
Abstract
This study examined the effects of secrecy on quality of life in a sample consisting of older adults (>50 years; N = 301). Three key components of secrecy were examined with the Tilburg Secrecy Scale-25 (TSS25; possession of a secret, self-concealment, and cognitive preoccupation). The TSS25 distinguishes between the tendency to conceal personal information (self-concealment) and the tendency to worry or ruminate about the secret (cognitive preoccupation), thereby enabling investigation of the effects of secrecy on quality of life in detail. Confirming previous findings in younger samples, we found a positive effect of possession of a secret on quality of life, after controlling for both TSS25’s self-concealment and cognitive preoccupation. This suggests that keeping secrets may have a positive association with quality of life in older adults as well, as long as they do not have the tendency to self-conceal and are not cognitively preoccupied with their secret.
The aim of this study was to investigate the effects of keeping secrets on quality of life in older adults. Secrecy prevalence rates range from 30% for emotionally disturbing secrets that are hardly shared with others to 99% for the more inconsequential daily secrets (Frijns & Finkenauer, 2009; Vangelisti, 1994). This shows that most people hold secrets. Secrets range from the most trivial events (such as not washing one’s hands after visiting the toilet or one’s caloric intake) to major secrets that have an enormous impact on the secret-keeper (such as having sexually abused your child). It is important to realize, however, that the way secrets affect us is idiosyncratic; an individual may be deeply affected by a secret that most of us would regard as irrelevant. That is, the burden of the secret is more important than its content.
The majority of secrecy research is conducted among college students or the general population, whereas the older adult population is neglected (Wismeijer, 2011). This is particularly striking as older adults, given their older age, have had more opportunities for secrets to develop and for secrets to potentially have an effect on well-being. Although no empirical data exists on the qualitative and quantitative differences in secret-keeping between younger and older adults, studying its effects in older adults may give a more complete picture of its effects than when studying secrets in a relatively young sample. Moreover, older adults might have been confronted with taboos, which are no longer considered as such nowadays. Despite the potential of an older population for secrecy research, to our knowledge no research exists that specifically targeted older adults.
Secrecy is a complex and multifaceted phenomenon. Perhaps as a result, several definitions of secrecy have been proposed, each emphasizing different aspects of keeping secrets (e.g., Bouman, 2003; Frijns, 2004; Hillix, Harari, & Mohr, 1979; Lane & Wegner, 1995; Margolis, 1974). Based on these definitions, Wismeijer (2011) proposed a synthesis, defining secrecy as the conscious and active process of social selective information exchange that uses cognitive resources and can be experienced as an emotional burden with possible physical consequences.
Secrecy consists of several components that should be distinguished. First, it is essential to distinguish between the act of keeping a secret, or possession of a secret (secrecy as a state), and being a secretive person, or a self-concealer (secrecy as a trait). Whereas possession of a secret often means that situational circumstances do not allow the information to be disclosed (Wetzer, Zeelenberg, & Pieters, 2007), self-concealment is defined by Larson and Chastain (1990) as “a predisposition to actively conceal from others of personal information that one perceives as distressing or negative” (p. 440).
The dominant view among psychologists and laypersons alike has long been that keeping secrets can negatively affect mental but also physical health (e.g., Frijns, Keijsers, Branje, & Meeus, 2010; Larson, Chastain, Hoyt, & Ayzenberg, 2015; Obasi & Leong, 2009; Vogel & Armstrong, 2010; but also see Consedine, Magai, & Bonanno, 2002 for a critical view). In line with this “inhibition hypothesis”, research has shown that disclosing personal stressful information has positive immediate and long-term effects on health (e.g., Pennebaker, 1989, 1997; Pennebaker & Beall, 1986). Disclosing personal information might furthermore increase personal closeness and plays an important role in constructing relationships (see Harvey & Omarzu, 1997), which in turn may positively affect well-being. Pointing to the possible mechanism underlying the negative effect of keeping secrets on well-being, Lane and Wegner’s (1995) research showed that keeping secrets requires suppression of thoughts related to the secret to prevent a so-called slip-of-the-tongue. This work is based on the well-known white bear paradigm, in which Wegner (1992, 1994) showed that thought suppression leads to intrusive thoughts about the secret, initiating a vicious circle that may cause an obsessive preoccupation with the secret information, negatively affecting one’s quality of life (Wismeijer, Van Assen, Sijtsma, & Vingerhoets, 2009).
