
Abstract
This paper explores Canadian professionals’ engagement in licit, illicit, and pharmaceutical substance use, their perspectives on what constitutes professional misconduct and conduct unbecoming in relation to substance use, and the dilemmas they face around self-disclosure in the context of professional regulation and social expectations. The study involved semi-structured, dialogical interviews with n = 52 professionals. Key findings are: (i) professionals do indeed use and have a history of using licit, illicit, and pharmaceutical substances, (ii) there is lack of consensus about expectations for professional conduct of substance use in one’s private life and an apparent lack of knowledge about legislation, jurisdiction of regulatory bodies, workplace policy, and workplace rights, and (iii) professionals use high discretion about personal disclosure of substance use to mitigate risk to public reputation and professional standing. Given the real potential for negative consequences associated with self-disclosure of substance use, professionals modify their use to be more consistent with perceived social standards and/or protect knowledge about their use from public disclosure. This can perpetuate assumptions that substance use by professionals is “unbecoming” and risks basing decisions and policies on incomplete and inadequate knowledge. Societally, classist ideologies that position professionals as distinct from non-professionals are reified.
Keywords
Introduction
Regulated professionals’ actions are governed through profession-specific codes of conduct and ethical principles designed to protect the public. Professional regulatory bodies determine what constitutes professional misconduct (ones’ actions at work) and conduct unbecoming (how one appropriately represents the profession in private life). In this article, we explore Canadian professionals’ engagement in substance use and the dilemmas they face around self-disclosure in the context of professional regulation and social expectations. Professionals are typically defined as being members of a profession-specific society, association, college, and/or regulatory body; subject to a code of professional ethics or code of conduct; and/or subject to professional licensure or accreditation. Substances “act on biologic systems at the chemical (molecular) level and alter their functions” (Katzung et al., 2019, p. 2), encompassing a variety of substances (i.e., medicines, poisons, foods, drink) used in everyday life (South, 1999). “Licit substances” refers to those legally available (e.g., alcohol), though they are not always used in accordance with law (e.g., underage drinking). “Pharmaceutical substances” refers to prescription and over-the-counter formulations, though these may be criminally distributed and/or used without medical management. “Illicit substances” are those criminally produced and/or distributed.
Professional Regulation of Personal Conduct
In Canada, regulated professionals are often licensed members of discipline-specific provincial legislated regulatory bodies. In the contemporary context, there is increasing perception of a need to protect the public from professionals (Adams, 2020; Salyzyn, 2014) and legislative measures are put in place to regulate the conduct of professionals. For instance, flight crew members, such as pilots, are prohibited from engaging in their role on an aircraft within 12 hours of consuming an alcoholic beverage, under Canadian Aviation Regulations (SOR/96-433) (2022). Lawyers face unique expectations around responsibility to the public. For instance, when it has been determined a lawyer has “improperly conducted himself or herself” through negligence or caused costs to be incurred without reasonable cause or as a result of undue delay, they may be held personally responsible to pay litigation costs (Salyzyn, 2014).
The literature acknowledges that health professionals’ conduct is uniquely scrutinized as their practices can directly cause harm, injury, damage, and even fatality (Currie et al., 2019). Examples of professional misconduct related to substances in the health professions include misappropriating controlled substances (e.g., Discipline Committee of the College of Nurses of Ontario, 2019), producing a controlled substances (e.g., College of Registered Nurses of Manitoba, 2016), misappropriating a narcotic intended for a client (e.g., Discipline Committee of the College of Nurses of Ontario, 2018a), practicing while intoxicated (e.g., Discipline Committee of the College of Nurses of Ontario, 2018b), and being subject to a criminal charge related to substance use or distribution (e.g., College of Occupational Therapists of Ontario, 2018).
Regulatory bodies of health professions have a duty to protect the public by governing and monitoring professionals’ practice (Adams, 2020). When allegations or concerns arise about a professional’s suitability to practice (e.g., guilty of criminal charges, competence, fitness to practice, adherence to professional ethics and standards of practice, abusing a client), and/or failing to uphold licensing responsibilities (e.g., adherence to quality assurance protocols), the professional may be subject to a disciplinary process involving an investigation and/or hearing. Disciplinary hearings of regulatory bodies are legally binding processes that determine whether or not a member is guilty of professional misconduct and, if so, what penalty the member will face (Law Reform Commission of Saskatchewan, 2017; Legal Profession Act, 2004 , c. 28, s. 1). Penalties for such conduct range broadly, such as engaging in professional development, having one’s professional license suspended, abstaining from alcohol and drugs, restricted practice, payment of costs, or revocation of membership.
Conduct unbecoming is classified as professional misconduct that reflects expectations of moral responsibility and occupational loyalty. A description of conduct unbecoming is provided by the College of Registered Psychotherapists of Ontario (CRPO) Standard 1.5: “Members […] conduct themselves privately and in the community in a manner consistent with the values, beliefs and standards to which they adhere professionally…Actions outside the practice of psychotherapy may be regarded as unbecoming a member of the profession, reflecting poorly on the member’s integrity and the profession as a whole” (2021, para. 3). Furthermore, it is expected that “members at all times refrain from conduct that, having regard to all the circumstances, would reasonably be regarded by members as disgraceful, dishonorable, unprofessional, or unbecoming a member of the profession” (College of Registered Psychotherapists of Ontario, 2021, para. 6). Criminal charges related to substance use may be related to conduct outside work hours, but are argued to be relevant to professional conduct. Arguments about the relevance of criminal charges of driving under the influence include, a “lack of self-discipline which is an important part of being a member of a self-regulating body” (Discipline Committee of the College of Nurses of Ontario, 2017a, p. 4) and “serious concerns about a member’s judgment and concern for others” (Discipline Committee of the College of Nurses of Ontario, 2017b).
In Canada, decisions of hearings are generally posted publicly on the regulatory body website. An example of conduct unbecoming involves a lawyer who was disciplined for conduct unbecoming following an incident when he consumed alcohol prior to driving a motor vehicle, caused an accident, removed a can of beer from his car to dispose of it, and used mouthwash to mask the smell of alcohol. It was argued by the Regulatory Body that “[t]he attempt to mask the smell of alcohol on his breath with the use of mouthwash and the attempt to dispose of the open can of beer were done to avoid facing the consequences of performing a breathalyzer test” (Law Society of British Columbia, 2005, pp. 11–12). This was considered “irresponsible” and to have “eroded” “public confidence in the administration of justice and in the legal profession” (Law Society of British Columbia, 2005, p. 12).
