
Abstract
Telemedicine provided older adults the ability to safely seek care during the coronavirus disease (COVID-19) pandemic. This study aimed to evaluate the potential impact of acculturation factors in telemedicine uptake between ethnic groups. As part of the National Health and Aging Trends Study 2018 survey, 303 participants (≥65 years) were interviewed. We assessed the impact of acculturation on telemedicine readiness by race and ethnicity. Compared to the white non-Hispanic immigrant population, Hispanic and Asian/Pacific Islander (API) populations had significantly lower telemedicine readiness and uptake. Limited English proficiency or older age at the time of migration was associated with telemedicine unreadiness and uptake in the Hispanic and API populations. Our findings suggested that acculturation factors play a substantial role in telemedicine uptake among older adult immigrants in the United States. Therefore, acculturation factors should be considered when promoting and adopting telemedicine technologies in older adults.
Introduction
Health disparities exist in the United States, particularly among minorities (Forrester et al., 2020; Thomson & Hoffman-Goetz, 2009). Health disparities in older adults, especially older minorities, reflect several factors, including limited access to care, poverty, unhealthy neighborhood, systemic racism, and acculturation (Arcaya et al., 2016; Lee et al., 2020a, 2020b; Ryvicker & Sridharan, 2018). Acculturation factors (defined as “the vehicle to assimilation by cultural adoption of the host society's norms, values, behaviors and attitudes”)—unlike other factors in health disparity—have been less studied as a source of health disparity (Wallace et al., 2010). Proxy measures for acculturation include age at migration and language proficiency. The impact on this population of telemedicine remains unclear and poorly studied (Thomson & Hoffman-Goetz, 2009). It is currently estimated that about 5 million older adults across the United States possess limited English proficiency (NCLER, 2019), and despite current work addressing disparities among older adults (Robert & Ruel, 2006), language barriers limit the quality of care received (United States Census Bureau). Specifically, prior studies have shown an increased number of hospitalizations, emergency department visits, readmissions, longer lengths of stay, and a lack of health literacy (Baker et al., 2002). In addition, foreign-born (first generation) older adults perceive themselves as having a lower health quality compared to subsequent generations (Acevedo-Garcia et al., 2010). Therefore, adequate education and equitable deployment of telemedicine alternatives may offer opportunities to reduce these inequities (Fulmer et al., 2021; López et al., 2011).
The expansion of telemedicine during the COVID-19 pandemic could give a unique opportunity to close those gaps in care. Evidence shows telemedicine-related improvements in health outcomes (Chevance et al., 2020; Comín-Colet et al., 2016; Gandolfi et al., 2017; Hong et al., 2017; Karhula et al., 2015; Kim et al., 2014; Liu et al., 2011; Logan et al., 2012; Trief et al., 2013; Wakefield et al., 2011; Wu et al., 2015), quality of life (Fortney et al., 2007; Hägglund et al., 2015; Liu et al., 2011; Seto et al., 2012; van der Weegen et al., 2015), medication management (Menon et al., 2018; Moore et al., 2015; Patel et al., 2013; Trief et al., 2013), and health literacy (Liu et al., 2011; Patel et al., 2013) among patients using telehealth prior to the pandemic. Nevertheless, it remains unknown how acculturation factors play a role in telemedicine uptake among older adults, especially older minorities. Designing and implementing culture-appropriate interventions to increase technology uptake in older minorities requires a comprehensive study of the roles of acculturation factors in healthcare technology readiness and uptake. Such a study has the potential to provide data to guide telemedicine approaches to narrow the digital divide in ethnic minorities. In this study, we aim to assess the association between acculturation and telemedicine uptake across race and ethnicity among older adults with limited English proficiency or who were foreign-born.
Methods
Sample
The present work is a cross-sectional study of community-dwelling participants from the 2018 National Health and Aging Trends Study (NHATS), which included 363 individuals (Freedman & Kasper, 2019). Of these, 12 (3.3%) participants were excluded because they were noncommunity residents (residential care or nursing home) and 48 (13.2%) because of cognitive decline, as detailed elsewhere (Rodríguez-Fernández et al., 2017; Rodríguez-Fernández et al., 2022). The remaining 303 individuals were included in the analysis. The NHATS protocol was approved by the the Johns Hopkins University Institutional Review Board, and all participants provided informed consent.
