
Abstract
Objective
Autism spectrum disorder (ASD) can affect vision both directly through central nervous system involvement and indirectly by complicating ophthalmological examinations due to limited eye contact and poor cooperation. Visual impairments may exacerbate social interaction difficulties and affect motor development in individuals with ASD. Previous studies reported ophthalmological involvement in 27-71% of children with ASD, including refractive errors, strabismus, and amblyopia. The purpose of this study was to investigate visual impairments in children with ASD and examine their relationship with ASD severity, anxiety levels, and attention disorders, while highlighting the importance of routine ophthalmological examinations.
Method
Participants were 57 children aged 7-18 years diagnosed with ASD. All except for 2 participants underwent comprehensive ophthalmological examinations and were assessed using the Childhood Autism Rating Scale (CARS), Turgay DSM-IV-based Child and Adolescent Behavior Disorders Screening Scale (T-DSM-IV-S), Strengths and Difficulties Questionnaire (SDQ), Screen for Child Anxiety Related Emotional Disorders (SCARED), and Repetitive Behaviors Scale-Revised (RBS-R).
Results
Visual impairment was detected in 24 (42.1%) participants, with exotropia (21%), stereopsis deficits (15.8%), and convergence insufficiency (5.3%) being the most common findings. The visually impaired group showed significantly higher scores in attention deficit (P < .001), peer relationship problems (P = .003), social phobia (P < .001), stereotypic behaviors (P < .001), and self-injurious behaviors (P < .001) compared to those without visual impairment.
Conclusions
Visual impairments significantly impact attention, peer relationships, social anxiety, and repetitive behaviors in children with ASD. Early identification and treatment of visual disorders through routine ophthalmological screening may improve overall outcomes in this population.
Keywords
Introduction
Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder that emerges in early childhood as a result of interactions between genetic and environmental factors. It is characterized by difficulties in social relations and communication, repetitive behaviors, and restricted areas of interest, which often persist into adulthood. 1 Revisions to the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5), have brought increased attention to sensory processing disorders in individuals with ASD, incorporating atypical sensory features into the diagnostic criteria.1,2 These atypical sensory features, reported in approximately 95% of individuals with ASD, may involve multiple sensory modalities, including taste, touch, hearing, smell, and vision. 3 Hypo- and/or hypersensitivity, particularly to visual stimuli such as light, color, and movement, may negatively affect visual perception and quality of life in individuals with ASD.3,4 Additionally, visual impairments such as reduced fixation, visual orientation difficulties, and abnormal visuospatial perception further exacerbate the social and cognitive challenges associated with ASD. 5
In addition to abnormalities in visual processing, ASD may contribute to other visual impairments through direct and indirect mechanisms. 4 Environmental factors, such as prematurity, congenital infections, and nutritional deficiencies, are crucial in the etiology of both ASD and visual disorders, including vision loss, blurred vision, and strabismus. Furthermore, several genetic conditions, such as Fragile X Syndrome, Down syndrome, Noonan syndrome, tuberous sclerosis, and neurofibromatosis type 1, are associated with an increased risk of both ASD and visual impairment. Beyond these shared etiologies, the common embryological origin of the eye and brain suggests that the direct effects of ASD on the central nervous system may contribute to visual impairments.4,5 Moreover, symptoms specific to ASD, such as limited eye contact, stereotyped behaviors, and poor cooperation, may indirectly affect visual functions by complicating ophthalmological examinations. 5
The reported incidence of ophthalmological involvement in children with ASD ranges from 27-71%.6,7 Vision and ocular disorders have been shown to be significantly more prevalent in children with ASD than in those without ASD. 4 Among children with ASD who have ophthalmological involvement, refractive errors have been reported in 20-44%, strabismus in approximately one-third, and amblyopia in about one-fifth. 8 Furthermore, a meta-analysis revealed that the prevalence of strabismus in individuals with ASD is 4.72 times higher than that in individuals without ASD. 4
There is strong evidence that individuals with visual impairment, regardless of ASD, experience difficulties in social interaction and communication.9,10 Visual impairment may lead to reduced eye contact and exacerbate social interaction difficulties, particularly in individuals with ASD. Additionally, impairments in distance and depth perceptions in individuals with ASD may adversely affect their motor skills.11,12 Consistent with these findings, studies have reported significant improvements in motor skills, learning capacity, and social functioning, along with reduced repetitive behaviors, in individuals with ASD following correction of visual impairments. 4
Thus, this study aimed to investigate visual impairments in children and adolescents with ASD and to compare those with and without visual impairment in terms of ASD severity, anxiety levels, and attention-related disorders. This study also aimed to raise awareness of visual impairments associated with ASD and to emphasize the importance of routine ophthalmological examinations.