Currie et al. (2019) suggest that professional misconduct be viewed as a continuum ranging from “actions that are illegal (prohibited by criminal and civil laws) to actions that are unethical (contrary to societal norms and expectations) or unprofessional (against professional codes of conduct and protocols)” (p. 152). This marks a shift from what they see as definitions of professional misconduct that assume internalization of moral responsibility for the greater societal good, “normative value” arising from a particular social role, and expectations of occupational loyalty (Currie et al., 2019, p. 152). Expectations around occupational loyalty muzzles professionals from voicing criticisms and advocating for social justice and rights (Mertz, 2020). For instance, a nurse was found guilty of professional misconduct in 2016 when she posted comments on her personal Facebook page about the quality of care her grandfather received while admitted to hospital, along with advice to the public. She also used Twitter to share information with Saskatchewan’s Minister of Health and the Saskatchewan Opposition Leader (Strom v Saskatchewan Registered Nurses’ Association, 2020). This decision was overturned in 2020 after appeal to the Court of Appeal for Saskatchewan, who concluded the nurse “posted as a granddaughter who had lost one grandparent…Although she identified as a nurse and an advocate, she was not and did not purport to be carrying out her duties as a nurse” (Strom v Saskatchewan Registered Nurses’ Association, 2020, para. 167).
The concept of conduct unbecoming raises questions around how professionals are expected to comport themselves outside work hours. One teacher was found guilty by the British Columbia College of Teachers of conduct unbecoming for “careless and reckless use of a firearm by firing it over the heads of his sons,” which was later overturned by the Supreme Court of British Columbia (Supreme Court of British Columbia, 2013, para. 7). The College argued this: “a teacher is a professional who occupies a special role in the community, and a standard of conduct higher than that required of to [sic] an ordinary citizen is to be expected of a teacher. The public depends on the teaching profession to meet this standard for the health of society. The community expects that teachers will both teach and personally conduct themselves in a manner consistent with their teaching” (Supreme Court of British Columbia, 2013, para. 30). Despite overturning the decision, the judge concurred with the argument that “there is off-duty behavior for which teachers should be subject to discipline in view of their position as role models” (para. 39) and took into consideration whether there was evidence that a “private matter was made public” (Supreme Court of British Columbia, 2013, para. 44).
In March of 2022, two hearings of “good character” were held regarding applicants to the Charter Professional Accountants of Ontario where it was determined the applicants failed to establish being a person of good character; one person was refused membership (Charter Professional Accountants of Ontario, 2022a) and one person was invited to re-apply the following year (Charter Professional Accountants of Ontario, 2022b). It was purported that the good character requirement protects members of the public, ensures the accounting profession “maintains a reputation for high professional and ethical standards” (Charter Professional Accountants of Ontario, 2022a, p. 26), and demonstrates that CPA Ontario effectively regulates chartered professional accountants (Charter Professional Accountants of Ontario, 2022a). Drawing on the definition of good character in Law Society of Upper Canada v Preya, 2000 CanLII 14383, it was stated: “Good character connotes moral or ethical strength, distinguishable as an amalgam of virtuous attributes or traits which undoubtedly include, among others, integrity, candour, empathy and honesty” (as cited in Charter Professional Accountants of Ontario, 2022a, p. 25). Citing criteria of good character outlined by Madam Justice South of the British Columbia Court of Appeal, good character is: 1. An appreciation of the difference between right and wrong; and 2. The moral fiber to do that which is right, no matter how uncomfortable the doing may be and not to do that which is wrong no matter what the consequences may be to oneself; 3. A belief that the law at least in so far as it forbids things which are malum in se must be upheld and the courage to see that it is upheld. (Charter Professional Accountants of Ontario, 2022a, p. 25)
Risks Associated With Disclosure
There are significant gaps in knowledge about substance use by professionals. Prevalence and patterns of substance use by professionals tend to be similar to matched non-professional comparison groups (Cottler et al., 2013; Hughes et al., 2002; Kenna & Wood, 2004; Kunyk, 2015); however, the majority of previous studies pertain to physicians, nurses, pharmacists, and dentists, while other professions are underrepresented and studies outdated. Among all professional groups, studies about self-reported effects of substance use or reasons for use tend to be informed by participants involved in treatment programs, neglecting the general population of professionals (Kiepek & Baron, 2017).
Public disclosure of substance use is acknowledged to pose a dilemma (Ross et al., 2020). On one hand, non-disclosure of substance use silences complex understandings and reifies perspectives that may continue to marginalize and Other (Ross et al., 2020). On the other hand, disclosure risks “social, professional and criminal sanctions” (Ross et al., 2020, p. 2). Indeed, professionals are reluctant to disclose substance use due to concerns of punishment, discipline, and negative appraisal (Lillibridge et al., 2002; Monroe et al., 2013). Findings from our previous research indicate that professionals and students in profession program are disinclined to disclose personal substance use due to a concern of negative judgment from others, such as being viewed as unprofessional, incompetent, and unsuitable for a professional role (Kiepek & Beagan, 2018). It is clear that when professionals’ personal conduct outside work is viewed by their regulatory body to contravene an expectation of particular moral and ethical values, professionals may have their membership revoked and subsequently lose the opportunity to retain employment in that job. Organizations may also hold employees accountable to standards of conduct outside of work, espousing an belief that employees should behave outside work in such a way that upholds the integrity of the workplace (Kaptein, 2019). Asymmetries between “professionals” and citizens extend beyond demarcations of formal knowledge and expertise (Harrits, 2016) to expectations of differential conduct in self presentation in person and on social media, including attire, style of interactions with others, and expression of opinions (Furnham et al., 2013; Packer et al., 2008; Weijs et al., 2017). As such, professionals may conceal aspects of their personal conduct and beliefs that do not conform with societal norms about professionals. Such expectations are increasingly extending beyond regulated professions, particularly those that are high profile in society, such as professional athletes and politicians; though through social media, a spotlight can shine on any person (Robards & Graf, 2022).
A result of non-disclosure is that certain experiences are hidden and silenced. Walker (2021) writes about the missing “I” in substance use research and positions herself as a person who uses substances as well as a researcher. She acknowledges self-disclosure as a “privilege” which she is afforded in her position as a “tenure-protected, white, cis-gender, middle class professional,” who lives in a relatively politically progressive region (p. 4). Although self-disclosure can pose a risk, due to social stigma and the criminalization of drugs, she reflects that having a “choice” whether to conceal or disclose use is not an equal opportunity for all people. The consequences of self-disclosure for many can be too high in contexts of “prohibition, medicalization, and professionalism reinforcing a cultural silence that itself sustains problematic assumptions and misinformation about drug use” (Walker, 2021, p. 2).
It is within this context we explored substance use by professionals, their perspectives on what constitutes professional misconduct and conduct unbecoming in relation to substance use, and the degree to which they disclose personal substance use. The research objectives were to better understand the distinct ways in which substances are used among professionals and the profession-specific factors that contribute to professional socialization regarding acceptable and unacceptable forms of substance use. The intent of our study was to uncover diverse experiences and perspectives regarding substance use among a professional population and to create space for concealed opinions and practices to be shared. We sought to understand types of substances used, frequency of use, impact on performance and experience, risk factors and protective factors that influence substance use, and factors of professional socialization that influence and/or reinforce substance use.