This research shows that next to the two already defined components of secrecy—possession of a secret and self-concealment—we have to consider a third component: cognitive preoccupation. The degree of cognitive preoccupation refers to the amount of time and energy the individual spends thinking and worrying about the secret. Cognitive preoccupation therefore affects the influence the secret may have in terms of behavioral and emotional outcomes. Each secret may pose a different cognitive burden for different people, which stresses the strong idiosyncratic nature of secrets. In their 2015 paper, Larson et al. refined their definition of self-concealment to “a complex-trait-like motivational construct where high levels of self-concealment motivation energize a range of goal-directed behaviors (e.g., keeping secrets, behavioral avoidance, lying) and dysfunctional strategies for the regulation of emotions (e.g., expressive suppression), which serve to conceal negative or personal information” (p.708), thereby not clearly distinguishing between concealing distressing or negative information and the dysfunctional emotional regulation strategies associated with this. However, in our definition of secrecy, self-concealment and cognitive preoccupation are clearly viewed as separate dimensions.
Although the dominant view is that secrets negatively affect health, the relation between secrecy and well-being changes when considering all different components of secrecy. Indeed, self-concealment (secrecy as a trait) has consistently been found to be negatively associated with physical and psychological problems (e.g., Cepeda-Benito & Short, 1998; Ichiyama et al., 1993; Kelly, 1998; Kelly & Achter, 1995; Masuda et al., 2011; Uysal, Lin, & Knee, 2010; Wismeijer, 2011), also after controlling for other variables such as social support, self-disclosure, and occurrence of a trauma (Larson et al., 2015). Paradoxically, studies that investigated the effect of possession of a secret (secrecy as a state) on well-being found that, after statistically controlling for self-concealment, possession of a secret is not per se negatively related to well-being (Kelly, 1998; Kelly & Yip, 2006; Maas, Wismeijer, Van Assen, & Aquarius, 2012; Wismeijer, et al., 2009). After controlling for the effect of self-concealment, possession of a secret was sometimes even positively related to well-being. This positive effect may be explained by the fact that keeping secrets can be considered a successful coping strategy to protect the secret-keeper by reducing or preventing negative social evaluative feedback, social disapproval, and stigmatization by others (Kelly, 2002).
Taken together, the picture emerges that some elements of secrecy can be potentially detrimental for well-being and other elements appear to be beneficial instead. How can these findings be reconciled with theories that predominantly view secrets as detrimental for well-being? The answer was recently proposed by Maas et al. (2012), who assessed the effect of possession of a major secret, namely the HIV status of a HIV-positive sample, on quality of life, by controlling for both self-concealment and cognitive preoccupation. Also note that in the Maas et al.’s study, similar to this study, self-concealment and cognitive preoccupation are defined as separate dimensions. Their model is depicted in Figure 1. They found a positive association between possession of a secret and quality of life, but only after controlling for both self-concealment and cognitive preoccupation. Maas et al. therefore suggested that cognitive preoccupation is the toxic element of self-concealment and possession of a secret. That is, possession of a secret and self-concealment were negatively associated with quality of life, but after adjusting for cognitive preoccupation, the relation between possession of a secret and well-being turned positive, whereas self-concealment remained a negative predictor of quality of life. This indicates that the distinction between self-concealment and cognitive preoccupation is important, as it provides us with the opportunity to study the effects of secrecy on well-being in more detail.
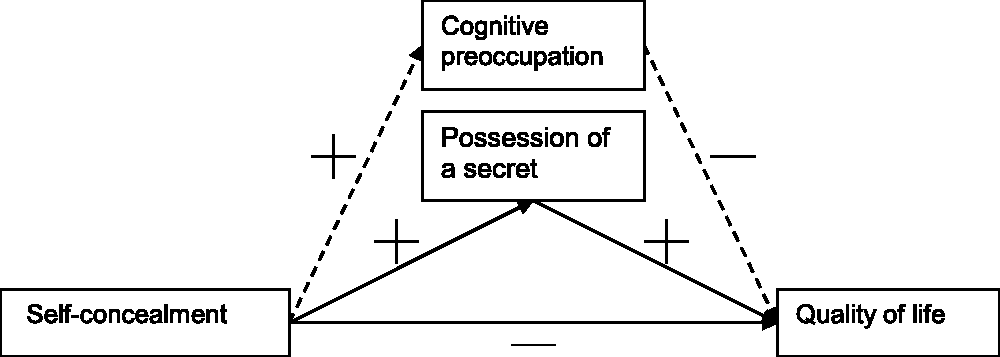
Maas et al.’s (2012) model.