Race and Ethnicity
National Health and Aging Trends Study participants were asked to mark one race and ethnicity with which they identified, including white, non-Hispanic; African American, Non-Hispanic; Hispanic/Latino; and non-Hispanic others, including Asians and Pacific Islanders (API). This categorization was used in the present study.
Acculturation Factors
Per prior work (Kang et al., 2021), acculturation was measured in two different ways: First, English proficiency was measured by (a) speaking and (b) listening skills using a four-point Likert scale (1 = very well, 4 = not at all). Participants who spoke English well or very well and understood spoken English well or very well were categorized as highly English proficient. Second, age at migration was measured as a continuous variable ranging from 0 to 76.
Telemedicine Readiness and Unreadiness
Telemedicine readiness was defined as one of the following: (1) contacting a medical provider online; (2) handling medical insurance matters online (coverage, comparing providers, bill status, or filing a claim); and (3) obtaining information about medical conditions online.
Telemedicine unreadiness was defined as any physical or technical factor that limited the communication between healthcare providers and the patient. Physical limitations included any of the following: difficulty hearing, difficulty watching television or reading a newspaper even with glasses, or problems speaking or making self-understood. Technical limitations included not owning a working telecommunication device (computer, cell phone, or telephone) or not knowing how to use them, or no recent use of email, texting, or Internet during the last month.
Medical Conditions
Participants or their proxies were asked if they had been diagnosed with any of the following medical conditions: cancer, myocardial infarction, heart disease (separate from myocardial infarction), hypertension, stroke, diabetes, lung disease, osteoarthritis, and osteoporosis. Self-reports of chronic conditions have shown good diagnostic accuracy against claims and medical records (kappa ranging from 0.6 to 0.82) (Miller et al., 2008). Depression and anxiety symptoms were assessed using two validated screening questionnaires, the Patient Health Questionnaire-2 (PHQ-2) and the Generalized Anxiety Disorder-2 scale (GAD-2). We used a PHQ-2 score ≥ 3 to define substantial depression and a GAD-2 score ≥ 3 for anxiety symptoms; both questionnaires are validated clinical tools among older adults (Boyle et al., 2011; Wild et al., 2014).
Statistical Analysis
Demographic characteristics and acculturation factors of community-dwelling participants were compared between each telemedicine group; those who met any of readiness criteria and those who did not, and between those with unreadiness (physical or technical) and those without this condition, using χ2 tests. To account for the effects of age, we dichotomized age as younger than 80 versus older than 80 since the latter is more likely to lack technological exposure and have higher frailty levels limiting technological implementation and acquisition (Harvie et al., 2014; Harvie et al., 2016). Next, frequency rates of telemedicine readiness and unreadiness factors across acculturation factors were calculated. Adjusted logistic regression models were used to estimate telemedicine readiness and unreadiness due to physical or technical factors by acculturation factors. We adjusted for potentially confounding factors, including age, gender, education, marital status, and medical conditions (Rodríguez-Fernández et al., 2022). For all associations, we performed residual analyses to assess the fit of the data, checked assumptions, and examined the potential influence of outliers. Since our analyses were mainly exploratory, statistical significance was fixed a priori at a two-sided P-value <.05. Statistical analyses were conducted using Stata 12 SE version (Stata Corp, TX) and R version 4 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Demographic Characteristics by Race and Ethnicity
Table 1 shows the demographics, clinical characteristics, and medical conditions of the study sample by race and ethnicity. No age or gender differences were noted across groups. White non-Hispanic and APIs were more likely to be married and have a college graduate degree compared to African American non-Hispanic and Hispanic. Regarding acculturation, the age of migration to the United States was significantly higher for African American non-Hispanic and API. Lack of English proficiency was more prevalent among APIs and Hispanics. Regarding medical conditions for African American non-Hispanic and Hispanics were more likely to report diabetes, depression, and anxiety; lung disease and osteoporosis were more prevalent among APIs and Hispanics.
Demographic, Acculturation Factors, and Clinical Characteristics by Race/Ethnicity.