Methods
This funded study received ethics approval from the Dalhousie University Research Ethics Board. The interview findings reported here are part of a larger, mixed methods study that involved data collection using (i) survey, (ii) ecological momentary assessment (EMA), and (iii) semi-structured, dialogical interviews with Canadian professionals. N = 516 professionals completed the survey. Recruitment for the EMA and interviews portions occurred at the end of the completed survey and resulted in n = 52 interviewees. Each interviewee completed 3-weeks of EMA data entry, which included two interviews; one during the first week EMA data collection and one within a week of completion. Findings from the broader study are published elsewhere: one focused on meanings of substance use and associated activities (Kiepek, Ausman, et al., 2022) and one focused on gendered experiences (Kiepek, Beagan, et al., 2022).
Recruitment
Inclusion criteria
Professionals identified for recruitment included lawyers, engineers, accountants, nurses, teachers, architects, physiotherapists, speech-language pathologists, audiologists, pilots, paramedics, physicians, chiropractors, optometrists, veterinarians, journalists, occupational therapists, and social workers. Participants identified as professionals, residing in Canada, and 19-years or older. Initially, to be eligible for the interview, interviewees engaged in substance use in one of the following ways: (i) approximately daily use of a non-prescribed psychoactive substance (excluding caffeine only); (ii) non-prescribed used of one or more substances on approximately a weekly basis, or (iii) infrequent (less than weekly) but heavy use (e.g., binge use). Due to challenges with recruitment, we opened eligibility to people who used only caffeine daily, as this population would offer equally valuable perspectives on professional regulation.
Recruitment process
Recruitment for the study involved print and virtual advertising for involvement in a survey about substance use by professionals. Virtual advertising for recruitment included select national and provincial professional associations and societies, advertising through university alumni channels, advertising on the project website, advertisement on social media (e.g., Facebook, Twitter, Instagram), newspaper advertisements (print and online), and snowball recruitment through informant contacts and research participants. Postcard advertisements were distributed to local areas in Halifax, Nova Scotia, such as workplaces. Postcards were also distributed across Dalhousie University campus in buildings where professionals are known to visit campus. Some postcards were also distributed in other places across Canada when the research team would travel. All advertisements provided a link to the project website, and where possible, a copy of the recruitment letter and consent form were included in emails to prospective participants. Interviewees were remunerated $25 per interview.
Data Collection
Interviews took place between November 2018 and August 2019. Questions related to personal use of substances and effects, personal disclosure, and perspectives on professional regulation of substance use. We included questions that sought personal perspectives on professional regulation of substances and, more specifically, about professional misconduct (referring to professionals’ actions at work) and conduct unbecoming (referring to appropriate representation of the profession in one’s private life). We asked interviews to propose recommendations about professional regulations and elicited responses to brief scenarios, such as “If you found out that a colleague in your profession was using marijuana each evening, what would you do? What if they were using cocaine once a month? What would you think if you found out a colleague was using medication for depression or anxiety? When does it become a problem?”
Not all interviewees were available for two interviews, so in these instances, the two interviews were condensed, which resulted in 100 interviews. Research assistants transcribed interviewers using ExpressScribe software, with markers for select prosodic features to assist analysis. Online software was used to randomly generate 2-letter identifiers for interviewees for dissemination purposes.
Analysis
Qualitative analysis of the interviews was shaped by an interest in learning about perspectives on professional regulation and implications for self-disclosure. Initially, the second author deductively coded a selection of 11 interviews using Atlas.ti software. The first author reviewed the coded data and revised the codes to reflect emergent themes identified inductively. The first author reviewed the data to ascertain the effectiveness of the codes, conduct a preliminarily analysis, and inductively identify new codes. The first author then coded all 100 interviews and organized coded data into themes (Braun & Clarke, 2006) in collaboration with the second author, who had in-depth knowledge of the interviews through her roles in facilitating interviews and transcribing. All team members contributed to refining the analysis and presenting the findings.
Results
The results reported here emerged from the interview data alone. The majority of interviewees (n = 52) were regulated health professionals (71.09%) and female (67.92%). The types of professions are provided in Table 1. Interviewees were asked about all current substance use, previous use when a professional, and previous use when a student in a professional program (see Table 2). The most commonly used substances were alcohol, caffeine, pain suppressants, and cannabis. Three of the six people who reported not currently using alcohol did currently use cannabis.
Profession.
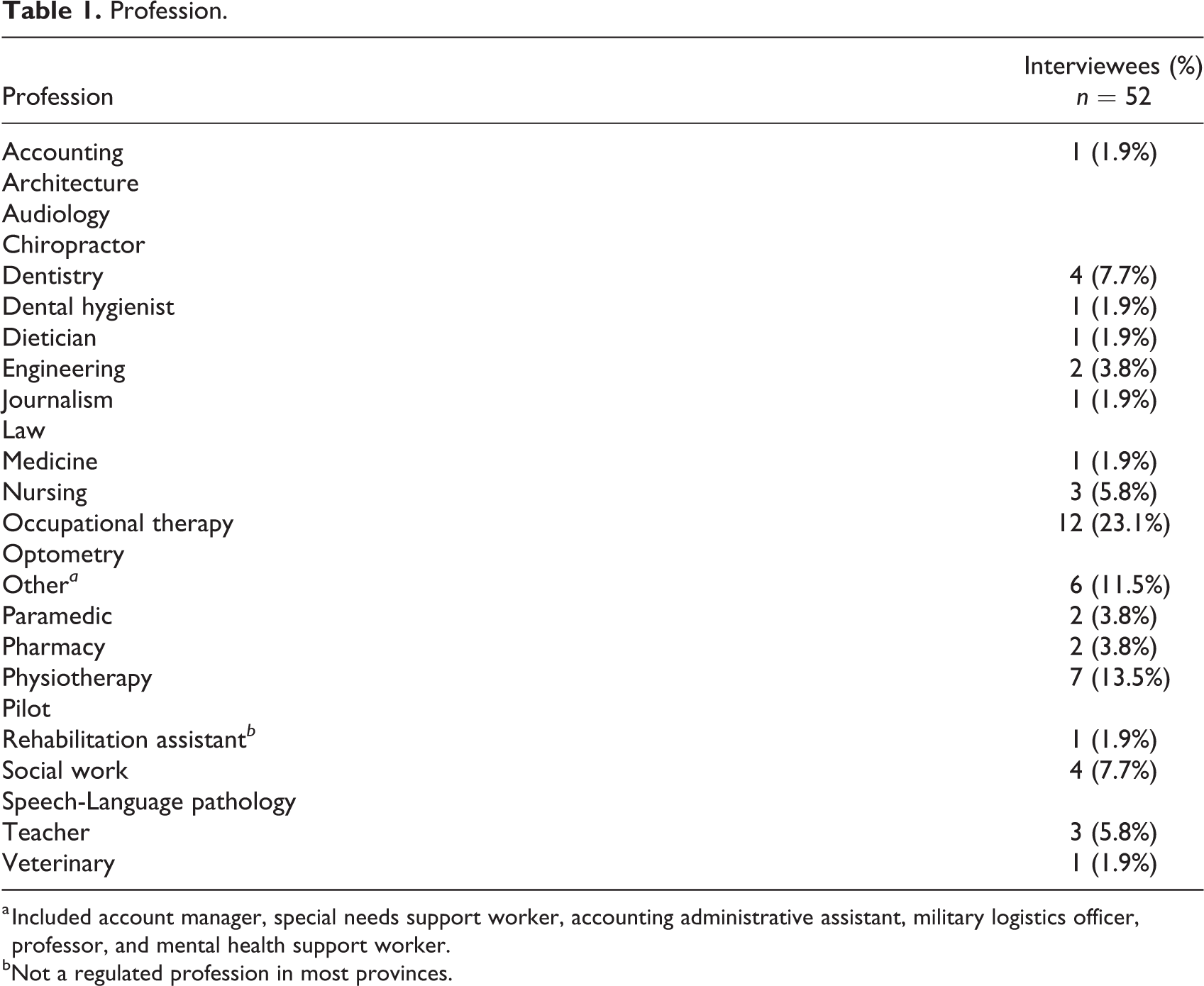
a Included account manager, special needs support worker, accounting administrative assistant, military logistics officer, professor, and mental health support worker.
bNot a regulated profession in most provinces.