As previous research has only focused on college students and the general population, and the model proposed by Maas et al. (2012) was only tested in a HIV-positive sample who all held the same secret, namely being HIV-positive, the aim of this article was to investigate how secrets affect well-being in a sample consisting of older adults with more diverse secrets. In line with Maas et al. (2012), we used quality of life as a well-being index. Next to assessing general quality of life (WHOQOL-BREF; WHOQOL Group, 1998), we added a module specifically designed to assess quality of life in older adults (WHOQOL-OLD; Power, Quinn, Schmidt, & The WHOQOL group, 2005). The separate components of secrecy—possession of a secret, self-concealment, and cognitive preoccupation—were assessed with the Tilburg Secrecy Scale-25 (TSS25; Wismeijer, 2011), enabling the separate investigation of self-concealment and cognitive preoccupation. We applied the model of Maas et al. (2012) (see Figure 1) to this data.
In line with Kelly and Yip (2006) and Maas et al. (2012), we expected self-concealment to have a negative effect on quality of life, controlling for possession of a secret and cognitive preoccupation. However, in line with the view that cognitive preoccupation is the toxic element of secrecy, we expected possession of a secret to have a positive effect on quality of life, but only when controlling for self-concealment as well as for cognitive preoccupation. Similarly, we expected a negative effect of cognitive preoccupation on quality of life, controlling for self-concealment and possession of a secret.
Methods
Procedure
The data were collected through an online questionnaire, called the Senioren Barometer. The Senioren Barometer is a questionnaire that is published online (www.seniorenbarometer.nl) and is used to explore opinions about varying aspects of life in a population consisting of Dutch citizens aged 50 years and older. The Senioren Barometer is marketed as a tool that could help policymakers to better understand the needs of the elderly and is an initiative of Tilburg University. Each year a new questionnaire is published, probing a myriad of topics, ranging from how elderly cope with the newest developments in information and communication technology, their present medical situation, to how satisfied they are with how the Dutch government addresses their economical needs. Psychological variables are also assessed and, for example, include personality styles and levels of well-being. Participants are constantly recruited by advertisements in the media, as well as by organizations targeted toward elderly people.
Measures
Secrecy
The different elements of secrecy were assessed with the TSS25 (Maas et al., 2012; Wismeijer, 2011), which consists of five subscales each measuring a conceptually independent aspect of secrecy: self-concealment, possession of a secret, cognitive preoccupation, apprehension, and social distance. Unlike Larson and Chastain’s Self-Concealment Scale, the TSS25 thus explicitly distinguishes between the tendency to conceal personal information (self-concealment) and the tendency to worry or ruminate about the secret (cognitive preoccupation). In the sample used by Maas et al. (2012), the self-concealment subscale of the TSS25 correlated strongly with the SCS (r = .73, p < .001). To answer our hypotheses in this study, only self-concealment, possession of a secret, and cognitive preoccupation were used. As asking people directly about a particular secret makes people apprehensive answering questions, the TSS25 asks people to answer how they tend to deal with personal situations involving sharing or concealing information. This means that answers do not reflect behavior or feelings regarding a particular secret people have at that moment, but how they tend to typically behave and feel when they have a secret. Item examples of these scales are as follows: I usually don’t share personal information with other people (self-concealment), I have a secret that I will absolutely never share with anyone (possession of a secret), and I have a secret I think about a lot (cognitive preoccupation). All subscales consist of five positively worded items, which have to be rated on a 5-point Likert-type scale (1 = this does not apply to me at all, 5 = this is very applicable). In this study, Cronbach’s α’s of the Self-Concealment, Possession of a Secret, and Cognitive Preoccupation Scale were .85, .91, and .88, respectively. In addition to the TSS25, we asked how long people have held their secret.
Quality of life
Quality of life was assessed with the 26-item World Health Organization Quality of life Assessment Instrument-BREF (The WHOQOL group, 1998). This version includes four quality of life domains: (a) physical health, (b) psychological health, (c) social relationships, and (d) environment. All questions have to be answered using a 5-point Likert-type scale. A higher score means a higher quality of life. The WHOQOL-BREF is a generic, multidimensional, self-report quality of life measure that is easy to score and has good psychometric properties. In this study, the total score of the four subscales was used, which had a Cronbach’s α of .92.
Quality of life—older adults
The WHOQOL-OLD (Power et al., 2005) was used to assess quality of life of older adults specifically. The WHOQOL-OLD can be used as an add-on module to the WHOQOL-BREF in older populations. It includes 24 questions, which have to be answered on a 5-point Likert-type scale. A higher score means a higher quality of life. The items can be divided into six subscales: (a) sensory abilities, (b) autonomy, (c) past, present, and future activities, (d) social participation, (e) death and dying, and (f) intimacy. In this study, the total score was used, which had a Cronbach’s α of .81.