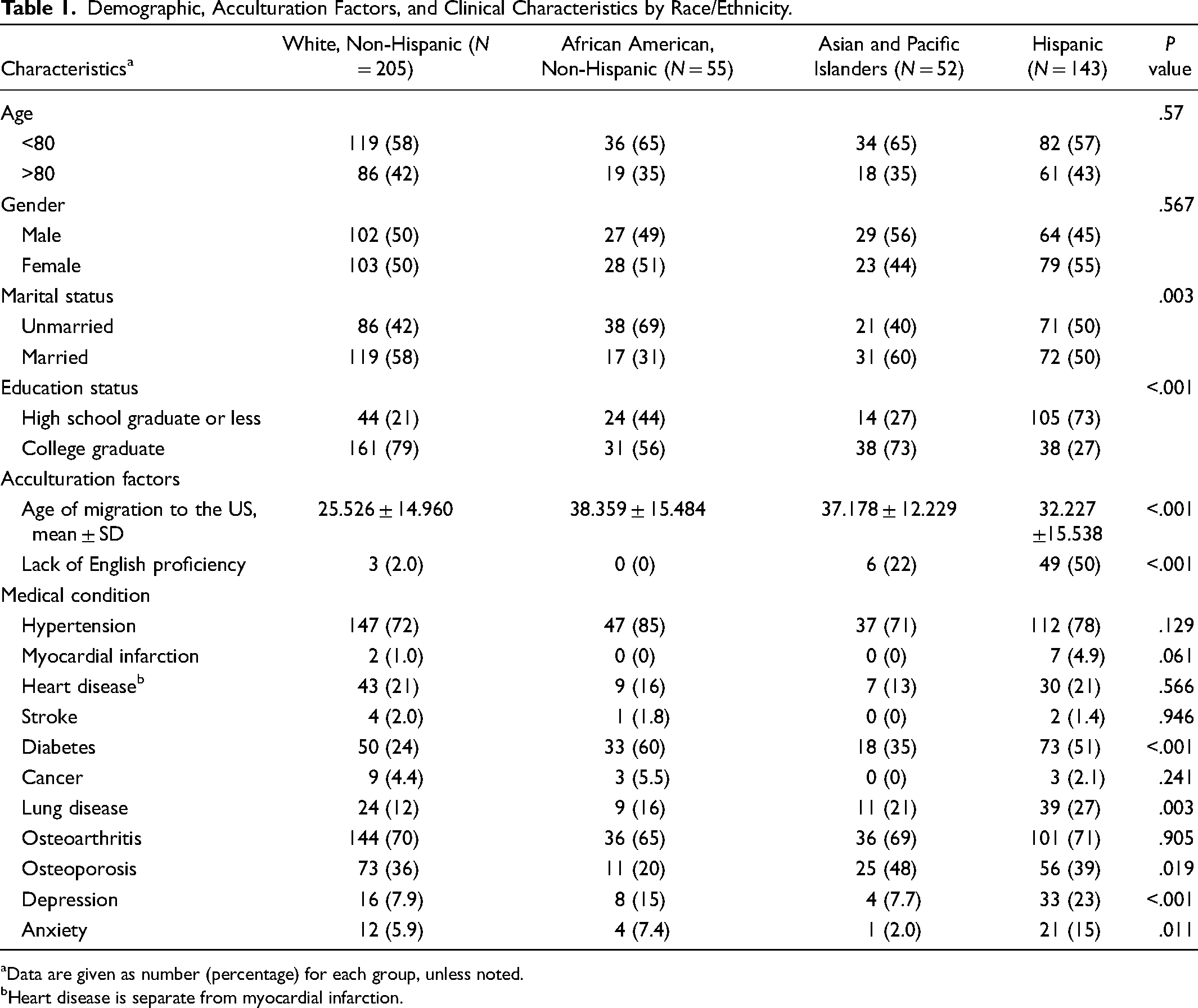
Data are given as number (percentage) for each group, unless noted.
Heart disease is separate from myocardial infarction.
Telemedicine Factors by Race and Ethnicity
Table 2 shows the prevalence of each telemedicine category by race and ethnicity. In regard to telemedicine readiness, being able to look for medical information online and contact medical providers online were more prevalent in white non-Hispanics (47% and 43%, respectively). Regarding physical unreadiness, difficulty reading the newspaper even with glasses was noted to be more prevalent among APIs (13%) and Hispanics (11%) compared with white Non-Hispanic and African American Non-Hispanic. For technical unreadiness, no recent internet use in the last month was the most prevalent (52%), followed by no recent email or texting use in the last month (65%), not having a working computer (54%), among Hispanic older adults.
