
Abstract
Introduction
MDMA (3,4-methylenedioxymethamphetamine)-related deaths and other harms have been a topical subject in Australia in recent years (Rigg & Sharp, 2018). MDMA and other psychoactive drugs have a long history of association with party cultures, and the potential for experiencing drug-related harm in these settings has been well-documented (AAP, 2017; Anderson, 2017; Ferraro, 2006; Grahame, 2019; Parliament of Victoria, 2003; Spanos, 2021). Despite dominant perceptions of drug use in party settings as harmful, research suggests that most illicit drug use among Australian partygoers is “occasional and relatively non-problematic” (Hughes et al., 2019, p. 7).
Grounded in justice and human rights, harm reduction policies, programs, and practices “aim to minimise negative health, social, and legal impacts associated with drug use, drug policies, and drug laws” (Harm Reduction International, 2022, n.p.). Despite the inclusion of harm reduction as one of the three central pillars of Australia's National Drug Strategy 2017–2026 (NDS), the most recent estimation of expenditure in 2009/2010 suggested that harm reduction received just 2% of funding (Australian Government, 2017; Ritter et al., 2013). The implementation, availability, and accessibility of harm reduction and other support services affects the agentic capacity of people who use MDMA to avoid or reduce harms. However, barriers to accessing support—including ongoing stigma and discrimination toward people who use drugs—can alienate people who use drugs from the broader service system, resulting in decreased abilities to manage their overall health (AIVL, 2011, 2017; Harm Reduction Australia, 2022; Link & Phelan, 2006). Moreover, Ritter et al. (2013) suggest that the financial imbalances of the NDS mean that Australia's drug policy effectively criminalizes people who use drugs rather than reducing drug-related harms, and therefore may exaggerate or contribute toward harms.
Discourses around MDMA consumption in public health, political, and academic spheres, tend to focus on harm, risk, and the problems with people who use MDMA (AOD Media Watch, 2022). The positive aspects of MDMA use are often ignored in risk-centric discourses, and so too are the ways in which people who use MDMA act to mediate and avoid potential harms to achieve desired effects. It has been suggested that separating drug-related harms and pleasures prevents a nuanced understanding of drug consumption and experiences, as risks cannot be fully understood without properly acknowledging the pleasures associated with drug use (Duff, 2008; Duff et al., 2007; Pennay & Moore, 2010; White et al., 2006). To overcome patterns of cultural exclusion, Duff (2008) encourages researchers and policymakers to embrace the nuance and complexity of the pleasurable and painful elements of MDMA use, where drug use may serve a fundamental coping and spiritual purpose.
In academic literature, the task of documenting risks associated with MDMA use has sometimes overshadowed attempts to foreground narratives of the lived experience of drug use. Australian literature on what are considered more harmful consumption practices around MDMA has identified numerous “risky” behaviors, including double dropping (two doses of MDMA at once) (Grigg et al., 2018, 2022; Page et al., 2022), higher rates of alcohol consumption while using MDMA (Page et al., 2022; Kinner et al., 2012; Peacock et al., 2016), polysubstance use (Page et al., 2022; Peacock et al., 2016), and consuming high quantities of MDMA in a single session (Page et al., 2022). Physical harms related to MDMA are well-documented in the literature (Todd et al., 2019; White et al., 2006) and although uncommon, can include hypertension (Vollenweider et al., 1998), hyperthermia (Green et al., 2004), serotonin syndrome (Parrott, 2002), seizures (Giorgi et al., 2006), stroke (Darke et al., 2019), hyponatremia (Budisavljevic et al., 2003), and cardiac arrest (Fonseca et al., 2021). In nightclubs and festivals, where MDMA is commonly used, these harms are heightened by environmental factors, including overcrowding, elevated temperatures, inadequate ventilation, and a lack of water (leading to dehydration) (Palamar & Sönmez, 2022; Parrott, 2012). The Australian context can further amplify people's experiences of these harms due to the region's typically high ambient temperatures, the popularity of remote outdoor events, adulterated MDMA supply, and relatively low provision of harm reduction services such as drug checking services (McCarthy, 2013; Peck et al., 2019; UNODC, 2019). Similarly, comorbidity research has highlighted how higher frequencies of MDMA use are associated with increased psychological distress (Kinner et al., 2012; White et al., 2006), impulsivity (Meikle et al., 2020), and depressive symptomatology (Matthews & Bruno, 2010). However, documentation of the ways in which people who use drugs attempt to mitigate potential physiological and cognitive harms, and the caution that they may apply to protect themselves when consuming substances, is absent from much of this knowledge.
A handful of articles have identified why people may adjust consumption practices to avoid potential harms associated with criminalization and prohibition. For example, drinking more heavily than usual, “preloading” (i.e., consuming alcohol and other drugs before an event), panic consumption, internal concealment, and consuming higher doses, have been identified as techniques employed to avoid negative interactions with law enforcement (Grewcock & Sentas, 2019; Grigg et al., 2022; Malins, 2019; McGowan, 2019). These behaviors may also result in increased harm, suggesting that Australia's current approach to policing drugs produces conditions where people engage in risky behaviors. This highlights a delicate balance for people who use drugs to negotiate (Duff et al., 2007; Pennay & Moore, 2010).
Global literature documenting the practical strategies adopted by people who use MDMA and the role of these strategies in reducing drug-related harms has been conducted ad hoc, and generally reflects the work of smaller, qualitative projects, as opposed to large-scale and ongoing data collection procedures. In the past decade, research such as the Global Drug Survey (Winstock et al., 2021) indicates a gradual shift toward the representation of the voices of people who use drugs, and a consideration of the nuances of drug use in large-scale quantitative drug research. Australia is fortunate to have annual research from the National Drug and Alcohol Research Centre (NDARC) Drug Trends program, including the Ecstasy and related Drugs Reporting System (EDRS), which monitors some behaviors of people who use MDMA (NDARC, 2022). However, the EDRS is not funded sufficiently to thoroughly describe the world through the eyes of people who use drugs and their subsequent techniques of maintaining their welfare when navigating how to act toward drugs. Similarly, Australia's National Drug Strategy Household Survey (NDSHS) is an important large-scale data collection tool but lacks a focus on the views of people who use drugs and affected communities (Lancaster et al., 2013b, Lancaster et al., 2017).
The present study was conducted with consideration of the evidence for investing in harm reduction programs, the dominance of risk-centric research on people who use MDMA, and the importance of considering both risk and protective factors. The aim was to identify Australian literature that investigated the harm reduction practices adopted by people who use MDMA and to map what is known about the protective factors at play for people engaging in these activities. The research question guiding the review is: “What is known about the practices of harm reduction among people who use MDMA in Australia?” A scoping review methodology was chosen to synthesize a broad range of sources, including peer-reviewed and gray literature, quantitative data, and qualitative research that captured the voices of people who use MDMA. Scoping reviews provide a rapid overview of a specific area of knowledge to identify the main sources of evidence for a given field of research (Arksey & O’Malley, 2005; Levac et al., 2010; Peters et al., 2015, 2020; Tricco et al., 2018). The primary objectives were to understand the potential gaps that exist in the literature pertaining to drug-safety strategies utilized by people who use MDMA, and to provide insight into the ways in which we might approach drug use and drug policy reform.