Materials and Methods
Population and Sample
The study population comprised patients aged 7-18 years who were being followed-up with a diagnosis of ASD based on the DSM-5 diagnostic criteria at the Ege University Faculty of Medicine, Department of Child and Adolescent Mental Health and Diseases Developmental Disorders and Autism Polyclinic. To minimize selection bias, all eligible patients consecutively followed in the outpatient clinic were invited to participate either during routine visits or via telephone contact. Inclusion was limited to verbally communicative individuals with sufficient cooperation to complete ophthalmological and psychometric assessments, as these procedures require active participation. Accordingly, non-verbal patients, those with severe functional impairment, and individuals with comorbid genetic disorders were excluded. A total of 78 children and adolescents met the inclusion criteria and were invited to participate in the study. Of these, 57 (73.1%) attended the outpatient clinic, completed the ophthalmological and psychometric assessments, and were included in the final analysis. Detailed information on the study was provided to the parents of all patients, as well as to patients with sufficient communication skills. Written informed consent was obtained from all parents in accordance with the Declaration of Helsinki. The study was approved by the Ege University Clinical Research Ethics Committee.
Data Collection
A sociodemographic data form was completed during interviews with all patients and their parents. ASD severity was measured using the Childhood Autism Rating Scale (CARS). Parents completed the Turgay Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV)-based Child and Adolescent Behavior Disorders Screening and Rating Scale Parent Form (T-DSM-IV-S-P), Strengths and Difficulties Questionnaire (SDQ) Screen for Child Anxiety Related Emotional Disorders Parent Form (SCARED-P), and Repetitive Behaviors Scale-Revised (RBS-R). All patients underwent a comprehensive ophthalmological examination at the Department of Ophthalmology, Ege University Faculty of Medicine.
Sociodemographic Data Form
Patient age, sex, developmental stage, school attendance, and family-related information were recorded using a form created by the researchers.
Turgay DSM-IV-Based Child and Adolescent Behavior Disorders Screening and Rating Scale-Parent Form (T-DSM-IV-S-P)
This 41-item, 4-point Likert-type scale was developed by Turgay (1994). It consists of inattention (9 items), hyperactivity (6 items), impulsivity (3 items), oppositional defiant disorder (8 items), and conduct disorder (15 items) subscales. Each item is assigned a score between 0 (absent) and 3 (severe). 15 The validity and reliability of the Turkish version of the scale were assessed by Ercan et al. 16
Strengths and Difficulties Questionnaire-Parent Form (SDQ-P)
This 25-item, 3-point Likert-type scale was developed by Goodman in 1997 to evaluate emotional and behavioral problems 17 and was adapted into Turkish by Guvenir et al. 18 The scale consists of inattention/hyperactivity, conduct problems, emotional symptoms, peer relationship problems, and prosocial behaviors subscales. Each item is assigned a score between 0 (not true) and 2 (certainly true). The total difficulty score is calculated by summing the scores on the first 4 subscales.17,18
The Screen for Child Anxiety-Related Emotional Disorders-Parent Form (SCARED-P)
