
Abstract
Objective
The purpose of this study was to investigate the prevalence of depression, anxiety disorder, hopelessness, and suicide among first-degree relatives of patients hospitalized in medical and anesthesia intensive care units at an academic medical centre.
Methods
In this case–control study conducted in Türkiye, 32 first-degree relatives of 32 patients hospitalized for 14 days or more in intensive care units and 32 healthy volunteers were assessed. The Beck Depression Scale (BDS), Beck Anxiety Scale (BAS), Beck Hopelessness Scale (BHS), and Suicide Probability Scale (SPS) were administered to participants.
Results
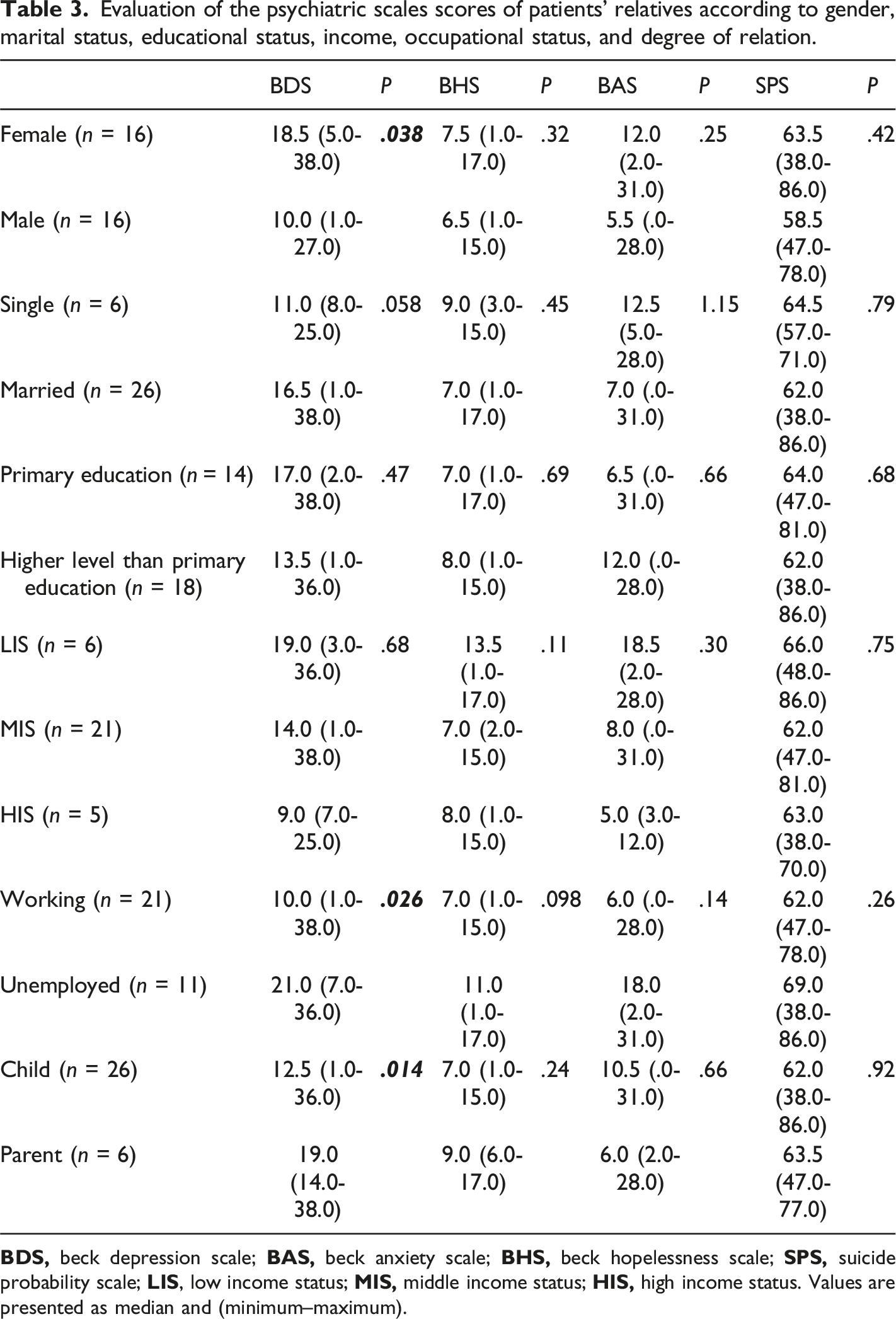
The mean age of patients’ relatives was 42.1 ± 11.6 years and that of the controls was 43.0 ± 11.3 years. The median scores for the BDS, BHS, and SPS were significantly higher among the relatives of the patients than among controls (P = .008, P = .013, and P = .001, respectively). Based on cutoff scores for the BDS and BAS, significant depressive symptoms were observed in 56.3% of the relatives of the patients and significant anxiety symptoms were observed in 46.9%. Among patients’ relatives, the median score for the BDS was significantly higher among female participants than among male participants (P = .038).