Statistical Analyses
Path analysis/structural equation modeling (SEM) was carried out using AMOS 20.0. Since missing data (1.2% of all responses) were present, the full information maximum likelihood estimation procedure was applied by estimating a model including means and intercepts. Each variable in the SEM models was measured using the corresponding scale’s sum score. To saturate the model, we added covariances between the errors of possession of a secret and cognitive preoccupation and of the two quality of life scales. These errors and their covariances are not depicted in the figures. Sobel tests were carried out to test for mediation (MacKinnon, 2008). The Sobel test is a well-known and easy to carry out test of mediation (MacKinnon, 2008), albeit slightly less powerful than more advanced tests that are less easy to carry out.
One-tailed tests were executed since all hypotheses were directional. SPSS 19.0 was used for the descriptive analyses. Note that fit indices cannot be provided for saturated models. Post hoc power analyses using G*Power 3.1.1 (Faul, Erdfelder, Lang, & Bucher, 2007) revealed we had a power of 0.54 (1.00) to detect a small (medium) correlation using a one-tailed test (α = .05) with a sample size of 301 and 0.69 (1.00) to detect a small (medium) effect in a regression analysis (fixed model: R2 increase) comparable to the SEM models we fitted.
Results
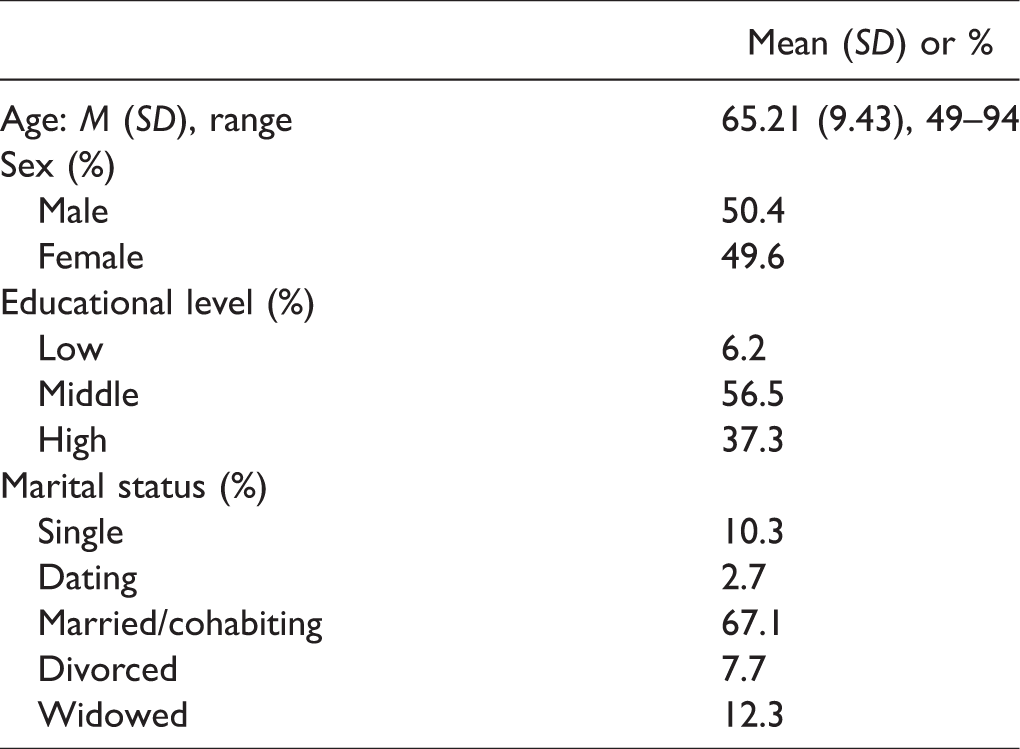
Sociodemographic characteristics are presented in Table 1. Next to the different elements of secrecy, we asked how long people have held their secret (see Methods). The large majority of participants (84.5%) indicated that they have had their secret for more than 10 years. A total of 680 people started this study’s survey, of which 301 participants (44.26%) completed the full majority of the questionnaire. In the data of these 301 participants, only 1.2% of the questionnaire data was missing. Informed consent was obtained from all participants.
Sociodemographic Characteristics of the Sample (N =301).