Method
The review was conducted in accordance with the Arksey and O’Malley (2005) methodology for scoping reviews, along with Levac et al. (2010) recommendations for seeking to analyze data, not in terms of quality, but to describe existing knowledge. A Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for scoping review (PRISMA-ScR) framework was incorporated to strengthen the rigor of the data searching, charting, and extraction phases of the review (see Supplemental Appendix A for PRISMA-ScR Checklist) (Tricco et al., 2018).
The search strategy was developed with the input of two researchers from Students for Sensible Drug Policy (SSDP) Australia's Research Circle and two members of SSDP's Melbourne University Campus Team, who received guidance from an independent advisory committee of researchers in the AOD harm reduction field.
Population, Concept, and Context
The target population were people who use MDMA in Australia, aged 14 years and older. Young people are disproportionately impacted by drugs and drug policy and were therefore considered an important group to include in the sample (AIHW, 2020, 2021; Lancaster et al., 2013a). The eligibility criteria for the review are shown in Table 1.
Eligibility Criteria.
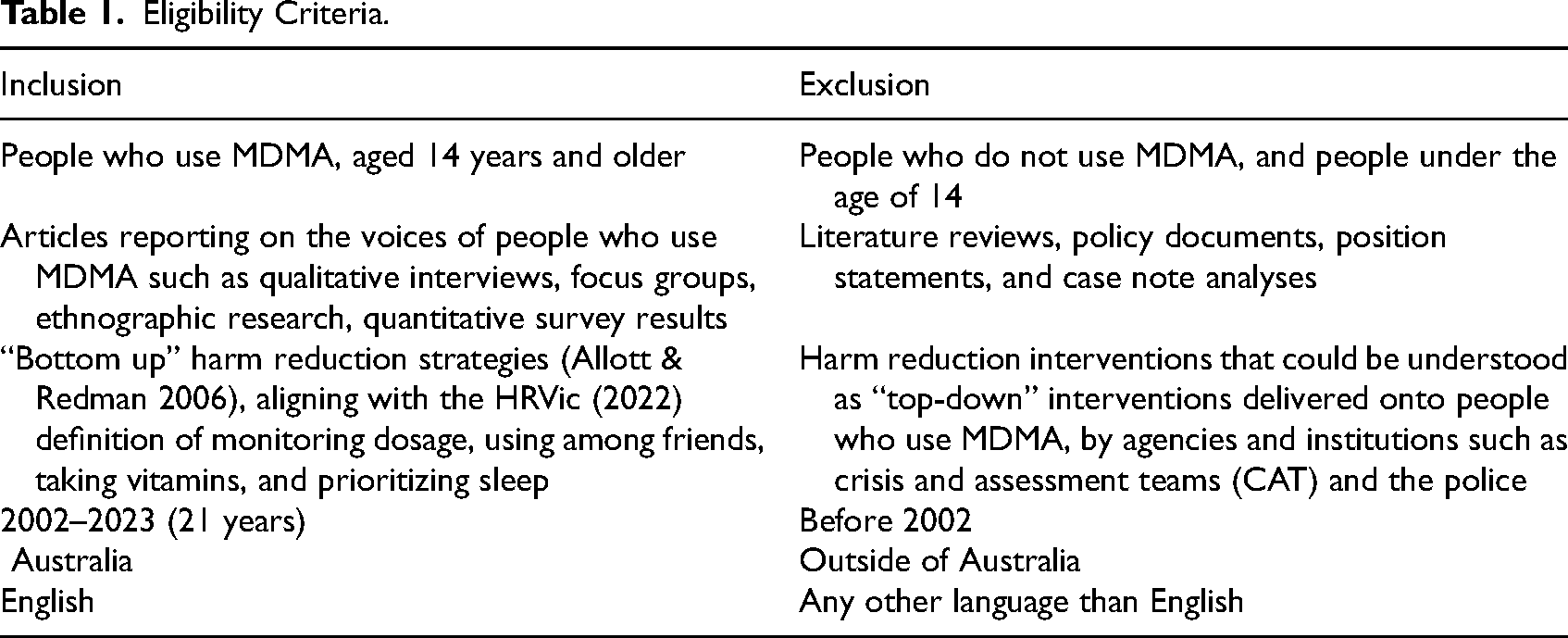
We explored “bottom-up” harm reduction, which was defined as the use of strategies by people who use drugs to prevent or reduce harmful consequences associated with drug use (Allott & Redman, 2006). Harm Reduction Victoria's (HRVic, 2022, n.p.) MDMA resources framed the conceptualization of harm reduction strategies: “using MDMA around people you trust, eating about 30 min before, avoiding +25C heat, awareness of overheating or elevated heart rate, waiting at least 2 h before redosing”. Other practices of self-care were also considered, including “help seeking behaviors” (AIVL, 2017), such as accessing health services for drug-related support. Harm reduction strategies were not specific to MDMA use as many of the eligible studies reported on people who use MDMA, as well as people who use MDMA and other drugs, and their harm reduction practices more broadly.
Australia was selected as the geographical context for the review with consideration of how policy and experiential contexts may differ substantially when compared to international jurisdictions. Specifically, reluctance from Australian governments to reform drug policy and implement harm reduction services such as drug checking, has created a policy and service gap where people who use MDMA are not receiving timely health advice and support.
Eligible study designs were limited to those which specifically included the perspectives of people who use MDMA as primary evidence, including interviews, focus groups, surveys, case studies, action research, and ethnography. Both qualitative and quantitative data were included. Secondary evidence such as case notes and hospital data analyses, policy analyses, and literature reviews were not considered. Only English language material was considered, and literature published from 2002 onwards shaped a 20-year date-range, ideally capturing the popularity of MDMA throughout the 2000s in major cities (Roxburgh et al., 2013).