This 41-item, 3-point Likert-type scale was developed by Birmaher et al (1997) to evaluate anxiety in children. 19 The scale assesses disorder symptoms of generalized anxiety (9 items), separation anxiety (8 items), social anxiety (7 items), somatic/panic (13 items), and social phobia (4 items). Each item is assigned a score between 0 (not true) and 2 (often true). A total score of 25 or higher indicate the presence of clinically significant anxiety. 19 The validity and reliability studies of the Turkish version of the scale were conducted by Çakmakçı. 20
Repetitive Behaviors Scale-Revised (RBS-R)
This 43-item, 4-point Likert-type scale was developed by Bodfish et al to evaluate restrictive, repetitive, and stereotyped behaviors. 21 This scale consists of stereotyped, self-injurious, compulsive, routine, sameness, and restricted behavior subscales. Each item is assigned a score between 0 (behavior does not occur) and 3 (behavior occurs and is a severe problem). Higher scores indicate greater symptom severity of repetitive behaviors and restricted interest. The validity and reliability studies of the Turkish version of the scale were conducted by Akçamuş et al in 2019. 22
Statistical Analysis
Statistical analyses of the collected data were conducted using SPSS version 25.0 (IBM Corp., Armonk, NY, USA, 2017). The results of the statistical analyses are expressed in descriptive statistics, ie, mean ± standard deviation values for continuous (numerical) variables with a normal distribution, median with minimum and maximum values for continuous (numerical) variables without normal distribution, and numbers (n) and percentage (%) values for categorical variables. Normality of numerical variables was assessed using Shapiro-Wilk and Kolmogorov-Smirnov tests. Differences between 2 independent groups were analyzed using the independent sample t-test for normally distributed variables and the Mann-Whitney U test for non-normally distributed variables. A P value ≤ .05 was considered statistically significant.
