherently automatic or instinctual, a sensation awaiting release; instead, it is attained by enacting specific behaviors that require prior learning. The implementation of harm reduction strategies potentiated the pleasure derived from drug use while also supporting people in managing their internal conflicts around drug use. Research participants used drugs, which were prohibited, thus adopting a behavior still perceived as transgressive by mainstream society, but at the same time, applied a series of strategies to minimize the potential risks and guarantee that their social position was not questioned (Duff, 2005; Parker et al., 1999; Parker et al., 2002). In fact, even people with behaviors that might be perceived as “deviant” created a set of rules that help them construct an “ideal” and strive to achieve it, while looking down on those who stray from it. We observed that several of our participants stated that, unlike them, their friends were not responsible in their drug use: I don’t want to do anything stupid or just be in danger and don’t know what to do. […] I don’t know why, like my friends … they just don’t care. (KM) I'm usually the most careful one and me and the group of people. Um, so most of them wouldn't have done it[test their drugs]. (JH) We are all experienced users, but I have always been more responsible. I like knowing what I’m taking and, as I said, knowing the risks. I like knowing and kind of controlling what's going on in my body. […] and they[my friends]are like free spirits, they don’t care, they trust the process, all that (laughing), yeah. (BZ) I have always been careful. Maybe it's like a control thing, which is just part of me. (OG) I think it's like 50–50, like 50% of the people just like do things without really thinking about it,, just kind of irresponsibly. And then the other half, I think they consider what they must do to be safe. (AA) I think I’m like 1%, hopefully … I think I’m one of the few people that would be concern about this. Everybody else would say “fuck it,” i’ll use anyway, but I can’t do this. (NM) I test MDMA, by taking a little bit a little bit of it, a little bit. It's a lot of people, you know, especially young kids, they just shuffle a handful of pills and follow it with drinks and then … then there's tragedies, you know… (BZ) Some people are lazy. They just can't be bothered going there and being there. They just want to have fun. (FP) If there's a service like that available, why not take advantage of it? You feel almost stupid not to do it really. (RS)
It was clear that our participants valued the ideals of responsibility and trust, and using the DCS put them in what they perceived as a superior position, an advantage concerning others who use drugs but didn’t make such “intelligent” choices (Taylor et al., 2020).
Beck (1992, 1999) has analysed the tension between the “experts” determination of risk and the assessment made by non-experts that do a culturally determined risk analysis grounded in direct experience, what he calls the “lay knowledge”: our participants seem to navigate between the value they attributed to “experts knowledge,” that they found in the papers and books they read, and their own experiences and feelings, to help them deal with their drug experiences (Duff, 2003).
In this context, DCS is a pragmatic and responsible response that helped our participants manage the perceived risks and enhance the potential benefits of drug use for themselves and others, providing them with some personal control over the possible consequences of their drug use (Campbell, 2021).
Drug Checking as a Care Practice
Kosmicare's harm reduction responses at the Boom Festival created a structure from where solidarity and care systems could be potentiated by facilitating peer interaction and disseminating pro-health norms that promoted loyalty to the idea of responsible drug use and the festival code of conduct. Setting up a full-spectrum harm reduction service like Kosmicare within the festival indicated the organizers’ commitment to care. The dissemination of the services’ location and purposes, harm reduction information and drug-checking alerts via the festival's app, website, social media platforms and other means of communication with Boomers set the tone for the communal care and solidarity networks that were created during the festival, promoting an “enabling environment” for reducing drug-related harm (Duff, 2009; Moore & Dietze, 2005). Matured from the theoretical framework developed by Rhodes (2009, 2002) of “risk environment” as “the space— whether social or physical—in which a variety of factors interact to increase the chances of drug-related harm” (Rhodes, 2002, p. 88); Moore and Dietze (2005) defined an “enabling environment” as an environment that potentiates the reduction of drug-related harm through identification and removal of barriers to harm reduction and the promotion of public policy and drug policy reforms. Duff (2009), in a qualitative work about the importance of affect and repair in the development of enabling environments, described “pill testing” efforts as trustworthy and reliable, “way of enhancing community networks and social repair relations enhancing the experience of reciprocity and solidarity within these communities and contributing to the generation of discrete cultures of care” (p. 207).
This environment is further potentiated by the Boom Festival organization that funded and supported setting up a caring, inclusive, and educational space for Festival patrons, where honest conversations about drugs could emerge between people who perceive themselves as equals. Grounded in peer work, Kosmicare's intervention offered the possibility of accessing specialized care within the framework of a collaborative exchange between people who do not have authority over each other (UNODC, 2003).