SEM Analyses
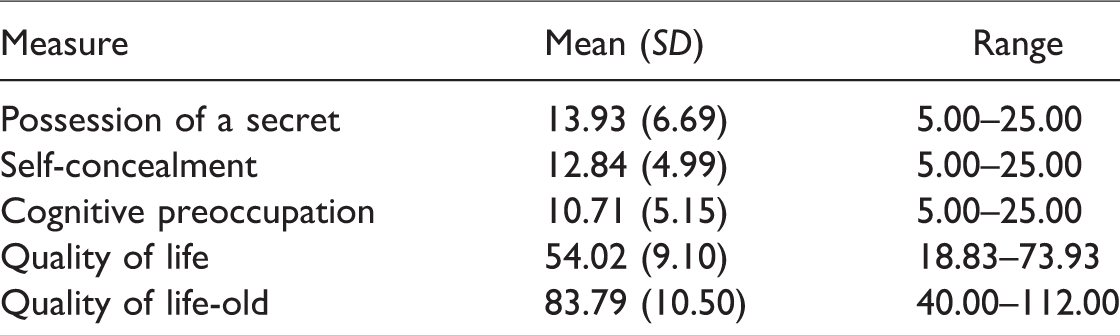
Means and standard deviations of the variables used in the SEM analyses of this study are reported in Table 2, and correlations between the variables are reported in Table 3. The three secrecy scales correlated significantly (all significant at p < .01) with the two quality of life measures. All correlations point to a negative association between secrecy and quality of life, with correlations varying from −.15 (between possession of a secret and quality of life-old) to −.40 (between cognitive preoccupation and quality of life). Correlations between the secrecy scales were medium to strong (varying from r = .39 between possession of a secret and self-concealment to r = .65 between possession of a secret and cognitive preoccupations), and the two quality of life measure were strongly correlated (r = .74).
Descriptive Statistics of the Sample (N =301).
Correlations Between Scale Scores.
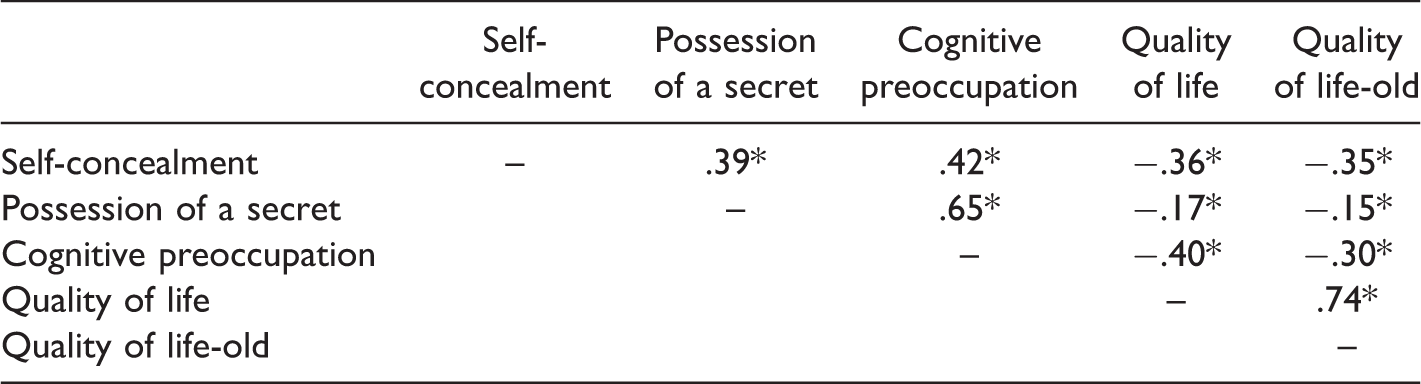
*p < .01.
Mediation of the effect of self-concealment on quality of life by possession of a secret
The model that is represented by the solid lines in Figure 2 was fitted to the data. Table 4 reports the unstandardized estimates of both the total effect of self-concealment (first row) as well as the direct effects of self-concealment and possession of a secret (Model 1). As the total effect is the sum of indirect effects (not shown) and direct effects, the total effect of self-concealment is dissected into self-concealment’s direct effect and an effect via possession of a secret. The total effect of self-concealment was negative (b = −.65 and b = −.70, p < .001). The (total) effect of self-concealment on possession of a secret was positive (b = .53, p < .001). No effect of possession of a secret on quality of life was observed after controlling for self-concealment (b = −.042, p = .60), that is, controlling for self-concealment did not reverse the association between possession of a secret and quality of life but neutralized it. Finally, as expected, self-concealment was still negatively related to quality of life, after controlling for the effect of possession of a secret (b = −.62 and b = −.69, p < .001). Possession of a secret did not mediate the effect of self-concealment on quality of life (Sobel tests’ p < .5 for both measures). Explained variance for possession of a secret was 15%, and 13% and 11% for quality of life and quality of life-old, respectively.