Interviewee Current and Past Use of Substances (n = 52).
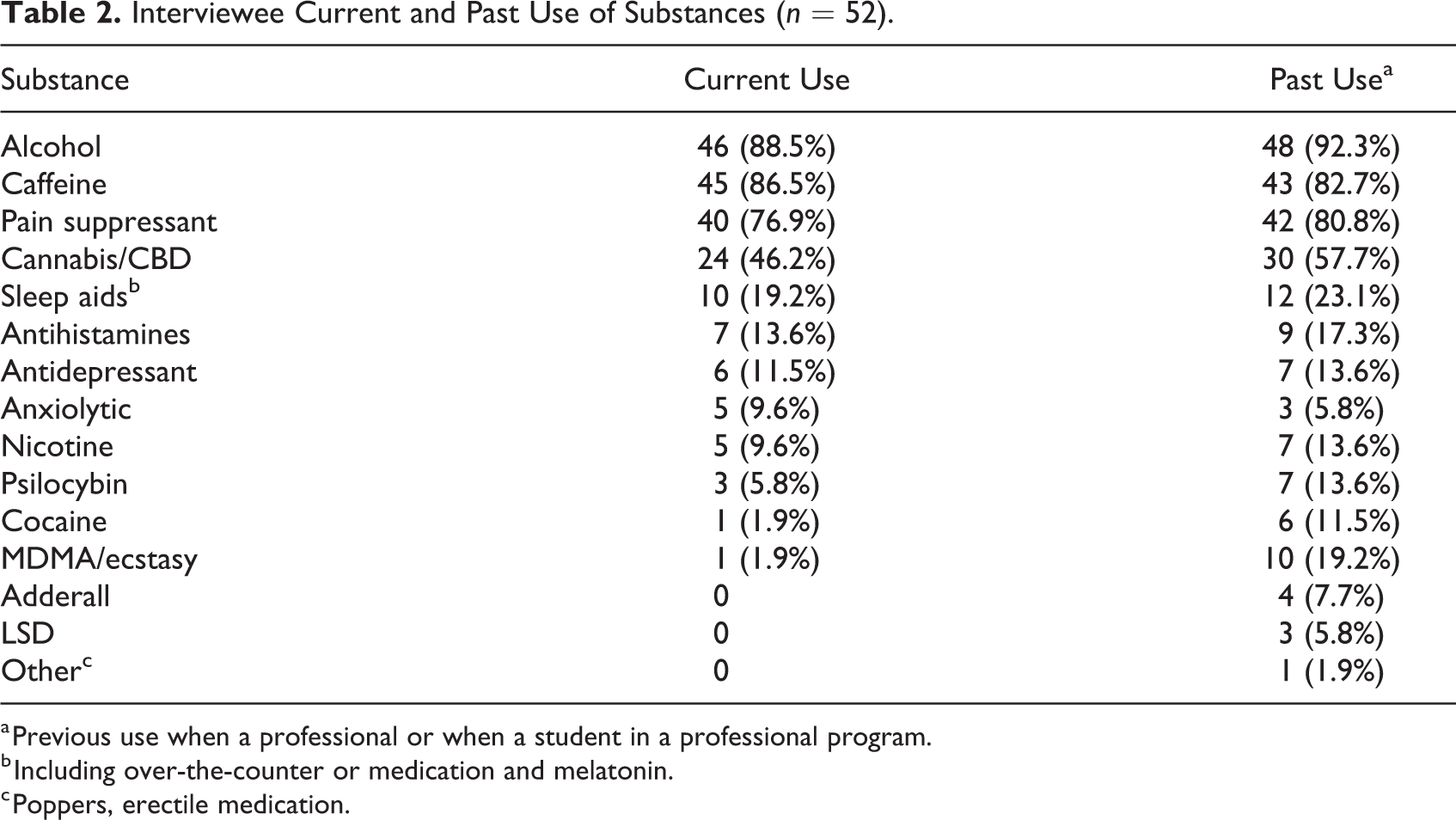
a Previous use when a professional or when a student in a professional program.
b Including over-the-counter or medication and melatonin.
c Poppers, erectile medication.
Perspectives on Substance Use
In general, certain substances are accepted, condoned, and even expected in certain circumstances. Caffeine is typically integrated into workplaces and workplace culture. Alcohol use can be a way to strength cohesion in collegial relationships and can enhance professional networking. Pharmaceuticals, such as sleeping medication, antidepressants, and antianxiety medications were acceptable, but use was less likely to be disclosed.
Cigarettes, even among interviewees who smoke, were viewed less favorably. Interviewee JK said, “I think of cigarettes almost like dirty and I feel like somebody in that high of a position…they’re like a role model. If you are doing that, then you should be hiding it.” Cigarettes were positioned by this interviewee as reflective of “lower class”; “it’s always viewed negatively. More people spending money on cigarettes, it’s bad for your health, and it’s very surprising to see someone in a good job, educated position, and they’re a smoker…people view it as ‘you know better’. You shouldn’t be smoking. Especially somebody like doctors.”
Class positioning of substances was mentioned by other interviewees. Interviewee BX observed “it’s much cleaner in a lot of ways to show someone holding a Starbucks latte than it is to show them smoking a cigarette. Culturally, here and now. One is seen as being much more upper class, which you associate much more with professional life, one is seen less” and “people see drinking wine as classy, currently, a lot more than smoking cigarettes. Cigarettes are dirty.” Expectations that professionals should uniquely control their use of substances was also presented as a classist belief, distinguishing “good people and bad people,” where “bad people are the ones who use substances and that’s why they occupy the positions they do socially” (Interviewee HD).
Interviewee BX provided an interpretation of how substances are viewed in relation to one another, that captures many of the complexities discussed across interviews: [cannabis is] in between cigarettes, coffee, and cocaine. It’s like that awkward triangle in that it was illegal so it’s like cocaine, but it’s not anymore so it’s not quite there. And it’s [used by] smoking which is bad for you, which is like cigarettes, but it’s seen as not quite as bad because there’s not as many chemicals, so it’s not quite there yet. And it’s recreational so it’s like alcohol or caffeine, but it was illegal, so it’s not quite there yet. It’s kind of stuck in the middle where it hasn’t quite figured out which category it’s like enough yet to know whether or not it’s acceptable.
