
Abstract
This study aimed to examine whether hypertension prevalence varies by race/ethnicity and within age groups in a nationally representative sample of men in the United States. Hypertension was defined as blood pressure (BP) readings of 140 mm Hg and higher for systolic BP, 90 mm Hg and higher for diastolic BP, or self-reports of taking medication for hypertension. Modified Poisson models estimated prevalence ratios (PRs) and 95% confidence intervals (CI) for race and age group associations with hypertension. The prevalence of hypertension was 38% overall and 46% of the men were aged 50 and older. Analyses that focused on older men (50 years of age or older) found that non-Hispanic Black men had a higher prevalence of hypertension (PR = 1.28, 95% CI: 1.19 − 1.37) compared to non-Hispanic White men. We suggest future research utilize life course perspectives to better identify which cumulative experiences impact hypertension disparities.
The prevalence of high blood pressure, or hypertension, presents a global challenge for mortality and cardiovascular disease (Fisher & Curfman, 2018; Forouzanfar et al., 2015). Globally, hypertension increased from the fourth leading risk factor for premature death and disability in 1990 to the number one leading risk factor in 2010 (Lim et al., 2012). In the United States (US), hypertension is the primary, preventable risk factor for heart disease and accounts for $131 billion in annual healthcare costs (Benjamin et al., 2019; Kirkland et al., 2018). Literature focused on US men's burden of hypertension is limited but provides some indication of disparities between men of different racial/ethnic groups (Aggarwal et al., 2021; Benjamin et al., 2019; Pathak, 2018). A recent international study comparing population health in high-income countries found that men in the US reported the highest prevalence of hypertension (Gunja et al., 2022). In the US, age-adjusted estimates reported hypertension prevalence was highest for non-Hispanic Black men (NHB; 58.3%), followed by non-Hispanic White (NHW; 51.0%) and Hispanic men (50.6%) (Tsao et al., 2022). Furthermore, NHB men's hypertension profile is a public health concern. Studies suggest NHB men's higher hypertension prevalence has persisted since 1999 (Benjamin et al., 2019; Tsao et al., 2022). Collectively, this evidence supports the previous claim that NHB men have the highest rate of hypertension in the world (Gadson, 2006).
Amid evidence showing that NHB men gain less health benefits from increased socioeconomic status (SES) (e.g., educational attainment, income, employment, and poverty) relative to NHW men (Bell et al., 2018, 2020; Gilmore et al., 2022; Williams, 2003), it has become clear that the relationship between such SES indicators and health is not uniformly comparable across racial groups. Numerous studies have documented weaker effects of SES on health for NHBs and other marginalized populations compared to NHWs in America (Assari, 2018b, 2018a; Bell et al., 2020; Braveman et al., 2005; Hudson et al., 2020; Kaufman et al., 1997; Navarro, 1991; Wilson et al., 2017). Conversely, research reports elevated health risks for men at all levels of SES (Assari, 2018c; Leng et al., 2015; Williams, 2003; Zare et al., 2021). Some evidence offers that excessive exposure to psychosocial factors such as stressful life events, discrimination, racism, John Henryism (a high effort coping style towards upward mobility that incurs wear and tear on bodies and detected as poor cardiometabolic health) (Brody et al., 2018; James, 1994), medical mistrust, and limited access to care are reasons for NHB men's distinct hypertension burden (Blyler & Rader, 2019; Control & Prevention, 2010; Subramanyam et al., 2013). One study found that NHB men have a higher prevalence of allostatic load (a chronic stress measure that incorporates blood pressure) than NHW men with the same level of education (Tavares et al., 2022). This study suggests that SES alone may not protect NHB men's health. Furthermore, these factors have been shown to impact health through their accumulation over time (Gee & Ford, 2011; Gilbert et al., 2016; Thorpe et al., 2016; Williams, 2003 2019).