Search Strategy
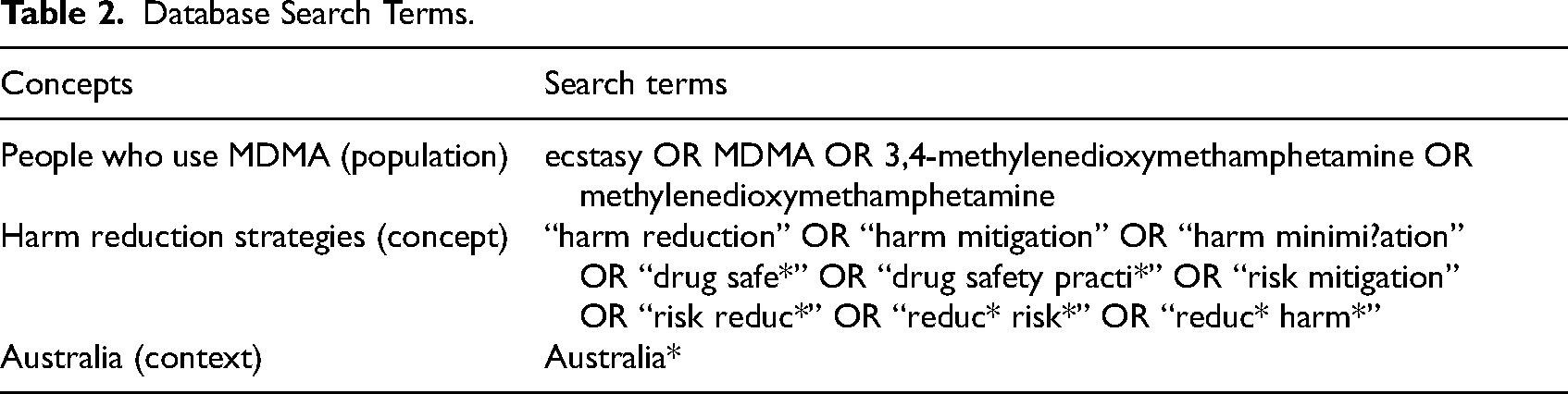
On February 15, 2023, seven topic-specific and multidisciplinary databases were searched from social science, allied-health, and biomedical areas: SociNDEX, CINAHL, Web of Science, Embase, PsycINFO, Medline, and Drug (University of Melbourne, 2022). The search terms used are displayed in Table 2. Both peer-reviewed and gray literature uncovered through the database searches were included, as well as peer-reviewed articles and EDRS national reports identified through a hand-search from the reference lists of eligible articles. While the original scope of the review was to focus on scholarly publications only, it was decided to include the gray literature identified in the database searches that fit within the eligibility criteria and made a significant contribution to the academic knowledge base. The research protocol was registered on the Open Science Framework (OSF) (osf.io/c763h).
Database Search Terms.
Following the search, all identified citations were uploaded into EndNote X9, transferred into Covidence and duplicates were removed automatically. A pilot screening process of 30 articles was undertaken by four SSDP reviewers in line with Peters et al. (2015) who recommended an alignment of 75% across reviewers in respect to decisions made about the inclusion and exclusion of articles. All citations were screened independently by two reviewers at the title and abstract, and full text screening stages. Conflicts were resolved by a vote among all reviewers with 75% consensus. Any ongoing discrepancies were resolved via consultation with the advisory committee.
Eligible data sources were independently coded by two reviewers in NVivo12 through a process of open coding and axial coding, followed by triangulation at each key stage, and theme revision with the advisory committee. Articles were coded and analyzed abductively (Tavory & Timmermans, 2014), drawing on Hsieh and Shannon's (2005) conventional content analysis process and Braun and Clarke's (2006) thematic analysis framework. Harm reduction strategies were identified in three ways: when a text reported a behavior as a harm reduction strategy, when a strategy was identified by participants as an attempt to mediate harms, and when authors reported on a behavior that the reviewers identified as a harm reduction strategy based on the definitions outlined above. Quantitative results were then generated following the confirmation of higher-order themes.
Two reviewers populated the Data Extraction Table (Supplemental Appendix B) with descriptive information and compared their entries to reach consensus and accurately reflect information in line with the research question. Descriptive information included details of eligible sources’ participants, authors, study methods and key findings relevant to the review. The template provided by Arksey and O’Malley (2005) formed the starting point of the data extraction tool that was adapted iteratively throughout the data charting process.
No formal assessment of the quality of individual studies eligible for extraction was undertaken in line with scoping review methodology (Arksey & O’Malley, 2005; Levac et al., 2010; Peters et al., 2015, 2020; Tricco et al., 2018).
Results
Study Selection
Of 280 records identified, 86 were removed as duplicates, 105 were excluded during the title and abstract screen, and 71 were removed at the full text stage, leaving 18 eligible records. The reviewers then hand-searched the reference lists of eligible articles, where another five records were screened and included in the final count of 23 eligible records. Reasons for the exclusion of sources at all the stages of the screening process were presented in a PRISMA-ScR flow diagram in Figure 1 (Tricco et al., 2018).
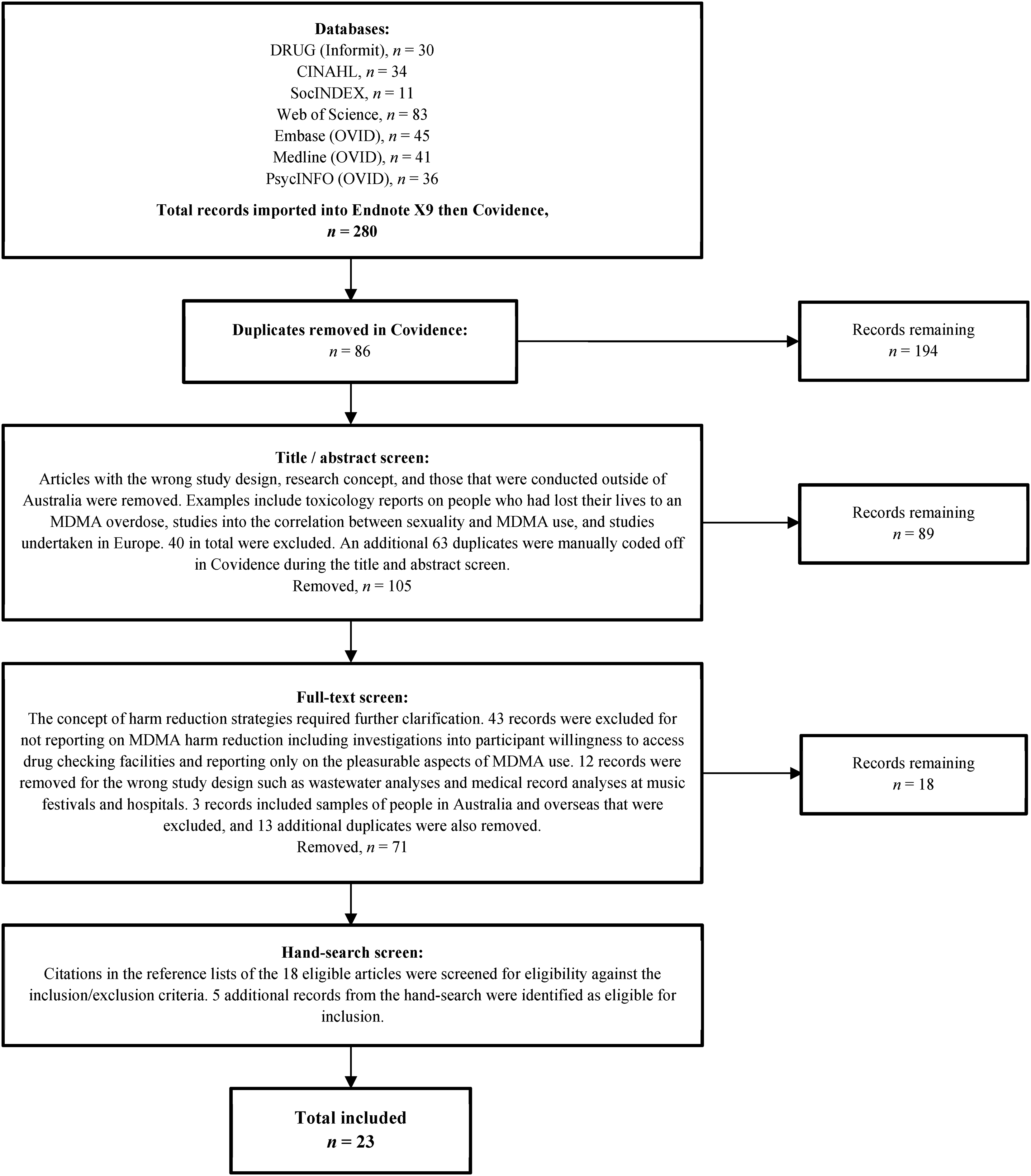
PRISMA-ScR flow diagram.