This quote also captures, in general, the social positioning of particular substances as more or less socially acceptable.
Alcohol use was said to be ubiquitous in personal social contexts during the time interviewees were enrolled in professional education programs, with binge drinking being a norm. Professional programs were perceived as intensive and stressful, with alcohol serving as a means to relax and unwind. However, after entering professional employment, the majority of interviewees shifted to more “mature” forms of substance use, which might involve abstaining from certain substances, reducing amounts use (e.g., refraining from binging), and using less frequently. Several factors contributed to these changes, such as less tolerance for adverse effects and increased personal responsibilities; however, expectations about how substance use relates to a professional image was an influential factor. Interviewee MO described, “it’s an evolution that happens while you’re obtaining your training, and once you get your license, and your first years’ practice. Modifying who you are from a student to a young professional and accepting the responsibilities that come along with it.”
Professional Conduct in Private and Public Contexts
The interviews elicited perspectives about what it means to be a professional and how one’s private life is conceptualized. Some people felt that professionals’ personal and private lives should be distinct, whereas others thought professional values should consistently inform decisions in one’s private life.
A contested topic was the degree to which a person’s professional and private life intersect. Some people were adamant that their professional and personal lives were completely distinct and separate. Interviewee LW stated, “It should be at work, versus not at work, versus when I’m on the clock, versus in my own personal time.” Interviewee HC shared a similar perspective, saying, “When I’m at work I’m a [professional], I’m the utmost professional, I will do everything that I need to be, I will do it by the book, by the line, whatever. When I’m outside of work, I may be a [professional], but I’m still a person, I’m still a human and I like to participate in recreational activities.” Several interviewees used the term “human” as a distinction from expectations pertaining to one’s professional role [Interviewees BX, QS, TT, CS, EW, AW, MF], such as “during the day, when you are in a professional job as a professional, then of course you are a role model…but when you come off the clock, you know, you should be allowed to be human again” (Interviewee CS).
Others saw these boundaries as more nebulous, as described by Interviewee BX: “doing something outside of work when you have a professional image that you have to uphold—we live in a society where you cannot keep your world separate…so that blending is going to happen and part of being a professional is being prepared for that blending to happen.” Other interviewees shared this belief, stating, “You’re pretty much always on duty. You’re always representing yourself and your profession” (Interviewee AO), “You’re you but you also are your profession. That’s part of who you are” (Interviewee TQ), and “it would be really nice to say my work life and my private life are absolutely 100% separate, but they’re not because I’m in the middle of both of them right? I’m the connection between those two things and they can effect each other” (Interviewee IT1).
Interviewees discussed the complexities of distinguishing between the professional and the private, saying, “I think there still needs to be a distinction that we’re a professional but we’re still a person. We do treat ourselves as professionals twenty-four seven, but we are still, people as well” (Interviewee AU). Interviewee ML argued, “there definitely needs to be a line. You can’t be expected to be on all the time…there’s gonna be divide between your personal and professional life…Like say…three thirty or four o’clock when you walk away from work and just be clear of it, but that’s not the reality of it. Especially if you’re doing it in your personal life…that’s being seen by the public.” Interviewee CF noted the importance of “upholding this level of integrity,” elaborating, “it’s really hard to draw a line there in what is considered appropriate for your own personal life without always feeling like your life is being dictated by your work or by your profession.”
There was a general perception that professionals are held to a “higher standard than the average person” (Interviewee TT) in all areas of their life, attributed “automatic trust” (Interviewee VY), expected to be “perfect role models” (Interviewee HC), and expected to comport ones’ self at “a level of perfection” (Interviewee BX). A number of interviewees countered that professionals are no different from anyone else, as exemplified by Interviewee QS who said “everybody’s human. Some people will take professionals above, thinking ‘well they’re professional so they’re different’, well they’re not.” This person elaborated that the public should be aware and understand that “everybody’s the same and you will see problems with professionals just as much as you will see problems with people who sweep the floor.” Comparisons were made to other unregulated professions; for, instance, postal delivery employees work in the public eye, carpenters’ jobs require high competence, and heavy machinery operators’ jobs are associated with risk. Several people argued against higher expectations around professionals as reflective of artificial social bias against trades or blue-collar work, which undervalues social contributions and social standing.
Others spoke of professionals as being entitled to engage in the same types of activities as everyone else. Interviewee EW declared, I think that people do look up at police, nurses, social workers, all those kinds of professions as being role models. We need to recognize that everyone is human and everyone is entitled to their own personal life. Maybe we look up to that person and their professional role, or maybe that person is someone who is really respected in our neighborhood, but doesn’t mean that they’re not allowed to have their fun and make their own choices.
Interviewee QF went so far as to say, “people think that you put on a white coat and you’re magically somehow not vulnerable to the same things they are. Or too up your own ass to enjoy things they would enjoy. There’s a certain ‘oh but you’re a [professional]. You should know better. You should be above that.”
Some professionals felt expectations of higher standards were warranted: there is a carry-over into your own personal life that hopefully the values that you hold and uphold during your work environment are also things that carry-over outside of the work environment.…we have a certain kinda bias that healthcare professionals are supposed to act a certain way or they’re a certain type of personality typically, they’re caring, empathetic, what not…taking substances in excess or inappropriately does say something about who you are and your profession is part of who you are so, yeah, I would say it’s important that the values transcend between domains. (Interviewee OI)
Interviewee OE described that as a professional, “you have a responsibility to conduct yourself in a manner that—what’s the word I’m looking for—that’s acceptable I guess?”
There were diverse perspectives on the social positionings of professionals and the standards to which they are held, which influence how professionals view substance use by themselves and other professionals. At the same time, it was apparent that professionals typically had limited knowledge about the effects of substances they had never used and limited knowledge about professional regulations and workplace rights related to substance use. Interviewees perspectives are organized into six general categories.
I really pride myself on eating right and exercising and being mindful health. Being a healthcare professional, a lot of your education and what you’re giving to your clients is all about trying to have a really good state of wellbeing…sometimes I feel guilty when it’s been a couple of days in a row and I’ve had a cup of coffee, ‘cause I know it’s not this ideal state of wellbeing.
Interviewee CF also related substance use to the context of a healthy lifestyle, saying, “if I ever wanted my patients to exercise regularly, I should do the same. When it comes to substance use…I think substance use is encompassed in terms of a healthy lifestyle. So they are linked.” In particular, health professionals were more likely to hold health and wellbeing as a dominant value and felt it was their role as health professionals to model health lifestyles.
there’s not actually a law or anything saying that we can’t be out to the bars or drinking or anything, but it’s almost like—what is the word I’m looking for—a rule of thought that you shouldn’t do this. It’s just like, you’re not supposed to do this. Because, if it gets back to like the boss that you’ve been out to the bar and you saw clients, it just looks really bad. There is no law but I feel like, it kind of is a law. That you have to be mindful of your drinking and your substance use in public.