The prevalence of hypertension increases with age among men. Using NHANES 2017 to 2018 data, it was shown that men's overall prevalence of hypertension was 51% (Ostchega & Nguyen, 2020). When disaggregated by age group, the prevalence was 31.2% among men aged 18−39, 59.4% among men aged 40−59, and 75.2% among men aged 60 and over. Whereas men's life expectancy in 2019 was 76.2 years, the rapid increase in hypertension prevalence across age and among men is concerning (Kochanek et al., 2020). Given NHB men's excess hypertension burden and lagging life expectancy compared to non-Hispanic White men, this is especially troubling (Benjamin et al., 2019; Bond & Herman, 2016).
Presently, the dearth of research on hypertension at the intersections of race and age among men in the US context is an important limitation to aging research. In part, this is because empirical studies tend to adjust for some combination of age, gender, or race in statistical analyses. It is important to consider the role of age, race/ethnicity, and gender simultaneously to increase our understanding of the pattern of hypertension disparities as men grow older. Doing so may inform more appropriately tailored interventions and policy recommendations to advance men's health equity. Therefore, the objective of this study was to examine whether hypertension prevalence varies by race/ethnicity and within age groups in a nationally representative sample of men living in the US. Identifying whether disparities in hypertension remain constant at distinct life stages may provide important insights to reduce the burden of hypertension among men and attenuate cardiovascular disease, disability, and mortality.
Research Methods
Sample
We used 2011−2014 and 2015−2018 data from the National Health and Nutrition Examination Survey (NHANES), which is a nationally representative sample of the civilian noninstitutionalized population of adults 18 or older (Chen et al., 2020). These cross-sectional surveys used a stratified, multistage probability sampling design ((NHANES, 2018; Zipf et al., 2013). NHANES public use data files are released biannually (e.g., NHANES 1999–2000, NHANES 2001–2002, NHANES 2003–2004, etc.). NHANES data collection occurs in two parts. First, participants provide their health history, health behaviors, and risk factors via at home interviews. Second, participants received a detailed physical examination at a mobile examination center (Johnson et al., 2013; Thorpe et al., 2008). This analysis included all men who: had valid data on SBP and DBP; self-identified as NHW or NHB, and at least 20 years old. We excluded men younger than 20 because many control variables were collected only for men 20 years and older. From our original sample of 8,052 participants, we have excluded 1,946 because of missing values for independent and outcome variables. This yielded an analytic sample of 6,106 men, which included 3,819 NHW and 2,287 NHB men.
Outcome Variable
We defined hypertension as readings 140 mm Hg and higher for SBP or readings of 90 and higher for DBP or reports of taking antihypertensive medications in accordance with the Seventh Report of the Joint National Committee (JNC 7) (Chobanian et al., 2003). As a sensitivity analysis, we defined hypertension using the 2017 guideline from the American College of Cardiology and American Heart Association (ACC/AHA) (Whelton et al., 2018). Using this guideline, hypertension was defined as readings 130 mm Hg and higher for SBP or readings of 80 and higher for DBP.
Independent Variable
The primary independent variable was an indicator of race/ethnicity. NHANES allows five categories for race/ethnicity: Mexican American, other Hispanic, non-Hispanic White (NHW), non-Hispanic Black (NHB), and other race including multiracial. We excluded respondents that identified as Mexican American, other Hispanic, and other race. An indicator variable was created to identify men as NHW or NHB, where NHW was the reference group.
Covariates
Models controlled for demographic and health-related characteristics associated with race/ethnicity in previous literature (Miao et al., 2020; Ostchega et al., 2012). Demographic variables included age (years), married (1 = yes, 0 = no), income level (<$34,999, $35,000–74,999, ≥$75,000), and education level measured across three categories (less than high school graduate, high school graduate or general equivalency diploma equivalent recipient, more than high school). Health-related characteristics included the number of visits (index representing number of times seen a doctor or other health care professional health at a doctor's office, a clinic, a hospital emergency room, at home, or some other place during last year), number of chronic conditions (a variable to count how many of the following conditions a men reported: diabetes, obesity, congestive heart failure (CHF), coronary heart disease, heart attack, and stroke), and health behaviors including smoking and drinking status (0 = never, 1 = current, 2 = former).