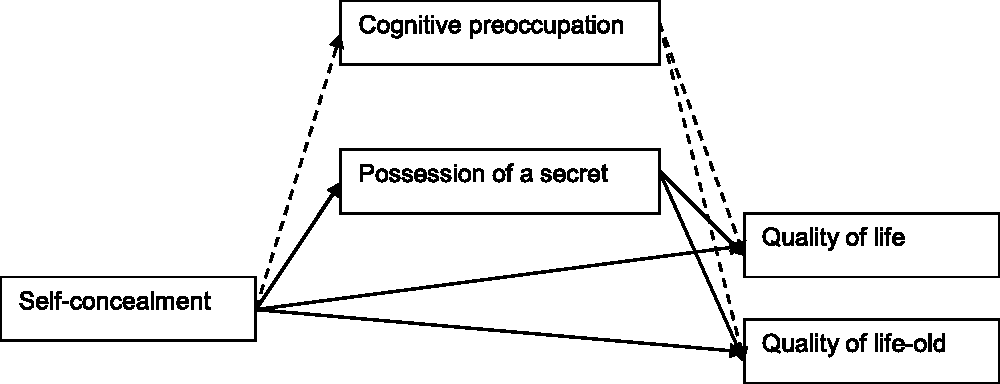
Effect of self-concealment on quality of life mediated by possession of a secret and cognitive preoccupation.
Total Unstandardized Effects of Self-Concealment on Quality of Life, Unstandardized Direct Effects of Self-Concealment, Possession of a Secret, Cognitive Preoccupation on Quality of Life (Standard Errors), and Sobel Tests. a
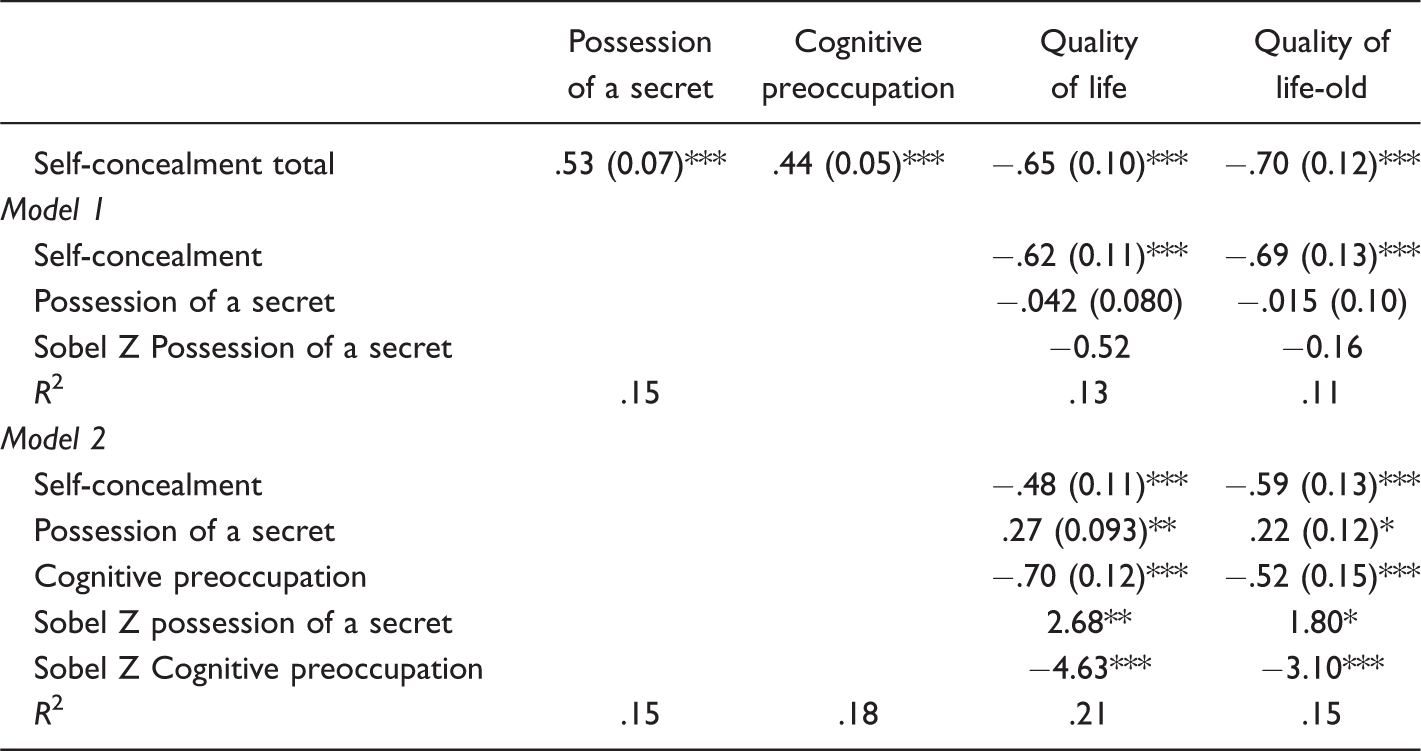
aPredictors are in the rows, criterion variables in the columns.
*p < .05. **p < .01. *** p < .001.