Results
Sociodemographic Characteristics of Participants and Their Parents
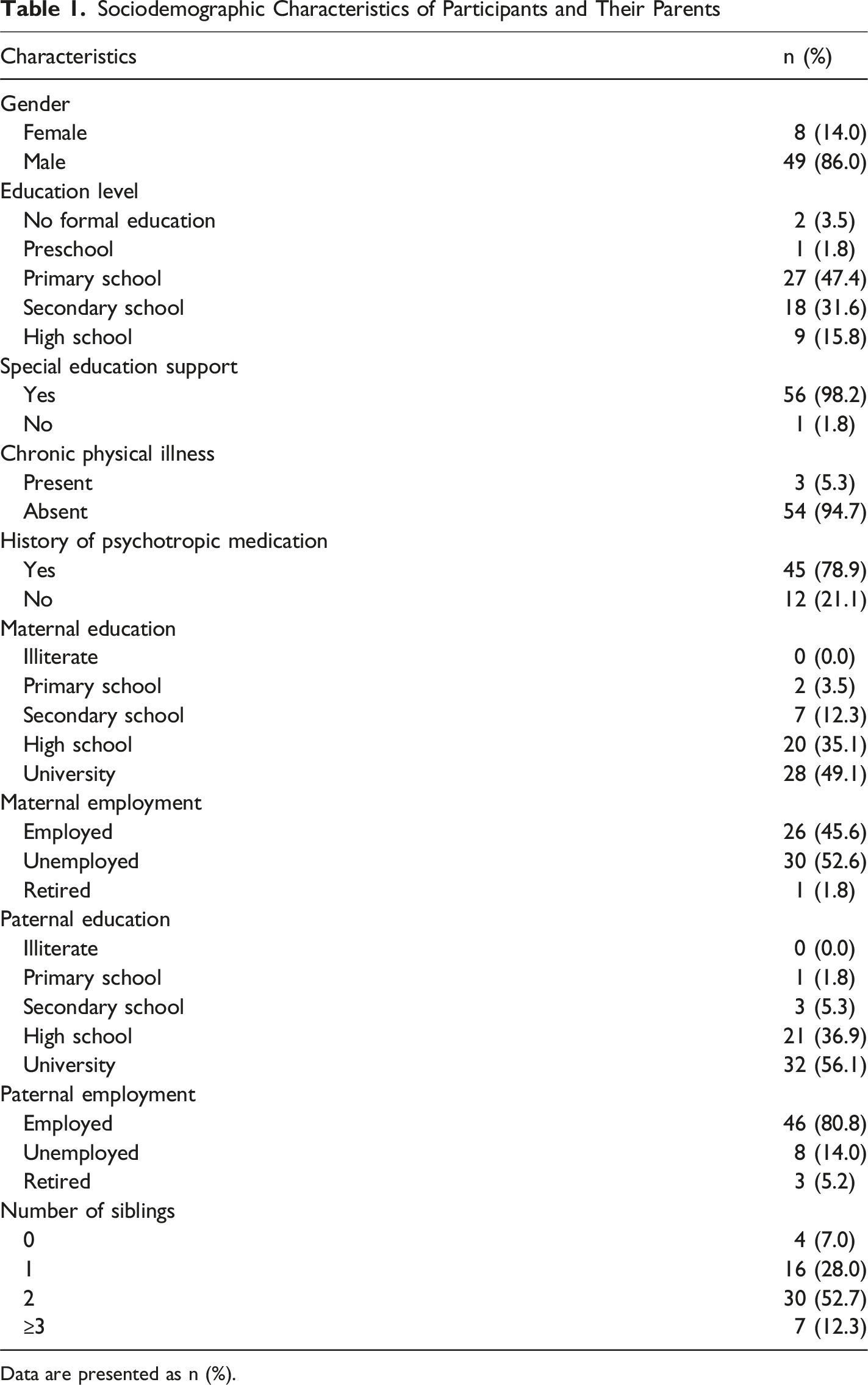
Data are presented as n (%).
Baseline Demographic Characteristics of the Visual Impairment Group (VIG) and the Non-Visual Impairment Group (NVIG)
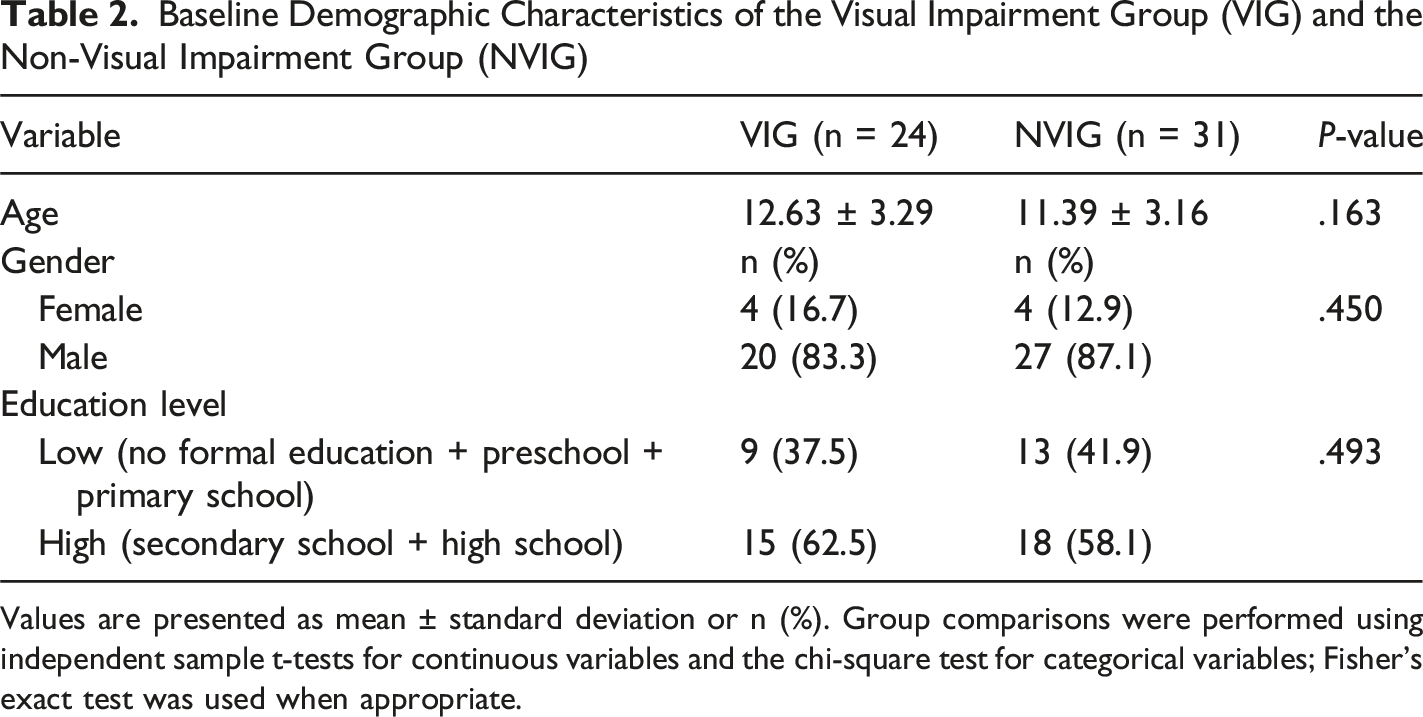
Values are presented as mean ± standard deviation or n (%). Group comparisons were performed using independent sample t-tests for continuous variables and the chi-square test for categorical variables; Fisher’s exact test was used when appropriate.
Visual impairment was detected in 24 patients (42.1%). Among these patients, 12 (%21) had exotropia, 9 (%15.8) had stereopsis, and 3 (%5.3) had isolated convergence insufficiency.
Further analysis of strabismus subtypes among patients with ASD and visual impairment revealed intermittent exotropia in 9 patients (15.8%), esotropia in 2 (3.5%), and left monocular exotropia in 1 (1.8%). No cases of amblyopia were detected.
No significant difference in ASD severity was observed between the visually impaired group (VIG) and the non-visually impaired group (NVIG)
Comparison of Scale Scores Between the Visual Impairment Group (VIG) and Non-Visual Impairment Group (NVIG)
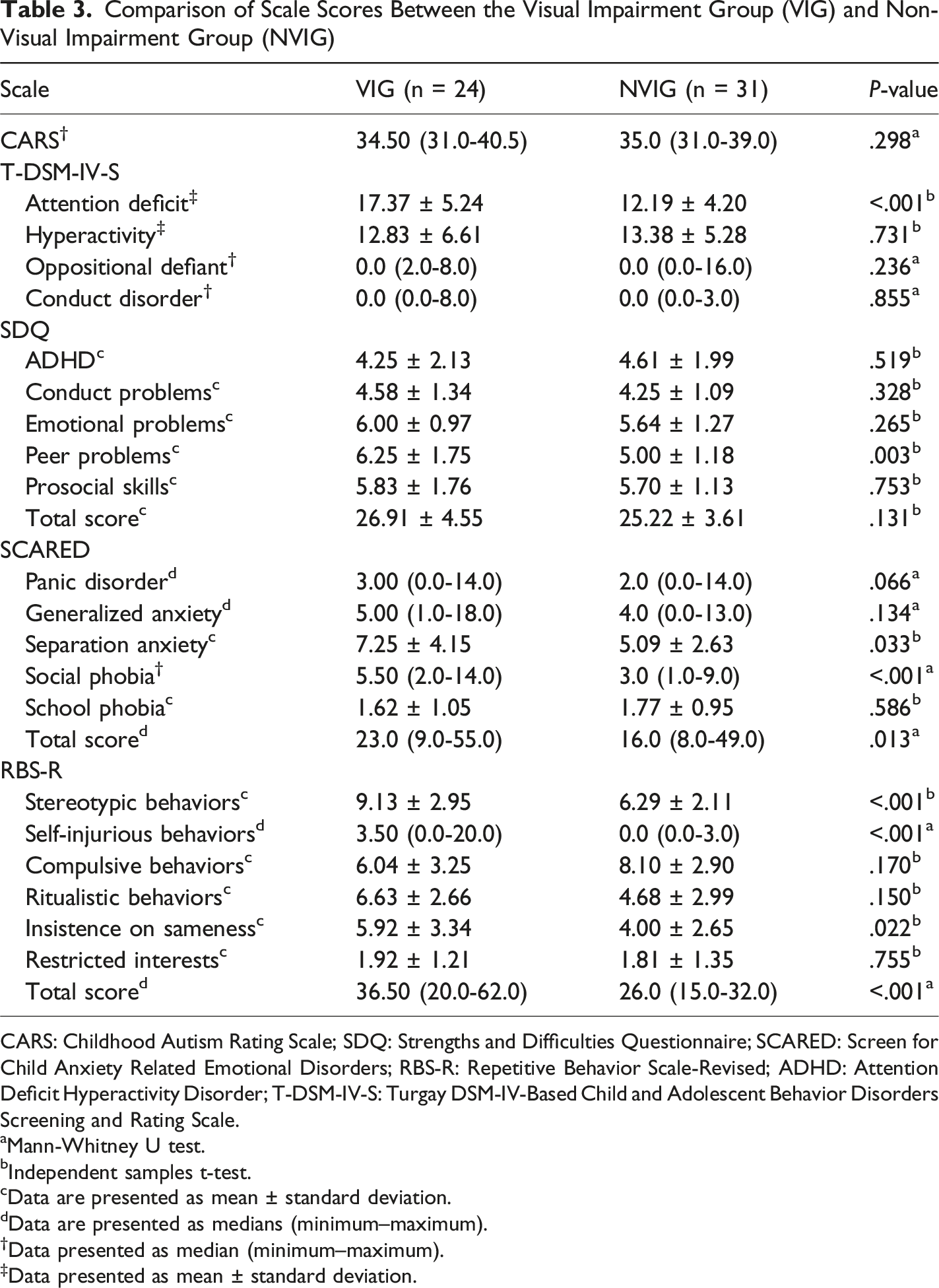
CARS: Childhood Autism Rating Scale; SDQ: Strengths and Difficulties Questionnaire; SCARED: Screen for Child Anxiety Related Emotional Disorders; RBS-R: Repetitive Behavior Scale-Revised; ADHD: Attention Deficit Hyperactivity Disorder; T-DSM-IV-S: Turgay DSM-IV-Based Child and Adolescent Behavior Disorders Screening and Rating Scale.
aMann-Whitney U test.
bIndependent samples t-test.
cData are presented as mean ± standard deviation.
dData are presented as medians (minimum–maximum).