When reflecting upon their experience with Kosmicare's services, interviewees said: [After getting the test result] We knew what we were taking, we knew that there were people there to take care of us if something was wrong … so we were relaxed. Even the ones who didn’t want to test their drugs were happy in the end. (KM) [Kosmicare services] For me, it brings a nice feeling to the festival. I feel I am being taken care of. It feels safer even if I don’t need it. (SG) I can just say that it's awesome that people can have their stuff tested and hopefully don't harm themselves. I think they [Kosmicare] also kind of, uh, reduce the bad stigma and the bad stereotype that all drugs have, I guess. (FP) Boom is the only place where I've ever used it, mainly because I needed to. I would always use if it were available, basically. If it's available, it's a bit of a no-brainer not to use it. So yeah. (DK)
Our participants have also overwhelmingly expressed concern about the well-being of those around them. This feeling of shared responsibility toward fellow Boomers worked as a clear motivation to have drugs tested. Very eloquently, one of the participants called this specific role of testing for other people the “designated tester”: Kosmicare could create the designated tester. I would suggest creating something like that, like in the alcohol campaigns, because it's already in practice at the festival. (NB) I tested for a friend and his boyfriend. It was their first time at the last Boom festival, which is why I also decided to check the drugs because it was their first time. So, I felt a little bit responsible… (NB) Everyone (all my friends) was interested in testing, but I was the one who was organizing it. (OG) We were with friends, so we got a certain amount of MDMA, and again, we just decided it would be best to have it checked, and I went there and had the sample tested. It was from the same source, so that makes sense; I was testing a sample for all of us. (OG) At the time, I was buying stuff from the Dark Web, but I wasn’t sure about the stuff I was getting. I was buying for my friends, so I wanted to test it. … It was the best thing to do. (SG)
Solidarity emerges between groups of people who use drugs through collective action to produce collective good (Douglas et al., 2015). Several “goods” are exchanged between Boom Festival Patrons, such as companionship and a sense of common purpose derived from collective participation in a joint project with shared values and purposes. It's no coincidence that the festival's motto is “We are one,” promoting this sense of communion and belonging among Boom patrons. The festival website states, “Caring for each other and respecting each other's differences. Our kindness and compassion is what makes us human and what makes us boomers. We believe in a culture of interdependence where we are free of corporate exploitation, thus creating a festival by the people, for the people” (Boom Festival 2023, n.d.).
In the case of people using DCS, these collective goods involved the exchange of information about drug content and specific harm reduction practices, as well as a shared sense of responsibility for the community's well-being. People organized themselves to have a better festival experience, which implied the division of tasks, and going to the DCS was seen as a relevant action to guarantee a good festival experience. The person responsible for testing and getting relevant information for the group worked as a multiplier health and well-being agent. These results are consistent with those from other studies. Larnder et al. (2021), for example, reported that testing drugs on behalf of others, what the authors call third-party drug checking, is a prevalent practice among their survey respondents (N = 1653). Fifty-two per cent of the service users reported using the drug checking service for others or themselves and others, and 12% admitted testing to sell. Most respondents who did third-party drug checking did it for their friends (Larnder et al., 2021). This reinforces the social aspect, not only of drug use but also of DCS, emphasizing practices of care among people who use drugs. This is very important as research shows that social networks highly influence risk perception, playing a vital role in adopting risk protective measures (Kelly et al., 2012, 2013; Kubicek et al., 2007; Parker et al., 2002).
Third-party drug checking is also a way to reinforce service accessibility and range. The information from DCS has the potential to reach larger audiences when people test for other people, and its impact can go beyond the individual and impact the behavior of larger groups and communities. Palamar et al. (2019) also explored the motivations for people to have their drugs tested, and the findings were also consistent with our results: the participants expressed a clear motivation to protect other people who use drugs from harm. They displayed altruistic purposes and a desire to increase their community's safety.
These behaviors underline a sense of solidarity and internalized responsibility that has been previously described in the literature about communities of partygoers (Kavanaugh & Anderson, 2008; Van Havere et al., 2015) and harm reduction collectives can exploit that to increase the impact and reach of their interventions.