Conclusions
First-degree relatives of patients hospitalized in intensive care units have a higher prevalence of depression, hopelessness, and suicidality. Female relatives scored higher on depressive symptoms than male relatives. Psychiatric evaluation/screening of the relatives of patients hospitalized in intensive care units in Turkey is essential.
Introduction
An intensive care unit (ICU) is a multidisciplinary speciality department where patients with, or at risk of, acute and life-threatening organ dysfunction receive comprehensive care. 1 Family members of patients admitted to the ICU are exposed to a potentially traumatic environment. 2 Fear of losing a loved 1, uncertainty about the disease course, the unfamiliar environment, the instruments and equipment connected to the patient, and similar reasons may cause family members to experience psychiatric distress, and they may require psychological support. 3 Emotional conflicts, financial concerns, role changes, and disruptions of routine may also cause anxiety and depression among them. 4
In addition to high levels of traumatic stress, anxiety, and depression, family members may also experience symptoms such as fatigue, sadness, and fear during a patient’s stay in the ICU. 5 When clinicians recognise this situation, long-term negative outcomes, such as complicated grief and major depression among family members, can be prevented. 5
This study aimed to investigate the probability of depression, anxiety, hopelessness, and suicidal thoughts among first-degree relatives of patients hospitalised in the ICU. It also aimed to determine the relationship between these parameters and sociodemographic and clinical factors, such as the Glasgow Coma Scale (GCS) and need for mechanical ventilation (MV).
Method
Sample
This case–control study included 32 first-degree relatives of 32 patients who were followed up and treated for 14 days or longer in the Internal Medicine and Anaesthesia ICUs of Akdeniz University Faculty of Medicine Hospital between May and November 2023. Thirty-two healthy volunteers with similar sociodemographic characteristics were also included. The responsible physician communicated with the families daily and granted them a 30-minute visit. During the interviews, the patients’ mechanical ventilator dependency, APACHE II Score, and GCS score were assessed. The APACHE II Score is a predictor of intensive care mortality and predicts the estimated percentage of death; the GCS is used to assess neurological damage and a score of less than 8 points is associated with poor neurological status. Scores from these assessments were reported and explained to the patients’ relatives. The relatives who agreed to participate in the study were interviewed individually in a private room after the 14-day hospitalisation period.
The inclusion criteria were as follows: being a first-degree relative of a patient hospitalised in the ICU for ≥14 days; being ≥18 years of age; and having at least a primary education. The exclusion criteria were as follows: being the relative of a patient hospitalised in ICU for <14 days and having a known history of psychiatric illness or medication use. In this study, 51 patients hospitalised in ICU for ≥14 days were identified. However, eight patients’ relatives were excluded because they were not first-degree relatives, six because they were taking psychiatric medication at the time and being psychiatric followed up, and five because did not agree to participate.
Individuals comprising the control group were selected from healthy people who voluntarily participated. They underwent psychiatric evaluation for routine driver’s licence competency by a psychiatrist involved in our study; those who met the inclusion criteria were included. Volunteers who were deemed physically and mentally healthy, had no first-degree relatives with health problems, and did not use medication were included as participants in the control group.
Instruments and assessments
The sociodemographic data form, Beck Depression Scale (BDS), Beck Anxiety Scale (BAS), Beck Hopelessness Scale (BHS), and Suicide Probability Scale (SPS) were administered to all participants.