Telemedicine Factors by Race/Ethnicity.
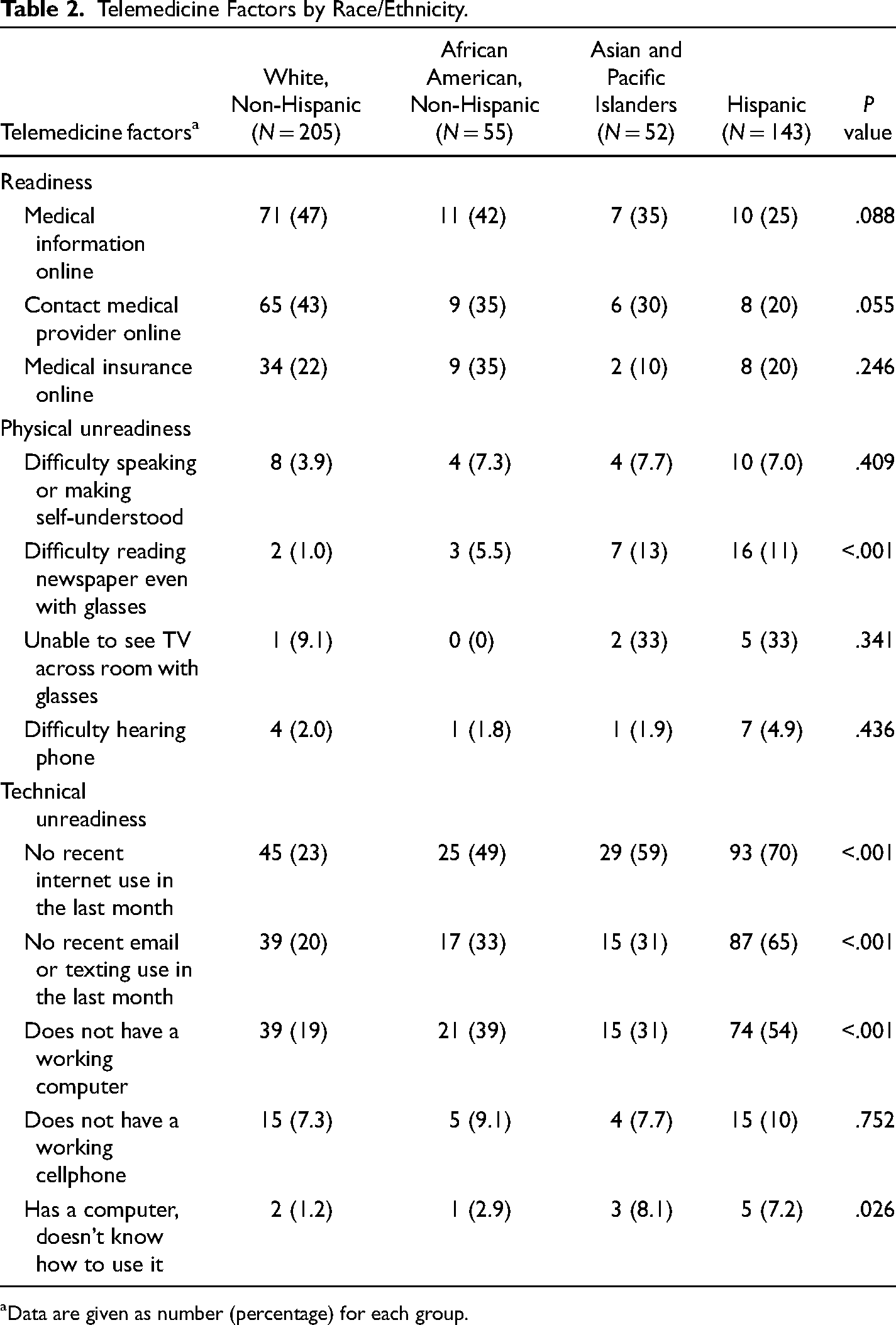
Data are given as number (percentage) for each group.