Analytic Strategy
Mean and proportional differences for demographic and health-related characteristics were evaluated for the total sample and by race/ethnicity using Student's t-tests and chi-square tests, respectively. Since the prevalence of hypertension was greater than 10% in this sample, a modified Poisson regression was used (McNutt et al., 2003; Thorpe et al., 2017; Zou, 2004). Two models were tested to examine the relationship between race/ethnicity (independent variable) and hypertension (dependent variable) while controlling for possible confounders. In model 1, we examined the association between race/ethnicity and hypertension, adjusting for all covariates for men 20 years and older. In model 2, we ran the same analysis for men 50 years and older. All analyses were weighted using the NHANES individual-level sampling weights for four waves of data (NHANES 2011–2018). We considered all p-values <0.05 statistically significant, and all tests were two-sided. All statistical procedures were performed using STATA statistical software, version 15.
Results
The distribution of select characteristics of NHB and NHW men 20 years of age and older for the total sample and by race/ethnicity is shown in Table 1. Of the 6,106 men, most of the men: were NHW (86.1%), had more than high school education, were married, and were current drinkers. On average, the men reported 2.2 (1.4) medical visits during last year and 0.6 (0.7) chronic conditions. Thirty-eight percent of the men were hypertensive and 46% of the men were 50 years of age or older. When examining race/ethnic differences in the select characteristics, a smaller portion of NHB men were 50 years of age or older, had more than a high school education, had income greater than $75,000, were married, or a current drinker relative to NHW men. There was a larger portion of NHB men who reported being a current smoker or hypertensive than NHW men. On average, NHB men reported fewer medical visits than NHW men. There was no significant difference observed between NHB and NHW men with regard to number of chronic conditions.
Distribution of Select Characteristics of Non-Hispanic Black and Non-Hispanic White Men 20 Years of Age or Older for the Total Sample and by Race/Ethnicity, 2011–2018 NHANES.
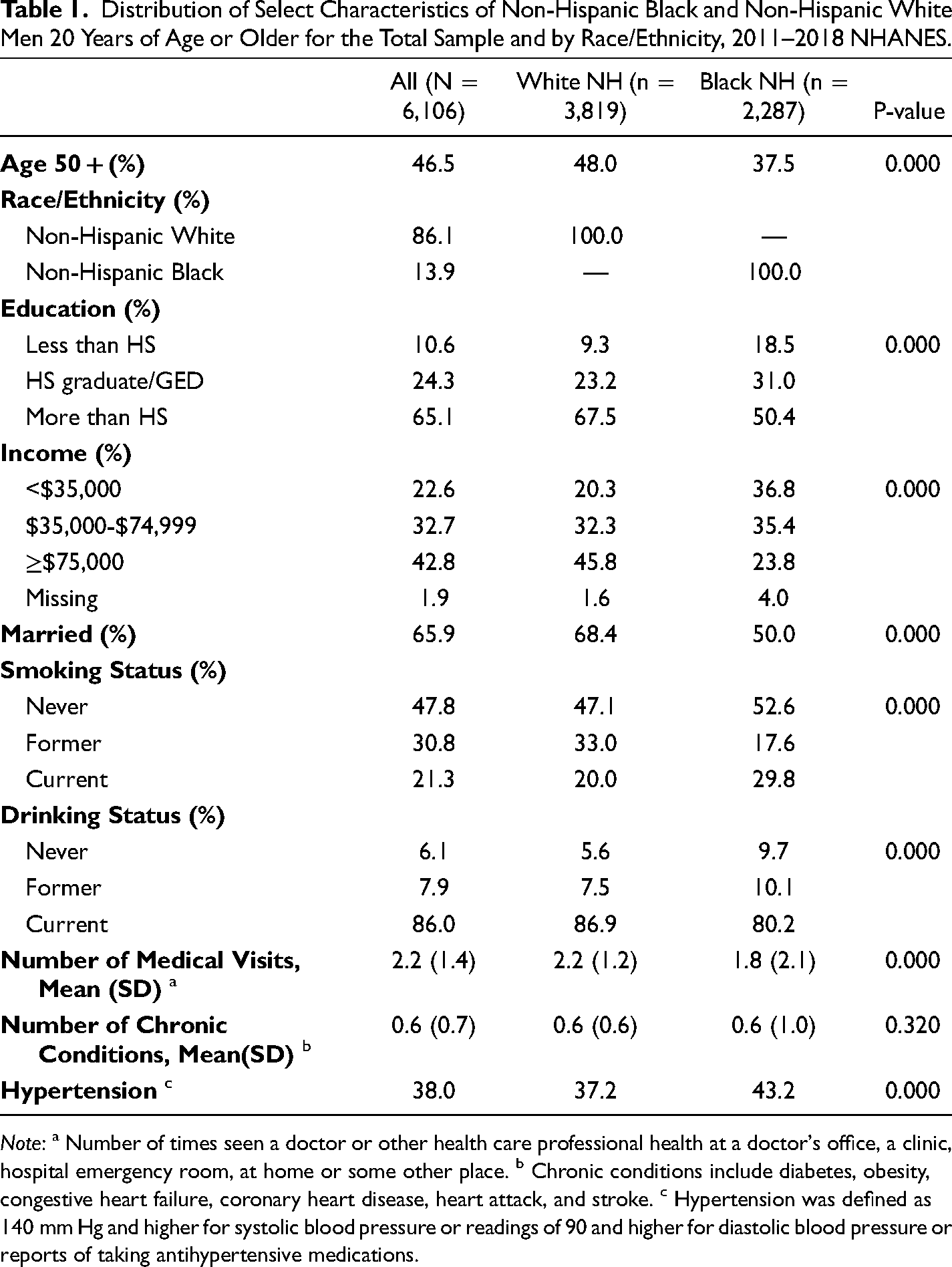