The BDS measures the vegetative, emotional, cognitive, and motivational symptoms of depression. 6 Participants are asked to score each item between between zero (0) and three (3), taking into account the previous one (1) week. A total score of 0-13 on the inventory indicates minimal depression, 14-19 indicates mild depression, 20-28 indicates moderate depression, and 29-63 indicates severe depression. 7
The BAS focuses on the somatic symptoms of anxiety. Developed as an important measure to distinguish between anxiety and depression, responses are rated on a four-point Likert scale and with scores ranging from 0 (not at all) to 3 (severely). Suggestions for interpreting scores are 0-9, normal or no anxiety; 10-18, mild to moderate anxiety; 19-29, moderate to severe anxiety; and 30-63, severe anxiety. 8
The 20-item self-report BHS is frequently encountered in the literature and has high validity and reliability. 9 The scale determines the degree of pessimism an individual holds towards the future. Each answer compatible with the given key is worth one point, and those incompatible are not allocated any points. The total score obtained is considered the hopelessness score. The score range of the scale is between 0 and 20. The scale consists of three factors: Future Related Emotions, Loss of Motivation, and Future Related Expectations. 10
The SPS was developed by Cull and Gill (1990) to identify adolescents and adults at risk of attempting suicide. The total score of the scale is calculated using a rubric ranging from 1 to 4 for each question. The total score that can be achieved with the scale varies between 36 and 144. All scores obtained from the scale indicate an increased likelihood of suicide. 11
All participants signed informed consent forms and the study was explained to them in detail. Written ethical approval (decision number, KAEK-343 dated 26 April 2023) was obtained from the Akdeniz University Faculty of Medicine Clinical Research Ethics Committee for the study. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Power analysis
To perform a power analysis, 14 pilot data points were collected from both groups due to the lack of similar studies in the literature. We used these pilot data to determine the effect size based on the mean and standard deviation of the BDS scores between the groups. Power analysis was conducted by assuming a 5% type I error rate (alpha) and a 1% to 20% type II error rate (beta). Based on these assumptions, we aimed to conduct the study with at least 38 individuals, with at least 19 individuals in each group. The analysis was performed using the trial version of MedCalc statistical software (MedCalc Software Ltd, Ostend, Belgium).
Statistical analysis
IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA) was used to statistically evaluate the data collected. The Shapiro–Wilk or Kolmogorov–Smirnov tests were used to evaluate whether the variables obtained as measurement values were normally distributed. Continuous variables are expressed as mean ± standard deviation (SD) or median (minimum) according to a normal distribution. Categorical variables are expressed as number (n) and percentage (%). Pearson’s chi-square and Fisher’s exact tests were used to compared categorical variables. To compare numerical data, an independent group t test was used for normally distributed independent variables and a Mann–Whitney U test was used for non-normally distributed independent variables. Correlations were evaluated using Pearson’s or Spearman’s rho tests according to the normal distribution. Statistical significance was set at P < .05.
Results
Sociodemographic characteristics of the study and control groups.