Acculturation Factors Across Telemedicine Readiness and Unreadiness
The association between telemedicine readiness and race and ethnicity was evaluated while adjusting for age, sex, marital status, education level, and chronic medical conditions. As shown in Table 3, a higherage at migration to the United States was significantly and negatively associated among APIs (odds ratio [OR] = 0.22, 95% confidence interval [CI] = 0.08–0.64, P < .01) and Hispanic older adults (OR = 0.22, 95%CI = 0.09–0.58, P < .01) with telemedicine readiness, while a positive association was observed for technical unreadiness in APIs (OR = 6.93, 95% CI = 2.50–19.23, P < .001) and Hispanic (OR = 3.22, 95% CI = 1.38–7.51, P < .01) older adults. Similarly, lack of English proficiency was significantly and negatively associated with APIs (OR = 0.14, 95% CI = 0.04–0.46, P < .01) for telemedicine readiness. Concerning physical unreadiness, APIs had a strong association with an OR of 5.04 (95%CI = 1.50–16.98, P < .01). Lastly, for technical unreadiness, a positive association was noted with Hispanic (OR = 2.70, 95%CI = 1.14–6.36, P < .05) and API (OR = 6.68 95%CI = 2.35–18.93, P < .001) older adults respectively, as compared with white older adults.
Adjusted Odds Ratios for Telemedicine Readiness and Unreadiness Across Race/Ethnicity and Acculturation Factors.
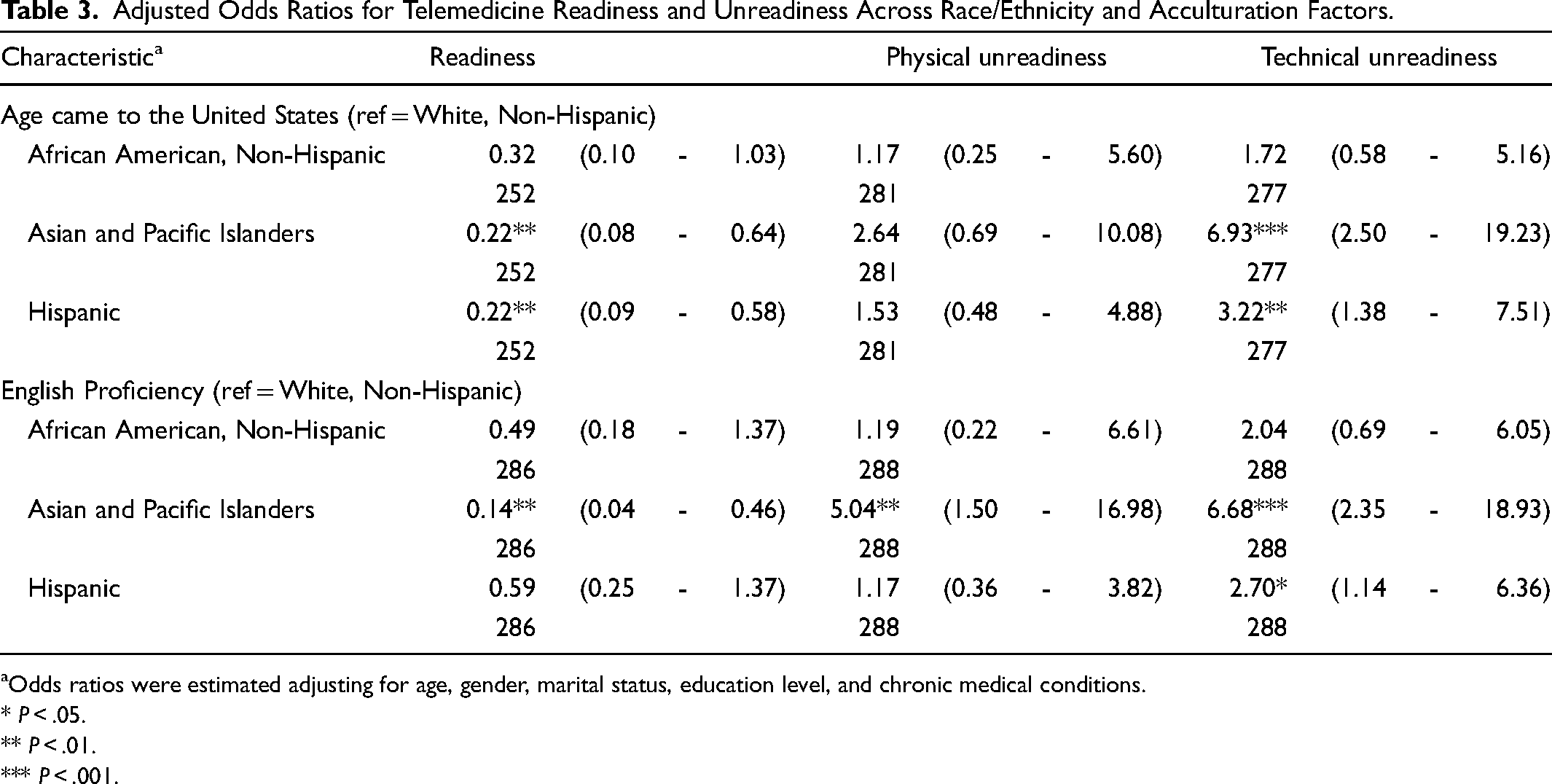
Odds ratios were estimated adjusting for age, gender, marital status, education level, and chronic medical conditions.