†Data presented as median (minimum–maximum).
‡Data presented as mean ± standard deviation.
Discussion
Visual impairment may adversely affect children’s language, motor, cognitive, and social development. Children with visual impairments often acquire movement and motor skills later than their peers without visual impairments. 23 Inadequate perception of facial expressions and gestures in visually impaired children may render them unable to correctly interpret social cues, resulting in delayed social development.24,25 Visual impairments accompanied by neurodevelopmental disorders may increase the severity of existing symptoms and cause lifelong difficulties in daily functioning, social participation, and health outcomes. 26
Studies have shown that both ASD and autistic traits are significantly more prevalent among children with congenital visual impairment.27,28 An epidemiological study conducted in Scotland reported that the prevalence of autism in visually impaired children and young adults was 3 times higher than that in the general population. 29 Another study suggests that visual impairments accompanying ASD may contribute to deficits in social communication and interaction. 30 However, in the present study, no significant difference in ASD severity was detected between patients with and without visual impairment. This discrepancy from previous findings may be partly attributed to the relatively small sample size of our study. Additionally, the heterogeneity of visual impairments in individuals with ASD suggests that individual differences may influence outcomes. For example, specific visual impairments, such as strabismus or low stereopsis, may have a greater impact on social communication skills, whereas other vision problems may exert less influence.