Scope of Studies
Table 3 presents the geography, methodology, and synthesis of the themes identified across the sample. Not all national studies collected data in every Australian jurisdiction, however the majority (n = 11) had done so (Black et al., 2008; Dietze et al., 2015; Dunn et al., 2006; Gibbs et al., 2023; Johnston et al., 2006; Peacock et al., 2019, 2021; Sindicich & Burns, 2011, 2015; Sindicich et al., 2016; Uporova et al., 2018). Of the 15 national studies, 11 reported on data from the EDRS. Outside of national projects, there were no eligible records identified that had conducted localized research in the ACT, NT, WA, SA, and TAS. In the three states where local research was conducted (VIC, NSW, QLD), the studies were older, with all except one (Southey et al., 2020) conducted outside of the past 5 years (Copeland et al., 2006; Dikes-Frayne, 2014; Duff et al., 2007; Gascoigne et al., 2004; Leslie et al., 2016; Panagopoulos & Ricciardelli, 2005; Pennay & Moore, 2010).
Scope of Context and Methods.
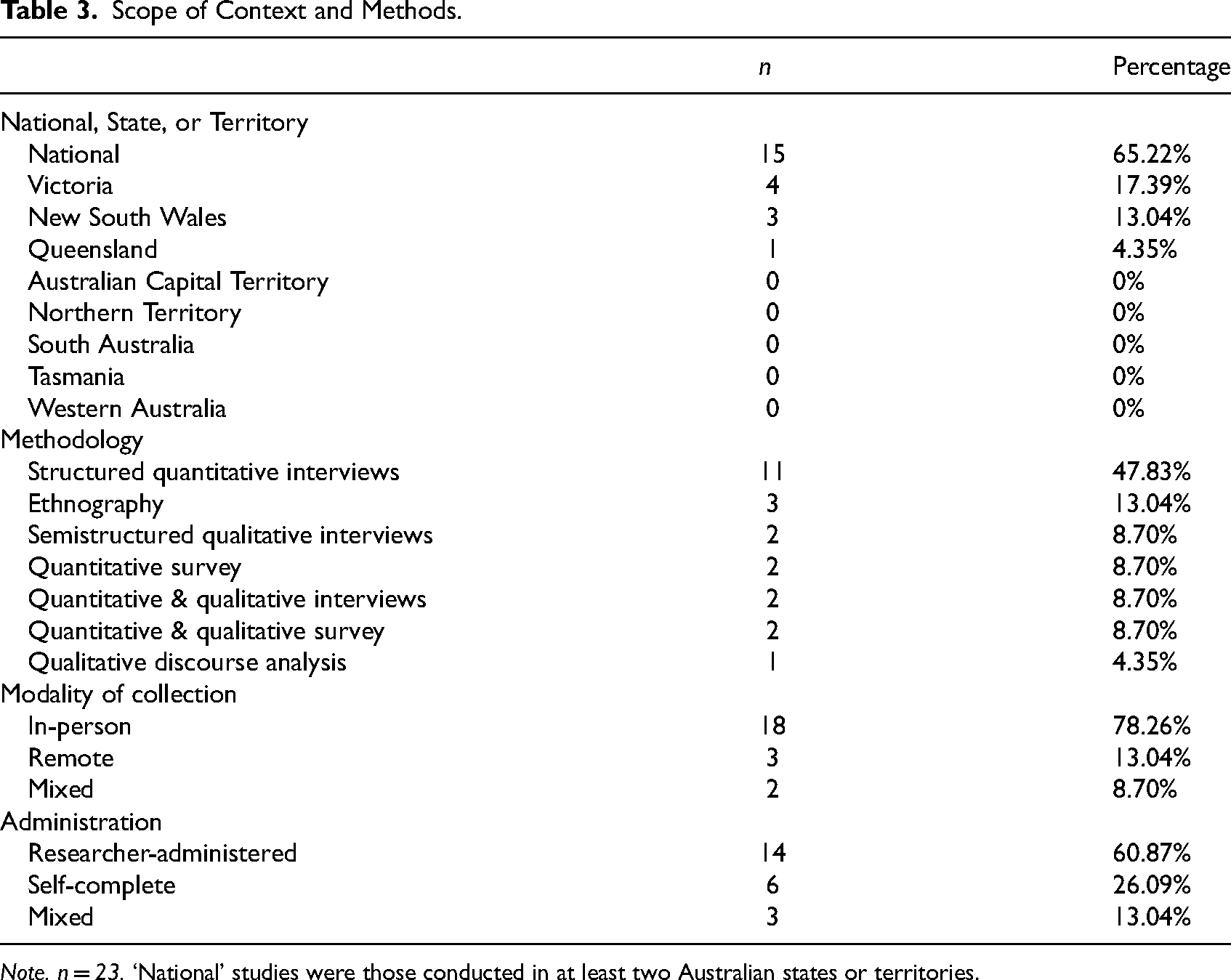
Note. n = 23. ‘National’ studies were those conducted in at least two Australian states or territories.