* P < .05.
** P < .01.
*** P < .001.
Discussion
In this nationally representative sample of older adults, we found limited telemedicine uptake among APIs and Hispanics based on their age of migration or English proficiency. Our results confirmed and extended previous findings. For example, data from a large cohort of older adults from a large healthcare system in California indicated that Black, Latino, and Filipino elders and those aged 75 years and older were less likely than non-Hispanic whites and Chinese elders to engage in eHealth technologies or use the patient portal, in part due to not having or not knowing how to use the devices (computers and smartphones) (Gordon & Hornbrook, 2016). However, this study did not account for acculturation factors across race and ethnicity in older adults, which may play a role in telemedicine uptake in this community. Overall, the findings in our study of health inequalities in telemedicine access and use among API and Hispanic populations underscored the need to develop targeted healthcare access-improving interventions that account for acculturation factors unique to this population.
Interestingly, telemedicine uptake for both API and Hispanic immigrants was worse based on their age of migration to the United States and limited English proficiency. Several explanations could account for these results. We know that older migration age is independently associated with a decline in physical and mental health after migration (Kang et al., 2021), with higher rates of mental health symptoms (Mui et al., 2003), multiple chronic medical conditions (Seo et al., 2017), social isolation (Lee et al., 2020a, 2020b), discrimination (Li & Dong, 2017), and social disparities (Lee et al., 2020a, 2020b). These factors may present barriers to telemedicine access to Hispanic older adults compared to their peers during the COVID-19 pandemic (Ryskina et al., 2021). Further work has shown that older minorities experience difficulties in telemedicine, especially during video visits, with the difficulty being further accentuated when needing an interpreter (Schifeling et al., 2020). Also, a lack of English proficiency and limited health literacy were noted to result in important communication barriers among older, adult Chinese American immigrants (Tsoh et al., 2016). In addition, despite policy changes by the Centers for Medicare and Medicaid Services (CMS), including paying providers for telehealth visits, minorities with limited English proficiency still experience disparities in their care, especially during the COVID-19 pandemic (Wilkins et al., 2021). Moreover, up to a third of the US health systems do not offer language services despite known mandates (Chen et al., 2007; Schiaffino et al., 2014). These barriers not only limit telemedicine access but also accentuate care gaps and previously existing suboptimal healthcare access among older minorities.
A substantial proportion of US older adults are more likely to lack access to technology and electronic health records portals and to have low digital health literacy (Smith, 2014). Currently, efforts by the National Institute on Aging include the promotion and support of research and other projects to improve the effectiveness of telemedicine for people with cognitive deficits, with the intention that such projects can be scaled and expanded to older adults without dementia (National Institute on Aging, 2020). In addition, the Federal Communications Commission (FCC) supported telehealth programs across the nation as part of the COVID-19 pandemic. Despite these efforts, current limitations include the limited infrastructure and providers supporting the offering of telemedicine services—especially in rural areas, a known limiting factor, as stated by the American Telemedicine Association (Humble et al., 2016). These prior efforts highlight the importance of developing interventions to enhance and optimize telemedicine uptake among older adults—especially older minorities. To achieve such optimization, telehealth experts offer two major recommendations: (1) optimizing telemedicine efforts outside health care (design and testing) and within healthcare (evaluating healthcare delivery, determinants of health, and increasing access) and (2) ensuring privacy and access as part of the 21st Century Cures Act (Humble et al., 2016).