The incidence of ophthalmological disorders, particularly refractive errors, strabismus, and amblyopia, is higher in children with ASD. 7 In a study published by Ikeda et al. 31 in 2013 that evaluated ophthalmological findings in 154 children with ASD, ocular pathology was detected in 40% of the children; 21% had strabismus (most commonly accommodative exotropia, followed by non-accommodative esotropia and infantile esotropia), and 10.4% had amblyopia. Similarly, in a study evaluating ophthalmological findings in Turkish children with ASD published by Kabataş et al., 32 it was reported that 26.9% of the patients had an ocular pathology, 22.5% had a significant refractive error (most commonly hypermetropia), and 8.6% had strabismus. Conversely, another study conducted in Turkey of 24 patients diagnosed with ASD, strabismus was not detected. 33 Herein, the incidence of strabismus was 21% in our sample of 57 patients, whereas amblyopia was not detected in any patient. Unlike in the other 2 studies, intermittent exotropia was the most common strabismus subtype observed. These discrepancies across studies may be attributed to the fact that sensory sensitivity, limited eye contact, stereotypies, and atypical features in the visual processing of children with ASD make it difficult for them to cooperate during ophthalmological examinations, which affects the consistency and accuracy of the collected data.
Studies have reported that exotropia is more prevalent than esotropia in children with neurological or developmental disorders.34,35 Phillips et al suggested that exotropia may represent a relatively mild manifestation of neurodevelopmental disorders, including autism. 35 In a study evaluating eye posture in 34 children using the occlusion test, Scharre and Creedon 36 identified significant strabismus in 7 children (21%), 6 of whom had exotropia. Our findings are consistent with these observations.
Studies on peer relationships among individuals with visual impairments, including blindness and low vision, indicate that they face certain difficulties in their social interactions, face challenges in establishing and maintaining peer relationships, and are at increased risk of social isolation. 37 Children with visual impairment have been shown to interact less frequently with their peers than other children 38 and are less likely to initiate social interactions. 39 Huurre and Aro 40 reported that adolescents with visual impairment experience greater difficulties in social relationships and have trouble forming friendships. Similarly, Lifshitz et al (2007) found that friendship quality among individuals with visual impairment was lower than that among those without visual impairment. They attributed this to limited access to visual cues, lack of social skills, and negative societal attitudes toward the visually impaired. 37 Consistent with these findings, we identified that visual impairment may further exacerbate social communication difficulties, a core symptom of ASD, thereby hindering the formation of social bonds and the development of sustainable relationships.
In a study of 87 children with visual impairment and 102 with developmental problems concomitant to visual impairment, it was reported that the total SDQ-P and SDQ subscale scores of children with developmental problems and visual impairment were significantly higher than those of children without developmental problems. 23 In another study comparing 158 adolescents affected by visual impairment with 158 adolescents without visual impairment, those with visual impairment experienced more peer relationship and emotional problems than their healthy peers, and their SDQ total scores were higher. 41 Similarly, the SDQ-P peer relationship problem subscale score was significantly higher in the VIG than that in the NVIG group. We also found that the total SDQ-P and SDQ-P conduct problems, emotional symptoms, and prosocial behavior subscale scores were higher in the VIG than those in the NVIG, although not significantly different.
Cognitive functions such as attention and memory are impaired in children with low vision and other visual impairments; their attention capacity is lower than that of healthy children, and therefore their learning processes are negatively affected. 42 Visual impairments, such as strabismus and refractive errors, may present with symptoms that mimic the neurocognitive features of attention deficit hyperactivity disorder (ADHD). 43 Early onset visual impairment may increase the risk of ADHD, particularly if not treated appropriately in a timely manner. 44 Furthermore, we found that visual impairments accompanying ASD may further exacerbate attentional difficulties and negatively affect cognitive functions and learning processes.