Just over half of the studies (n = 13) solely collected quantitative data through surveys (Allott & Redman, 2006; Barratt et al., 2018) and interviews, which was significantly influenced by the 11 EDRS outputs utilizing a structured interview methodology (Black et al., 2008; Dietze et al., 2015; Dunn et al., 2006; Gibbs et al., 2023; Johnston et al., 2006; Peacock et al., 2019, 2021; Sindicich & Burns, 2011, 2015; Sindicich et al., 2016; Uporova et al., 2018). Four studies collected both qualitative and quantitative data via surveys (Day et al., 2018; Southey et al., 2020) and interviews (Copeland et al., 2006; Gascoigne et al., 2004). There was a mix of qualitative research designs, including ethnography (Dilkes-Frayne, 2014; Duff et al., 2007; Pennay & Moore, 2010), semistructured interviews (Leslie et al., 2016; Panagopoulos & Ricciardelli, 2005), and qualitative discourse analysis (Barratt et al., 2014).
Themes
The synthesis of articles was summarized under five main themes. Each theme was a higher-order abstraction of the initial codes, and some of the content has therefore been condensed, with conceptual overlap across categories. Across the five main themes were specific harm reduction practices identified in the literature, and a quantitative summary of these practices is shown in Table 4.
Summary of Themes.
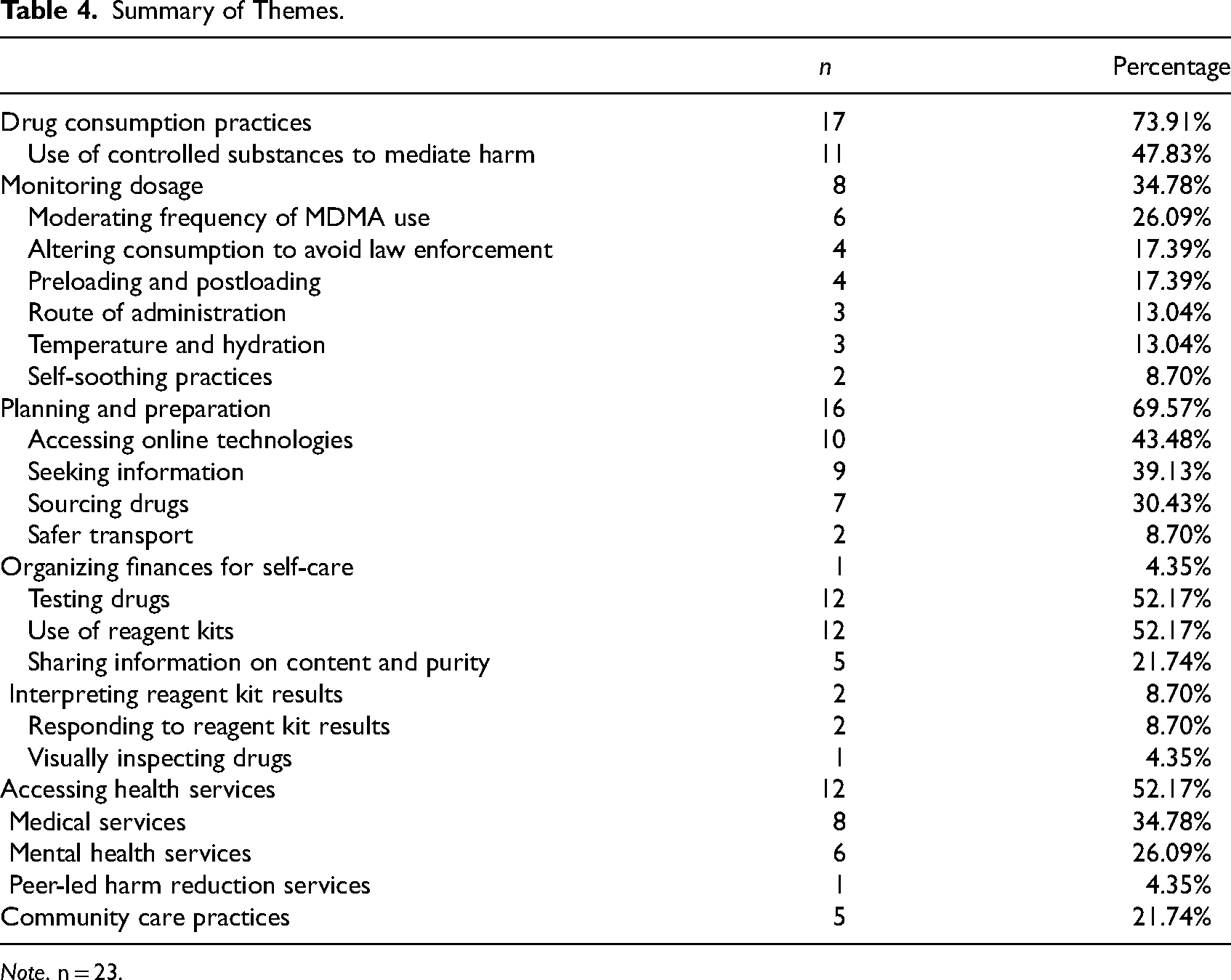
Note. n = 23.
Drug Consumption Practices
Seventeen studies (73.91%) found a range of drug consumption practices utilized to manage MDMA-related harms while maximizing “highs” (Allott & Redman, 2006; Barratt et al., 2018; Black et al., 2008; Copeland et al., 2006; Dietze et al., 2015; Dilkes-Frayne, 2014; Duff et al., 2007; Dunn et al., 2006; Gascoigne et al., 2004; Gibbs et al., 2023; Leslie et al., 2016; Panagopoulos & Ricciardelli, 2005; Peacock et al., 2019, 2021; Pennay & Moore, 2010; Sindicich & Burns, 2011, 2015; Sindicich et al., 2016).
Use of controlled substances was frequently reported as a means of shaping drug effects, namely, to alleviate comedown effects and look after oneself (n = 11, 47.83%) (Allott & Redman, 2006; Black et al., 2008; Copeland et al., 2006; Duff et al., 2007; Dunn et al., 2006; Gascoigne et al., 2004; Leslie et al., 2016; Panagopoulos & Ricciardelli, 2005; Sindicich & Burns, 2011, 2015; Sindicich et al., 2016). Cannabis was said to alleviate distress and aid sleep (Allott & Redman, 2006; Black et al., 2008; Dunn et al., 2006; Gascoigne et al., 2004; Leslie et al., 2016), while pharmaceuticals, including benzodiazepines, were mentioned for similar purposes of cushioning unpleasant effects (Allott & Redman, 2006; Copeland et al., 2006; Gascoigne et al., 2004; Panagopoulos & Ricciardelli, 2005), and alcohol was consumed to aid sleep and reduce anxiety before, during, and after consumption (Allott & Redman, 2006; Black et al., 2008; Leslie et al., 2016).
Preloading and postloading were reported through the consumption of supplements (5-HTP), multivitamins, fruit juice, and some foods to rejuvenate blood sugar levels and avoid neurotoxicity (n = 4, 17.39%) (Allott & Redman, 2006; Copeland et al., 2006; Duff et al., 2007; Leslie et al., 2016). The controlled use of substances was also evidenced to facilitate the MDMA “high” by amplifying pleasures via ADHD medication, cocaine, cannabis, alcohol, and preloading and postloading practices (Allott & Redman, 2006; Copeland et al., 2006; Gascoigne et al., 2004; Leslie et al., 2016).