Drug Checking as a (Mis)Trust Practice
Our participant's narratives also underlined the importance of their relationship with drug suppliers. Mistrusting the source was the most common reason for using Kosmicare's DCS. As we have observed, the most relevant harm reduction strategies applied by our participants were also related to the person selling them drugs, for example, “buying from a trustworthy source.” All our participants mention feeling uncomfortable when they need to make purchases at parties or festivals from people they don’t know: I think, you know, buying, buying at a festival when you don't really know … it just makes complete sense to get tested it! Yeah! (DK) The person we bought the drug from, I didn’t know her. It was just a random person, I don’t know. Can I trust her? Is she really selling me good stuff? Since I knew it was my first time, she could tell me any lies she wanted, so I really wanted to be sure. So, that's why it made total sense to test. (KM)
Trust was mentioned as the most crucial factor mediating the relationship between seller and buyer in drug transactions and one of the main drivers for using or not the DCS at Boom Festival. When delineating the ten principles in health risk communication for DCS, the EMCDDA (2023) defined trust and credibility as the most important principles to consider. Audiences respond positively to communicators they perceive as trustworthy and are sceptical of messages from people or organizations they distrust. Trust becomes even more critical when a context is marked by insecurity, like illegal drug transactions (Gambetta, 2000).
Our interviewees overwhelmingly discussed the importance of trusting their suppliers and how their relationship with the supplier impacted their drug-using behaviors: Only trust. Only trust … I’ve known this person for a long time, for 5/7 years. … Maybe more. I only buy from people I trust. (NM) I would like to take other substances like ecstasy and amphetamine sometimes, but because I don't have good people to get it from, I don’t do it … a lot of it is terrible quality. I think the dealers are more trustworthy in the psychedelic world, so I prefer to use psychedelics. (RS) I would need to be extra careful if you're at a really big festival because there are people there that can make a profit. (KH)
Participants also discussed the importance of clear and open communication with the people who supply them. When people who sell seem knowledgeable about what they have to sell, people's sense of trust is increased: Normally, I talk a little bit to the person to get a feeling if the person is informed or not. I ask the person, “How strong is strong"? And they say, “Well, my friend said, it's very strong.” And that's the only information the person can give me; I'm like, “Sorry, I'm not interested because this is super unspecific.” So, my strategy is to talk to the person who is selling and ask other people if they know the pill. Yeah, that's my strategy. (JH) Some things we bought from home, and others were from people we know and like; we talk a lot with the people selling us the stuff. We felt they were sure about what they had, and we felt very comfortable taking them; we didn’t feel the need to test. In this festival edition, we bought something from a person; she said that it was mescaline, and because we were interested in taking it, we bought it, but we didn't feel that she knew a lot about it. She wasn’t sufficiently informed about the stuff she was selling, and we were already a little bit like, Humm, let's see. And then we talked to a friend, who said this cannot be mescaline. Mescaline cannot be in this presentation. And then we said let's check it … and we took the stuff to Kosmicare. (BZ) I don’t know, I think they were just pretty confident, like I’m sure what is, I’m sure, I’m taking it, and I wasn’t that sure because the person we bought the drug from, I didn’t know her. It was just a random person, I don’t know. Can I trust her? Is she really selling me good stuff? Since, I know it was my first time, she could tell me any lies she wanted, so I really wanted to be sure. And they were more like “I trust this person,” and yeah. … No, it was a random person form the festival. So, that's why I … they were … I don’t know … really confident about it and I wasn’t. (KM)
The quality of the products is subjectively assessed based on the length and type of relationship participants establish with their sources. The motivation to test decreases considerably when the relationship with the person who sells is well established. I don’t test because I always use the same dealers and the same drugs. I trust my dealer. (AF)
Our participants’ narratives are consonant with other literature that indicates that using a trusted and reliable supplier is seen as a fundamental harm reduction strategy by most people who use drugs (Bardwell et al., 2019; Carroll et al., 2017; McKnight & Des Jarlais, 2018; Soukup-Baljak et al., 2015; Taylor & Potter, 2013). Also, many of our participants (16) mentioned feeling uncomfortable when they needed to make purchases at parties or festivals from strangers. Bardwell et al. (2019) also mentioned that their research participants disliked buying at parties and mentioned unknown suppliers could display a lack of responsibility toward their customers.