According to this perspective, members of regulatory bodies are “always professionals” and expected to maintain a professional image in their private lives. This perspective is reinforced by beliefs that “your private life is not private in many respects” (Interviewee IT), “you’re pretty much always on duty. You’re always representing yourself and your profession” (Interviewee AO), and “It’s not just you anymore you are now a member of this profession” (Interviewee MO). Interviewee MO explained, “at 5 o’clock you don’t leave your profession at the door, we’re licensed professionals and that’s the difference. It’s not a job, it’s a career.” From this point of view, professionals should be allowed to use licit substances, but in “responsible” ways. Binge drinking would be dissuaded, as noted by Interviewee JR: “I think there’s an association of frequent binge drinking with being less responsible.”
While it is expected that professionals might engage in licit substance use, they are thought to have a “responsibility to demonstrate proper behavior…in this case, responsible use of substances” (Interviewee WZ) and not use in ways that are “obviously debilitating” (Interviewee VH). As stated by Interviewee AU, “we’re still people. We’re still allowed to socialize and do things that are socially acceptable and fully legal…I think people know they can’t be complete idiots especially out in the public realm. But that we can go out and do what a normal individual would. We can have wine at supper.”
It is expected for professionals to avoid public intoxication and “be in some level of control of yourself so you’re not doing stupid things” (Interviewee QA). Interviewee CU elaborated, “there’s a high expectation for a professional that they don’t live a social life…That you’re going to have like good morals and respect the ethics of the profession. That like you wouldn’t become impaired.” For the most part, interviewees acknowledged that professionals may not always refrain from intoxication or maintain constant decorum, but at the very least these instances should not be made public. To cross this line is considered “bad judgment” and interpreted as “an ethical problem” (Interviewee TT).
Interviewee WZ explained, our conduct, both at work and in life in general is supposed to be professional…we are expected to conduct ourselves, in the public, in a professional manner. And I think that’s good. I agree with that expectation. It would be embarrassing to me if people in my profession were known as being drunks. I wanna be seen as belonging to a professional organization who, other [members] are conducting themselves in a professional way.
Many people believed that certain substances used outside work hours was an indication of a problem, dangerous, likely to impact on work, and likely to harm the image of the profession, as indicated by Interviewee VG: if I find out that somebody witnessed another [health professional] doing cocaine, I would be absolutely that is not okay. Not on any level is that okay…Because personally I believe that public representation when you are a public servant is paramount to your service…I would have a very large problem with that if the community at large was labelling one of my co-workers as a dangerous consumer. But if it’s something that’s legalized or prescribable and it’s not done to the point where they are bringing detrimental effect into work, I really don’t care about it.
Interviewee QF opined, okay yes. I am a [health professional] and we’re the most trusted profession and blah blah blah blah blah. But, people who are these professionals, your doctor, whomever. We are people. The fact that you wanna cut loose and do whatever on your off time, I think that should be your own damn business. Again, I’m not someone who particularly does that…If you can keep your professionalism, keep your pro face on when you’re at work, then if what you’re doing in your off hours isn’t affecting how you are performing your job, then it shouldn’t matter.
Interviewee XS shared this perspective, saying, “what you do in your spare time, that’s fine, you’re not hurting anyone, you’re relaxing. And by the next morning you’re going to be, you know, ready for work again.” Interviewee QF emphasized the importance of performing optimally, stating, “if I fuck something up someone dies.”
Interviewees in this category tended to adhere to the belief there should be a clear distinction between work and private life, with Interviewee JK asserting, “when I get off at four thirty then that’s private life. That’s my time.” Interviewee EW further contended, “if you wanna go out and do whatever with your friends, and you aren’t at work, and you’re not missing work, you’re not missing things that you’re supposed to be doing, then I think that’s your time. I don’t think my profession owns me. It’s a part of who I am but it is not who I am as an entirety, and I think that it’s unreasonable, um, to kind of put that owning on someone because they’ve chosen a career.”
There were some exceptions to the perspective that all use or effects should occur outside work hours. For instance, some people spoke about having a glass of wine while doing paperwork at home, alcohol was associated with travel and/or conference attendance, with some noting it was an accepted part of “doing business,” and some had experiences of alcohol as a collective fun or special event scheduled into a work day.
Within this category, the general belief was that anything that occurs within one’s personal life, outside work hours, and not negatively impacting work, should be outside the purview of regulatory bodies.
Although these perspectives were presented categorically, many interviewees held multiple, sometimes contradictory beliefs. For instance, certain illicit substances might be viewed as more or less acceptable and certain professionals (e.g., surgeons, teachers) might be expected to comport themselves according to idealized social standards. Absent from rationales within these six categories is an informed integration of specific knowledge about applicable legislation, jurisdiction of regulatory bodies, workplace policy, and workplace rights. Instead, perspectives were largely based on opinion, values, and assumptions.
A number of interviewees, particularly health professionals who used substances, reported perceived benefits of bringing lived experience to their roles, such as increasing empathy, knowing drug-related terminology, and being able to respond to adverse effects. Interviewee DV provides an example, describing personal benefits of psilocybin accordingly: I would say [magic mushrooms] they are the best thing that have happened to my life actually. They have, opened up my mind to mindfulness…and that’s what I’ve been using to get through [professional] school and through all the stresses in my life. It has made life much more enjoyable and easier…it’s very positive for me…also has given me the ability to be able to understand people more. I feel like I am way less judgmental than before.
Personal Disclosure
Although the majority of interviewees conveyed a belief that professionals have the right to a private life, there was nevertheless acknowledgment that public figures do face real consequences associated with public disclosure of certain social transgressions, regardless of whether or not substances are involved. For example, a number of political figures in Canada resigned or were demoted for following personal international travel during the COVID-19 outbreak related to showing “poor judgment” (Williams, 2021), whereas other Canadians did not experience sanctions for similar decisions. Interviewees noted that certain professions are more likely to be exposed to public scrutiny, such as public figures (e.g., journalists, military officers), people in professions that are positioned as role models (e.g., teachers, police), and people whose decisions impact others’ well-being (e.g., pilots, physicians). With respect to certain people being held to higher standard, Interviewee TT noted, “This might not be really fair because people are people and humans are humans. But I think that’s real.” Interviewee OP mentioned that when you are in the “public eye” “it’s hard to separate who you are as an individual without including what your occupation is.”
Professionals in small towns are more visible within communities, so their actions might be more closely monitored. Interviewee AU describes the experiences of teachers in a small town: your student’s teacher would be at the social event too right? I know there were some teachers that would get bugged by parents for going out and having a good time on weekends…I think they’re held to, a behavioral standard as well that is sometimes unrealistic. That people think they should be a role model twenty-four seven, for kids. And not be a regular person. They’re held to that standard in terms of like, twenty-four seven, professionalism to a certain extent.