Managing dosage was also thought to soothe negative emotions and accentuate the positives (n = 8, 34.78%) (Allott & Redman, 2006; Dilkes-Frayne, 2014; Duff et al., 2007; Leslie et al., 2016; Panagopoulos & Ricciardelli, 2005; Peacock et al., 2019; Peacock et al., 2021; Pennay & Moore, 2010). To avoid over-intoxication, people set dosage limits before going out, consumed test quantities, decreased use on single occasions, and spaced-out dosages (Allott & Redman, 2006; Panagopoulos & Ricciardelli, 2005; Peacock et al., 2019; Peacock et al., 2021).
The moderation and limitation of the frequency of drug use was cited as a means of reducing harms (n = 6, 26.09%) (Allott & Redman, 2006; Barratt et al., 2018; Duff et al., 2007; Leslie et al., 2016; Panagopoulos & Ricciardelli, 2005; Pennay & Moore, 2010). “Self-control” (Leslie et al., 2016; Duff et al., 2007) was considered important to maximize benefits and reduce harms, including consuming MDMA only at significant events and not on one's own, intentionally leaving drugs at home, not using MDMA if unwell, seeking out nondrug-related activities, and gradually desisting use as work and family commitments took hold (Duff et al., 2007; Leslie et al., 2016; Panagopoulos & Ricciardelli, 2005; Pennay & Moore, 2010).
Safer modes of consuming MDMA were also cited, including swallowing half-doses, and not snorting MDMA (n = 4, 17.39%) (Black et al., 2008; Dilkes-Frayne, 2014; Duff et al., 2007; Panagopoulos & Ricciardelli, 2005). Many of these practices were learned from friends and peers. Peers also shared strategies to avoid contact with law enforcement and detection by drug dogs, including concealing MDMA capsules before entering festivals (n = 4, 17.39%) (Black et al., 2008; Dilkes-Frayne, 2014; Gibbs et al., 2023; Panagopoulos & Ricciardelli, 2005). Other harm reduction strategies were engaging in self-soothing and positive self-talk (Panagopoulos & Ricciardelli, 2005; Duff et al., 2007), managing body temperature and consuming water, and taking rest breaks from physical activity (Allott & Redman, 2006; Leslie et al., 2016; Panagopoulos & Ricciardelli, 2005).
Planning and Preparation
Sixteen studies (69.57%) reported on the ways that planning and organization, information seeking, and sourcing MDMA helped people to mediate harms (Allott & Redman, 2006; Barratt et al., 2014, 2018; Black et al., 2008; Day et al., 2018; Dietze et al., 2015; Dilkes-Frayne, 2014; Duff et al., 2007; Gascoigne et al., 2004; Johnston et al., 2006; Leslie et al., 2016; Panagopoulos & Ricciardelli, 2005; Peacock et al., 2019, 2021; Pennay & Moore, 2010; Sindicich & Burns, 2011). Learning more about MDMA by asking peers and assessing various sources on the internet was considered a viable and useful harm reduction strategy, and also enabled people to enhance the benefits of MDMA (n = 10, 43.48%) (Allott & Redman, 2006; Barratt et al., 2014, , 2018; Black et al., 2008; Day et al., 2018; Duff et al., 2007; Gascoigne et al., 2004; Johnston et al., 2006; Peacock et al., 2019, 2021). Drug forums and websites with peer-to-peer information sharing (e.g., “Pillreports” and “Bluelight.org”) were often cited as popular and trustworthy (Barratt et al., 2014, 2018; Duff et al., 2007; Gascoigne et al., 2004; Peacock et al., 2019).
Health service websites were accessed to investigate harm reduction techniques such as preloading and postloading (Allott & Redman, 2006; Duff et al., 2007; Gascoigne et al., 2004; Peacock et al., 2021). Online technologies were further used to purchase drug testing kits and preloading and postloading products (Allott & Redman, 2006; Peacock et al., 2021). Seeking information from drug suppliers about the content and purity of drugs sold as MDMA was also commonly reported (n = 9, 39.13%) (Allott & Redman, 2006; Barratt et al., 2018; Black et al., 2008; Day et al., 2018; Duff et al., 2007; Gascoigne et al., 2004; Johnston et al., 2006; Peacock et al., 2019, 2021).
The planning of reciprocal relationships with others was also seen to negotiate better access to pure, consistent supplies of MDMA (n = 7, 30.43%) (Allott & Redman, 2006; Dilkes-Frayne, 2014; Duff et al., 2007; Leslie et al., 2016; Panagopoulos & Ricciardelli, 2005; Pennay & Moore, 2010; Sindicich & Burns, 2011). Mutual rapport between supplier and purchaser was perceived as reducing the likelihood of being sold poor-quality substances (Duff et al., 2007; Leslie et al., 2016; Panagopoulos & Ricciardelli, 2005). Friends also established norms of not buying MDMA off people they did not know (Dilkes-Frayne, 2014; Duff et al., 2007; Panagopoulos & Ricciardelli, 2005). Some peers decided to buy MDMA in bulk from trusted sources to receive higher-quality substances and avoid adulteration by lower-level suppliers (Leslie et al., 2016; Panagopoulos & Ricciardelli, 2005; Sindicich & Burns, 2011). Other planning-type practices included arranging money to get home safely and to have available for the following day (Panagopoulos & Ricciardelli, 2005), and choosing safer transport options, including avoiding driving after consuming MDMA, not traveling in the car with someone drug-affected, and using rideshare companies (Dietze et al., 2015; Panagopoulos & Ricciardelli, 2005).
Testing Drugs
Twelve studies (52.17%) reported on practices of drug checking, largely involving the use of reagent kits, to find out the content and purity of what was believed to be MDMA (Allott & Redman, 2006; Barratt et al., 2014, 2018; Black et al., 2008; Day et al., 2018; Duff et al., 2007; Johnston et al., 2006; Leslie et al., 2016; Panagopoulos & Ricciardelli, 2005; Peacock et al., 2019, 2021). The proportion of participants who had used reagent kits varied between studies (Johnston et al., 2006; Peacock et al., 2021), with mixed levels of confidence interpreting test results (Duff et al., 2007; Johnston et al., 2006). Panagopoulos and Ricciardelli (2005) also noted visual and taste inspections of drugs for signs of adulteration. Two studies reported participant responses to test results, including spreading out doses longer than usual, and consuming a test dose due to suspicious results (Leslie et al., 2016; Peacock et al., 2021).