Our interviewees provided a central role to the people who sell drugs, believing they hold a high level of control over their supply. Our participants seemed to disregard the structural fluctuations that the informal drug market is subjected to, as only one linked it with adulteration. I think [using the DCS] changed the way that I relate to the people selling the drugs at the festivals because until then, I had always had the perception and the experience that people at trance festivals have good intentions and don't mean to, hum, poison people, you know, just do bad things and just make money. Um, so until then, I had that thought, and that kind of changed my head. (FP) The results from the test made me change my perception of dealers in trance parties, I thought they were cool, not real dealers … but they just want to get profit. (NM)
When a trustful relationship is not established, if a substance was adulterated or did not have the intended effect, our participants assumed the person supplying it was responsible. This breach of trust usually came as a surprise to our interviewees, who tended to have a favorable opinion of the people who supply drugs in psychedelic events, like the Boom Festival. One of our participants stated this by saying that the results from the DCS made him change his perception about people selling at trance parties. He believed they were not “real dealers,” reinforcing the stigma attached by mainstream society to the word “dealer” as someone unscrupulous that preys on people who use drugs (Coomber, 2006). Once again, it underlines the perceived exceptionality of the people who use and supply drugs in these settings. Our participants’ narratives convey the idea that people selling drugs have a high degree of control over their supply, attributing them much power. However, the distinction between seller and buyer can be much more fluid than these discourses (Boyd, 2014).
Two of our participants admitted to selling drugs, and both of them perceived themselves as “trustworthy,” stating they used DCS as a practice of care toward their clients: I know many other people who sell do the same thing I do, and we try to test the stuff before selling so we know what we have. We have experience with the stuff we sell. I always do that … Whenever I get new stuff, I take it. (SG) When I can, I test the stuff to tell people the result. At Boom, I did that, just tested the first day. People feel much safer knowing the result. (SG) Yes, I went on the first day because I promised … (here, it's also a bit more personal). I took things to boom with the intention of selling them. So, the first thing I did to be sure that what I had would not cause damage to anyone was to get it tested. I tested the first day the service opened […] I want people to be ok. (GP)
The two people we interviewed who disclosed selling drugs used the DCS as a way to be more responsible toward their drug use but were also concerned about the people they were selling to. It became clear from their narratives that they were not confident about their sources, and when a DCS was not available, they tested the drugs on themselves. Like many people who use drugs, one of the sellers was getting their supply from dark web markets and was unsure about the actual contents of the products they were selling.
For people supplying drugs, DCS can work not only as a safety and care practice but also as a marketing strategy. One of our interviewees who admitted to selling drugs mentioned buyers would feel more comfortable acquiring substances when they know they “are ok.” Palamar et al. (2019, p. 167) also identified a “small group of ‘altruistic people who sell drugs’ who tested their products before sale, partly to protect their clients and partly as a ‘sales pitch’ to generate repeat business.” Betsos et al. (2021), in an ethnographic study of drug sellers, explored the discourses that they had about the drug market and how DCS affected their understanding of the drugs they were selling, as well as which strategies they employed to reduce harm. Their results evidenced that drug sellers used the drugs and tested them as ways to mitigate risks for themselves and others. The suppliers interviewed by Betsos et al. (2021) also mentioned that DCS worked as a strategy for supplying drugs that met consumer demands, hence as a marketing strategy.
It is clear from our participants’ discourses that suppliers assume crucial importance in the decision-making process of people who use drugs, not only regarding the use of DCS but also the dosages ingested and other harm reduction strategies. How this role could be integrated or exploited by harm reduction collectives is highly challenging and virtually impossible for many harm reduction services, particularly DCS, as many are prohibited by law from testing to known suppliers. However, a reflection is demanded on how to engage these key actors in harm-reduction efforts, particularly peers who might engage in social supply.
Limitations
This study presents some limitations. The sampling strategy was based on convenience sampling. Invitations to participate were sent to everyone who used Kosmicare's DCS and agreed to share their email address.
Convenience sampling presents obvious generability issues, so the results discussed in this manuscript cannot be transposed to people who use DCS in different settings. However, after comparing the sample under study to the entire population of people who used Kosmicare's DCS during the 2018 Boom Festival, only minor differences in socio-demographic characteristics were found. The 343 individuals who used the DCS in 2018 had an average age of 29, with 59% identifying as cismale, 76% holding a university degree, and 80% currently employed. The current sample size comprises 22 individuals, with an average age of 29, 68% identifying as cismale, 77% holding a university degree and 100% being employed.
All the interviews were performed online. To be able to answer, participants needed internet access as well as the technological expertise to use Zoom. Also, researchers could not control the environment in which the interview took place on the side of the interviewees. Still, we believe using the Zoom platform did not interfere much with the recruitment process, considering the specific context of this study.