DeCarlo et al found that 47.4% of children with low vision due to refractive errors had at least 1 type of anxiety disorder. 45 A school-based study conducted on adolescents aged 11-18 found a strong correlation between low vision and anxiety. 46 In another study, 8 of 42 children with strabismus were diagnosed with social phobia, and it was found that the total SCARED and SCARED separation anxiety disorder and social phobia symptoms subscale scores were significantly higher in patients with strabismus than those in control subjects. 47 Consistent with these findings, we detected higher levels of social anxiety in patients with ASD and visual impairments.
Motor stereotypies, a core symptom of ASD, are common among visually impaired individuals. 11 Studies have suggested that these stereotypical behaviors are caused by several factors, such as motor limitations, reduced exploratory capacity, limited environmental conditions, reduced sensory stimulation, and a lack of mobility. 48 However, no study has directly examined the effect of visual problems on stereotypical behaviors in children with ASD. Our findings revealed that visual impairment increases not only motor stereotypies but also self-injurious behaviors, suggesting that vision problems have a negative impact on the behavioral patterns of individuals with ASD.
Study Limitations
This study had limitations. First, the relatively small sample size may have limited statistical power, particularly for detecting associations between ASD severity and visual impairment. Accordingly, a post-hoc power analysis was conducted using G*Power software indicated that the present sample size provided limited statistical power to detect small-to-moderate effect sizes. Therefore, the lack of a significant association should be interpreted cautiously and may reflect insufficient power rather than a true absence of association.
Second, the absence of a typically developing control group limits the ability to isolate the effects of visual impairment independent of ASD and direct comparisons with non-ASD populations, thereby affecting the generalizability of the findings. Third, this was a single-center study; hence, the results may not be fully representative of broader ASD populations or other clinical and geographic settings. Fourth, the cross-sectional design and the absence of follow-up data after ophthalmological interventions preclude conclusions regarding the long-term effects of vision correction on behavioral, emotional, and social outcomes in children with ASD.
Fifth, the study sample primarily consisted of verbally communicative children and adolescents with mild-to-moderate ASD, which may limit the applicability of the findings to individuals with more severe impairments. In addition, formal standardized intelligence quotient assessments were not performed, and intellectual functioning may have acted as a potential confounding factor. Although psychiatric comorbid symptoms were assessed using validated dimensional scales, formal DSM-based psychiatric diagnoses and stratified analyses by specific comorbidities (eg, ASD with ADHD) were not performed. Furthermore, while psychotropic medication use (eg, stimulants and antidepressants) was common and documented, medication-specific effects on ophthalmological findings could not be systematically analyzed due to sample size limitations and treatment heterogeneity.
Conclusions
This study demonstrates that visual impairments accompanying ASD are associated with significant adverse effects on attention, peer relationships, social anxiety, and repetitive behaviors, including motor stereotypies and self-injurious behaviors. Vision-related problems appear to be common in children and adolescents with ASD and, if not identified and treated in a timely manner, may further exacerbate existing difficulties in social communication and behavioral regulation.
From a clinical perspective, visual impairments may intensify social anxiety and peer relationship difficulties by limiting eye contact, facial recognition, and the interpretation of non-verbal social cues—domains that are already challenging for individuals with ASD. Thus, early identification and appropriate ophthalmological interventions, such as refractive correction and treatment of strabismus or convergence insufficiency, may enhance engagement in social skills training, peer-based interventions, and school-based rehabilitation programs.
Therefore, integrating routine ophthalmological screening and timely visual interventions into multidisciplinary ASD care may indirectly support psychosocial rehabilitation outcomes, improve overall functioning, and enhance quality of life in children and adolescents with ASD.
Footnotes
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.