Surpassing the existing limitations on telemedicine uptake includes the comprehensive evaluation of digital literacy, support for internet infrastructure (e.g., 5G wireless, fiber optic cable, and Wi-Fi, especially in rural and minority-dense areas), health literacy and language proficiency support, reduction of technical and physical barriers for all seniors, especially among API and Hispanic older adults. Our study, in particular, noted the strong effects of digital literacy and technical factors, consistent with prior work (Gordon & Hornbrook, 2016; Rodriguez et al., 2021; Wilcock et al., 2019). As per a recent systematic review (Kruse et al., 2020), the most common factor limiting telemedicine interventions included technical factors, motivation, and costs. These findings were replicated by our study even after we accounted for acculturation factors. However, technical factors do not account for the entire problem. Therefore, further research evaluating interventions across patient–provider communication and patient empowerment is needed, especially among older adult minorities experiencing communication barriers, as telemedicine continues to expand across all healthcare settings (clinics, nursing homes, postacute care, and hospitals).
Our results have several implications. From a clinical perspective, our work suggested that clinicians should be aware that immigrant older adults and those with limited English proficiency are more likely to experience difficulties with telemedicine, extending prior work on the barriers to telemedicine among older adults (Foster & Sethares, 2014; Kruse et al., 2020). With that awareness, clinicians may need to ask if a patient's family member or caregiver might be present to facilitate the visit. Alternatively, the visit might be recorded—thus allowing the patient to listen or watch the visit encounters by themselves with or without a more health-literate family member. Also, our findings highlighted the value of communication optimization for healthcare delivery, as English proficiency enhances healthcare access as per the Andersen Behavioral Model (Andersen, 1995). Interpreter availability should be increased to close the gap in healthcare access among older adult minorities. From a public health perspective, our study highlighted the importance of the continued expansion of telemedicine services, especially in underserved communities, with the federal support of the FCC and payment approvals by Medicare and private healthcare insurance companies. Furthermore, reimbursement continuation and equality for telemedicine visits from commercial services and CMS need to be maintained as compared to the more complex earlier guidelines pre-COVID-19. Our results suggest that from an institutional level, providers should be aware of the high rate of limited health literacy and communication barriers in older adult minorities with low English proficiency or those who were foreign-born. They also should be aware of the need for the development of streamlined protocols for language interpreters to be available to facilitate patient–provider communication and decrease gaps in healthcare access. Finally, inflation of type I error might have occurred in analyses due to multiple testing, and the observed associations should not be interpreted as causal relationships (Le Strat & Hoertel, 2011).
The strengths of our study include a relatively large sample size and its national representativeness. Results should also be interpreted in light of limitations common to most large-scale surveys. Although the NHATS is a nationally representative sample, it does not include non-Medicare beneficiaries or undocumented immigrants. Moreover, since this survey was conducted in English and Spanish, it is possible that immigrants who were not familiar with either language may not have been included in this survey. In addition, reporting devices or technical issues can potentially lead to over- or underestimation of the true rates of readiness or unreadiness. Also, the severity and possible consequences of telemedicine unreadiness were not evaluated, leaving the impact on older adults’ health overtime unclear. Longitudinal data are needed to examine the course of acculturation barriers and to evaluate older adults’ responses to either readiness or unreadiness.
Despite these limitations, our study constituted a critical step in the importance of racial and ethnic disparities and acculturation factors in telemedicine readiness and unreadiness in the United States. In a large, nationally representative sample of older, foreign-born US adults, a lack of English proficiency was associated with a lack of telemedicine readiness for Hispanics and APIs. Given the ongoing efforts to provide and enhance care through telemedicine for older adults during the COVID-19 pandemic, these results support the need to consider acculturation factors by race and ethnicity to facilitate telemedicine usage and adoption in older adults.
Footnotes
IRB Review
Since all the analyses were performed on de-identified NHATS data which is publicly available for download, IRB review was not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.