Interviews that require people to disclose intimate and/or illegal behaviors, like using or selling drugs, might be tainted by some desirability bias, with people being inclined to convey the idea that they are highly responsible and careful to avoid judgements. Still, our findings regarding adopting harm reduction strategies align with previous quantitative work done with the same sample and other research with similar groups.
Two participants felt comfortable disclosing that they sold drugs and were using the DCS not only for themselves but for others. It is possible that other participants who have mentioned testing for other people could also be suppliers but didn’t feel comfortable sharing this information in an online interview that is being recorded. Also, the interview was not designed to uncover this information directly for ethical reasons.
Conclusion
Our data reinforces the idea that people in recreational settings present high levels of knowledge about the psychoactive substances they use and apply a considerable amount of energy to manage the risks and benefits they attribute to their drug use. These people are very interested in using harm reduction services and work as multiplier agents of the messages disseminated by harm reduction services.
Our findings expand the current literature that demonstrates the usefulness of DCS as an intervention to mitigate individual risks of drug use within the unregulated market but provide indications of the considerable communitarian potential of this type of intervention as a means to expand a “culture of care,” within the partygoers’ community. A culture of care in this context refers to the tendency to provide support and watch out for one another within a group (Hurley, 2002). People who come to the DCS to test for others work as health multiplier agents having a fundamental role in enhancing the range and impact of harm reduction messages, particularly if we consider that harm reduction projects have limited resources. At the Boom festival, for example, Kosmicare can only test a limited amount of drug samples for a limited amount of people: “This creates a ‘bottleneck’ effect where only the most motivated and organized patrons will access DCS” (Valente et al., 2022b). The service must rely on these “designated testers” and, eventually, on suppliers to disseminate information to a broader audience that does not want or cannot access the service. The complete integration of people who use drugs appears as a necessary step toward opening up DCS data to larger audiences. This can be done by engaging more peers in harm reduction work, living up to the activist participation motto “Nothing about us without us” (Jürgens, 2005). The integration of people who use drugs in DCS should happen from the moment of planning the service to its evaluation. This participation should be adequately supported through financial compensation and capacity-building activities to support the work of peer workers and educators.
It becomes clear from our participants’ discourses, and also from previous research on this field, that people who use drugs rely on friends and trusted suppliers not only to get drugs but to get information about them and make informed decisions (Decorte, 2001; Panagopoulos & Ricciardelli, 2005; Sheridan et al., 2009). Understanding the dynamics of social supply 1 and the fluidity between supplying and using drugs, might provide an opportunity for people who use but also supply drugs to further engage with harm reduction services, namely by using DCS and disseminating harm reduction information to people who otherwise might not access the services.
Our findings are aligned with other research on the topic (Betsos et al., 2021; Coomber, 2006) that refutes the idea, usually conveyed by society and mainstream media, that people supplying drugs are all predatory, criminal individuals. Indeed, we demonstrate that very often they do not differ much from people using drugs. However, due to legal restrictions and politics, in most countries, it is still impossible or extremely controversial to include people selling drugs in the design and implementation of drug responses. The Portuguese decriminalization policy, although criminalizing drug trafficking, might be a privileged context to rethink alternative accessibility and ethical policies that could allow people who use and supply drugs to access the services and disclose their identity without fear of prosecution. Doing so could permit harm reduction collectives to take advantage of their position within the drug market to improve communication and tailor harm reduction strategies to wider audiences (Betsos et al., 2021), potentially leading to more effective and targeted harm-reduction interventions (Soukup-Baljak et al., 2015; Taylor & Potter, 2013).
Footnotes
Acknowledgments
We would like to acknowledge the contribution of Joana Castro, Filipa Gonçalves, and Sara Adão and all the members of the Kosmicare team working at Boom 2018. A special thanks to the Boom Festival organization for their unconditional endorsement of harm reduction and for their openness and support to this research project in particular.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Helena Valente and Daniel Martins are members of Kosmicare. Monica J. Barratt is a volunteer for the Loop Australia.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Helena Valente was supported by the Foundation for Science and Technology, through a research grant with the references (PD/BD/135079/2017 and COVID/BD/152358/2022) supported by the European Social Fund and funds of the MCTES. Daniel Martins was supported by the Foundation for Science and Technology, through a research grant with the reference PD/BD/135122/2017 supported by the European Social Fund and funds of the MCTES.