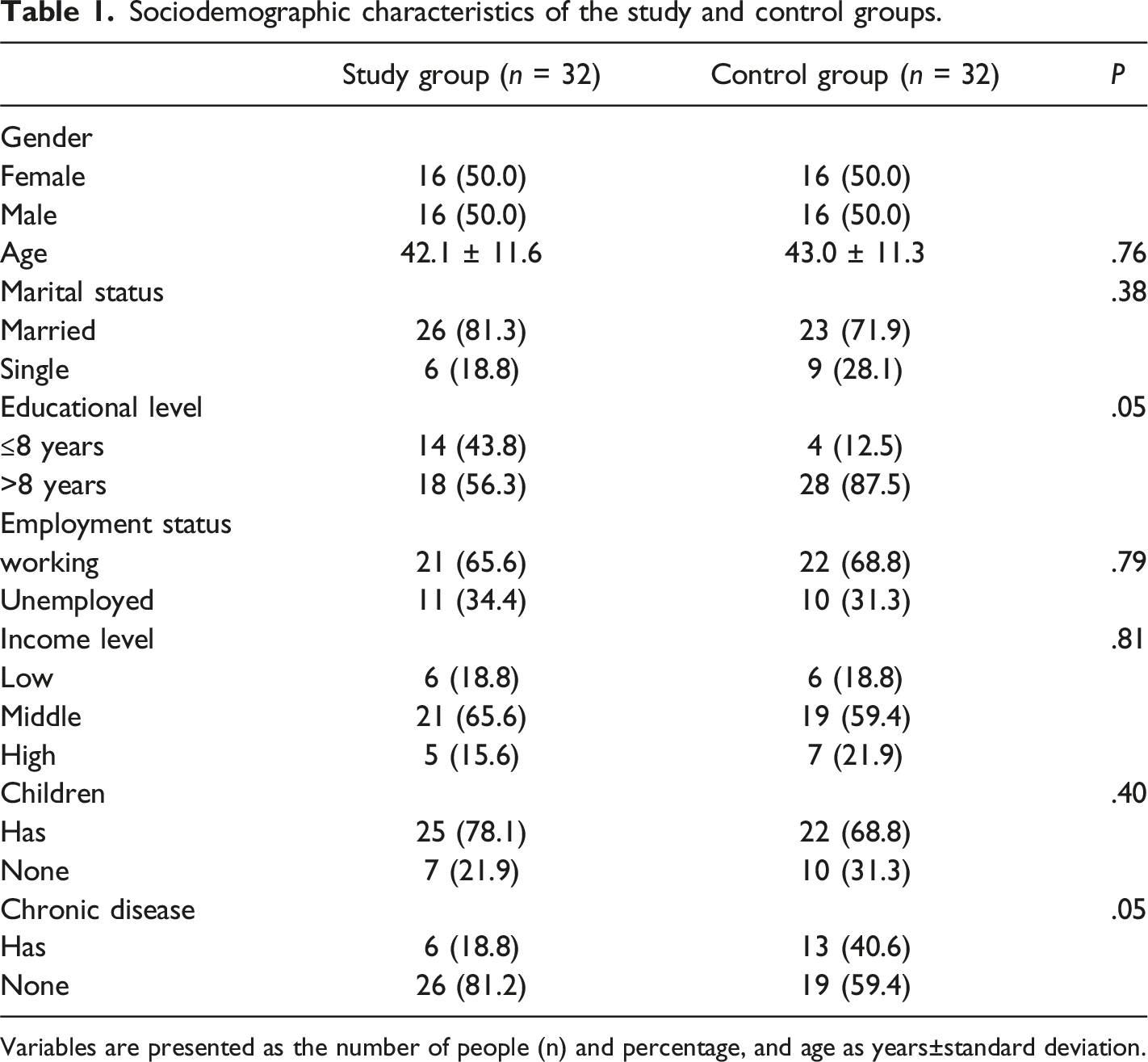
Variables are presented as the number of people (n) and percentage, and age as years±standard deviation.
Comparison of psychiatric scales between the study and control groups.