Mediation of the effect of self-concealment on quality of life by possession of a secret and cognitive preoccupation
The unstandardized estimates of the model including both solid and dashed lines of Figure 2 (Model 2) are reported in the lower half and in the first row of Table 4. In line with our hypotheses, self-concealment had a positive effect on cognitive preoccupation (b = .44, p < .001, first row Table 4). Cognitive preoccupation had a negative effect on both quality of life measures (b = −.70 and b = −.52, p < .001) after controlling for the effect of the other secrecy scales, which is in line with our expectations. The Sobel tests indicate that cognitive preoccupation mediated the effect of self-concealment on quality of life (Sobel Z of −4.63 and −3.10, with p < .001).
After controlling for cognitive preoccupation, possession of a secret had a positive effect (b = .27 and b = .22, p < .01) and self-concealment a negative effect (b = −.48 and b = −.59, p < .001) on both quality of life measures, which is in line with our expectations. The Sobel tests indicate that the effect of self-concealment on quality of life is also mediated by possession of a secret, after controlling for cognitive preoccupation (Sobel Z of 2.68 and 1.80, with p = .004 and p = .04, respectively). However, the mediation is inconsistent, that is, the negative direct effect of self-concealment on quality of life becomes stronger after controlling for possession of a secret. The effect of self-concealment on quality of life is reduced from −.65 to −.48 and from −.70 to −.59 on quality of life-old, after controlling for both possession of a secret and cognitive preoccupation. The amount of variance explained was 15% for possession of a secret, 18% for cognitive preoccupation, 21% for quality of life-old, and 15% for quality of life.
Discussion
Previous studies found that possession of a secret is positively associated with well-being after controlling for self-concealment (Kelly & Yip, 2006; Larson et al., 2015) and cognitive preoccupation (Maas et al., 2012). Most studies have focused on college students and the general population. When limiting secrecy research to a relatively young population, it remains unclear how the effects of secret-keeping on well-being unfold when people age. This study therefore examined Kelly and Yip’s and Maas et al.’s secrecy models in a sample consisting of older adults. The TSS25 was used to assess the different elements of secrecy, enabling us to clearly distinguish self-concealment and cognitive preoccupation.
Results of this study showed that the association between possession of a secret and quality of life was negative before controlling for the potential confounding effects of self-concealment and cognitive preoccupation. In line with the study by Maas et al. (2012), we found that the association between possession of a secret and quality of life turned neutral after controlling only for self-concealment, and indeed turned positive after taking both self-concealment and cognitive preoccupation into account. Secrets held by the sample of our current study were more heterogeneous than the sample of Maas et al. as their sample only focused on keeping one’s HIV status a secret. The fact that we replicated the results by Maas et al. could therefore be considered as a strength, since Maas et al.’s model holds in a more heterogeneous sample. Furthermore, as the current sample consisted of older participants and the majority of these participants indicated to have held their secret for more than 10 years, this suggests that Maas et al.’s model may also hold in the longer term.
As Maas et al. (2012) introduced cognitive preoccupation into the model, thereby extending, but not disproving the model of Kelly and Yip (2006), our results are also in line with Kelly and Yip. Kelly and Yip, however, found a positive association between possession of a secret and well-being after controlling for self-concealment, whereas we found no such association. Only after also controlling for cognitive preoccupation we found a positive association between possession of a secret and quality of life. This could be explained by the fact that the Self-Concealment Scale (Larson & Chastain, 1990) used by Kelly and Yip also contains items with a cognitive preoccupation content (Wismeijer, 2011), not allowing for a clear distinction between all secrecy dimensions. Our results are, however, in line with Larson and Chastain’s working model of self-concealment as Larson et al.’s (2015) definition of self-concealment—“a complex-trait-like motivational construct where high levels of self-concealment motivation energize a range of goal-directed behaviors (e.g., keeping secrets, behavioral avoidance, lying) and dysfunctional strategies for the regulation of emotions (e.g., expressive suppression)” (p. 708)—involves cognitive preoccupation. Larson et al. furthermore explain in their article that indeed the maladaptive emotion regulation and the behavioral avoidance make secret-keeping toxic. The TSS25, which we used in this study, is able to measure cognitive preoccupation separately from the tendency to conceal personal information. Indeed as expected, in this study, using the TSS25 secrecy dimensions, self-concealment and cognitive preoccupation were both found to be negatively associated with quality of life. This suggests that the conceptual domain of self-concealment of the TSS25 differs from the Larson and Chastain’s Self-Concealment Scale that has been used in earlier studies. In our opinion, and according to our and Maas et al.’s results, the distinction between self-concealment and cognitive preoccupation is important and should also be considered in future research. Very recently, in a series of 10 studies, Slepian, Chun, and Mason (2017) indeed demonstrated that the frequency of mind-wandering to secrets predicts well-being, rather than active concealment of secrets. In fact, they state that active concealment is not that common, as people are usually not exposed to social situations in which they have to actively conceal their secret on a daily basis.