Interviewee HC provided an account of an incident of self-disclosure of cannabis that impacted employment. Prior to legalization, the interviewee was speaking to a colleague in the staff room about “getting high” in a way that was “a little too cavalier.” As a result, she described: I was taken [aside by a staff member] saying “I heard you had this conversation, I think you should be careful about the kind of things you talk about because we wouldn’t want it to impact your career.” And I was just flabbergasted that I was in a room of adults and talking about something with another adult…Saying that your activities could impact your career? That just blew my mind, and then from then on the [supervisor] would not look me in the eye and that would be the only time that my habits directly impacted my career.
With the potential for negative impacts associated with self-disclosure of substance use, one mitigating strategy is to ensure one’s private life does not become public knowledge. Interviewee IT described this as, “in some ways you’re always representing the organization you work for, but I think we’re also allowed to have a personal life and maybe it’s just a choice about how you choose to portray some of those things. So do you post those things online? Or do you use it in your private life but you’re not sort of overtly advertising some of your use.” Interviewee TQ practiced this type of discretion, noting, if you’re gonna use it, be smart about it. Always portray yourself in a professional manner. I do, in my own home, I’m safe and in my own space, and I don’t let it affect anyone else or my work, or nobody sees it. But I’m using these substances. And it’s under controlled environment. No one from work is seeing this or I’m not posting it online.
Professionals’ social media accounts are carefully curated to both construct a public professional image and retain privacy about anything perceived as contentious, stigmatized, or incongruent with professionalism. Many professionals ensure their social media accounts do not include reference to their profession and many use high privacy settings. A shared perception is that with social media one’s private life becomes public. Interviewees warn that social media should considered public, with Interviewee AO cautioning, “don’t put anything on social media that you wouldn’t be happy to have on a notice board on your front yard facing the world as they drive by” and Interviewee TT advising only posting what “you’d be comfortable with that being on the front page and your mother read[ing] that.”
Interviewees tended to engage in substance use in private settings and with select others. Interviewees said that personal substance use is not asked about in the workplace; “People don’t ask. It’s uncool to ask, that’s for sure” (Interviewee TT), but when imagining how they would respond if directly asked, some said they would lie. Others said they might admit to past use, but not current use. Interviewee HC said that personal disclosure requires “making the decision on what people to trust and what people not to trust…Some colleagues I would put in the range of yeah I would trust you and tell you about my habits, and then others colleagues I wouldn’t tell them anything.” The most common concern was negative judgment from family, friends, colleagues, and the public or that people might make assumptions about their competence at work.
As interviews occurred around the time of cannabis legalization, it seemed conversations about cannabis increased. Interviewers mentioned that more people were openly sharing about their use of substances. People were reported to be less “ashamed to admit” using cannabis (Interviewee WZ) and conversations appeared more casual and less “taboo” (Interviewee AU). Yet, many interviewees who used cannabis said they would engage in these conversations without revealing they used. Interviewee SD revealed, “just because it’s legalized doesn’t mean people are comfortable saying that they either do it or want to do it. That’s same thing with my work, no one really talks about it that much. There’s been a few people where they’ll make jokes and I’ll be like ‘oh I know what you mean’. Sounds like I’m a square. I’m not, at all.”
Interviewees evaded disclosure of illicit substances and most did not disclose use of cannabis use, tobacco, or pharmaceuticals, or patterns of use that do not conform with the image of being a professional (e.g., binging). Interviewee SD was adamant, “I would never tell my family that I did MDMA or mushrooms, I would never tell my co-workers or my bosses, oh my gosh, like, no, no, no. No, I would never tell them that.” Interviewee BX was similarly circumspect about self-disclosure, stating, “put it this way as far as I know you are the only person who knows what medication I’m taking. You and my doctor.” In fact, “hiding use” was viewed in some ways as a professional responsibility, as indicated by Interviewee JK: “people in those kind of positions, it’s almost like they have to live up to their standards. It almost seems like, okay well if they’re gonna do something that doesn’t exactly fit with their roles, like smoking or drinking, I feel like it almost needs to be hidden.”
Within this context of “don’t ask, don’t tell,” it should not be surprising that misinformation and biases about the effects of substances is perpetuated. For the most part, people who do not use particular substances are shielded from the fact that others around them might use. Interviewee JV expressed dissatisfaction with how professionals misrepresent themselves publicly: “Medicine has this culture of like, uprightness…They pretend they’ve always been these upright I-would-never-abuse-a-prescription-drug. People are just full of crap. Like, doctors are full of crap.” This interviewee had positive experiences of using illicit substances, but also they said they would not publicly admit to using, even if directly asked.
There was concern that boundaries between private and public are increasingly nebulous in all areas of life, as described by Interviewee XB: “Whether it be religious or political or drug use or sexual orientation…those private things now matter in ways that they previously didn’t.” In this context, “public representation” becomes “paramount to your service” (Interviewee VG). Professionals are not simply expected to bring a particular set of knowledge and skills to a job, but are expect to demonstrate they are “a stand-up member of that profession” (Interviewee VY) and community.
Discussion
The findings from our study uncover the “nebulous boundaries” between what is “professional” and what is “private.” Key findings deliberated in this discussion are: (i) professionals do indeed use and have a history of using licit, illicit, and pharmaceutical substances, (ii) there is lack of consensus about expectation for professional conduct of substance use in one’s private life and an apparent lack of knowledge about legislation, jurisdiction of regulatory bodies, workplace policy, and workplace rights, and (iii) professionals use high discretion about personal disclosure of substance use to mitigate risk to public reputation and professional standing.
Substance Use Within the Canadian Context
The 2017 Canadian Tobacco, Alcohol and Drugs Survey (CTADS) involved n = 16,349 telephone interviews conducted with residents aged 15 years and older (Government of Canada, 2019a). Our research about substance use among professionals has consistently found rates of past-year prevalence of substance use that well exceed what is reported in the CTADS study (Kiepek, Ausman, et al., 2022; Kiepek et al., 2019). This may, in part, be accounted for by the anonymized nature of our online survey compared to phone interviews conducted by the federal government. In these studies (Kiepek, Ausman, et al., 2022; Kiepek et al., 2019), the most commonly reported substance use effects are positive or non-problematic (i.e., enjoyment, pleasure, relaxation).
Given the real potential for negative consequences associated with self-disclosure of substance use, professionals frequently modify their use to be more consistent with perceived social standards and/or protect themselves from public disclosure. This can perpetuate assumptions that substance use by professionals is “unbecoming” and risks decisions and policies based on incomplete and inadequate knowledge. Societally, classist ideologies that position professionals as distinct from non-professionals is reified.
Workplace Rights
Professionals did not appear to have knowledge about the parameters of regulatory bodies to govern professional conduct of substance use nor workplace rights around substance use, as applied to themselves or their colleagues. Self-regulating professionals have a responsibility to report concerns of misconduct to regulatory bodies. This, compounded by certain erroneous beliefs around substances, can be problematic. Reported separately, our study found that cocaine was used by 7% of Canadian professionals in the past-year and 19.8% ever (Kiepek, Ausman, et al., 2022). Commonly reported effects included socializing enhanced, awake/alert, confidence, and energy increased, with no reports of work performance or missing work obligations. Yet, our qualitative findings show that people who used cocaine did not disclose their use to colleagues. People who did not use cocaine, or did not know about cocaine use among others, appeared to assume that cocaine could not be used in controlled ways that would not impact work or that it is a sign of problems in the person’s life that might impact work. In contrast, unless people had familiarity with the potential adverse effects of pharmaceuticals, these substances were viewed as responsible and contributing positively to work performance. People familiar with potential adverse effects were more likely to present a more nuanced understanding about how adverse effects could be impairing, but were necessary and acceptable assuming strategies were in place to mitigate potential for harm to others.