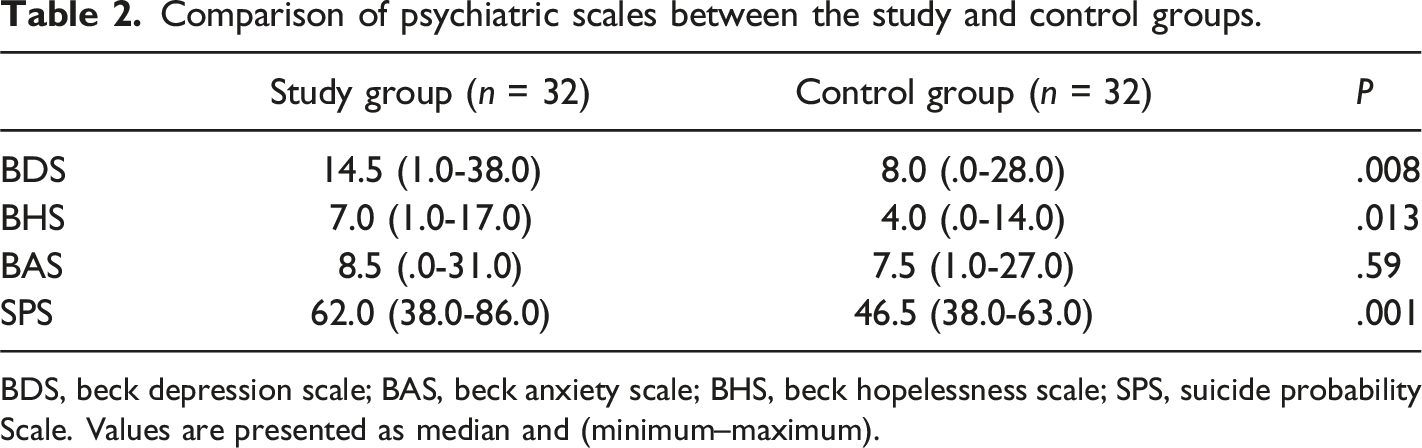
BDS, beck depression scale; BAS, beck anxiety scale; BHS, beck hopelessness scale; SPS, suicide probability Scale. Values are presented as median and (minimum–maximum).
Evaluation of the psychiatric scales scores of patients’ relatives according to gender, marital status, educational status, income, occupational status, and degree of relation.
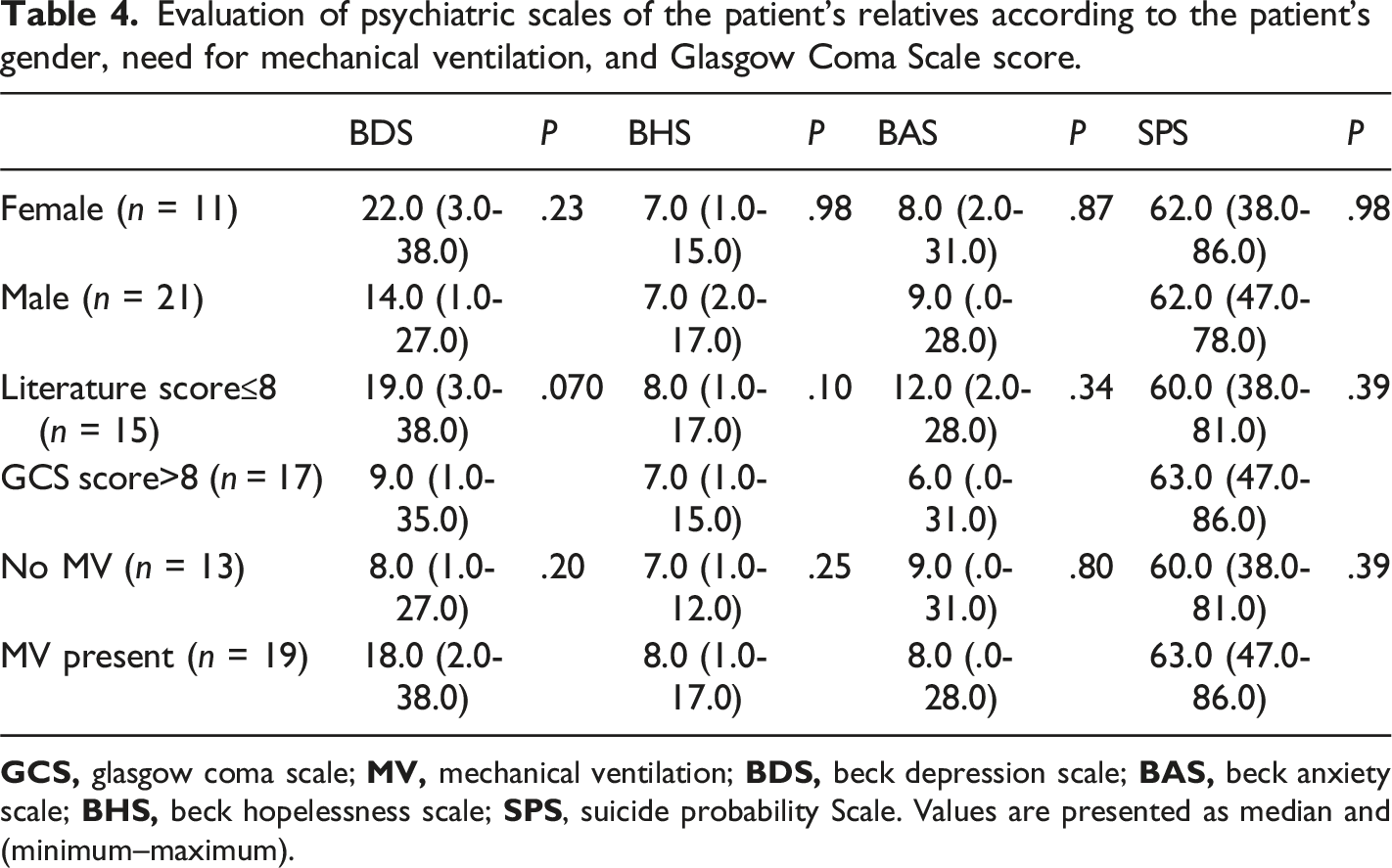
Evaluation of psychiatric scales of the patient’s relatives according to the patient’s gender, need for mechanical ventilation, and Glasgow Coma Scale score.