More research is needed to understand how important the (emotional) content of secrets is in relation to quality of life. In this study, we did not ask people about the content, its emotional valence, or the emotional distress surrounding their secret. In a similar vein, as we were primarily interested in the psychological consequences of secret-keeping, and not in parameters of the secret itself, we also did not assess whether the secret regards oneself or regards secret information of others. This is a limitation of our design. However, the relevance of a secret for the secret-keeper is not as much determined by its exact content or whether it is someone’s own secret or a secret from others. The toxicity of a secret lies primarily in the accompanying cognitive preoccupation it causes (Maas et al., 2012; Pachankis, 2007; Slepian et al., 2017; Wismeijer, 2011). Not only may explicitly asking respondents about the content of their secret prompt respondents to quit the study, also it is difficult to determine categories of secrecy. That is, even within a certain category of secrets, there is an almost infinite number of variations of secrets possible. For example, one can be unfaithful in very different ways and degrees. Hence, likely little is to be gained by exploring the correlations between topics of secrecy and the level of emotional distress or cognitive preoccupation. Notwithstanding, we encourage future studies to assess the degree of emotional distress surrounding the secret as an emotional indicator of the secret, apart from the level of cognitive preoccupation.
Since lot of the secret-keeping was yet unexplained in our study, future research may also address other possible factors explaining secrecy, such as previous experiences, demographics, personality, and the social network. Another important area for future research is to investigate the effects of positive secrets on quality of life, for example, planning to propose to your partner or being pregnant. Are positive secrets, accompanied by a high level of cognitive preoccupation, also negatively related to health in high self-concealers?
Because we adopted a correlational design, we cannot rule out that the causal ordering of the variables is different than the ordering we proposed. Third, variables could also play a role in the relation between possession of a secret, self-concealment, and cognitive preoccupation. For example, instead of the possession of a secret itself driving the positive outcome on well-being, individuals with the self-restraint that enables them to conceal their secret may possess self-regulator skills that in turn may lead to positive outcomes. Future research can clarify this issue.
Another limitation is that we used an online self-report questionnaire, which enables participants to give socially desirable answers. Yet, although secrets potentially form a sensitive topic (enhancing the probability of giving socially desirable answers), in this study we did not ask participants about the content of their secret but asked for general aspects of keeping personal information. This likely reduced the need to provide a socially desirable answer. Nevertheless, that secrecy remains a sensitive topic was reflected in our study by the high amount of participants (56%) who dropped out before completing the entire survey. This could have resulted in biased responses. Some participants may not have liked being reminded about their secret and may therefore have chosen not to complete the survey. However, this only yields a more conservative estimation of the true effects, as individuals with more severe secrets may have dropped out.
Furthermore, as the sample consisted of a voluntary online panel, this means our results are not necessarily generalizable to the general population. As we used a Dutch sample, this limited generalizability also extends to different cultural groups. Other cultural groups may interpret secrecy or stigma differently. For example, in a study on concealing HIV status and stigmatization Rao, Pryor, Gaddist, and Mayer (2008) found that Black respondents indicated greater stigmatization in situations where others discriminated against them, whereas White respondents indicated greater stigmatization in situations of interpersonal rejection. Future research may focus on intercultural differences with regard to secrecy and stigma, as not much is known yet about the differential impact of secrecy between cultures. Future research may also examine whether our findings could be generalized to other areas of (psychological) health, and whether the effects are similar in a clinical or medical context.
Aside from these limitations, this study replicated and extended existing findings in the literature. Our results suggest that disclosing secrets might not always be beneficial for quality of life, which is in line with previous studies (Kelly and Yip, 2006; Maas et al., 2012) that investigated younger samples. Our findings also corroborate the preoccupation model of Lane and Wegner (1995) and indicate that it is important to distinguish between self-concealment and cognitive preoccupation. Self-concealment and cognitive preoccupation seem to affect self-reported quality of life negatively, whereas sole possession of a secret has a positive effect on self-reported quality of life. Contrasting popular belief, quality of life may be enhanced, rather than diminished, by keeping secrets, if people do not have a secretive personality and are not preoccupied with their secrets. The fact that the secrecy model of Maas et al. holds in an older sample of whom the majority have held their secret for more than 10 years may suggest that quality of life is also not affected negatively by keeping secrets in the long term. Although future research is needed to further generalize and elucidate these findings, secret-keeping is an important area of research as it affects people across their lifespan and in multiple areas of their lives.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.