Friends also played a significant role in testing drugs and sharing test results (n = 5, 21.74%) (Duff et al., 2007; Johnston et al., 2006; Leslie et al., 2016; Peacock et al., 2019, 2021). Peacock et al. (2021) found that of the 36% of their sample who had tested their drugs, 52% had another person conduct the test on their behalf, and for those who conducted the test themselves, 29% reported the results to peers and 11% to their supplier. Moreover, some peer networks had a designated “tester” who shared their results with others before communal drug consumption (Duff et al., 2007; Johnston et al., 2006; Leslie et al., 2016).
Accessing Health Services
Twelve studies (52.17%) reported participants accessing conventional health services to seek support for MDMA and other drug use (Allott & Redman, 2006; Barratt et al., 2018; Black et al., 2008; Duff et al., 2007; Dunn et al., 2006; Gascoigne et al., 2004; Panagopoulos & Ricciardelli, 2005; Sindicich & Burns, 2011, 2015; Sindicich et al., 2016; Southey et al., 2020; Uporova et al., 2018). Medical services were the most common service type, including general practitioners, dentists, ambulances, and hospital admissions (n = 8, 34.78%) (Barratt et al., 2018; Black et al., 2008; Dunn et al., 2006; Gascoigne et al., 2004; Sindicich & Burns, 2011, 2015; Sindicich et al., 2016; Uporova et al., 2018). Of lesser prevalence was access to mental health and outreach services such as counselors, psychologists, psychiatrists, and social workers (n = 6, 26.09%) (Allott & Redman, 2006; Black et al., 2008; Dunn et al., 2006; Gascoigne et al., 2004; Sindicich & Burns, 2011; Uporova et al., 2018). Interestingly, accessing peer-led harm reduction programs was only reported in one study (Duff et al., 2007). The reviewed literature framed the act of accessing health services as a form of help seeking, reflecting the personal autonomy of people who use MDMA to care for their health in a way that they see fit. However, specific reasons or motivations for accessing these services were not explicitly outlined, thereby highlighting a knowledge gap.
Community Care
Five articles (21.74%) reported on the way that peer groups shared information and cared for one another (Allott & Redman, 2006; Duff et al., 2007; Leslie et al., 2016; Panagopoulos & Ricciardelli, 2005). People with more experience were cited as being well-respected and listened to (Allott & Redman, 2006; Duff et al., 2007; Leslie et al., 2016; Panagopoulos & Ricciardelli, 2005), and were called upon to assist in emergencies and support the group (Panagopoulos & Ricciardelli, 2005). Additional care practices involved having a sober driver and/or friend present, dosing at the same time, taking one another home, keeping friends walking and breathing, administering first aid, keeping an eye on one another, not leaving friends alone, calling an ambulance, not providing drugs to friends already intoxicated, notifying others of their whereabouts, reminding each other to drink water, and monitoring one another's temperature (Panagopoulos & Ricciardelli, 2005). Exclusionary group practices also served a protective function of not accepting higher-risk drug use in the group, and not disclosing their drug use to strangers who could be undercover police (Dilkes-Frayne, 2014; Panagopoulos & Ricciardelli, 2005).
Discussion
Given the importance of taking a holistic approach that considers both risk and protective factors and foregrounds lived experiences, this review aimed to identify Australian literature reporting on the harm reduction practices adopted by people who use MDMA, and to map what is known about the protective factors at play for those engaging in these activities. We identified five dominant themes across the literature, including the importance of harm reduction practices related to drug consumption, planning and preparation, testing drugs, accessing health services, and community care (Table 4). These themes offer a clearer picture of the evidence supporting the practice of harm reduction strategies by people who use MDMA in Australia.
This review reports on practices that were identified as harm reduction strategies by the authors of the literature reviewed and by people who use MDMA. It was not our intention to “fit” the data within a theoretical framework or directly to better understand the behaviors of people who use MDMA, although we acknowledge the latter's value for future research. In aligning with scoping review methodology, an assessment of the quality of various studies included in the review was not undertaken, and we therefore have not sought to evaluate the reliability of this evidence. Our findings demonstrate practices that people who use MDMA engage in, but do not suggest a complete nor generalizable framework that holds relevance for all user communities. The review constrained the search terms to focus on people who use MDMA instead of other drugs associated with party settings to keep the research within a manageable scope. While the search strategy aimed to collect all relevant terminology related to the research question, it is acknowledged that other definitions may have existed outside the parameters of the review, and not all relevant literature may have been collected. The themes generated in this review reflect both how Australian literature has reported on harm reduction strategies, and how participants in these studies portrayed their practices of harm reduction as relational and contingent on various technologies, services, and social networks.
An overarching theme was the role of peers in sharing information, both in-person and online, and fostering a culture of care. These findings were consistent with international literature (Anderson et al., 2019; Hunt et al., 2010; Van Havere et al., 2015; Van Schipstal et al., 2016). Some researchers have also interpreted online technologies, including peer forums, as an opportunity for AOD organizations and governments to capitalize on the possibility of circulating more precise, preventative messages in the hope of disseminating credible drug safety information and health warnings to people who could benefit (Adley et al., 2023; Barratt et al., 2014; Duff et al., 2007; Gascoigne et al., 2004; Measham, 2019; Measham & Turnbull, 2021).
Utilizing reagent testing kits was another widely adopted strategy for seeking information on the content and purity of drugs sourced as MDMA, with findings suggesting that people who use drugs would be receptive to health advice from a peer workforce delivered in a culturally safe setting, such as Australia's DanceWize programs, and the CanTEST fixed-site drug checking pilot in the ACT (CAHMA, 2022; Duff et al., 2007). Moreover, existing literature on drug checking pilots at Australia's Groovin the Moo festival in the ACT have indicated that people will discard their “MDMA” at the advice of health professionals when there is an indication that the substance may be dangerous (Makkai et al., 2018; Olsen et al., 2019; Vumbaca et al., 2019).
Overall, participants of these studies took care to identify and reduce unwanted harms. Some of these strategies may not always result in decreased harms—rather, we interpret them as reflections of the ways in which people act toward drugs within broader social and cultural contexts of drug use and drug prohibition. For example, while polysubstance use is often framed as harmful (including in many of the sources we reviewed) and indeed can increase the risk of harms experienced, it is important to recognize an alternative narrative around the functionality and relevance of combining certain substances to alleviate harms. For people who use MDMA, the use of licit and illicit substances before, during, and after drug consumption may take on a protective function in practices of harm reduction.
It is important to recognize that knowledge of harms and harm reduction may not always translate to action. In Duff’s (2008) words, “drug use ought to be understood as a complex and heterogeneous assemblage of risks, conscious and unconscious choices and decisions, physical and psychical sensations, affects, corporeal processes, structural and contextual forces” (p. 385). With all drug consumption experiences, harms and pleasures are co-produced by a multitude of different human and nonhuman actors, such as police, peers, temperatures, water, other substances, drug information, transport options, stigma, rural or isolated locations, and the availability of drug checking or other health services (Dilkes-Frayne, 2014; Duff, 2013; Rhodes, 2002, 2009). We suggest that policy reform which adequately considers the complex intra-actions that shape harms and individual capacities to reduce harms, can facilitate people's agency to look after themselves and their peers.