Discussion
In our study, the relatives of patients in the ICU had significantly higher BDS, BHS, and SPS scores than the control group. This is in line with Koukoli et al, 12 who reported that family members experience intense and variable emotions that could have long-term psychological effects. More than two-thirds of family members visiting patients in the ICU have symptoms of anxiety or depression. In the study by Gregorio rez-S et al, the mean depression scores in the study group were significantly higher than those in the control group, indicating that individuals with relatives hospitalised in ICUs should have psychiatric follow ups. 13
In our study, the likelihood of relatives of patients in the ICU attempting suicide was higher than controls. Few studies have evaluated the relatives of patients in ICU in terms of suicide probability and or susceptibility to suicide. In a study by Rodriguez et al, 14 family members scored higher on depression with suicidal ideation and anxious depression. In that study, patients were followed up for 4 years, and a decrease in suicidal ideation was observed at the end of the process. Our study indicates that a significant risk of suicide among family members of patients receiving critical care exists. As patients receive the required medical care and assistance, so too should their relatives. We believe that patients and their relatives should be considered as a whole within the health system and, if necessary, support services should establish.
In the present study, female participants had significantly higher median BDS scores than male participants. Our results are consistent with results reported in the general literature. Community-acquired risk factors for depression in women are likely to have a biological basis, such as differences in physical strength and personality traits, leading to a higher prevalence of depression among women. 15 This finding aligned with our expectation that, due to many factors, women have a high rate of depressed mood. The data we gathered showed that the relatives of patients in critical care have high rates of depression, particularly in women. Therefore, we believe professional psychiatrists should be consulted when treating depression in both men and women.
Mitchell et al reported significantly higher uncertainty and anxiety levels among parents than among daughters or sons of patients. 16 Parents find it particularly difficult to deal with their child’s critical illness. 16 Chui and Chan 17 found higher levels of stress among the relatives of patients who were parents than among other family members. Azoulay et al. 18 stated that being the child of a patient was among the independent factors with an Impact of Event Scale score above 30. In contrast to other studies, Anderson et al 19 reported that both anxiety and depression were not related to the degree of closeness with the patient.
Similarly, in our study, no statistically significant difference was found in the BAS, BHS, and SPS scores of participants who were children or parents of the patient, compared to participants with other degrees of closeness with the patient. Considering the responsibilities of parenthood, socially imposed roles, and lifelong nature of the relationships—which are prone to high levels of binding—anxiety and depression levels are likely to be high among parents. The high levels of depression in the subgroup in our study may be related to these factors.