Note: a Number of times seen a doctor or other health care professional health at a doctor's office, a clinic, hospital emergency room, at home or some other place. b Chronic conditions include diabetes, obesity, congestive heart failure, coronary heart disease, heart attack, and stroke. c Hypertension was defined as 140 mm Hg and higher for systolic blood pressure or readings of 90 and higher for diastolic blood pressure or reports of taking antihypertensive medications.
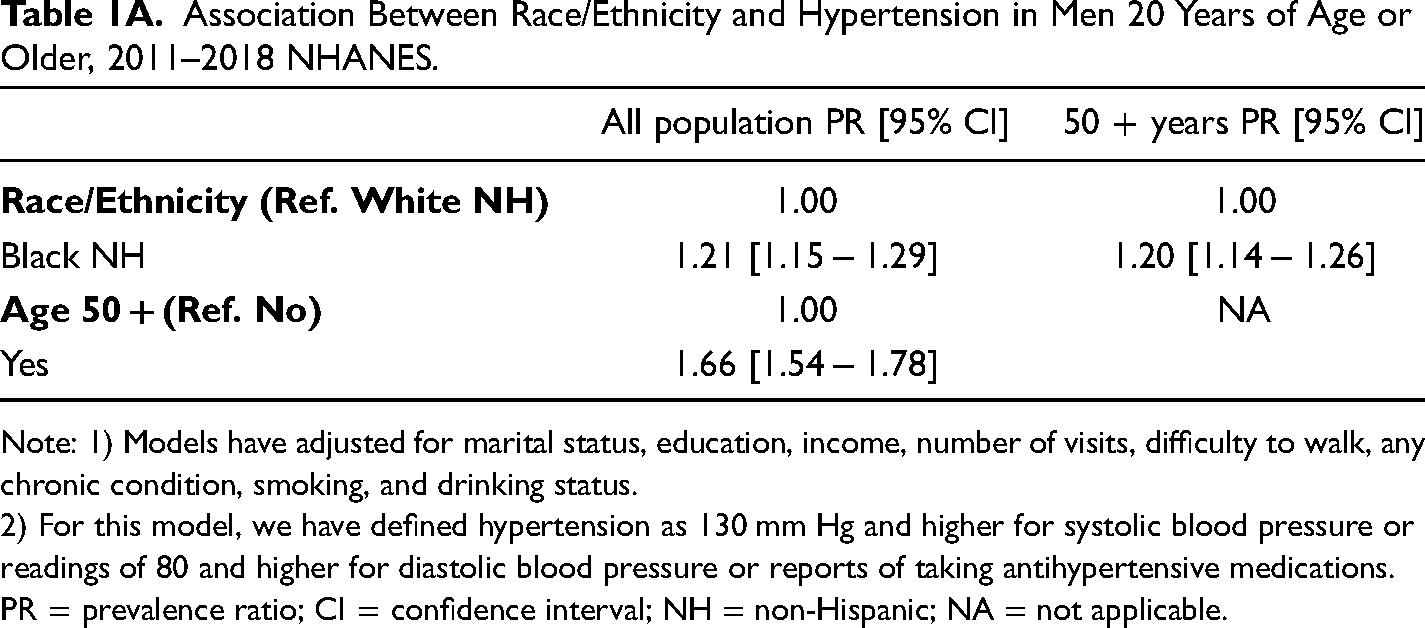
The association between race/ethnicity and hypertension among NHB and NHW men 20 years of age and older is displayed in Table 2. In the total sample, NHB men had a higher prevalence of hypertension (PR: 1.33, 95%; CI: 1.24–1.43) compared to NHW. Similarly, when examining men who are 50 years of age or older, NHB men had a higher prevalence of hypertension (PR: 1.28, 95% CI: 1.19–1.37) compared to NHW men. As a sensitivity analyses, we applied the AHA 2017 guidelines for hypertension. The overall results did not change.
Association Between Race/Ethnicity and Hypertension in Men 20 Years of Age or Older, 2011–2018 NHANES.
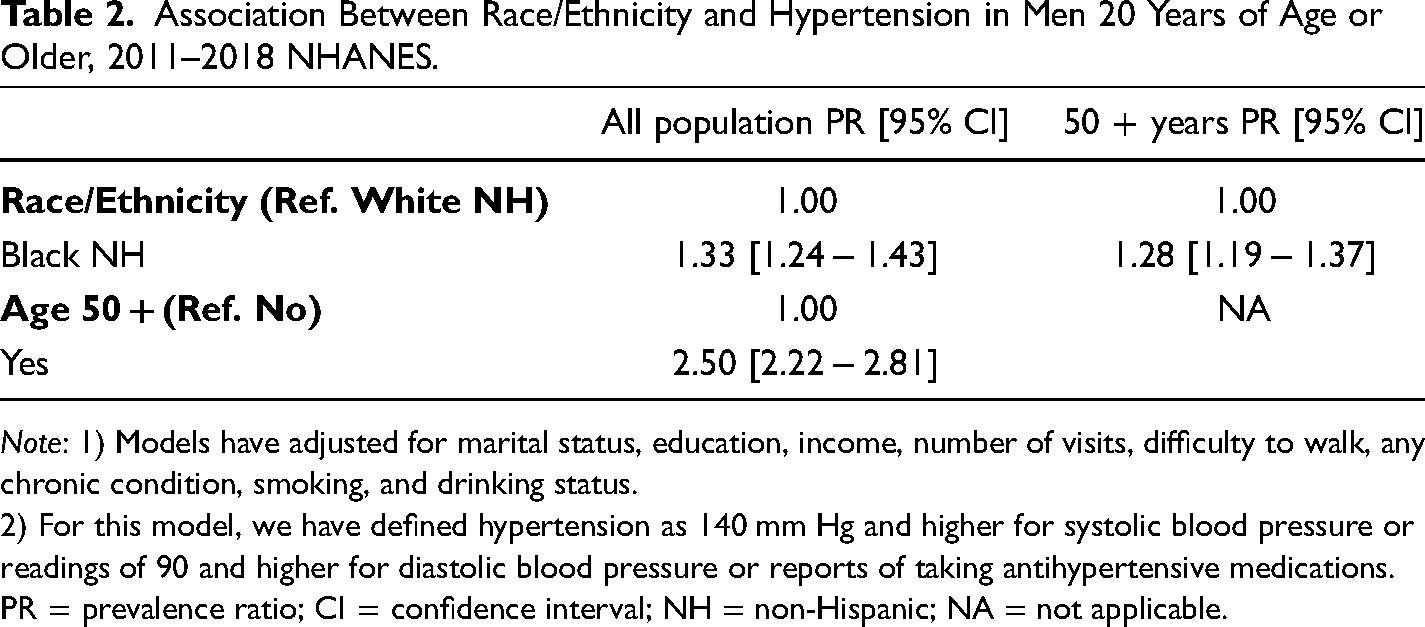
Note: 1) Models have adjusted for marital status, education, income, number of visits, difficulty to walk, any chronic condition, smoking, and drinking status.