Employees’ rights are protected by the Canada Labour Code and the Canadian Human Rights Act. The labour code defines substance use as “any use of alcohol or illicit drugs; the misuse of prescription or over-the-counter (OTC) drugs or; any accepted use of prescription or OTC drugs which results in adverse side-effects or reactions” (Government of Canada, 2012, para. 1). Employers have responsibilities of ensuring health and safety in the workplace while protecting employees’ human and privacy rights, and establishing policies (Canadian Human Rights Commission, 2017; Government of Canada, 2019b). The Canadian Human Rights Act states, “In addition to alcohol and drug use, there are many other factors—such as fatigue, stress, anxiety and personal problems—that lead to employee impairment and jeopardize workplace safety. The Commission encourages employers to adopt programs and policies that focus on identifying impairment and safety risks, and that are remedial, not punitive” (Canadian Human Rights Commission, 2009, p. 11).
The Canadian Human Rights Act prohibits discrimination, which includes previous or current substance dependence and “the actual or perceived possibility that an individual may develop a drug or alcohol dependency in the future” (Canadian Human Rights Commission, 2009). The place of “casual” or “recreation” substances in relation to human rights legislation is debated (Canadian Human Rights Commission, 2009). A number of interviewees proposed that concerns about a colleague’s substance use should be reported to either the employer or regulatory bodies in order to facilitate access to support services, which was presumably grounded in compassion for colleagues and concerns for safety in the workplace; however, these measures would need to be established in workplace policy with clear rationale and processes to mitigate discrimination.
Drug testing is prima facie discriminatory under Canadian human rights law, permissible under certain circumstances (Canadian Human Rights Commission, 2009). Employers must demonstrate employees are in “safety-sensitive” positions where concerns for safety risks outweigh intrusion into employee privacy. Fair processes must be in place to accommodate employees who test positive (Canadian Human Rights Commission, 2009; Government of Canada, 2019b). Employees prescribed substances (including cannabis) for medical purposes must be accommodated to the point of undue hardship (Canadian Human Rights Commission, 2009; Government of Canada, 2019b).
Self-Disclosure in the Context of Professional Regulation
Professional regulation is a form of institutionalized governance that influences personal decisions. Individual actions are surveilled by regulatory bodies, peers, the “public,” and oneself (Foucault, 1988). Being professional extends beyond specialized knowledge and particular jobs; it means adopting particular values (Micallef, 2014), ways of comporting oneself in public (Ross et al., 2013), dressing (Furnham et al., 2013; Splendore et al., 2016), talking (Park & Schallert, 2019), and ways of engaging in substance use (Kiepek & Beagan, 2018). A Canadian judge articulated: Becoming a member of a regulated profession comes with benefits but at a cost. Those who sign up as doctors, nurses, lawyers, engineers, or any other of the regulated professions that crowd the statute books choose to subject themselves to the requirements, rules and processes imposed by legislation, to applicable codes of conduct and professional standards, and to the authority of the regulator. It is entirely legitimate for a professional regulator to impose requirements relating to civility, respectful communication, confidentiality, advertising, and other matters that impact freedom of expression. Failing to abide by such rules can be found to constitute professional misconduct. (Strom v Saskatchewan Registered Nurses’ Association, 2020, para. 165)
At the same time, it is recognized by the Court “that does not mean the entire life of a professional should be subject to inordinate scrutiny” (Strom v Saskatchewan Registered Nurses’ Association, 2020, para. 166): that would lead to a substantial invasion of the privacy rights and fundamental freedoms of professionals…Nurses, doctors, lawyers and other professionals are also sisters and brothers, and sons and daughters. They are dancers and athletes, coaches and bloggers, and community and political volunteers. They communicate with friends and others on social media. They have voices in all of these roles. The professional bargain does not require that they fall silent. It does, however, allow the regulator to impose limits. (Strom v Saskatchewan Registered Nurses’ Association, 2020, para. 166)
While professionals are undoubtedly expected to conform to legislation, to applicable codes of conduct and professional standards, conduct unbecoming extends considerations of professional misconduct to interrogate a person’s integrity and honor in their comportment outside work hours. However, as contended by Adams (2020), “Understandings of the public interest are socially constructed, varying across time and place” (p. 6). There is a risk that professionals are positioned in society to be unrealistically virtuous. As such, professionals are expected to either adopt ways of being and interacting that meet a “higher” standard or to conceal controversial opinions or actions. The first instance is evidence of classist beliefs that certain groups of people are more or less valued members of society. In the second instance, erroneous beliefs and stigma are perpetuated and more complex understandings impeded.
Disclosure of personal substance use extends to social media and other online presence of professionals. The Canadian Medical Protective Association cautions physicians, “You’re more than just you…Society expects that physicians will adhere to the highest standards of professionalism,” (para. 1) advising they not be affiliated with anything that could be perceived as “unprofessional” (para. 4). The Newfoundland and Labrador Teachers’ Association (2019) video about social media reminds teachers, “teaching is a role model profession, a position of trust and confidentiality. A teacher is always a teacher. Your off-duty conduct can have an impact on you professionally.” The Chartered Accountants Canada frame their advice with respect to conveying a brand and scaling relationships while mitigating reputational risk and public embarrassment (Chartered Professional Accountants Canada, 2021). The International Federation of Air Line Pilots’ Associations (2018) similarly advises that online comments, photos, and videos can have serious consequences for their “flying career and private life” (p. 1).
Given some professionals’ perspectives that certain substances are inherently problematic conduct for a professional and professionals are expected to consistently model ideal social norms, self-disclosure about substance poses personal and professional risks. For professionals to disclose their use and perspectives about substances, there needs to be protection from professional disciplinary action. This study is a step toward providing a space for professionals to confidentially disclose their experiences and to bring visibility to hidden, private practices. In doing so, the public may be better informed about what it means to be a professional—which may or may not involve using substances.
Limitations
Recruitment for this study was challenging, with professional societies and associations acting to some extent as gatekeepers and methods of sharing the research invitations varying. There are a number of factors that could influence interest in the study, impacting representativeness of the sample; yet, substances use was highly variable, indicating a range of perspectives included. It is possible interviewees were influenced by social desirability bias to minimize disclosure of less socially desirable effects and experience.
Footnotes
Authors' Note
This project received ethics approval from the Dalhousie University Research Ethics Board REB#2018-4500.
Acknowledgments
We extend our appreciate to the research team members who contributed to the development and design of the project. We also acknowledge all participants of this study who shared their experiences and perspectives to help us better understand substance use among Canadian professionals.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Sciences and Humanities Research Council of Canada, Award Number 430-2017-00515.