McAdam et al 5 predicted that a younger age of the patient would increase the likelihood of depression, anxiety, and suicide because deaths at a young age are more devastating and unexpected, whereas the death of older patients is met with more acceptabilty. They reported that the only patient-related factor determining the severity of anxiety and depression symptoms is young age. However, no correlation was found between the psychiatric scale scores used in the current study and the age of the patient’s relatives, or the age of the patient hospitalised in the ICU. SAPSII score is a measurement observed in intensive care and indicating an increased risk of death in intensive care. Pochard et al 20 found that older age and a high Simplified Acute Physiology Score II (SAPS II) are associated with increased mortality in the ICU; similar to the APACHE II score, score were significantly associated with anxiety and depression. Similar to our study, Paparrigopoulas et al 21 did not observe any relationship between the age of the patient’s relatives and symptoms of anxiety and depression; Maruiti et al 4 reported that, among the relatives of 39 patients hospitalised in the ICU, no relationship between the age of the relatives and symptoms of anxiety and depression were observed; and Chui and Chan 17 reported that no significant relationship between different age groups and Impact of Event Scale scores was observed.
The GCS is scored based on observed abilities in three subscale scores (including motor, verbal, and eye opening) on a 15-point scale (range, 3-15). 22 The total score can reflect the severity of the neurological condition, and scores of ≤8 are often used to define coma. 23 In the present study, no statistically significant difference was found in the BDS, BHS, BAS, and SPS scores between low (≤8) and high (>8) GCS groups. When these patients were evaluated in terms of the need for MV, no statistically significant differences were found in the psychiatric scales. A literature analysis indicated that the effect of the GCS has not previously been examined. A study involving the relatives of 74 patients with an APACHE II score of >20 who were hospitalised in the ICU for >72 hours and in need of MV was conducted; patients were defined as being at high risk of death with the criteria of a Hospital Anxiety and Depression Scale. 5 The researchers described that, when the borderline group was included, anxiety and depression symptoms were observed in 79.7% and 70.3%, respectively. Gregorio et al found that more than 50% of the family members of patients with severe trauma who were followed up and treated in ICU had symptoms of depression. 13 In their study of 300 relatives of patients with cancer who had been followed up and treated for more than 72 hours, Lins-Fumis and Deheinzelin 24 found that anxiety and depression were associated with the need for prolonged MV and the presence of metastatic disease in the patient.
We were unable to confirm our hypothesis that psychiatric scales would be worse in cases in which poor disease severity and poor neurological recovery were predicted.
In particular, intensive care admission is an indication for the patient’s relatives that the patient’s condition is serious. Additionally, because intensive care hospitalisation is socially perceived as the bad situation possible, relatives may fail to understand the health status findings of patients in intensive care. Therefore, health care professionals should closely monitor the psychiatric well-being of all relatives, whether critically ill or not. In the study by Tokur et al, 25 76% of the relatives of patients hospitalised in ICU perceived the condition of the patient to be severe. Admission to intensive care is frightening and causes despair; belief may help with acceptance of this. 26
The strength of our study is that it is one of the few studies to evaluate depression, anxiety, suicidality, and hopelessness among relatives of patients hospitalised in the ICU.
Limitations
Our study had several limitations. First, the sample size of our study was relatively small. Second, the nature of the convenience sample selection method introduces potential bias, as participants were not randomly selected but rather recruited based on availability or willingness to participate. Third, our study did not employ multivariate analyses to control for other potential factors that could explain the observed differences in outcomes among the relatives of patients in ICUs. The limited number of patients at the endpoint precluded the possibility of conducting reliable multivariable regression analysis. Therefore, although our findings provide valuable insights into the experiences and needs of the relatives of patients in ICUs, caution should be exercised when generalising these results to a broader population. Future research with large, diverse samples and rigorous methodology, including multivariate analyses, is needed to further explore the factors influencing the experiences of such relatives.
Conclusions and recommendations
Intensive care is a long and exhausting process for both the patient and their relatives. In this study, the BDS, BHS, and SPS scores were found to be high among first-degree family members of patients hospitalized in the ICU for more than 14 days. Intensive care specialists and staff should be aware that they have a key role in detecting negative states in the families of such patients. Remembering that the patient is not the only individual affected by hospitalisation is important. The present study’s results should be expanded and elaborated on using a large sample and groups that are defined in more detail.
Footnotes
Acknowledgements
The edit was performed by professional editors at Editage, a division of Cactus Communications, in cooperation with Sage Author Services. Thanks for their support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.