2) For this model, we have defined hypertension as 140 mm Hg and higher for systolic blood pressure or readings of 90 and higher for diastolic blood pressure or reports of taking antihypertensive medications.
PR = prevalence ratio; CI = confidence interval; NH = non-Hispanic; NA = not applicable.
Discussion
This study examined the prevalence of hypertension by race/ethnicity and whether race differences remained after centering analyses at older age among US men. Results provide evidence that NHB men had a higher prevalence of hypertension than NHW men. Most important, analyses that centered on older men observed that this race difference remained. Our findings highlight a disparity in hypertension prevalence between NHB and NHW men in later life. Moreover, because less research has focused on differences in hypertension prevalence at the intersections of gender, race, and age, our study findings add to literature on hypertension and aging.
The current study's finding of a race disparity in hypertension among men aged 50 and older is consistent with extant literature on race disparities in hypertension among men overall (Fryar et al., 2017; Sampson et al., 2014). However, most of the previous studies on hypertension disparities are difficult to compare because they adjust for age, exclude older adults, or emphasize differences in hypertension across gender groups (Commodore-Mensah et al., 2021; Everett & Zajacova, 2015; Howard et al., 2017; Sampson et al., 2014). Some studies using nationally representative data reveal that the prevalence of hypertension is higher for Black men compared to White men (Commodore-Mensah et al., 2021; Fryar et al., 2017; Ostchega & Nguyen, 2020). Similarly, most research using population-based samples report that NHB men were more likely to have hypertension compared to NHW men (Carnethon et al., 2017; Howard et al., 2017; Sampson et al., 2014). For example, one study based on the southeastern United States found that NHB men had increased odds for self-reported hypertension than NHW men (Sampson et al., 2014). In contrast, evidence from the REGARDS study did not observe Black-White differences in hypertension incidence rates in older men (Howard et al., 2017).
While the current study's central finding of a persistent Black-White hypertension disparity among men and in old age is not surprising, it complements literature that calls attention to using a life course approach in research. Hypertension develops over time and the same is true for disparities in hypertension. It is suggested that the accumulation of social disadvantages and stressors over the life course is the primary pathway to adverse health among minority populations (Larson et al., 2018; Thorpe, Duru et al., 2015; Thorpe et al., 2016). Some studies offer evidence that race disparities in high blood pressure originate in youth (Bruce et al., 2015; Carnethon et al., 2017). In addition, disparities that begin early in life may evolve over time with increased exposure to unfavorable environmental conditions (Thorpe, Kennedy-Hendricks et al., 2015). These disparities are bolstered by differences in the structural conditions where people are born, live, and eventually age that unequally distribute needed resources for optimal health and well-being across race/ethnicity and social class—social determinants of health (Dawes, 2018; Thorpe et al., 2008; Usher et al., 2018). Previous research shows that health disparities dissipate when Black and White men live under the same environmental conditions (Baxter et al., 2021; Caldwell et al., 2017; Gaskin et al., 2014; Thorpe, Kennedy-Hendricks et al., 2015; Thorpe et al., 2014; Thorpe, Kelley et al., 2015). This is because they experience similar access and barriers to resources and opportunities that shape health.