We identified most of the recommended harm reduction strategies outlined in peer drug education resources, including MDMA resources from DanceWize VIC and DanceWize NSW (HRVic, 2022; NUAA, 2022), with the exclusion of eating 30 min before consuming MDMA, considering the “set and setting” of MDMA use and surrounding environments, and consuming electrolytes during a session. Interestingly, there was no mention in the literature reviewed about people avoiding certain drug combinations, including the use of serotonergic drugs in combination with MDMA, which increases the risk of serotonin syndrome (i.e., serotonin toxicity) (Silins et al., 2007). These gaps between academic knowledge and peer education strengthen the case for improving and consolidating current knowledge, and documenting what people who use MDMA do to take care of themselves and others when choosing to engage in a stigmatized activity such as using illicit drugs (AIVL, 2011; AOD Media Watch, 2022; Link & Phelan, 2006).
Our results should also be interpreted with acknowledgement of the significant proportion of evidence that was produced through NDARC's EDRS studies. There were only 12 eligible records that were not part of NDARC's federally funded Drug Trends program (NDARC, 2022). This highlights the invaluable contribution of the EDRS toward the academic knowledge base and the ways Australians see and hear information about illicit drug use. However, the EDRS is principally funded to monitor illicit drug trends, and its quantitative design cannot fully capture the experiences of being a person who uses MDMA. The overrepresentation of EDRS outputs in our sample also indicates a low prevalence of localized and large-scale research with qualitative and/or quantitative designs. Variations in the questions included in the structured interviews of the EDRS each year, and differences in reporting between jurisdictions, led to the decision to include all eligible EDRS records in the final sample. However, we suggest that what is known about the harm reduction practices of people who use MDMA in Australian literature is largely structured by a single source of evidence, and as such, there is a need for different approaches to researching this population to add to and complement existing knowledge.
This review was conducted following SSDP Australia's research principles, with a reviewer team of peers, students, and young people. The reviewers’ experiences and worldviews shaped how we conducted the review, and the lens through which we interpreted the findings. Interestingly, only one study pointed to the importance of a participatory approach involving co-design and working in partnership with the community of focus (Duff et al., 2007). In a field increasingly valuing the role of peer workers and those with lived and living experience of drug use (Duff et al., 2007; Leslie et al., 2016; Panagopoulos & Ricciardelli, 2005), participation of the communities most impacted by gaps in the service sector is essential to developing meaningful policy change. Research that interprets and constructs meaning in a way that reflects the interests of, and accurately represents the voices of people who use drugs, would contribute significantly to Australian knowledge and greatly inform service reform (McNiff, 2013; Stowe et al., 2022). This is especially the case when considering that people who use drugs are typically alienated from the broader service sector due to their current or previous drug use (AIVL, 2011, 2017; Duff et al., 2007; Link & Phelan, 2006).
The articles in the review which more directly answered the research question with diverse explanations for the ways people who use MDMA keep themselves as safe as possible, all utilized qualitative methodologies, including ethnographic approaches of small focus groups, diary entries, and observational strategies (Dilkes-Frayne, 2014; Duff et al., 2007; Leslie et al., 2016; Panagopoulos & Ricciardelli, 2005; Pennay & Moore, 2010). Yet, all these studies were at least 5 years old. Given that drug markets and drug popularity continue to shift significantly, it may be time to invest in broader research designs whereby drug safety practices are documented for this cohort in a respectful, nonjudgmental way, honoring their expertise as people belonging to a marginalized community.
Conclusion
Ultimately the participants in the articles reviewed actively engaged in a broad range of harm reduction practices to stay healthier and safer, and were generally aware of risks associated with their drug use. The main ways participants mediated the harms and increased the pleasures of MDMA use was by altering their consumption practices, and planning and preparing for substance use. This was largely achieved via pathways of their peer group and websites, including peer forums, where lived experience and experiential knowledges were shared online. A diverse range of drug consumption patterns were also intentionally adopted, such as taking half-doses and not snorting MDMA to avoid over-intoxication. Reagent tests were also utilized to find out about the content and purity of drugs thought to be MDMA, and people reported access to medical, psychological, and other harm reduction services for support. Friends, networks, and suppliers played a significant role in the dissemination of test results, practicing a form of community care.
The review exposed an overrepresentation of large-scale, annual, quantitative studies (e.g., the EDRS), and a lower proportion of study designs, both small and large scale, which centrally answered the research question and utilized qualitative methodologies. We recommend the prioritization of participatory research projects that are co-designed with communities who use drugs, where lateral decision making ensures that research findings align with the experiences of people who use drugs, and that community expertise is valued. Such reasoning may sit outside the parameters of conventional academic wisdom and requires a degree of cultural sensitivity that future researchers need to negotiate, particularly if they do not identify with the community of focus. By engaging in an ethical dialogue, more accurate findings may inform understanding of the risk and protective factors currently at play for people who use drugs (Rose, 1996, 1999, 2004). As user communities often experience alienation from mainstream services, tailoring interventions that meet their needs could be more effective than repeating older patterns, such as predominantly funding law enforcement efforts over health and community initiatives, which has not achieved a zero-harm result for drug use throughout Australia (AIVL, 2011; Link & Phelan, 2006; Ritter et al., 2013).
Supplemental Material
sj-docx-1-cdx-10.1177_00914509231214342 - Supplemental material for A Scoping Review of Australian Literature on People Who Use MDMA and Their Harm Reduction Practices
Supplemental material, sj-docx-1-cdx-10.1177_00914509231214342 for A Scoping Review of Australian Literature on People Who Use MDMA and Their Harm Reduction Practices by Chloe Span, Baillee Farah, Nathan Ivetìc and Oisin Stronach in Contemporary Drug Problems
Footnotes
Acknowledgments
SSDP Australia and SSDP UniMelb are both independent, largely unfunded entities that operate via the commitment of student volunteers. This unfunded research was supported by the Masters of Social Work program at the University of Melbourne as part of the first author's qualification. We are also very grateful to the project advisory committee, Dr. Amy Peacock, Dr. Kate Seear, and Dr. Steven Bright for their generous pro bono academic guidance and advice. We would also like to acknowledge people who use MDMA and other drugs, who hold a wealth of knowledge and wisdom. This includes people who have shared their experiences with researchers and those who continue to grapple with the difficulties of the drug policy landscape and the obstacles it presents to leading a healthy and fulfilling life.
Author Contributions
All authors contributed to the study design and data extraction stages. CS and BF undertook data analysis and all authors reviewed results, while NI populated the data extraction tool. CS prepared the first draft of the manuscript as part of a student research project, and BF and CS edited the manuscript for publication. All authors reviewed, edited, and approved the final version.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.