Few studies have examined the impact of neighborhood environments on hypertension disparities and available evidence is context specific and mixed (Morenoff et al., 2007; Thorpe et al., 2008; Usher et al., 2018). Research has shown that Black men who grew up and worked in racially segregated environments were more likely to be diagnosed with hypertension than Black men who did not (Gilbert et al., 2015). Conversely, one study observed that Black-White hypertension disparities were non-existent when NHB and NHW individuals lived in gentrifying US neighborhoods (Smith et al., 2020). On the other hand, a cross-sectional study on hypertension in older adults found that Black older adults living in predominantly Black, integrated, and predominantly White neighborhoods had higher odds of hypertension compared to White older adults living in predominantly White neighborhoods (Usher et al., 2018). NHB men's separation from NHW men in work and residential environments and higher hypertension prevalence may be explained by the accumulation of biopsychosocial determinants over the life span that are produced by structural racism (Churchwell et al., 2020; Hines et al., 2022; Thorpe & Halkitis, 2016). This is important because racism is associated with stress exposures and hypertension-related risk factors (Brondolo et al., 2011; Forde et al., 2020; Hicken et al., 2014; Thorpe et al., 2017). Findings from the present study suggest that hypertension disparities persist over time in men and warrant further investigation into the core drivers that initiate and maintain NHB men's hypertension burden over the life course.
This paper has some limitations. We used cross-sectional data, so causality cannot be determined. Since NHANES is publicly available data, we were not able to include geographic variables in analyses, which may have impacted findings. The majority of NHBs live in the southeastern US, which is also known as the Stroke Belt. This study also has some strengths. To our knowledge, this is the first study to examine hypertension prevalence among older men with a wide range of NHANES data. The use of weighted models allowed findings to be nationally representative, which increases generalizability.
The findings of this study suggest the need for practices and policies to reduce the hypertension prevalence among NHB men before age 50. This will require an intentional focus on men and eliminating race/ethnicity disparities in community and health care settings. Interventions that are place-based, equity-focused, and male-centered need to take a multilevel approach to focus on stress coping, structural racism, and other societal causes of high blood pressure. This strategy has the potential to uncover culturally appropriate practices for blood pressure maintenance that meet men where they are. Following the National Quality Forum's roadmap for promoting health equity, accumulating research can encourage health care systems to incentivize reductions in health disparities (Anderson et al., 2018; National Quality Forum, 2017). Health care systems can do this by developing health equity performance measures that focus on their own practice, community outreach, and financial investments in community organizations that can meet the needs of populations with increased risk for hypertension, like NHB men. Reducing race/ethnicity disparities in hypertension among older men will require a combination of these strategies to be simultaneously implemented and prioritize younger populations of men.
Conclusion
In a nationally representative sample, a Black-White disparity in hypertension was observed among men and older men in particular. The study's keys findings of the hypertension disparity among BNH and WNH men and in old age is not surprising but has not been shown in prior work, to our knowledge. However, the mechanisms underlying NHB older men's higher risk of hypertension were not explored in this study. We suggest future research utilize life course perspectives to better identify which cumulative experiences impact hypertension disparities in late life. Additionally, more longitudinal studies are needed to delineate how hypertension disparities fluctuate within age groups and over time for men. Such approaches to health equity and aging research may inform interventions and policy towards the elimination of race/ethnic disparities.
Footnotes
Acknowledgments
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by grants K02AG059140 and U54MD000214.
Appendix
Association Between Race/Ethnicity and Hypertension in Men 20 Years of Age or Older, 2011–2018 NHANES.
| All population PR [95% CI] | 50 + years PR [95% CI] | |
|---|---|---|
|
|
1.00 | 1.00 |
| Black NH | 1.21 [1.15 − 1.29] | 1.20 [1.14 − 1.26] |
|
|
1.00 | NA |
| Yes | 1.66 [1.54 − 1.78] |
Note: 1) Models have adjusted for marital status, education, income, number of visits, difficulty to walk, any chronic condition, smoking, and drinking status.
2) For this model, we have defined hypertension as 130 mm Hg and higher for systolic blood pressure or readings of 80 and higher for diastolic blood pressure or reports of taking antihypertensive medications.
PR = prevalence ratio; CI = confidence interval; NH = non-Hispanic; NA = not applicable.